
Abstract
Introduction
Pain of nursing homes residents with Alzheimer’s disease remains under detected compared to their cognitively intact counterparts. Communication difficulties may partly explain this poor quality of care but the influence of stigmatization on pain assessment has never been explored.
Research question
The objective of this research was to analyze whether a diagnosis label of Alzheimer’s disease or the stage of the disease may bias pain assessment scores and empathic reactions of health care staff in nursing homes.
Methods
Two studies were conducted based on a similar experimental between-subjects design with a video showing an older adult woman experiencing undefined pain. Different labels and vignettes were manipulated to characterize the subject of the video. In the first study, 84 certified nursing assistants were asked to watch the video and then to assess the pain intensity and their empathic reaction. Participants were randomized in two conditions that varied the disease label (Alzheimer’s disease vs no diagnosis). In the second study, 67 certified nursing assistants were enrolled who did not participate in the first study. They watched the same video as in the first study and assessed the pain intensity and their empathic reaction. They were randomized in two conditions that varied the stage of the Alzheimer’s disease (mild stage vs severe stage).
Results
Alzheimer’s disease label had no influence on assessment scores. In contrast, the stage of the disease had a significant effect on the health care staff assessments with severe stage associated with lower pain intensity scores and empathic reactions.
Conclusion
These results confirm that the Alzheimer’s disease stigma is a real phenomenon that tends to be mainly elicited by the symptoms of the acute phase of the disease. These findings are crucial to better understand the stigma related to Alzheimer’s disease and to enhance the pain management of this frail population.
Introduction
Pain is a common problem in people with dementia and represents a core aspect of treatment and care (Corbett et al., 2014). Nevertheless, the quality of pain management concerning this population remains suboptimal (Agit et al., 2018; Domenichiello & Ramsden, 2019). This issue is patent in nursing homes where it has been estimated that 50% of the residents with dementia experience pain on a regular basis (Björk et al., 2016; Corbett et al., 2012; Knopp-Sihota et al., 2019; Van Kooten et al., 2017) with detrimental consequences on their physical and psychological wellbeing (Rostad et al., 2017). Studies report a deterioration of physical and cognitive ability, in addition to increased risk of falls, appetite disturbance, and sleeping disorders (Corbett et al., 2014; Van Dam et al., 2019). Pain may also trigger or worsen neuropsychiatric symptoms, such as agitation and aggression (Husebo et al., 2014; Van Dalen-Kok et al., 2015). Despite an increasing awareness of institutions and staff, residents with dementia are at greater risk for inadequate pain management. Indeed, compared to their cognitively intact counterparts, their pain experience is less often assessed (Nakashima et al., 2019; Tan et al., 2015) and they generally receive fewer analgesics (Griffioen et al., 2017; Tan et al., 2015). However, people with dementia are equally susceptible to painful conditions and there is no scientific evidence that their pain experience is altered by the neurodegenerative process (Gagliese et al., 2017). The basic justification for these pain management inequalities is the difficulty that cognitively impaired individuals have communicating about their pain experience (Lichtner et al., 2014). Challenging behaviors such as agitation and aggression may be considered as attempts to communicate their pain. But these signs are generally misinterpreted as consequences of the neurodegenerative process and treated with psychotropic medication that confer risks to the patient and do not address the pain (Pergolizzi et al., 2019).
Observational tools have been developed to address these difficulties but their adequate use requires specific conditions (training, multidisciplinary team rating, and regular reassessments) that are scarcely ever met in practice (Husebo et al., 2016). Moreover, they rely on a linear and controlled conception of the assessment process rather than acknowledging the prevalence of more intuitive subconscious approaches to judgement and decision making (Dowding et al., 2016).
In long term care facilities, certified nursing assistants are in the front line to detect if a resident with dementia is experiencing pain but they receive little training in pain assessment (Cervo et al., 2012; De Witt Jansen et al., 2017; Liu, 2014). Several guidelines have been provided to improve pain management in older people (Hadjistavropoulos et al., 2014; Zwakhalen et al., 2018). However, these recommendations have difficulty being circulated and put into practice in long term care facilities due to organizational constraints and lack of prioritization. Thus, pain assessment is not performed routinely by health care staff and they may not follow, or even be aware of, these pain management guidelines (Husebo et al., 2016; Zwakhalen et al., 2018).
Interestingly, some conceptual research explored further sources of these care inequalities and focused on the dementia diagnosis that may overshadow the personality and needs of the person who is only seen through the lens of his illness (Dupuis et al., 2012; Malloy & Hadjistavropoulos, 2004). An experimental study confirmed that the dementia diagnosis associated with negative beliefs about the personhood of the people with dementia have the potential to influence care practice, including decisions about pain management (Hunter et al., 2013). More specifically, in this study, healthcare providers were more likely to recommend anxiolytic versus analgesic medication for an individual who displayed pain-related behaviors if he or she had dementia. The objective of this latter study was to operationalize Kitwood’s theory about the influence of the perception of the staff about “personhood” of the person with dementia on intended care (Kitwood & Bredin, 1992). However, as the study manipulated the diagnosis label, its results may also be discussed in the scope of the stigmatization process related to dementia.
