
Abstract
This article explores how individuals with dementia and their relatives discursively construct dementia-friendliness in a situation where different definitions of this term exists. Thirteen semi-structured interviews were conducted, including seven individual interviews with people living with dementia. The remaining six interviews consisted of three interviews with the relatives of a person with dementia and three with married couples of which one were diagnosed with dementia. Notes taken by the first author during 6 months of fieldwork at a day centre and a drop-in centre for people with dementia and their families were used to supplement the interviews. Critical discourse analysis provides an analytical tool for revealing the discourses constructing dementia-friendliness. The analysis revealed that people with dementia and their relatives draw on the three discourses of sameness, security and care and autonomy during their attempts to construct dementia-friendliness. The ensuing discursive battles over dementia-friendliness appear to constitute a tightrope walk between the inclusion and exclusion of people with dementia, which underscores the importance of including the voices of people living with dementia when dementia-friendly initiatives and communities are developed.
Introduction
Across Europe, including in Denmark, the number of people living with dementia is expected to increase over the coming decades. With increases in the average life expectancy resulting in larger proportions of older individuals, the number of people with dementia in Denmark today is expected to rise from 1.51% to 2.65% of the total population by 2050 (Alzheimer Europe, 2019). Dementia affects an individual’s cognitive abilities in various ways, causing the gradual deterioration of memory, attention, language skills and planning abilities. Changes in behaviour, such as moodiness and anxiety, have also been noted. Living with dementia is, therefore, associated with physical, mental and social changes that often interfere with the affected individual’s ability to maintain activities of daily living (Jørgensen, 2018). With no pending cure in sight, the expected increase in the number of people with dementia is reflected by the emergence of dementia-friendliness and the ongoing development of dementia-friendly communities and dementia villages.
Different definitions of dementia-friendliness exist. However, they appear to be open for individual interpretation, with no guarantee that dementia-friendly initiatives will reflect the actual needs of people with dementia and their families (Lin, 2017). Alzheimer’s Disease International defines dementia-friendly communities as ‘a place or culture in which people with dementia and their carers are empowered, supported and included in society, understand their rights and recognise their full potential’ (Alzheimer’s Disease International, 2016 p. 10) – and further argue for dementia-friendliness being a social construct (Alzheimer’s Disease International, 2016 p. 8) and the need for communities to be able to adapt the broad principles to local and cultural contexts (Alzheimer’s Disease International, 2016). The principles are informed by the goal that the physical, social or cultural environment should support the everyday lives of people with dementia and their families. The efforts to develop and establish dementia-friendly initiatives have ranged from small-scale municipal initiatives, such as using coloured signs to help individuals orient themselves within local shops (Alzheimer’s Disease International, 2016; Hebert & Scales, 2017), to larger-scale initiatives, such as attempts to educate the larger community about the disease and how to meet and interact with people with dementia (Alzheimer Europe, 2015; Alzheimer’s Disease International, 2016; 2017; 2018; Shannon et al., 2019; Williamson, 2016).
Since the publication of the Danish action plan on dementia in 2017 (Danish Ministry of Health, 2017), municipalities and non-governmental organisations have worked towards the goal of transforming Denmark into a dementia-friendly country. The action plan states that a dementia-friendly society is one in which people with dementia and their families feel secure because the public has been educated in dementia issues and the physical environment has been arranged to support people living with dementia (Danish Ministry of Health, 2017). The Danish Dementia Alliance was established in 2014 by the Trade Union of Public Employees, the Danish Association of Occupational Therapists, the Danish Nurses Organization and others. This alliance outlined six ambitions for dementia-friendly municipalities, focussing on the following issues: (1) improving the possibility of early diagnosis; (2) supporting the families of the dementia-affected individuals; (3) improving the competencies of caregivers working in the field; (4) increasing the general accessibility and inclusion of people with dementia; (5) providing housing that better suits the needs of people with dementia; and (6) supporting dementia-relevant research (Demensalliancen, 2016b). In addition to creating dementia-friendly communities, the dementia-friendly ‘movement’ in Denmark has included the intent to establish dementia villages. Inspired by the Dutch dementia village of Hogeweyk, several Danish municipalities are planning to establish or have already established nursing home care services and dementia villages, with the explicit aim of being dementia-friendly (Danish Ministry of Health, 2017; Demensalliancen, 2016a; Healthcare Denmark, 2018; Peoples et al., 2018). In the aim of dementia-friendliness the intention of the villages is to create designated areas within the local communities in which people with dementia experience feeling safe and a high degree of freedom. Thus, dementia villages in Denmark tends to approximate for dementia-friendliness (Peoples et al., 2018).
The vagueness associated with existing definitions of dementia-friendliness has resulted in multiple interpretations of this term and the development of heterogeneous interventions. Despite a shared political objective (Hansen, Praestegaard, et al., 2021) to effectively respond to the needs and expectations of individuals with dementia and their families, the lack of their voices has resulted in a general sense of uncertainty regarding whether the implemented interventions meet the actual needs and expectations of dementia-affected individuals. Regarding how people with dementia and their families construct dementia-friendliness little is known; therefore, this study aimed to explore how people with dementia and their relatives ascribe meaning to and discursively construct dementia-friendliness.
Materials and methods
This study was conducted as multi-sited ethnographic fieldwork (Marcus, 1995) in Denmark between September 2018 and March 2019. The methods included participant observation, conversations and interviews.
Setting
By subscribing to the idea that local places are connected to and influenced by large-scale entities (Marcus, 1995), the multi-sited fieldwork made it possible to follow the movements and connections to uncover how dementia-friendliness is both transformed and constructed by people in different locations. The ethnographic fieldwork occurred at a day centre and at a drop-in centre in one of Denmark’s largest municipalities, which features approximately 205,000 inhabitants, and both observation sites represented municipal services that were offered by the state. At the time of data collection, a planned dementia village was being developed by the municipality. The dementia village received much attention among the residents of the municipality, including the participants in this study.
The day centre was located in a nursing home annexe in the municipality. According to the Danish Act on Social Services, day centres are obligated to offer sustaining activities for people with dementia and others with similar needs (Retsinformation & Social-og Indenrigsministeriet, 2019). Referral to the day centre is administered by local authorities, whose decisions are based on the evaluation of an individual’s dementia symptoms. Activities in the day centre are focused on supporting the visitors’ abilities to recover and maintain skills that are necessary for independent living (X Kommune. Ældre og handicapforvaltningen, 2017). During workdays, the day centre was visited by an average of eight people, all of whom were diagnosed with dementia. Depending on each individual’s dementia symptoms and needs for support, some visited the centre several days each week, whereas others only visited once a week.
The drop-in centre was a counselling and activity centre located on the outskirts of the same city, which offered activities for people in the early to moderate stages of dementia and their families. This centre was open to everyone, regardless of whether they had received a dementia diagnosis or had received a referral to the centre. Activities, such as choir singing, gymnastics, bowling, and an open café and counselling service, were offered at the centre, which aimed to create a welcoming community (Demensfællesskabet Kallerupvej, u.å).
