
Abstract
Background
Cognition and the ability to take care of daily activities and oneself gradually declines among people with dementia. Studies are scarce, especially regarding how people with young-onset dementia (YOD) (<65 years) experience the quality of their lives with the progression of dementia. People with dementia living alone face special challenges.
Aim
To examine the experience of the quality of life with YOD as a single person.
Method
The study presents a longitudinal case study with in-depth interviews exploring the experiences of a person with YOD. Individual interviews were conducted seven times over a period of three years from 2014 to 2017.
Findings
We examined if and how seven themes concerning the quality of life and well-being were fruitful for understanding the experiences of dementia in the everyday life of a single individual. The study explored needs and challenges during the development of dementia, and how the person reacted over time, set in context. The themes significant for well-being are: identity, connectedness, security, autonomy, meaning, growth and joy.
Conclusion
The study shows how treatment, support, and services must be individualized when dementia develops in order to support identity, resources and mastering capacity, and promote well-being.
Keywords
Introduction
Dementia is ordinarily conceived as an ‘old-age disease’ (Prince et al., 2013). However, it may develop before the age of 65 years, and when it does, it is often referred to as young-onset dementia (YOD). Compared to the calculated 80,000 people with late-onset dementia in Norway, the number of people with YOD is estimated to be 4500–5000 (Engedal & Laks, 2017; Prince et al., 2013; Zhu et al., 2015). The most common type of dementia occurring at a younger age is Alzheimer’s disease, followed by vascular dementia and frontotemporal dementia (Engedal & Laks, 2017).
Gradually, cognition declines among people with dementia (Harvey, Skelton-Robinson, & Rossor, 2003; Koedam et al., 2008; Luscombe, Brodaty, & Freeth, 1998), reducing the ability to perform activities of daily living and to care for oneself. To localize and move around on one’s own become more difficult as the disorder gradually worsens (Johannessen & Möller, 2013; Spreadbury & Kipps, 2016).
In research on dementia, less attention has been given to how persons with dementia experience and evaluate their situation and how the environment can support their coping resources. Recent studies have shown that persons with dementia actively respond and adapt to the disease with their resources and abilities (Johannessen & Möller, 2013; Spreadbury & Kipps, 2016). Still, the essence of the experience of dementia is that the development of the self is undermined (Caddell & Clare, 2010; Westius, Kallenberg, & Norberg, 2010).
According to the World Health Organization and government policies in Norway, people with dementia should remain living at home for as long as possible (World Health Organization & Alzheimer’s Disease International, 2012; Ministry of Health and Care Services, 2015). However, a review study shows that people with dementia living alone have an increased risk of moving to a nursing home compared to those living with a partner (Luppa et al., 2009), and people living alone with dementia have significantly more unmet needs (Miranda-Castillo, Woods, & Orrell, 2010).
Few studies have focused on how people with YOD experience the deterioration of dementia when living alone over time and how their existence and everyday lives are affected. With this background, we conducted a longitudinal study aiming to examine the experience of the quality of life with YOD as a single person.
Theoretical background
Quality of life and well-being
The subjective quality of life is mainly studied by satisfaction with life and concerns to what degree people feel and think positively about life (Diener & Biswas-Diener, 2011). Using various measures, studies have shown that people with chronic diseases and impairments experience a lower quality of life than their healthy counterparts. People with impairments are more often lonely (Nicolaisen & Thorsen, 2017; Theeke, 2009), suffer depressive symptoms (Chen et al., 2012; Thorsen & Clausen, 2008) and are less satisfied with their lives (Patrick, Kinne, Engelberg, & Pearlman, 2000; Putzke, Richards, Hicken, & DeVivo, 2002) than those without impairments.
Several models were presented over the last few decades concerning somewhat different indicators of well-being for people with dementia, as guiding perspectives for changing the culture of care as: person-centred care (Edvardsson, Winblad, & Sandman, 2008; Kitwood, 1997), person-directed care (Fox et al., 2005), relationship-centred care (Suchman, 2006) and authentic partnerships in care (Dupuis et al., 2012).