Is dementia a stigmatized condition?
Stigmatization has been described as a social cognitive process that comprises four stages (Link & Phelan, 2001). Stigmatization of an individual occurs when that individual is (1) labeled, (2) negatively stereotyped, (3) discriminated against, and (4) experiences status loss as a result of the stigma. Dementia and its most common diagnosis Alzheimer’s disease (AD) have been widely recognized as stigmatized conditions but are scarcely the specific target of research in the area of stigma (Nguyen & Li, 2020). Our knowledge on the subject mainly relies on the literature about mental health stigma even though the processes and determinants may differ in some ways, given that dementia diagnoses do not elicit the same kind of emotional and cognitive attributions (Corrigan, 2007; Corrigan et al., 2003; Link et al., 1989; Werner et al., 2010, 2011). Indeed, a review by Werner (2014) summarized the negative consequences of the stigmatization process related to AD that may occur at the individual level (low self-esteem, feelings of shame and humiliation, and social isolation), family level (feelings of shame, social isolation, moral failure as a family, increased burden, depression, as well as concealment and decreased use of services), professional and societal levels (differential access and use of services, etc.). Noteworthy, the stigmatization is not only endorsed by lay persons but also by healthcare providers (Mukadam & Livingston, 2012). In this later context, discrimination seems to underpin a large range of problematic behaviors like delayed diagnoses, exclusion of the decision-making process, questionable treatment decisions, increased institutionalization, coercion to restraint physically or medically, etc.
Is pain assessment susceptible to stigma?
Pain assessment tasks—where no “correct” answer is obvious—represent a clinical and experimental context where indicators of bias are quite obvious (Tait & Chibnall, 2014). Indeed, the personal and subjective nature of pain has long been acknowledged. For few decades, the argument that pain is “what the person in pain says it is” has finally become a consensual watchword and self-report is now commonly considered as the “gold-standard” in the pain assessment domain (Schiavenato & Craig, 2010). Nevertheless, in clinical practice, underestimation of the patient’s pain by healthcare providers is a well-documented phenomenon suggesting that pain assessment might not solely be based on the subjective report of the patient (Prkachin et al., 2007; Seers et al., 2018). Studies on physicians and nurses have shown that personal characteristics such as seniority (Prkachin et al., 2007), empathy (Goubert et al., 2009; Green et al., 2009), and burnout (Gleichgerrcht & Decety, 2014) may influence the pain assessment ratings of the observers. A recent study that focused on certified nursing assistants in long term care facilities showed that their pain assessment scores decreased with experience and expertise (Vitou et al., 2021). Studies about the influence of the observers’ sex and age in a care context are scarce and show inconsistent results (Gingras et al., 2021; Ruben et al., 2018).
The complex nature of the pain assessment process has been conceptualized through several theoretical models (Craig, 2009; Gagliese et al., 2017; Hadjistavropoulos & Craig, 2002; Hadjistavropoulos et al., 2011; Prkachin et al., 2007; Schiavenato & Craig, 2010; Snow, O’Malley, et al., 2004). For example, Schiavenato and Craig (2010) described pain assessment process as a transaction that encompasses the person in pain (called “the patient” in the model) and the health practitioner. First, contributing factors are the foundation of the transaction: they form the personal and social contexts that impact both stakeholders. These contributing factors include either biological, sociocultural, psychological, experience, or contextual/situational determinants. Second, the assessment process itself is represented as a feedback loop composed of five stages that starts with the pain stimulus, and travels from the patient (pain experience and expression) to the clinician, whose judgment and intervention (or lack thereof) directly affect the patient’s pain experience. The whole process is considered as “successful” when patient and clinician reach a high level of consensus regarding to the meaning of the pain experience of the patient. According to this model, either patient- and clinician-related contributing factors mediate all the steps of the assessment process and significantly contribute to its success or failure.
Furthermore, some authors underline that, in absence of medical evidence, the variability of pain judgement follows the patterns consistent with models of social judgement (De Ruddere et al., 2013; Tait, 2013). Indeed, the uncertainty inherent to the pain assessment situation leaves the observer free to project onto the person in pain its attitudes, beliefs, opinions, making clinical judgement exposed to the influence of stereotyping (Tait & Chibnall, 2014). The activation of stereotypes may advantage individuals who fit positive stereotypes and disadvantage individuals who do not by eliciting stigmatization and thus discrimination in pain assessment. This statement has been operationalized in the scope of stigmatized illness like HIV, obesity, chronic pain where studies showed that underestimation and/or undertreatment of pain might be the consequences of this deleterious process (Azevedo et al., 2014; De Ruddere & Craig, 2016; Decety et al., 2010). But to the best of our knowledge, the impact of dementia related stigma on pain assessment has not been investigated yet.