Participants
The study participants were recruited among those visitors to the two centres who were diagnosed with mild-to-moderate dementia (Jørgensen, 2018) between September 2018 and March 2019. Based on first author’s initial interactions and conversations with participants and together with the managers of the centres, potential participants were assessed for their cognitive abilities to provide informed consent based on observations of, for example, their ability to express themselves about their experiences. The consent was continuously negotiated during field work and at the introduction and at the end of all interviews (Davies, 2008; Thorogood et al., 2018).
Personal information.
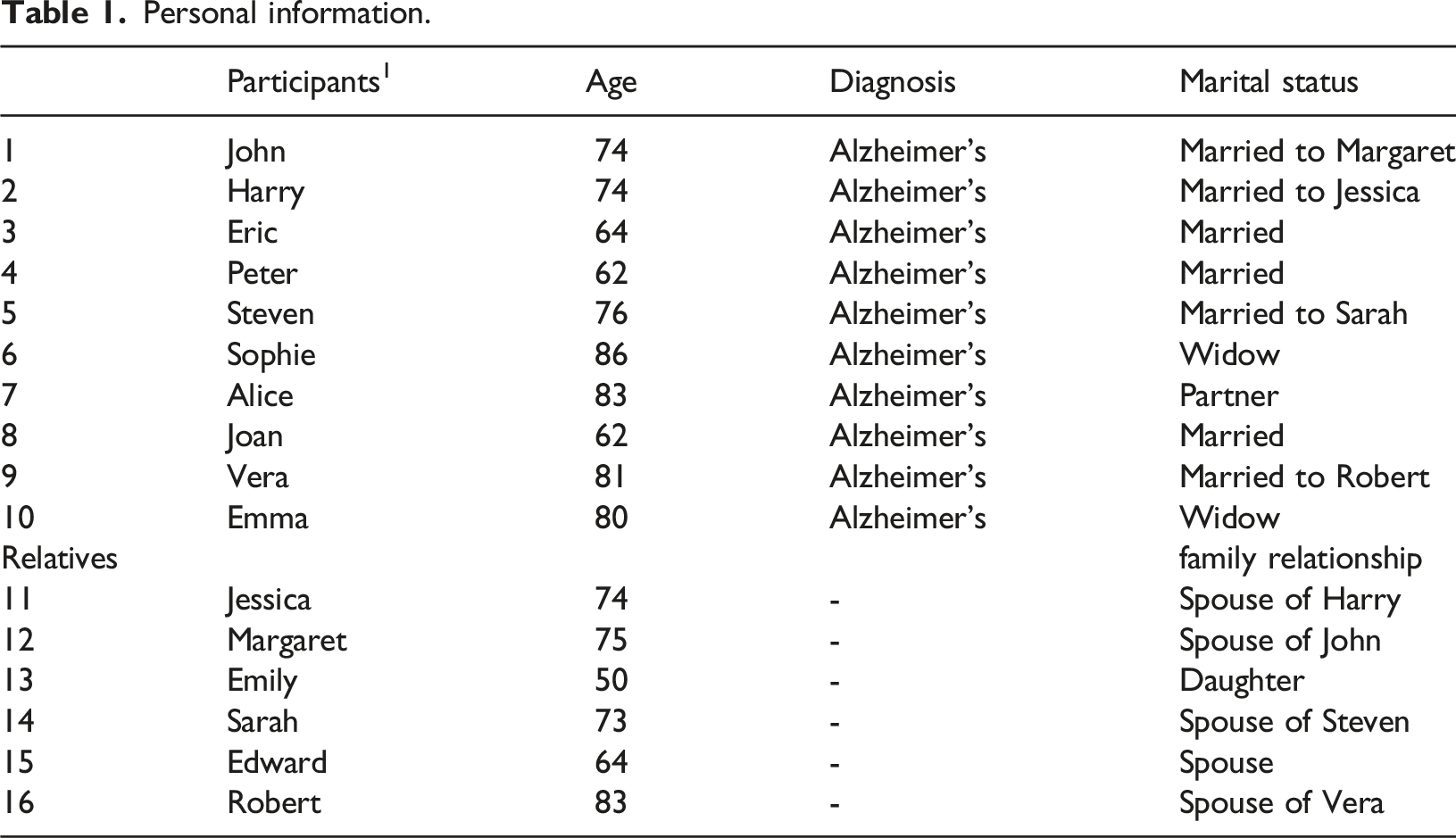
To secure their anonymity, the participants’ names have been changed, and other identifying information has been removed.
Participant observation
The choice of participant observation was made to enable first author to understand the notions of dementia-friendliness as they pertain to the physical, social and cultural environment (Bundgaard et al., 2018; Davies, 2008; Hammersley & Atkinson, 1983). During fieldwork at the day and drop-in centres, first author was present for two or three days each week. First author participated in scheduled activities, such as breakfast meals, café, singing, dancing, card-playing and excursions. Active engagement in the activities facilitated a better understanding of the relationships between dementia-friendliness and the environment, which also provided useful insights when interviewing the participants. The observations were described according to Spradley’s nine dimensions, focussing on physical surroundings, people, activities, objects, actions, events, time, goals, and the emotions felt and expressed (Spradley, 1980). The time spent in the centres provided first author with the opportunity to become familiar with the places, relate to their users and consider candidates for participation in the interview study. Participant observations included following seven of the participants with dementia to different places and activities outside of the centres, at the discretion and with the permission of the participants. Observations were documented using field notes and photos of the physical surroundings. The photos were used as a tool to document the appearances of the physical surroundings. The notes were prepared during activities, except where this was deemed inappropriate, in which case they were prepared or audio-recorded later, as described by Emerson, Fretz, and Shaw (Emerson et al., 2013) and Davies (Davies, 2008).
Conversations and interviews
The study included various types of interviews and conversations with the participants and centre staff. The conversations occurred spontaneously, such as during coffee breaks at the dining table, at meetings or in the living room. When first author participated in excursions or gymnastics, the conversations prompted questions about the participants’ experiences, providing a tool for gaining access to each participant’s lifeworld. The collected data provided an understanding of each participant’s experiences and immediate reflections on multiple topics and experiences (Davies, 2008; Hammersley & Atkinson, 1983; Mason, 2018).
Thirteen semi-structured interviews (Mason, 2018) were conducted by first author, seven of which were individual interviews with people living with dementia (Participants 2, 3, 4, 6, 7, 8 and 10), three of which were individual interviews with relatives (Participants 13, 14 and 15), and three of which were small-group interviews with married couples (Participants 1 and 12, Participants 5 and 11 and Participants 9 and 16). The times and places of the interviews were chosen by the participants. Three of the individual interviews were conducted at the drop-in centre, and four were conducted in the participants’ homes. The interviews with relatives and married couples were conducted at their homes.
Guide for semi-structured interviews of people with dementia and relatives.