Power (2017) presents his conceptual and theoretical framework perspective on dementia, relating the disease to a disability model and focusing on what brings well-being to people living with dementia. Referring to Fox et al. (2005), the model is described as a holistic, person-centred approach, agreeing with the intent of the person-centred models for dementia care. But he avoids the term care, in line with The Eden Alternative (Fox et al., 2005), which replaces care with living. The approach is based on a phenomenological theoretical perspective rooted in the life world of persons with dementia – they are ‘the true experts’. The goal is to enhance well-being, a concept within the research field of the quality of life, focusing on life satisfaction. Seven themes or ‘domains’ are presented as significance for well-being: identity, connectedness, security, autonomy, meaning, growth and joy. Dementia is defined as a ‘shift in the way a person experiences the world around her/him’ (Power, 2017) – an experiential definition. Dementia is conceptualized as changing disability (Power, 2017), parallel with other cognitive and functional disabilities.
Method
The article presents a case study that takes its material from a longitudinal study based on qualitative narrative methodology, with in-depth interviews exploring the experiences of single people living with YOD (Johannessen, Engedal, Haugen, Dourado, & Thorsen, 2018). The informants were from southern and western parts of Norway, recruited from six memory clinics. Among the informants, there were different dementia diagnoses and various comorbidities. A total of 10 people with YOD were asked to participate, and none declined. The sample comprised seven women and three men, ages 49 to 67 years. Our case informant here, called Elsa, was among the youngest.
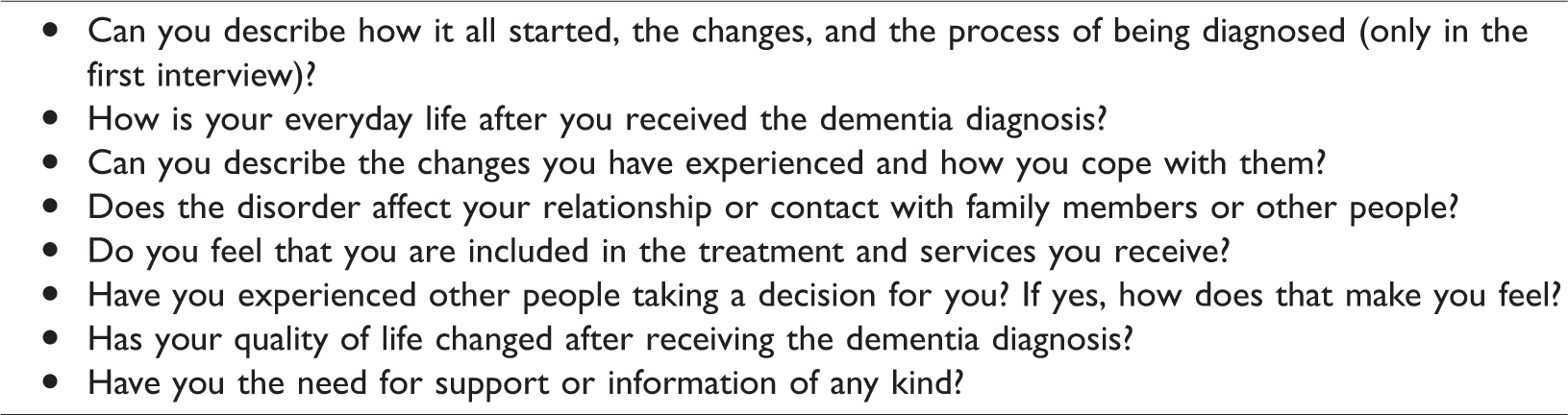
Individual qualitative interviews were conducted seven times over a period of three years. The first took place at the time of recruitment (2014) and shortly after the diagnosis was made; the other six interviews took place approximately every six months thereafter. This rather short period between the interviews with the participants was considered appropriate since significant aspects of dementia and life situation may change rapidly, such as the need for services or moving into a nursing home. The interviews, conducted by the last author (AJ), were performed at the most appropriate place for the informant (Kvale & Brinkmann, 2010). The interviews took the form of an open dialogue (Riessman, 2008), and it was important to establish trust and confidence to recruit participants for the longitudinal study as well. The interviews were audio recorded and transcribed in Norwegian verbatim by a professional typist within two weeks. A quality control check was performed by interviewer AJ, who listened to the tapes while reading the interviews. The questions are listed in Table 1. All interviews explored the experiences of the person on the day of each interview, as well as earlier experiences and reactions. Depending on their responses, the aspects and ideas raised by the informants led to further questions to obtain additional information and clarification.