Diagnosis label, disease stage… what is the most stigmatizing?
In the area of mental illness stigma, studies have tried to untangle the specific roles of the diagnosis label and other information related to the disease in the stigma process. But the topic is still open to debate. Several works have underlined the stigmatizing role of psychiatric diseases labels and their exacerbating effect on the course of the person’s disorder (Corrigan, 2007; Link et al., 1989). In the field of dementia or AD, studies revealed that the diagnosis label tends to elicit sympathy, that information about symptoms may decrease stigmatizing attitudes or have no effect and that the severity of the disease may have an influence on the stigma level (Cheng et al., 2011; Wadley & Haley, 2001; Werner, 2005, 2007; Werner & Giveon, 2008; Zhang & Cheng, 2019). Furthermore, a study addressing potential negative consequences of early diagnosis suggested that the AD label itself may not elicit stigma, but rather, the label association with expectations of certain future decline (Johnson et al., 2015).
Knowledge gap
Research on discriminatory behavior in care practice towards people with dementia is scarce. So far, studies were mainly concerned with structural consequences (delayed diagnosis, increased institutionalization) or general intentions (coercion to restraint physically or medically, treatment decision) (Herrmann et al., 2018). Moreover, these studies mostly provide results based on declarative measures which reliability may be questioned given their sensitivity to social desirability bias (Kane et al., 2020). It is also noteworthy that, to the best of our knowledge, no research about stigma outcomes related to dementia has ever focused on pain assessment by the nursing homes staff.
The current study
Given that context, our research question was to determine if the pain assessment process of institutionalized people with AD by certified nursing assistants may undergo the influence of stigmatization. The AD diagnosis was singled out as it accounts for 60–80% of the dementia cases (Rosin et al., 2020), and as such, it dominates public representation (Rizzi et al., 2014). Based on the modified labeling theory (Link & Phelan, 2001) and on previous studies on the influence of stigma on pain assessment (Azevedo et al., 2014; De Ruddere & Craig, 2016; Decety et al., 2010), we designed an experimental vignette/label protocol to manipulate different disease conditions. A unique video stimulus, validated as displaying a standard painful situation of the daily care practice of certified nursing assistants (Vitou et al., 2021), was proposed in order to control sources of bias related to the assessed person and the assessment context. Pain was assessed using two complementary measures: a visual analog scale (VAS) to collect the subjective clinical impression of the observer (Apinis et al., 2014) and then a structured observational tool, the Algoplus, recommended for the assessment of older people with communication difficulties, to provide a more objective evaluation (Rat et al., 2014). The affective reaction of the observer was also measured as it is considered to be a related but independent dimension of the empathy for pain process (Giummarra et al., 2015).
Operationally, the objectives of our study were to explore, whether the diagnosis label of AD (study 1) or information about the stage of the disease (study 2) would infer with pain assessment behaviors of health care staff in nursing homes. Our hypotheses were that (1) the diagnosis label would have a positive impact on assessment scores whereas (2) the severity of the disease would be related to lower assessment scores.
Material and method study 1 and study 2
Participants
Two independent convenience samples of female certified nursing assistants working in nursing homes have been formed: 84 were enrolled for study 1 (aged 21–62 years) and 67 for study 2 (aged 19–64 years). They were recruited in nineteen nursing homes in three regions of France (Grenoble, Lille, and Montpellier) through flyers posted in staff break areas and a verbal presentation by the researchers during team meetings.
As more than 90% of the certified nursing assistants in French nursing homes are female (French national institute for statistical and economic studies, 2020), only female certified nursing assistants were selected in order to avoid gender bias in pain assessment. The eligibility criteria were to be 18 years old, French speaking and to be willing to voluntarily participate in the study. Women with self-reported history of neurological or psychiatric illness were excluded. No compensation was provided.
Material
Demographics and professional characteristics
In both studies, age, educational attainment, occupational status, and current or past chronic pain experiences were recorded. Professional characteristics such as duration of experience in geriatric care and in the actual position, pain assessment training during their education or professional courses and prior use of the observational pain assessment tool used in this study (Algoplus) were also collected.
Video clip
In both studies, a unique 15-second video clip trial was presented to the participants. This video consisted of an older female actress who mimic undefined pain while standing up from a deep chair with the help of another person. The actress was recruited in the researchers’ entourage. She was 80 years old at the time she was videotaped and lived alone in the community. The video clip (see Supplementary Online Material) was conceived to display a typical day-to-day care situation without any specific emotional features. It displayed no blood, no wound, no sign susceptible to elicit disgust or physical discomfort. The video has been validated in a prior study as representing a standard painful situation experienced by an older adult woman with an inconspicuous cognitive status (Vitou et al., 2021).