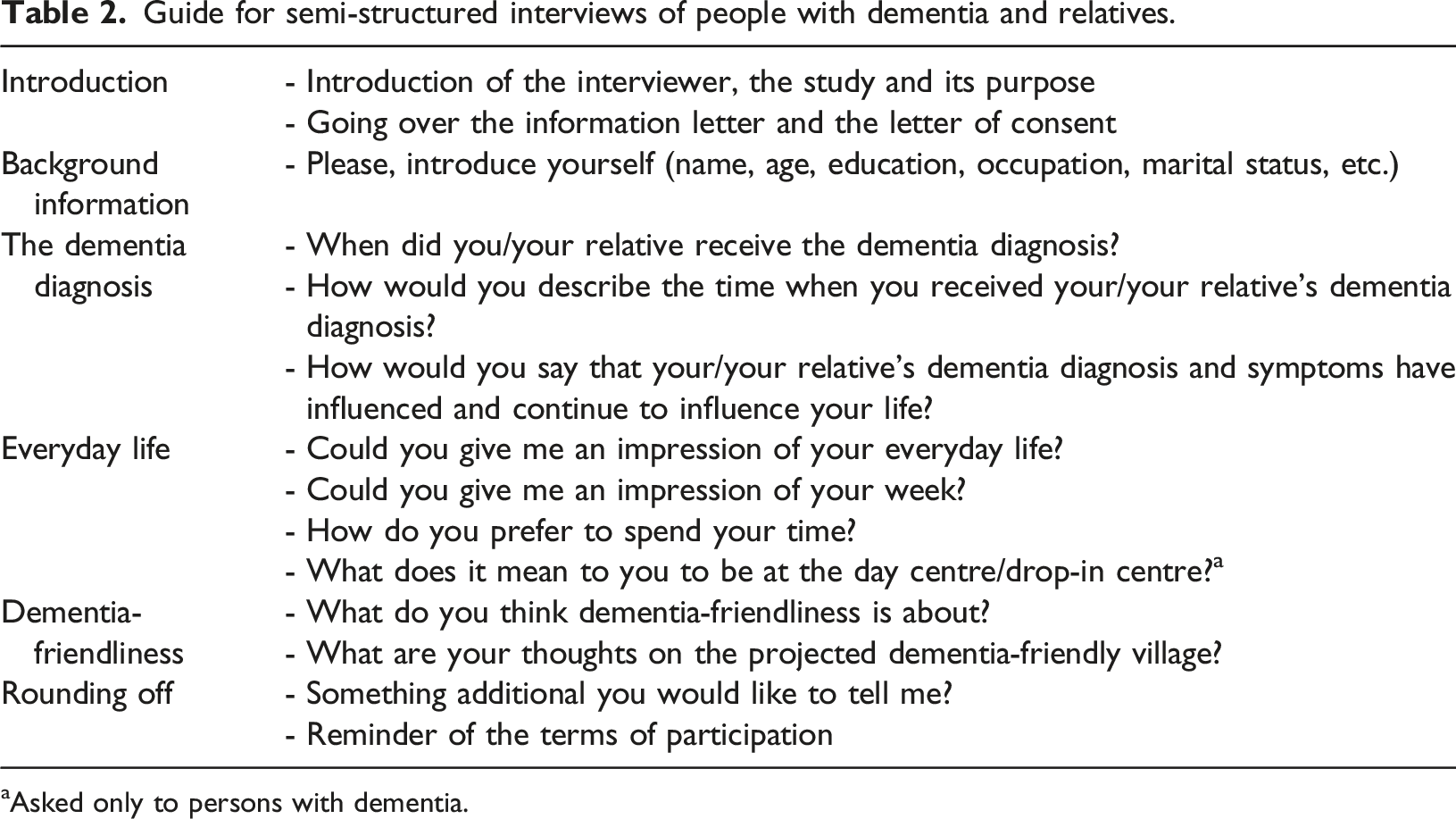
aAsked only to persons with dementia.
To build rapport with the participants and create a safe atmosphere within the interview situations, the initial questions focused on descriptions of the participants’ past lives. Afterwards, the questions concentrated on their current lives and, last, the participants were asked about their thoughts on dementia-friendliness and the projected dementia-friendly village. The interviews lasted approximately 60–90 min, and they were audio-recorded with permission from the participants and later transcribed verbatim.
Critical discourse analysis
To assess the discourses constructing dementia-friendliness, we conducted a critical discourse analysis, inspired by the method described by British professor and linguist Norman Fairclough. The concept of dementia-friendliness may be considered a discursive construction (Fairclough, 1993, 2003) based on the assumption that the ways in which we express ourselves in regard to a phenomenon, such as dementia-friendliness, simultaneously influences and is influenced by the position from which we speak and the words we use to describe the phenomenon. However, discourses are dynamic and mutable when they meet resistance, which may result in discursive battles. Words, concepts and designations can gain dominance and become integrated into the prevailing discourse. Discourses contribute to the production and exchange of knowledge, identities and social relationships; therefore, discourses are co-constituents of the perceptions of social practices and frame how we act, understand and refer to the phenomenon in question (Fairclough, 1993, 2003), which in this study is dementia-friendliness. Discourses have also been shown to reproduce or change social identities, resulting in the creation of unequal power relationships. According to Fairclough, social identities are expressed in discourse (1993; 2003), and the terms used by others to describe people with dementia and the terms that individuals with dementia use to describe themselves and others living with dementia represent a negotiation of the social identity that is ascribed to being a person living with dementia. The negotiation is assumed to influence the construction of dementia-friendliness, both by individuals and in the general discourse, which affects how dementia-friendly initiatives are developed and established to meet the needs of people with dementia.
Critical discourse analysis was used in this study to understand the language used by individuals with dementia and their families to construct dementia-friendliness. Transcriptions of interviews and conversations/situations from field notes were used to analyse the discursive construction of dementia-friendliness among people living with dementia and their relatives, based on interactions with these individuals, their use of language, and shared or opposing definitions and values.
Analytical strategy
Both written and spoken language use can be understood as communicative events (Fairclough, 1993). Additionally, Fairclough argues that gestures and facial expressions are components of a communicative event (Fairclough, 2003). Therefore, when analysing the field notes, they were largely treated similarly to written language.
Analytical levels, with questions (Fairclough, 1993, 2003).