Questions and themes in the interviews of the people with young-onset dementia living alone.
A qualitative narrative case study
Narrative inquiry is a distinctive form of discourse (Chase, 2011). It is conceptualized as the shaping or ordering of experience, a way of understanding one’s own or others’ actions. The person’s narrative involves organizing events and objects into a meaningful account, and connecting and seeing the consequences of actions and events over time. ‘Narration is the practice of constructing meaningful selves, identities and realities’ (Chase, 2011). Riessman (2008) argued that narrative research opens the door to stories that diverge from established perspectives and ‘truths’, indicating silenced voices and subjugated knowledge (Riessman, 2008). The voices of people with dementia certainly have been muted. Freeman (2006) called the narrative materials gathered from interviews ‘big stories’. The stories point to alternative paradigms for understanding and practice. Narrative researchers should present careful evidence for their claims (Riessman, 2008).
A case study is defined as ‘an intensive analysis of an individual unit (as a person or community) stressing developmental factors in relation to environment’ (Flyvbjerg, 2011). Case studies comprise greater detail, richness, completeness and variance – depths – for the unit included than do cross-unit studies. Case studies also indicate development over time and describe situations in context. The aim is to describe a case with many facets. The story of Elsa is chosen among the 10 participants for a case analysis, because it demonstrates her development through different stages of dementia set in her daily life. Her accounts are more detailed, and her experiences of the development of dementia more reflected on and more vividly narrated than narratives from the other informants. She gives ‘thick descriptions’ (Geertz, 1973) – including emotions, reflections, situations, people and actions – whereas the others present more meagre, matter-of-fact narratives. Her account describes the development of dementia placed in context, in time, place, situations, and interactions. Elsa is an extraordinary narrator with a rich vocabulary.
We analysed whether and how the seven themes/domains presented by Power (2017) were fruitful for understanding the vital experiences of YOD dementia of a single individual – Elsa – and how they interacted and developed over time set in context. We also explored if dominant themes were neglected by this analysis. We asked: What themes are significant for well-being, how do they interact, and what interferes with or hinders experiences of well-being when living with progressive dementia? The time axis in the analysis and presentation will be adhered to. We focus especially on the consequences of the main transition in her story; her move from a nursing home after the first interview, and then to her private home, and then again back to the nursing home before the fourth interview. Some themes are repeated in subsequent interviews, and to avoid unnecessary repetitions, we usually present details from the first elaborated interview on the theme.
Ethics
The study followed the ethics outlined in the revised Declaration of Helsinki (World Medical Association, 2013) and was approved by the Regional Committee for Ethics in Medical Research, Southern Norway (number 2013/2149). The Norwegian Data Protection Authority also approved the study (number 36797). The informant received oral and written information about the study and gave her written consent before each interviewed was conducted. We did not go into detail on her health situation in the presentation, and in other ways protected her identity.
Findings
The findings in our study are significant for well-being and are described throughout these seven themes: identity, connectedness, security, autonomy, meaning, growth and joy.
Identity
The opening question at the first interview is an invitation to Elsa to talk about her life with dementia and to inform about her former life. Since it is the first meeting, her presentation is detailed and retrospective. Elsa starts out by telling how she has changed as a person – cognitively and emotionally: The dementia has changed my head – I often cannot concentrate. I forget very much. I am also changed emotionally – I cry very easily. It is terrible, I feel ashamed. Earlier I could feel it before the tears came, I got a lump in my throat, and something happened in my stomach. You got a warning. Now it just pours out; I am not able to control anything. It is the same with laughter. I can laugh at the wrong occasions and discover that it was a mistake because other people give me a strange look.
She developed a strategy to hide her shortcomings: ‘I laughed a lot. I showed self-irony’. She adapted to other people’s derogation by belittling herself, pretending to adhere to their norms for normality. Her perception of herself was also undermined by her apologizing: ‘I feel I so often have to say I am sorry’. To say, she is sorry for doing her best and still failing undermines her self-confidence, dignity and self-worth as an individual.