In study 1 (see Figure 1), introducing the video clip, an information label appeared in full screen for 5 seconds in white text on black background. Two versions of the information label were created: (1) “Jeanine, 80 years old” (no diagnosis condition); (2) “Jeanine, 80 years old, with Alzheimer’s disease” (diagnosis condition). Participants were randomized to either condition. Experimental design of the label and video presentations (study 1).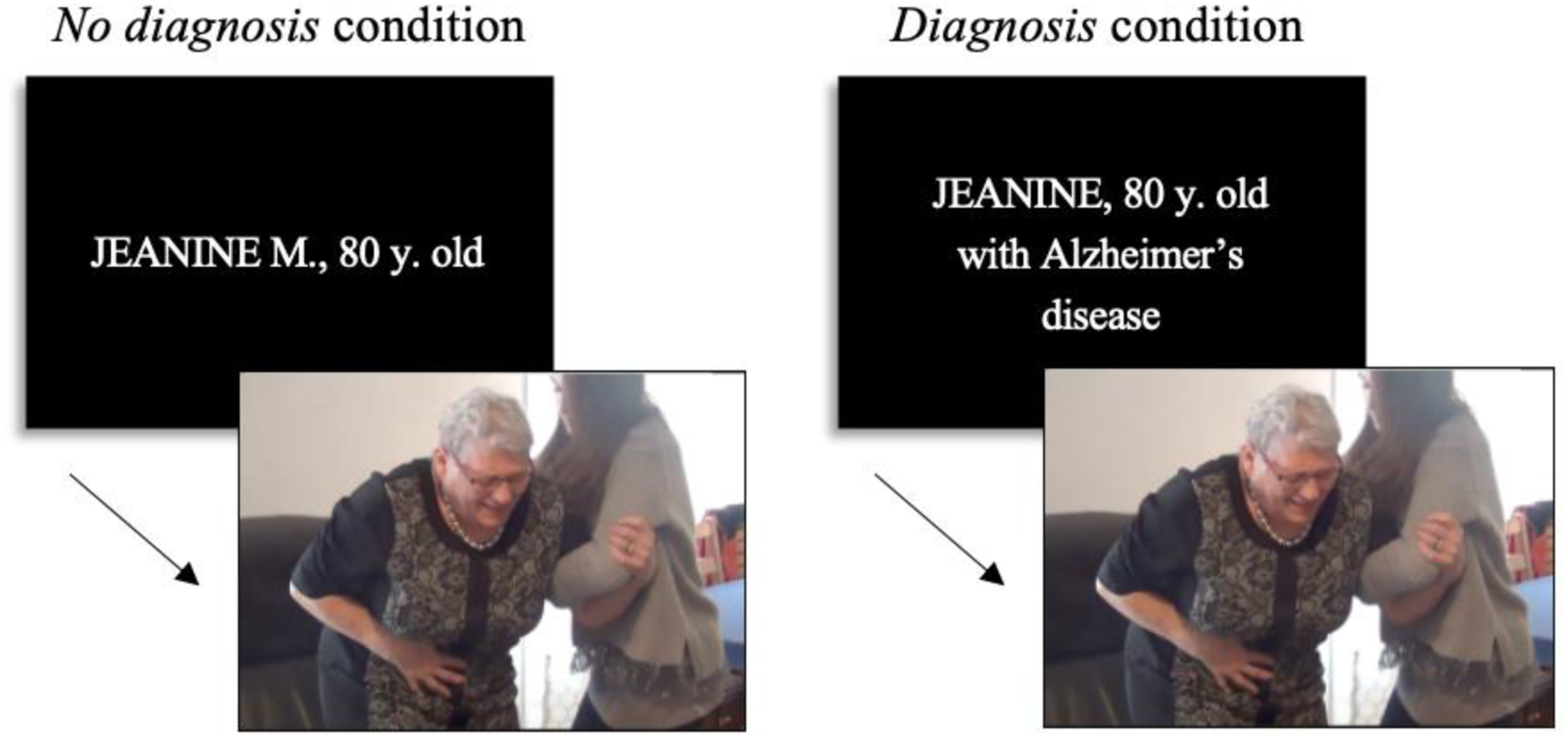
In study 2 (see Figure 2), before watching the video clip with a unique label “Jeanine, 80 years old, with Alzheimer’s disease,” participants were invited to read aloud a vignette. Two vignettes were created to describe the stage of the Alzheimer’s disease experienced by the older adult woman in the video clip. The descriptions were based on the items of the Clinical Dementia Rating Scale (Hughes et al., 1982) and included each of CDR’s six domains: memory, orientation, judgment and problem-solving, community affairs, homes and hobbies, and personal care. The first vignette (mild condition) presented symptoms corresponding to the mild stage in the CDR scale (see Appendix A). The second vignette (severe condition) presented symptoms corresponding to the severe stage in the CDR scale (see Appendix B). The face validity of the vignettes was evaluated in a pretest procedure by nursing homes professionals that were not taking part in the studies (physicians, certified nurses, psychologists, and other paramedical staff, except