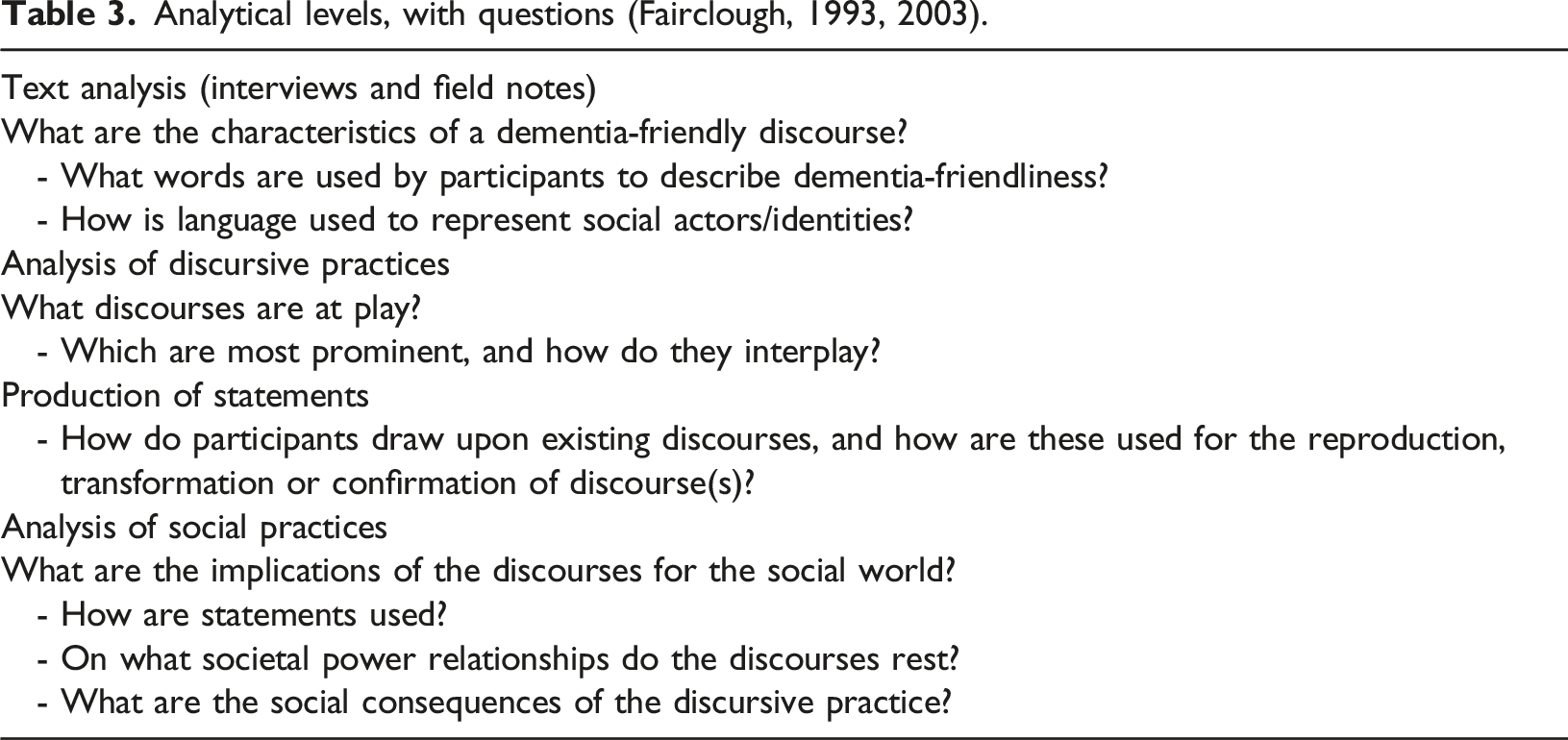
The formulations in Table 3 should be viewed as analytical abstractions designed to guide the analysis of the interviews and field notes (Fairclough, 1993). The analysis of the discourses related to dementia-friendliness is presented below.
Ethical considerations
Conducting participant observations and performing interviews, in general, require continuous ethical considerations (Davies, 2008; Mason, 2018). The recruitment of participants occurred in consultation with the respective leaders of the day centre and the drop-in centre. Although the participants expressed openness to the presence of first author, ongoing negotiations occurred, particularly at the beginning of the fieldwork but also along the way (e.g. when a participant asked, ‘Why are you here’?). Therefore, consent was continuously and verbally negotiated during the fieldwork period (Hellström et al., 2007; Mason, 2018).
The knowledge and familiarity gained from the participant observations contributed to the establishment of rapport with the participants during the interview situations. To avoid inflicting harm when conducting the interviews, first author continuously focused on adjusting the interview situation (Cridland et al., 2016; Hellström et al., 2007). The aim was to conduct the interviews at an appropriate pace, by being quiet and leaving space for the participant to think or repeat some of the answers (Cridland et al., 2016). When conducting the interviews with the married couples, an effort was made to allow both participants time to speak.
Ethical approval and consent
The study was designed according to guidelines established by the Danish Code of Conduct for Research Integrity (Ministry of Higher Education and Science, 2014) and followed the ethical principles of the Helsinki Declaration (World Medical Association, 2013). Accordingly, the participants were informed about the general aim of the study both in writing and verbally. Written consent approving inclusion into this study was obtained from all participants. The protocols for the ethical issues and management and security of data associated with this study was reviewed and approved by the Research and Innovation Organization, University of Southern Denmark (journal no. 18/32442).
Findings
The analytical findings are presented through quotes from the interviews and field note excerpts. Initially, we present the construction of dementia-friendliness expressed by people with dementia and their relatives to demonstrate the challenges that most participants encountered when constructing dementia-friendliness and their doubts regarding this concept, which they expressed in various ways.
Challenges when constructing the meaning of dementia-friendliness
Dementia-friendliness appeared to serve as an umbrella term, covering a multitude of discourses. The difficulties met when constructing the meaning of this concept were clear from the interviews and the conversations recorded in the field notes. This difficulty is illustrated in the following excerpt from field notes taken during an open café day at the drop-in centre. As people drop in, I say hello to each of them, introducing myself as a PhD student who is working on a project with a focus on dementia-friendliness in Denmark. Several people say, ‘Dementia-friendly’? adding that it sounds exciting or interesting, or that they have never heard of the phrase dementia-friendly before. Only Eric acknowledges his familiarity with the concept and gives me to understand that he finds it to be a good thing that I am doing this project, ‘as it seems no one knows what it means’ to be dementia-friendly. We are sitting around the dinner table. In addition to a centre volunteer, Carl, a married couple, two male centre users, and one female centre user are present. My introduction of the project stimulates a good deal of discussion around the table. Some discuss it among themselves, while others address me and those around me. This excerpt demonstrates the welcome that I received at the centre and the perceived relevance of the study. The questions raised over the use of the term friendly shows the presence of various views regarding dementia-friendliness. A man says he does not understand why it is called dementia-friendly and goes on to say, ‘I would think that everyone has to be friendly’. John says that he would like to see efforts to introduce a fast track for the diagnosis and treatment of dementia, similar to the fast track that has been introduced for cancer treatment. Joan chips in, saying that even if a lot is being done for people with dementia, it is not enough. The discussion continues as the term ‘dementia-friendly’ is discussed, and the group quickly agrees that the phrase is hard to define. Everyone agrees, though, that friendliness is generally a good thing.