Her identity crisis is described as the incongruence between her outer image – presenting herself as a youngish person – and her new persona, as transformed by dementia. The general ignorance regarding dementia adds to others’ denial of her dementia diagnosis. They do not believe it or accept it, even when they see the signs: ‘They do not understand that you can stop remembering. And a dementia diagnosis is something at least all the people I know think you can only get when you are old’. She is recently divorced from her husband. She mentions that he and her son do not believe in her diagnosis and do not see it as something to take notice of. They want the ‘old Elsa’ they knew back, and she emphasizes that she is ’not able to be that person’. She wishes she were not so aware of her transformation and deviation. The narrative about lacking support for her new identity with dementia continues in the subsequent meetings in her private flat.
However, at the fourth interview after having moved into the nursing home, Elsa experiences a great sense of relief. She still feels shame, but she is no longer reproached for her mistakes. She repeatedly emphasizes: ‘It is so important to be allowed to be yourself. In life outside, I use so much energy trying to pretend [to be] as normal as possible. But it always goes wrong (laughs)’. She moved into a nursing home with a different definition of normality, where her mistakes are accepted as normal for her disease.
Connectedness
At the first meeting, Elsa informs that she has left her husband after ‘many years of good marriage’. The change from close connection to disconnection is felt as dramatic and sad. Her son has been offered information about dementia but avoids talking about it. She thinks that he is not able to accept that his mother got dementia in her fifties. ‘The talk is much about what I was and I what did’. She has withdrawn from family gatherings, as her weakened memory makes them too demanding and difficult: I was fond of the family, but I was not able to participate in the conversations. I did not remember who had a birthday, when we met the last time, and which old grandmother had undergone an operation – all the things you normally remember. I made awkward situations, sad situations – and I withdrew.
It is easier for Elsa to have a dialogue with one person than with many. She appreciates that the interviewer is a calm and empathetic person. She is satisfied that the dementia has been the focus of their talk: ‘Nobody else asks about it’. She misses others being open to her reactions, which had implied respect for her and her experiences. ‘But probably it is ‘taboo’. We shall not talk about it. I think there is a lot of taboo around dementia’. When she feels that others are stressing and nagging at her, she prefers to be alone. Contact by phone is not an option. To get the correct cues in conversations, she depends on mimicry: I hate to speak on a telephone, for I do not see the person, and then it gets worse. It is about the whole expression on the face. As a human being, you read others. You can see much in a face that you do not see through a telephone.
At the fourth visit, when she has returned to the nursing home, she tells about the transformation to the social person she was earlier. She now prefers to sit in the living room with the other residents. Her feeling of security has restored her sense of connectedness to other people. ‘All [the] people here are nice. There is always someone to talk with’. She enjoys being with other persons.
Over time, the contact with other residents becomes more demanding, complicated, and exhausting. She does not remember who they are and has also forgotten earlier information. She feels the old ladies talk too much. In the last interviews, she remarks that all the other residents ‘are over 90 years old’ and says, ‘It is me and the old ladies. They are so sweet – and angry as well’. But now she misses someone like herself, of her own age, to talk to. She stays in her room much of the time with the door open. She is comforted by the voices of others but prefers to sit quietly, not participating.
Her son now knows more about dementia; he understands more about his mother’s reactions and has become ‘more clever’. But he still corrects his mother when she makes mistakes, saying, ‘You did not do that before, mother’. She experiences often being shut out of her family’s talk about everyday life. She senses that she is considered ‘too stupid’ to be informed and thus is placed outside normality.
Security
At the first interview, she remarks that she no longer trusts others – not even her closest family members – and reflects on feelings of security. Looking back at the hospital where she was assessed for a diagnosis, she says: I liked it very much, for it was safe. Nobody demanded anything, or asked me questions about why I forget. I could be myself. Nobody told me I had to sharpen me or corrected me or made me feel ashamed.
At the next interview, in her new flat, she is experiencing steadily increasing anxiety. She has written down her problems in order to report them accurately to the researcher: I have become afraid of being alone, and I have morning anxiety. It is difficult to put in words, but I am afraid to meet the new day. You know, nobody knows what everyday life will bring, but I am not able to handle it like I did before. I am very scared and much misunderstood.