certified nursing assistants, N = 25). The first vignette (mild condition) was assigned to the mild or moderate stage of dementia by 23 of these professionals when the second vignette (severe condition) was assigned to the severe stage of dementia by 20 of them. Experimental design of the vignette, label, and video presentations (study 2).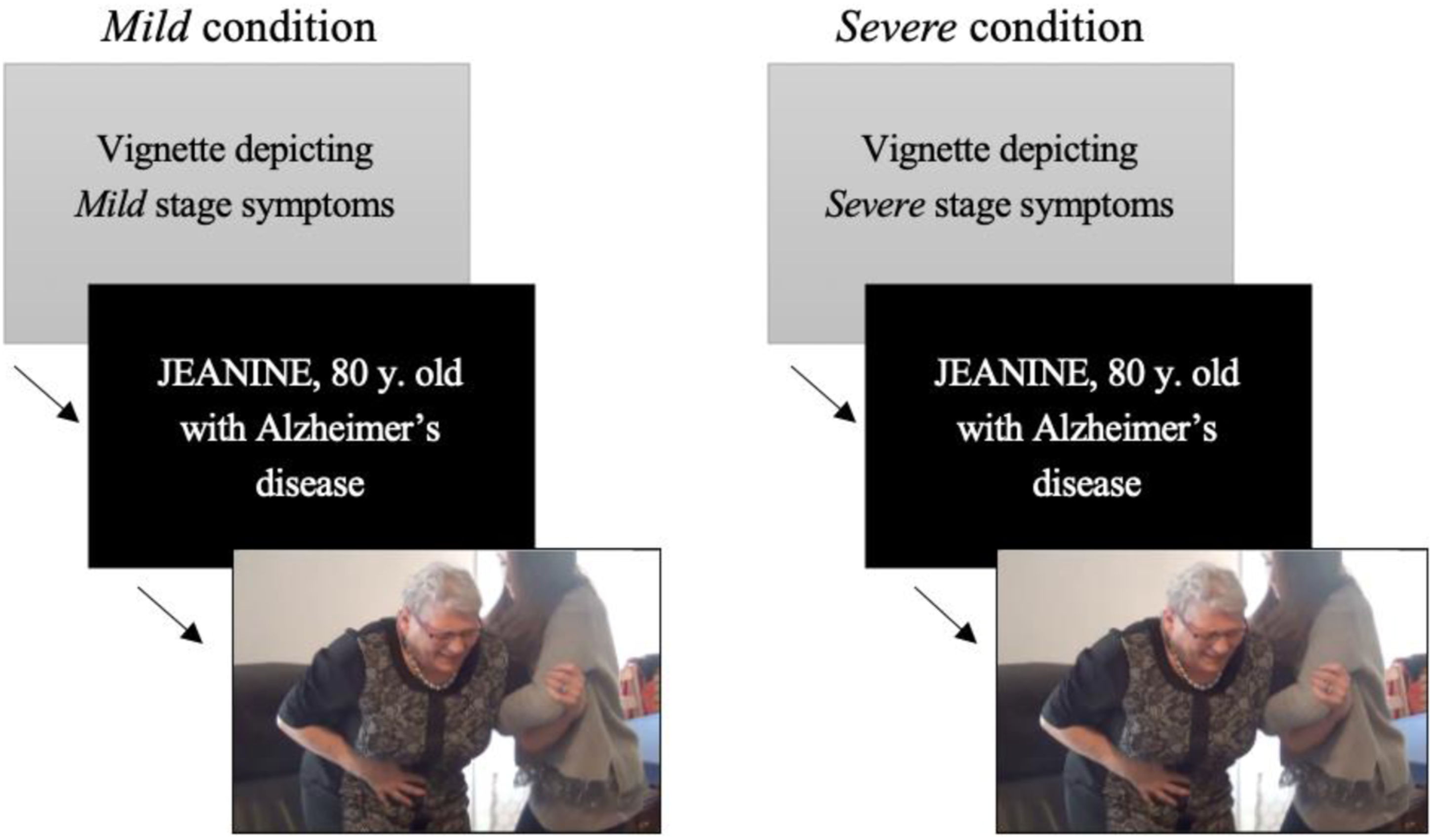
Participants of the current study were randomized to either condition (mild condition vs severe condition).
Pain and empathy for pain assessment
In both studies, after taking part in either of the conditions, participants completed the following scales.
Subjective assessment measures
Visual analog scales (VASs): VAS consisted in two horizontal lines 100 mm in length, with semantic anchors at each end points (score range = 0–100). The first VAS intended to evaluate the intensity of pain the person in the video clip was experiencing (Pain intensity VAS: left = no pain, right = worst possible pain). The second VAS was designed to rate their empathic reaction and more specifically the level of affective distress the participant was experiencing watching the video (Observer’s affective distress VAS: left = no affective distress, right = extreme affective distress). Additionally, in study 2, a third VAS was used to rate the level of affective distress the participant thought the person in the video clip was experiencing (Jeanine’s affective distress VAS: left = no affective distress, right = extreme affective distress).