The challenges faced by participants when attempting to describe dementia-friendliness may also indicate the general limitations that are inherent when asking people to describe a concept that largely leaves room for interpretation. One male spouse of an individual with dementia (Edward) referred to dementia-friendliness as a ‘fluffy concept’. When asked about the meaning of the term dementia-friendliness, a woman diagnosed with dementia and her husband responded: Wife: Well, I don’t know, really … I suppose … it means … I don’t know. (Vera) Husband: It can be many things. It can be something you have, which is kind of important to the individual, I suppose. And dementia-friendliness can also be the conditions you meet after [receiving the diagnosis], such as here at [name of day centre]. (Robert)
These quotes illustrate the participants’ doubts concerning the definition of dementia-friendliness. The husband emphasised one’s own experience of what is important and one’s interactions with one’s surroundings, which represent the discursive expressions of dementia-friendliness in dual reference to both individual and social meanings. Other participants expressed similar views when they spoke about visiting the drop-in centre.
In addition to the overall difficulties verbalising the meaning of dementia-friendliness, some participants dissociated themselves from the term itself, as exemplified by the following quote from a female spouse of an individual with dementia. The use of the word ‘label’ indicated that she found the term to be stigmatising: I actually think it’s an ugly word [laughs]. I actually think so because it’s like putting a label on that person. And you must be dementia-friendly, but I don’t know how … what other words to use to describe it … I think you’re sticking a label on that person. Like, now you need to take note of them – that sort of thing. I don’t like it. I can’t tell you why exactly. But I don’t like it. I suppose I take it very … that it’s a handicap. Which it is, really … Really. But I agree the idea behind it is good. The idea is good, I suppose, and I do think that it’s important that you accept that these people have a handicap and that they should receive help. Now I sound such a contrarian [laughs]. (Sarah)
The construct of dementia-friendliness appears to be open to individual and social interpretation and meaning-making. The following analysis shows how the participants construct dementia-friendliness by drawing on other discourses.
Sameness discourse
The sameness discourse was identified in the textual analysis, and the observed discursive practices framed the participants’ statements about meeting their peers and an ongoing discursive negotiation of the identity of being a person living with dementia. A male participant who was diagnosed with dementia explicitly connected the term dementia-friendly with being a drop-in centre user: ‘Why, dementia-friendly, that’s when we can meet at [name of drop-in centre] ...’ (John).
A woman with dementia emphasised the importance of the centre as a place to meet peers: ‘Knowing there’s a place I can go and talk to people in a similar situation – that means a lot. And having that café, I think it’s so nice. I really do’ (Joan).
A male spouse of an individual with dementia said that the dementia clinic had advised them to contact the drop-in centre immediately after his wife received the diagnosis. When they started visiting the centre, they were initially placed into different groups: one for people with dementia and another for relatives. He explained: Being with … er, you might say … for my wife, as the one who has dementia, I sensed that she felt secure when she was with them because ‘they’re just like me,’ you know? She could allow herself to be stupid [indicating quotation marks], she could afford to be forgetful without being embarrassed because the others did the same. For me, it was nice to meet other relatives in the same situation. We were able to talk about things that I couldn’t discuss with other people, and I’d say … I suppose that has been the biggest help for me. (Edward)
A woman with dementia similarly draws on a security and care discourse when discussing her neighbourhood, in which people are aware of her diagnosis: Yes, everyone in [name of suburb]. We’re almost natives here, aren’t we? They are aware that I have that illness. Yes, they do. You know, it means that I believe that people are attentive to me in such a closed community that we live in, aren’t they? Nice and safe, it really is. Absolutely. (Joan)
The participants stressed the feelings of security that they derived from knowing that their community was aware of their situation. The quote from Joan also appears to indicate an expectation that the environment will be attentive to people with dementia, thus supporting the individual’s feelings of belonging and security and the sense that they are cared for by the community.
The sameness discourse also appeared in discussions regarding whether the establishment of designated areas for people living with dementia, such as dementia villages, could be considered dementia-friendly. However, the connotations held by people living with dementia appeared to differ from those held by their families. Although many people living with dementia appeared to doubt the dementia-friendliness of grouping people with dementia, their relatives all expressed support for the idea. The differences expressed primarily concerned whether individuals with dementia should live together in a designated area or whether they should live in the community at large.
The daughter of a woman with dementia expressed her enthusiasm for the planned dementia village. Comparing the village to a commune, she supported the idea of grouping people with dementia: Why, I do think that would be ideal – rather than … because, otherwise, they would just sit in their own homes. But really, they’re cooped up in each their own places, aren’t they? Just sitting there. Where you might say that you could almost see it as a commune, right? … And right; then, they’d be with others who have dementia – and so what? I don’t know what it is, but there’s been this idea that you weren’t supposed to hide them away and that kind of thing; but, on the other hand, for whose sake? Who should we be taking care of here? Because, you know, the person with dementia would be just fine with a safe framework – a place where not too much is going on. (Emily)
The quote from Emily illustrates how a person with dementia was viewed as someone who would benefit from being with others in the same situation. Furthermore, the reference to people with dementia as ‘them’ and as someone who cannot be hidden out of sight uses language that represents individuals with dementia as a group of people who need to be acted upon. When negotiating the social identity of an individual diagnosed with dementia, this type of language might indicate an us-versus-them dichotomy between people with dementia and people who are unaffected by dementia.
Across the interviews, the dementia-diagnosed individuals also appeared to use language that represented a similar negotiation regarding their social identities as people living with dementia. When a woman with dementia expressed her dislike of living among other people with dementia, she appeared to be modifying her definition of a person with dementia, so that it did not apply to herself: So … on the upside, I’d say that that would be a town within the town, wouldn’t it? So, it would be good for those who may live with dementia. But I couldn’t see myself in a place like that. Er … for me, that is – with the condition I am in today – for me, I think that … well, how can I put it? I think that … er … But why would we establish communities like that, where everyone is the same? Really, I don’t care for that. I really don’t.… You know, I enjoy being out and about; but it’s for the diversity rather than being only with the demented, the carers and all that. That’s not for me. (Joan)
By questioning the establishment of dementia villages, the quote from Joan also illustrates the discursive battle surrounding people with dementia and whether they should live together in designated villages or within the community at large. Joan appeared to acknowledge her diagnosis when referring to ‘the condition I am in’. However, the use of ‘the demented’, which in general is a stigmatising terminology (The Dementia Engagement and Empowerment Project, 2014), together with her indication of not desiring to live together with other people with dementia, could be seen as distancing from others living with dementia. Similar views were expressed by another female participant with dementia. She also voiced her concerns about grouping people with dementia in a village: I’m not sure you should crowd such people like that. I’m … I’m … I’m a bit in doubt about that … In any case, it would have to be a place where you could get help … with the things you can’t manage yourself.… Because there’s many things you can’t do yourself. (Sophie)
Using the phrase ‘such people’, Sophie appeared to dissociate herself from others with dementia. Her reference to people with dementia as people in need of help due to declining abilities constitutes a negotiation of the social identity of people with dementia and their ability to manage life without help. The excerpt below from field notes taken at the day centre shows how gathering people with dementia caused situations in which language, both verbal and nonverbal, implied the ongoing negotiation of identity among various individuals with a dementia diagnosis. Ninety-year-old Paul visits the day centre three times a week. Paul appears well-dressed and trim. His dementia diagnosis causes symptoms that include impaired impulse control and sense of situation. He likes to sing the same drinking song and occasionally makes verbal attacks, such as telling people to ‘Shut up’. We [the centre users, a carer, and I] are sitting at the dinner table for afternoon coffee. Peter [another centre user] is sipping from his coffee when Paul looks at him and starts singing. ‘So he leans back his head and beholds the bottom of his glass, thinking back on the days of his youth that he’ll never see again’ (stressing ‘see’). [A carer] tries to stop him by saying, ‘It’s too early, Paul’. Smiling, Paul looks at Steve [another centre user] for a little while and says, ‘Yes … there is something to be said for everything’, to which Steve answers, ‘Yes, but it’s not everything there is something to be said for’. ‘You and I do know that’, Paul says. ‘Absolutely’, says Steve, smiling. Sitting across from me, Vera says to Paul, ‘Oh, shut up’. Rolling her eyes, she looks at me and says with a laugh, ‘He reminds me of an inebriated uncle’.