A support contact person comes once a week. (This is a person paid by the municipality for a number of hours a week to assist the person in everyday activities, provide social contact and follow the person to activities outside the home.) She has strengthened Elsa’s feelings of social security, and she brings delight. Elsa comments, ‘I always look forward to meeting her because she knows about dementia, and there is no fuss and stress about her. She is very nice’. She continues her contact with the support person throughout the entire interview period.
At the fourth interview, Elsa has found safety in the nursing home and is tremendously relieved. Safety has released her energy and lust for life: ‘Now I am well, safe, and can even sit quietly and take on knitting, which I have not done for a long time, and feel that it is peace – even if the elderly fuss a lot’ (laughs).
Autonomy
‘Inner’ autonomy is gradually reduced by Elsa’s memory problems. She explains at the first meeting that earlier she was … more organized in my head. I get so terribly tired of myself. I use so much energy trying to concentrate and get quite exhausted. Two hours are felt like a marathon. In daily life, there are issues popping up unexpectedly, when you have to concentrate on things that went smoothly earlier.
She hoped that her decision to move to a new, modern flat in the centre of the town would increase her coping abilities – but is not successful. She does not remember where things are, and says that she can use the whole day just looking for her things. Her autonomy at this stage is not restricted by outer authorities or physical and institutional barriers. She has set herself ‘free’ from a husband, and moved to the new flat to be on her own. ‘But it is extremely difficult. Sometimes I cry a lot. I am very afraid of the future. How am I able to manage to arrange for a so-called normal life?’ The autonomy she wanted, trying to manage on her own, has turned out to imply a lonely and scary existence.
Living alone has gradually reduced her autonomy and self-determination. She is no longer able to shop for groceries; she is dependent on help from shopkeepers. Ordinary, everyday activities are a ‘full-time job’ and she admits: ‘I give up a bit’. Her experience of losing control affects both her autonomy and security. Her anxiety and unrest are ‘because I am losing control. Yes, it is the strange control you normally have on your life. I am no good to discern danger from normality. Strange. I lose oversight’. Risks and dangers are potentially everywhere when one’s capacity to evaluate is diminished or gone. Moving to a nursing home restores autonomy; however, it is a different autonomy – an assisted autonomy performed in safe surroundings.
Meaning
Elsa describes a lack of meaning in the first interviews, talking about her loss of relationships. The meanings and functions of actions are gradually lost. Living alone makes the loss of meaning more evident. In addition, former meaningful and joyful activities lose their attractions. The efforts needed to perform even pleasurable activities are felt to be too great. Her life alone is dominated by striving to preserve as many of her meaningful and basic abilities as possible, but the rhythm of the day is hampered by her loss of time structure. ‘I have plenty of time, but do not remember when the last time things were done’.
As presented, meaning in life is lost when Elsa lives alone, but changes dramatically in the nursing home, where she experiences new vitality (more details in the next section).
The progressive memory loss has erased her remembrance of her life history. In the nursing home she has taken on the task of restoring parts of her biography. She has asked some of her old friends to write down what they remember she previously told them about her marriage. The story is intended to bolster her decision to divorce her husband but also to preserve the good moments: They have written for me so that I can read it, and that I agreed to move out. I have forgotten all about it; I forget so much. I had only some glimpses in my heart. I wanted to take care of that, so that I could read it and preserve a more correct picture.
Growth
Moving back to the nursing home brought a remarkable revival of Elsa’s personality and a revitalization of her meaningful activities and interests. Before the fourth interview starts, she wants to show the interviewer her small garden. ‘I like to be out here and look after the garden; it is so beautiful. Watering, planting, and digging. To find plants and flowers’. She is training intensively to preserve her abilities. She uses her PC every day, which was a work tool at her job for 20 years. I want to remember as much as possible. I understand that I should train and train. I can sit for two to three hours trying to pay my bills. I get angry, frustrated, and irritated, make mistakes, and I must repeat, but I shall manage. At last I do! I can tell you, now my brain is working! You can’t just sit in a chair. Earlier I always did useful things. It is important, even when it sometimes goes very slowly and things are placed in wrong places. And here they do not repeat and repeat, and point out, like they do outside. I also take a lot of photos of my neighbours, because they love to see pictures of themselves. I hang them in the corridor here, and change them after a while. ‘It is me!’ they say, and they look at them now and again and are so glad.