Objective pain rating
Algoplus: The Algoplus is a French validated observational scale for acute and chronic pain assessment in older persons with communication disorders (Martin et al., 2016; Rat et al., 2011). It consists of five items (facial expression, look, complaints, body position, and atypical behavior); each item is scored “yes” = 1 or “no” = 0. The existence of one behavior in each item is enough to tick “yes.” Each item ticked “yes” gives one point, for a total maximal score of 5. A score greater than 2 or equal suggests the presence of pain and thereafter initiation of an analgesic treatment.
Questionnaires
In both studies, the participants were asked to fill in the following questionnaires in order to anticipate potential covariates related to psychological traits or conditions.
The Interpersonal Reactivity Index—shortened French version (IRI—Braun et al, 2015) is adapted from the 28-item initial scale (Davis, 1980). It offers a measure of trait empathy (also called dispositional empathy) that comprises four subscales: perspective taking (predisposition to assume the psychological outlook of another person), fantasy scale (tendency to imagine oneself in the place of characters in books, movies, and plays), empathic concern (ability to feel sympathy and compassion for another), and personal distress (the extent to which an individual feels anxiety as a result of witnessing another’s emotional distress). The IRI was not designed to provide a global empathy score but specific dimensions of a multidimensional construct (Davis, 1983). Empathic concern and personal distress are considered two independent measures of emotional empathy focusing on the other- and self- oriented set of feelings elicited by an agent. Perspective taking, instead, is a measure of the cognitive aspect of empathy. The use of the fantasy subscale of the IRI has been questioned as a core component of the construct of empathy (Baldner & McGinley, 2014). First, considering the IRI is not designed to provide a global empathy score (Davis, 1983; Yu & Kirk, 2009), the IRI subscales can be used separately (Duarte et al., 2016). Moreover, Hunt et al. (2019), Duarte et al., (2016) and Tei et al., (2014) excluded the fantasy subscale from the IRI in their studies of healthcarers empathy, and Gleichgerrcht and Decety (2014) excluded the fantasy subscale from their study of physicians, as being not relevant. Relying on these arguments, we decided to exclude the fantasy subscale of our analyzes.
The Personhood in Dementia Questionnaire (PDQ—Hunter et al., 2013) is a 20-item self-report questionnaire that measures beliefs of nursing homes staff about personhood in dementia. Participants are asked to rate their agreement level with the questionnaire’s statements using 5-point scales ranging from 1 (disagree strongly) to 5 (agree strongly). A high total score indicates strong positive beliefs about personhood in dementia.
The Maslach Burnout Inventory (MBI—Dion & Tessier, 1994) is a 22-item self-report questionnaire that measures the frequency of perceived burnout among professionals, especially in the field of care. Participants are asked to rate using 7-point scales, how frequently they had a variety of feelings and experiences in their jobs (0 = never to 6 = every day). Maslach Burnout Inventory evaluates three independent dimensions: emotional exhaustion, depersonalization, and personal accomplishment. Burnout was defined by high scores on either emotional exhaustion (≥30), and/or depersonalization (≥12). The personal accomplishment dimension was not included in this study, given that this dimension is generally criticized and not used in the literature (Blanchard et al., 2010).
The Hamilton Anxiety and Depression Scale (HADS—Zigmond & Snaith, 1983) is a 14-item scale with two subscales, measuring anxiety and depression, in a 4-point (0–3) Likert scale. Scores for each subscale range from 0 to 21. Scores of 8 and above indicate presence of depression or anxiety symptoms. The use of the total score is recommended to differentiate individuals with or without distress in a general population (Mitchell et al., 2010).
Procedure
The research was conducted in accordance with the Declaration of Helsinki (World Medical Association, 2013) and was approved by the competent ethics committee of the Paul Valéry University. All participants were recruited on a volunteer basis and were free to interrupt their participation at any time without giving any reason and without any prejudice. After a complete description of the study, they filled in a written informed consent where it was specified that the data will be anonymized and only used in a consolidated way for research purpose.
In both studies, certified nursing assistants were encountered in their workplace. Demographics of the participants were collected during face-to-face interviews conducted by five trained final year students in psychology, supervised by the researchers.
After this interview, in both studies, participants were instructed that they would see a short video clip in which a person goes from sitting to standing and that they will have to complete various scales and questionnaires. The VAS were described with their specific semantic anchors (no pain/worst possible pain; no distress/extreme affective distress). Concerning the use of the Algoplus scale, the participants of both groups were given the following instruction: “Did you observe the following expressions of pain in this person? Yes or No” and were informed of the standard instructions (i.e., “the simple observation of a behavior mandates that it be checked as present, regardless of any etiological interpretation or the duration of its existence”).