This excerpt exemplifies how the identity of a person living with dementia is negotiated by individuals with dementia. On one hand, Vera compares Paul’s behaviour with that of a drunken uncle. On the other hand, Steve’s relationship with Paul appears friendlier, contrasting with and differing from that between Paul and Vera. However, we see that Paul’s behaviour prompts some kind of reaction from both Steve and Vera. The deprecating and belittling remarks aimed at Paul and his behaviour indicated that Paul seemed close to crossing the line of acceptable behaviour at the day centre.
One of the male participants with dementia compared dementia villages with general dementia-friendly trends in society: But I think it’s a really good idea … I really do. Because shared living has become the thing to do, and this is what it is, isn’t it? I think so, at least … you know, people keeping a bit of an eye on each other. (Peter)
The use of the phrase ‘keeping an eye on each other’ may indicate the view that dementia villages offer an attractive means through which individuals with dementia can care for each other. By emphasising the need for individuals with dementia to keep an eye on one another, Peter appears to discursively construct individuals with dementia as people in need of being managed.
At the core of the sameness discourse, we identified a negotiation of what it means to be a person with dementia. The negotiation, whether by those living with dementia or their families, reveals a discursive battle between opposing values regarding whether a person with dementia should be viewed as someone who can care for themselves or as someone who needs to be acted upon. Furthermore, the participants’ construction of dementia-friendliness and life in a designated area, such as a dementia village, highlighted a major challenge faced by the goals of dementia-friendliness in general, which is the balance between the inclusion and exclusion of people with dementia.
Security and care discourse
Expressions associated with a security and care discourse primarily reflected the influence of the physical environment on the feelings of security among people with dementia and their relatives. Similar to the statement associated with the sameness discourse, a discursive battle was observed in the statements associated with the security and care discourse. The battle primarily concerned whether people with dementia should live in designated areas, such as dementia villages, or in the community at large.
Speaking of dementia-friendliness, the daughter of a woman with dementia connected the discussion to the ideas of ‘freedom’ and ‘feeling secure’ among those living with dementia. I think that [the dementia village] is a fantastic idea. Because I think the area they can move in – it must be bounded because, what that actually means, is to give them the freedom to … er … be in a place where one actually … where one feels secure. (Emily)
By emphasising the presence of a physical delimitation as a means for providing people with dementia with a sense of freedom and security, Emily appeared to assume that the physical environment would protect an individual with dementia and compensate for the loss of competences and control.
A male participant living with dementia also emphasised a feeling of security and homeliness when speaking about dementia-friendliness, and he spoke in favour of dementia villages as bounded areas and the possibility of moving to one at an early stage of dementia. Using words, such as ‘homely’ and ‘secure’, he associated dementia-friendliness with opportunities to performing his daily activities: Well, I think it’s a really, really good idea, having such a dementia village, where … er … many of the things we do in our daily life – you can go on doing them inside that area, and I believe that’s a really, really good thing.… It would also mean that if you move there some time earlier and do some of the things and activities in the dementia village – you know what I mean – that would make you feel a bit more at home and secure. (Eric)
A female spouse of an individual with dementia also mentioned security and freedom as being associated with dementia-friendliness. However, she also expressed her concerns regarding people with dementia living in a designated area and the delimitation between people with dementia and the general population. I think it’s a good idea. That is, if the way it’s done is … they will have a village of their own, and they can feel secure there but, nevertheless, have the freedom to – if I understand it correctly – to go shopping and … so that they have their freedom and are not locked up inside, if you follow me. So, I think it’s a good thing. It’s a good initiative … I gather it’ll be fenced in. That would be the only minus, as I see it. But it’s hard to tell what the effects will be. I really can’t imagine it.… That’s really the only thing I worry about, that aspect. It will be … you know … it’ll be a small, closed community, if you can put it that way. I believe that would be the only minus, the way I look at it. But I still believe that the plusses outweigh the other things. (Jessica)
The use of contrasting words, such as ‘freedom’ and ‘locked up’, showed Jessica’s ambivalent feelings in regard to encroaching on the rights of people with dementia to remain autonomous and independent.
One of the male participants with dementia made a nuanced comment similar to the quote from Jessica. Emphasising the closed nature of a dementia village as a beneficial aspect for those living with more advanced stages of dementia, he opposed the idea of ‘being comfortable’ when ‘locked up’ for those living with milder forms of dementia. If you are deeply affected and can’t find your way around the place, then it’s fine, and those who are doing fairly … I’ll take my own example, again, as someone who is able to drive a car and find my way around … er … I would not be comfortable about being locked up, to put it bluntly, would I? (Steven)
Comparing himself with people living with advanced-stage dementia, he accepted the need to establish an isolated area for those living with advanced dementia and discursively constructed people with dementia at more advanced stages as people in need of care.
Expressions concerning whether people with dementia are able to care for themselves or are in need of being cared for within the security and care discourse also exemplified the ongoing negotiation of the social identity of a person with dementia. The participants’ contrasting statements regarding people with dementia living in a closed, designated area or in the community at large, combined with the ambivalence with which the participants appeared to connect the issue of designated living areas with dementia-friendliness and the dementia-friendly values of freedom and feeling secure and well-cared-for illustrate this ongoing negotiation.
Autonomy discourse
Throughout the interviews and conversations, the autonomy discourse reflected underlying values concerning independence and the exercise of free will. The participants with dementia primarily expressed this discourse through their use of words such as ‘independence’ and ‘collaboration’. These inherent values were challenged by their relatives, however.
Below, we present an excerpt from field notes recorded at the day centre. The excerpt exemplifies the health professional’s dilemma between doing the right thing and causing harm in a situation in which another person’s autonomy is at stake. We have just checked in. The day centre manager, a staff member, and I are discussing the day’s programme. It is Thursday, and the Thursday dance is on the schedule. The manager advises us to pay attention to two of the day centre users; a male and female. They had danced very closely at last week’s dance, she says. ‘At one point, he had his hands inside her blouse’. One of the other staff members had observed this and found it a bit too much but did not intervene. The manager says, ‘They are grown-ups, so I won’t interfere. I’ve been thinking whether I should ask them to go to another room’. The manager says it is a difficult issue. The staff member chips in, and they discuss the balance between self- and co-determination, and when it is appropriate to interfere.