At the last interview, her story has lost some of the euphoria from the first period in the nursing home; now she talks more about losing abilities. She makes more mistakes when writing. It worries her and brings forward the old feeling of shame. The loss of writing capacity also causes less contact with others; she has abandoned written contact with others since she writes so badly. Losing abilities has an impact on her identity. ‘You get sad when you feel stupid, when you never have been stupid before’.
Joy
It seems like a paradox that Elsa’s most joyful moments living alone at home were because of her support contact and not her friends and family. The support contact offers her assistance for everyday tasks, provides company, reduces anxiety about making mistakes, shares her interests, stimulates activities and brings sheer joy. ‘She is so sweet. Very all right. We do enjoy ourselves. Now we shall go and buy flowers and plants. I look forward to that’. The support contact is something of a substitute for her old friends.
The lust for life she experiences in the nursing home brings back earlier pleasures and joyful activities. ‘I have always liked to be smart and dress up, but when living alone, I was so scared that I did not think about it, but now I have started to smarten myself up’.
Living in the nursing home, her joy over the kind and supportive surroundings maybe brings about a revival of herself, but weakens somewhat over time. She emphasizes that it is important to appreciate what one has. Outdoor walks – looking at others – bring pleasure. ‘It is a strange feeling, just sitting out there and looking at people. I could have done that for days’. Looking at people has become a way of handling connectedness.
In the last interviews, her feeling of joy for being ‘safe’ is replaced by more mixed emotions. She differentiates between her outer circumstances and her inner status: Here in the nursing home, I have a good life, for people are kind and it is safe. But inside me, it goes up and down. I am maybe a little calmer, but I can quickly change emotionally, cry, but also be glad. I often feel like a child.
As a clown, everyone accepted her deviance from normality.
Discussion and conclusion
Elsa’s case revealed that the seven themes of identity, connectedness, security, autonomy, meaning, growth and joy have been fruitful to understand an individual’s existential living with dementia – the significant experiences. They seize how the individual is trying to preserve a valued self, meaning and life lust – with progressing disabilities. The proposed theoretical model of dementia as a disability (Power, 2017) seems to be in accordance with Elsa’s existential experiences.
A conclusion from the study is that the seven domains are intimately interrelated. There is a continuous interplay between the domains, sometimes in tune, sometimes in conflict. Elsa’s accounts give detailed descriptions of her existential turmoil living with dementia over time: how dementia disturbs memory, cognitive abilities, emotional reactions and functional capacities – and erodes control in her existential living. The multiple intertwined reactions may be presented in the description of one situation, and even told in one sentence.
The case study also shows that some of the seven themes are more fundamental than others. The dominant encompassing theme is identity. The experience of having continuity, living now in time, having a future to plan for and having a past – a life history – is gradually eroded. Elsa repeatedly underlines how important it is feel and be ‘herself’. Her narratives present and construct herself as the totality of complex and conflicting feelings. The case study reveals that to be yourself with dementia, to be seen, accepted and respected as an individual person is the core striving of existential living with dementia (Caddell & Clare, 2010; Westius et al., 2010). Identity needs confirmation from others to be sustained, especially when the person is vulnerable. We see how her identity loses positive feedback and confirmation from those who are nearest to her. They expect ‘the old Elsa’.
The study shows that the experiences of the erosion of self vary greatly in different living conditions. Family caring is not always supportive, but may undermine identity when the existential implications of dementia are denied. People must be recognized as individuals with dementia, and their human dignity must be respected (Norberg, 2017). The study also demonstrates that, for Elsa, security is the basis of identity, connections, autonomy, growth and joy, in line with the findings of Power (2017). When anxiety and protection against risk become dominant, her everyday life shrinks to isolation and inactivity.
Autonomy is defined by Fox et al. (2005) as ‘Liberty, self-government, self-determination, immunity from arbitrary exercise of authority, choice and freedom’ – high aspirations, even for people without cognitive impairments. Elsa reflects on how dementia erodes her capacities for self-determination. ‘Decisions are hopeless. Completely hopeless, because I do not know any longer what is for my best. I have no ideas’. Power (2017) underlines that security is needed to optimize autonomy, but he also warns that overemphasis on physical and emotional safety can erode one’s autonomy. He points primarily to security regulations at institutions and overprotective family members. But Elsa’s story shows how inner barriers, such as fright and shame, restrict her life world and her role as an actor. She feels unable to act in a ‘normal’ way, according to cultural norms. Her surroundings become frightening, resulting in withdrawal, disconnection and loneliness. Her new private home becomes a prison, and life is without growth and joy.