The video clip was then presented in full screen with a high sound level.
In study 1, participants were randomly showed the videoclip introduced by the label corresponding to the no diagnosis or diagnosis condition (see Figure 1).
In study 2, before viewing the video clip, the participants were randomly asked to read aloud either the vignette corresponding to the mild or severe condition (see Figure 2).
Afterwards, in both studies, participants completed the pain and empathic reaction measurement scales (VAS, Algoplus) and the questionnaires (HADS, IRI, MBI, and PDQ).
At the end of the procedure, an individual debriefing time was proposed to the participants in case of challenging emotional reaction. No participant expressed a need for it.
Statistical analysis
All statistical analyses were performed with IBM SPSS software version 24.0, with a 2-tailed α level of 5%. Data were tested for homogeneity of variance using the Levene test. No normal distribution was considered when absolute values for skewness and kurtosis were greater than 3 and 10, respectively (Weston & Gore, 2006). For normally distributed data, parametric tests were used (Student’s t-test, analysis of variance, and Greenhouse-Geisser adjusted degrees of freedom). For non-continuous or non-normally distributed data, non-parametric tests were used (Mann–Whitney U-test). To examine whether pain assessment rated on the VAS varied between conditions (study 1: no diagnosis vs diagnosis conditions; study 2: mild vs severe conditions) and their nature, multivariate analyses of variance (MANOVA) were performed with condition as between-subject factor and VAS type as the within-subject factor. A simple contrast analysis has been conducted. The Chi-square test was performed for categorical variables. In addition, we calculated the eta squared η2 and the Cohen’s d’ as measures of the effect size. The effect size was considered small (η2 = 0.01; d’ = 0.2), medium (η2 = 0.06; d’ = 0.50), or large (η2 = 0.14; d’ = 0.80) according to Cohen (1988). Relationships between our variables of interest were explored with Pearson or Spearman coefficients. According to Cohen (1988), a correlation between 0.10 and 0.30 represents a small effect, between 0.30 and 0.50 a medium effect, and above 0.50 a large effect.
Results study 1: Diagnosis label influence on pain assessment
Participants’ characteristics
No significant difference was found between participants of both groups (no diagnosis vs diagnosis) concerning demographics, socio-professional characteristics, and psychological measures (see Supplement Table S1 in supplementary material). In both groups, there was no significant correlations between the age of the participants and the variables of interest (VAS, Algoplus).
Pain intensity and empathic reaction assessments
On the whole sample (N = 84), the two VAS scores fell within acceptable normality ranges. Their distributions were wide spread and characterized by high variability (pain intensity VAS: M = 64.44, SD = 18.28; affective distress VAS: M = 50.68, SD = 27.02). Similar patterns of distribution were observed in both diagnosis label conditions. The Algoplus scores distribution were also wide spread (Mdn = 3; range = 1–5).