This excerpt illustrates a dilemma related to the autonomy and exercise of free will among individuals with dementia. A similar dilemma became evident in a statement from the daughter of a woman with dementia regarding whether forcing her mother to participate in activities would be considered dementia-friendly, while simultaneously indicating that she favoured taking over the responsibility. Er … and besides, actually, her memory. Much of it has gone – but then, at other times, there are things that she does remember. And then, you’d have to admit that there is this thing about her going to the day centre … but that was one place my mother surely wasn’t going. She was not going to be with those old people.… ‘Yes, Mum, you are going to the day centre.’ Is that what it is, dementia-friendliness – my forcing my mother to go? ... But if she says no to whatever else you suggest, I suppose we’ll have to do it. (Emily)
A male participant with dementia spoke about being independent and his freedom of movement. He somehow acknowledged others’ rights to interfere in his life: Then I’d say that I’m happy that I have my freedom of movement, so to speak, because … er... I was diagnosed with it [Alzheimer’s]. But … er ... there are some things that I can’t do, but then there are many other things that I can do…. Yes, and they also let me drive my car, you know. They haven’t taken that away from me. (John)
Adding nuance to the autonomy discourse, another male participant with dementia mentioned the power aspect: Actually, I think I’ve got it here. I do. I wrote it down at home… I believe I wrote something about power, you know. There is an aspect of power in this thing, which, which ... er … that also goes for the town, if you can put it that way.… But some of it, you know, first and foremost, I think, it is dementia-friendly if it avoids controlling too much, that is. In any case, if nothing else, there should be some kind of collaboration.… But … but this thing about ‘friendly’, you know – I think it can be a bit condescending. (Peter)
By emphasising ‘avoids controlling’ and ‘some kind of collaboration’, the participant challenged the idea that others should be entitled to interfere and control his life.
Another male diagnosed with dementia described how he managed to maintain his freedom of movement and independence. [B]ecause I don’t want to have to depend on others. I have … there’s a couple of times they’ve said that I didn’t … for example, I went missing and couldn’t find my way home, and there was one night I’d been gone for most of the time, you know, so … And then they say … er … ‘No, my dear. Now we can’t allow you to leave on your own anymore – we’ll be driving you.’ And I say, ‘No, I can’t accept that.’ And then we found this GPS thing. (Eric)
Eric also stressed the importance of being able to decide when to move away from home. The time when I move away from home … that would be, you know, when I’m unable to do anything at all, right? And that’s not … this here dementia village thing, I [with emphasis] can say … so I can say to my family, ‘You know what, now it’s becoming too hard for me. I’d like to go live there.’ And they can also come to me and say – my family – they can say to me, ‘[Name]… er … don’t you think this is becoming too much, all this? What would you think about moving over there?’ And we’ve discussed that – that it will be my decision when it’s time. (Eric)
Even though Eric imagined himself eventually living in a dementia village and acknowledged that his condition would deteriorate with the progression of the illness, he held on to his autonomy and the decision to determine when it would be time to move.
When asked about his view of dementia-friendliness, another male informant emphasised the advantages of staying in the village in which he lived: Well, you know … I’d put it this way – I think, in my situation, you know, living down in [name of suburb], I’d … you know, if I had to choose, I’d rather go on living here.… the way it is … you might say that the old culture of … of when … actually, when you live in the countryside, you take care of each other. (Peter)
When negotiating the situation of making important decisions about moving or staying in his own home, the participant referred to ‘my situation’. Although the culture of taking care of each other is presumably valued by all citizens in his village, his appreciation of this aspect of the culture somewhat underscores the importance of the environment for those living with dementia and their need to feel included among the community.
The autonomy discourse, similar to the sameness and the security and care discourses, revealed differing perspectives on autonomy and inherent values.
Autonomy fundamentally concerns values of independence, the exercise of free will, freedom of movement and participation in decision-making. Although primarily challenged by their relatives, these values were also questioned to some degree by the people with dementia. This self-contradictory position was largely centred on the limits of the autonomy of the person living with dementia and the situations in which other people were entitled to interfere with and take over responsibility for their lives.
Discussion
This study explored how people with dementia and their families discursively construct dementia-friendliness by drawing on the discourses of sameness, security and care, and autonomy. Our analysis demonstrated the challenges met when attempting to define dementia-friendliness. We observed how the construction of dementia-friendliness serves as an arena for individual interpretation, ambivalence and discursive battles.
Social identity construction in a person with dementia: A discursive battle
The discourses discussed here demonstrated the ongoing negotiations that occur regarding the social identity of being a person with dementia and the implications of this identity for the lives of these individuals. The identified negotiations and discursive battle tended to centre around whether individuals with dementia are capable of caring for themselves or whether they require others to manage them. The outcomes of these discussions could have repercussions on the emergence and development of dementia-friendliness in society and amongst individuals. Additionally, our understanding of whether and how well existing dementia-friendly initiatives actually meet the needs of people with dementia remains unclear.
The discursive battles surrounding the negotiation of social identity among people with dementia may also explain the battles concerning whether to group people with dementia. The discussions and societal trends associated with the inclusion or exclusion of people with dementia have been described by international organisations (World Health Organization, 2017; World Health Organization & Alzheimer’s Disease International, 2012), patient organisations (Green & Lakey, 2013) and researchers (Shakespeare et al., 2019; Swaffer, 2014; Thomas & Milligan, 2018), also similar themes were identified in the participants’ discursive construction of dementia-friendliness. These discussions regarding dementia-friendliness primarily focus on whether people with dementia should live in a designated area, such as a dementia village, or in the community at large, corroborating findings in a study of how professionals working within dementia care and dementia-friendly projects construct dementia-friendliness (Hansen, Præstegaard, et al., 2021). The families of individuals living with dementia appeared to largely favour the idea of people with dementia living in designated areas, emphasising the similarities among people with dementia and the use of limited physical surroundings as a means for providing a feeling of safety and security for both the individuals with dementia and their relatives. Although some of the participants with dementia stressed the importance of meeting with peers at the day centre or drop-in centre, they resisted the idea of living with others diagnosed with dementia, emphasising the value of meeting people who were unaffected by dementia and the underlying values of feeling free and autonomous.
Our analysis also indicated an us-versus-them dichotomy in the negotiations and discursive battles concerning the social identity of a person with dementia. This dichotomy may be ascribed to both historical and societal changes (Fairclough, 1993; Nedlund & Nordh, 2018). A review of the literature shows that the characterisation of people with dementia has shifted from purely focussing on the biomedical aspects of dementia to including a focus on their rights and resources, resulting in descriptions of people living with dementia that increasingly acknowledge them as persons who not only need care but also desire being viewed as active citizens with resources and individual rights (Alzheimer’s Disease International, 2019; de Vugt & Dröes, 2017; Mitchell et al., 2013; Nedlund & Nordh, 2018; Swaffer, 2014; Thomas & Milligan, 2018; Zeilig, 2015). However, the discursive battles surrounding the identity of people living with dementia appear to interfere with how dementia-friendliness is constructed and established. In general, the participants in this study connected values such as autonomy, security and safety with dementia-friendliness. However, they appeared to do so from differing perspectives. The relatives of individuals with dementia associated these values with a designated area, such as a dementia village, whereas the people living with dementia connect these values with living in the community at large.