The remarkable and significant result of the analysis is how Elsa regained security in the nursing home, revitalizing herself as an active person, stimulating her abilities and bringing joy back to her life. Modern nursing homes may provide just the kind of individualized support that optimizes autonomy and mastering capacity for people with dementia (Baker, 2007).
Narrative analysis is also concerned with what is not told, i.e. what is hidden or placed backstage. What themes are overshadowed by the seven positive, formulated, conceptual themes? These are the negative experiences – shock, despair, depression, shame, estrangement, disconnection, solitude and loneliness – that are experienced at different stages. However, all are included in the narratives. As shown in the presented accounts, Elsa consistently contrasts her reactions and evaluations. She distinguishes between her genuine self and the self that other people see or wish for. She divides the world between ‘inside’ and ‘outside’, the secure and scary places, the kind and nagging people and those she trusts and distrusts.
Is there a prominent theme in her stories that seems to be neglected in the research on dementia? A dominant repetitive theme in Elsa’s narratives is shame. Shame is a concept that places the individual in a social context, interrelated with others and immersed in the culture’s norms for normality and accepted conduct. Shame signifies personal feelings of failure and a lack of acceptance from others. Scheff (2003) proposes that shame is the master emotion of everyday life, but it is usually invisible in modern societies because of taboos. Shame is accentuated by the stigma of dementia, and the disbelief that Elsa, as a rather young woman, can have this disease. The stigma of dementia is well documented by a study of Behuniak (2011). and reports from people with dementia (Aquilina & Hughes, 2006; Taylor, 2007), which describe how people immediately change their communications and relationships when they are informed of the diagnosis (Simpson & Simpson, 1999).
Studies (Arons, Krabbe, Schölzel-Dorenbos, van Der Wilt, & Rikkert, 2013; Sands, Ferreira, Stewart, Brod, & Yaffe, 2004) have shown that information about the quality of life of people with dementia by proxy (e.g. family members, health personnel and staff in institutions) deviates from their own experiences. It is essential to give the voices of people experiencing dementia a far greater place in research, society, culture, and in care systems to make their existential lives as good as possible. Our narrative phenomenological study of dementia addresses the need for other longitudinal studies about self-reported experiences of dementia, and for rare forms of dementia where there is little qualitative research reported.
Strengths and limitations of the study
‘What is this case a case of?’ (Flyvbjerg, 2011). We argue that the themes analysed, based on Elsa’s narration as a case, offer insight into the experiences of dementia in one person over time that may be valid for many people with YOD who are living alone with dementia. Certainly, there are also great variations within a group of single people with YOD, and Elsa’s case does not inform about the situation for married or cohabitating couples. It is a ‘female story’ in regard to its content and rich vocabulary describing feelings, compared to the male stories in the larger study. It is also a story of dementia experienced by people with YOD and how their lives are affected by a disease associated with old people. The stories told at the end of a long life will be different.
The main strength of the case study is its detail, richness, completeness, and within-case variance. We carefully selected and presented rich material from Elsa’s narrative accounts as evidence (Riessman, 2008). The narratives show emotions, cognitions, evaluations, needs and actions, and how they are related in one person. The recounts are placed in context and show existential living with dementia developing over time.
Conclusion
The study documents that persons with dementia can present detailed descriptions of their emotional reactions and evaluations of life with dementia. The implication for the care system is that their opinions about their needs during the progression of the disease must be heard, and should provide the foundation of individualized support promoting well-being. Moreover, institutional settings must be transformed in order to support individual identities and mastering capacities.
Footnotes
Author Contributions
KT and AJ designed the study. AJ collected the data. KT was principally responsible for the analysis. The three authors contributed equally to the drafting of the manuscript and the final revision.
Acknowledgements
The authors wish to thank the participants for sharing their experiences, along with the Research Council of Norway, who supported the study. They also thank Anne-Lise Eriksen, who transcribed the interviews.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.