Linking independence with autonomy, the participants living with dementia emphasised the importance of supportive physical and social environments to compensate for their diminishing capabilities to maintain their everyday lives. Research has shown that people with dementia are ready to accept their dependence on others in exchange for the maintenance of autonomy (Smebye et al., 2016). The realisation that they will eventually become dependent on others as the disease progresses could explain their formulations regarding the ‘natural’, inherent legality of interference in their decisions.
The relatives of individuals with dementia also referred to inherent legality in relatively explicit terms. As dementia progresses, the legality of interference in the lives of people with dementia by relatives and other caretakers appears to increase, although no clear boundaries have been established. These difficulties were especially apparent when relatives described family members living with dementia as having the right to exercise their own free will, to a limited extent.
Dementia-friendliness: A stigmatising concept?
Some participants were explicit in taking exception to the idea of ‘dementia-friendliness’, associating it with a shift in power and the negative labelling of people with dementia. People with dementia and their families frequently experience stigma (Alzheimer’s Disease International, 2019a; Batsch & Mittelman, 2012; Swaffer, 2014; World Health Organization, 2017). According to sociologists Link and Phelan, stigma occurs ‘when elements of labelling, stereotyping, separation, status loss, and discrimination co-occur in a power situation’ (Link & Phelan, 2001, p. 367). Stigmatising and distancing language is often used not only by groups unaffected by dementia but also among people with dementia, who use such language to describe other people with dementia. The words used to describe people with dementia might indicate stigmatising processes or reflect methods used to construct otherness, which unfolds when they compare themselves with others living with dementia, drawing attention to differences in their symptoms and associated functional decline. Thus, although people with dementia emphasise the importance of meeting with their peers, they also attempt to dissociate themselves from others with dementia. As described by the social anthropologist Marianne Gullestad, ‘sameness’ refers to processes in which people with dementia and their families ‘consider themselves as more or less the same in order to feel of equal value’ (2002, p. 46). The feeling of sameness depends on others’ recognition of one’s identity. If this recognition is absent, the result may be avoidance and, ultimately, exclusion (Gullestad, 2002). This negotiation appears to occur bilaterally, establishing sameness between oneself and others while simultaneously maintaining distance by highlighting differences (Gullestad, 2002).
Constructing dementia-friendliness
The construction of dementia-friendliness is another discursive battlefield. The participants themselves can exert their influence on the discursive negotiations surrounding dementia-friendliness. For those participants with mild-to-moderate Alzheimer’s disease, as well as for some of their relatives, a future life in a designated dementia village may be difficult to conceptualise. The promotion of dementia-friendliness and dementia-friendly villages has numerous aims, including the improving the everyday lives of people with dementia, informing society in general and fostering inclusiveness towards people with dementia (Alzheimer’s Disease International, 2015; 2016; 2017; Crampton & Eley, 2013; Green & Lakey, 2013; Hebert & Scales, 2017; Lin, 2017; Shannon et al., 2019; Williamson, 2016; World Health Organization, 2017; World Health Organization & Alzheimer’s Disease International, 2012). When constructing dementia-friendliness, the participants in this study drew on sameness discourses to formulate elements of importance to themselves, including meeting and being with their peers, experiencing a secure and caring environment, the influence of the environment on the experiences of autonomy and security, and the feeling of being independent and exercising one’s free will. As interpreted by Fairclough, this could be viewed as the discourses from one social domain infusing those of others (Fairclough, 2013), which might explain the ambivalence expressed within the participants’ construction of dementia-friendliness. Their emphasis on the values of importance to themselves indicated a mix of discourses that derived from the various settings in which the participants encountered the notions of dementia and dementia-friendliness, such as the media (Harvey & Brookes, 2019; Van Beveren et al., 2020) or social policies (Nedlund & Nordh, 2018). These mixed discourses may also explain the discursive battles that surround dementia-friendliness, further contributing to the development of an us-versus-them dichotomy.
Therefore, although people with dementia and their families are the prime targets of dementia-friendly initiatives (Shannon et al., 2019), our analysis demonstrated that dementia-friendliness and the associated discourses represent a precarious tightrope walk between the inclusion and exclusion of people with dementia from the larger community.
Limitations
A study sample of 10 individuals with dementia and six relatives of individuals with dementia provides no guarantee of maximum variation. However, the variations in sociodemographic characteristics among our sample, including sex, age, and marital status, compensates for the limited sample population. The extensive fieldwork performed during this study further strengthens the validity of the findings and their interpretations.
Although only one child (an adult daughter) of an individual with dementia participated in this study, her contribution to the discursive construction of dementia-friendliness lent nuance by demonstrating the dilemmas experienced by the relatives of people with dementia.
The difficulty associated with gaining access to people with dementia and obtaining their consent to participate may have influenced the results. However, people with dementia are the target group for the development of dementia-friendly initiatives. Although their cognitive abilities and levels of abstraction are affected by their condition, people with dementia live the experience of dementia; therefore, their perspectives are necessary to understand the experience of dementia and how best to focus our efforts to alleviate the challenges associated with living with dementia. Dementia-friendliness aims to increase general knowledge regarding the experience of living with dementia to foster a sense of inclusiveness for people with dementia. Therefore, although the study did not include individuals at more advanced stages of dementia, our results are likely to benefit all people living with dementia
Conclusions
This study has demonstrated the discursive construction of dementia-friendliness among people who live with dementia and their relatives. This analysis revealed that dementia-friendliness is a construct that is open to highly individual interpretations and serves as an arena for ambivalence and discursive battles. We demonstrated the difficulties encountered by people with dementia and their families when attempting to construct dementia-friendliness, and the participants in this study drew on three existing discourses for this construction: the sameness discourse, the security and care discourse, and the autonomy discourse. Our analysis has revealed the ongoing discursive negotiations that underlie the description of people with dementia as either a group that is able to care for themselves or as a group relying on care by others. This work contributes by enabling people with dementia and their relatives to express their views on dementia-friendliness implying their desire to be heard in the development processes related to dementia-friendly initiatives and communities. However, the attempts by authorities and families to include people with dementia in society without excluding them appears to pose a constant dilemma, which again underscores the importance of including the voices of people living with dementia when dementia-friendly initiatives and communities are developed.
Footnotes
Author contribution
All authors have contributed substantially to this paper.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Research Foundation at the Danish Occupational Therapists Association [grant number FF2-R69-A1566] and the Research Foundation at the Danish Alzheimer’s Association [grant number 181003].