As shown in Figure 3, a significant main effect of VAS type (i.e., pain intensity and affective distress) was observed with a large effect size (F = 29.09, p < 0.001, η2 = 0.262). Participants had lower scores on the affective distress VAS compared to pain intensity VAS. There was no significant main effect of the diagnosis label for VAS scores (F = 3.65, p > 0.05). The interaction effect between diagnosis label and VAS type was not significant (F = 2.34, p > 0.05). Finally, no diagnosis label effect was observed for the Algoplus scores (U = 762.00, z = −0.835, p = 0.40). Pain intensity and observer’s affective distress VAS for the no diagnosis and diagnosis groups (study 1).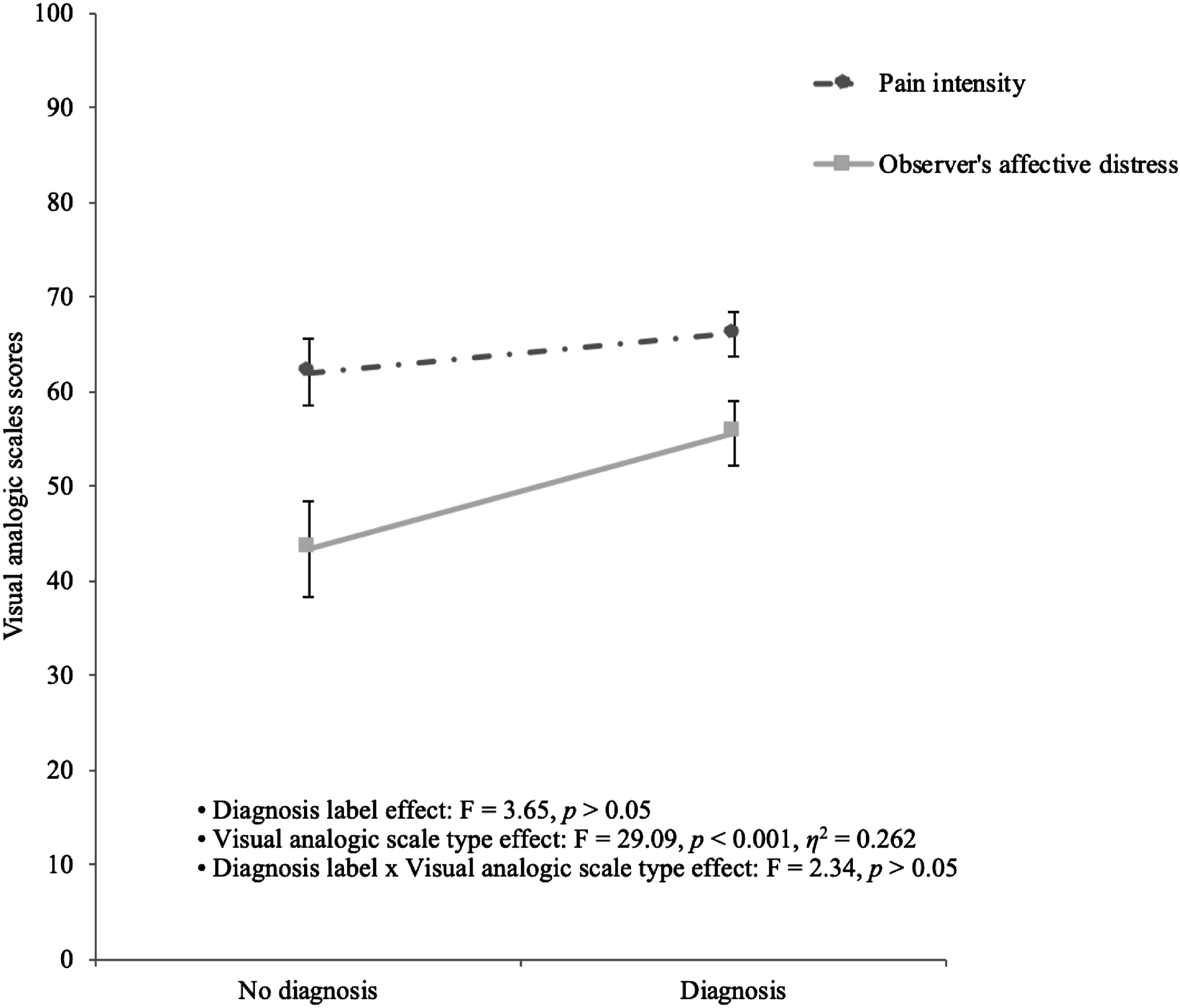
Nevertheless, focusing on the affective distress VAS scores, a significant difference was found between the two diagnosis label conditions. Participants of the no diagnosis label condition displayed less affective distress than those of the diagnosis label condition (t (82) = −2.09, p < 0.05).
Results study 2: Stage of the disease influence on pain assessment
Participants’ characteristics
No significant difference was found between “disease stage” groups concerning demographics, socioprofessional characteristics, and psychological measures (see Supplement Table S2 in supplementary material), except for the “empathic concern” dimension of the IRI (t (60) = 2.15, p = 0.03) with a small-sized effect (r = 0.27). In both groups, there were no significant correlations between the age of the participants and the variables of interest (VAS, Algoplus).
Pain intensity and empathic reactions scores
On the whole sample (N = 67), the three VAS scores fell within acceptable normality ranges. Their distributions were wide spread and characterized by high variability (pain intensity VAS: M = 63.04, SD = 17.98; observer’s affective distress VAS: M = 52.48, SD = 30.15; Jeanine’s affective distress: M = 70.81, SD = 19.07). Similar patterns of distribution were observed in both disease stage conditions. The Algoplus scores distribution was also wide spread (Mdn = 3; range: 1–5).
No disease stage effect was observed for the Algoplus scores (U = 527.00, z = −0.44, p = 0.66).
The results of the 2 (disease stage) × 3 (VAS type) MANOVA with pain and empathy for pain assessment measures as dependent variables are illustrated in Figure 4. There was a significant disease stage effect for the VAS scores with a medium-to-large effect size after controlling the effect of the “empathic concern” dimension of the IRI (F = 17.45, p < 0.005, η2 = 0.13). As shown in Figure 4, participants of the mild condition had globally higher assessment scores (pain intensity: M = 69.68, SD = 16.11; observer’s affective distress: M = 59.41, SD = 29.95; Jeanine’s affective distress: M = 79.24, SD = 15.14) compared with the severe condition (pain intensity: M = 55.60, SD = 17.58; observer’s affective distress: M = 48.13, SD = 28.99; Jeanine’s affective distress: M = 63.00, SD = 19.44). Pain intensity, observer’s affective distress, and estimated sufferer’s affective distress VAS for the mild and severe condition groups (study 2).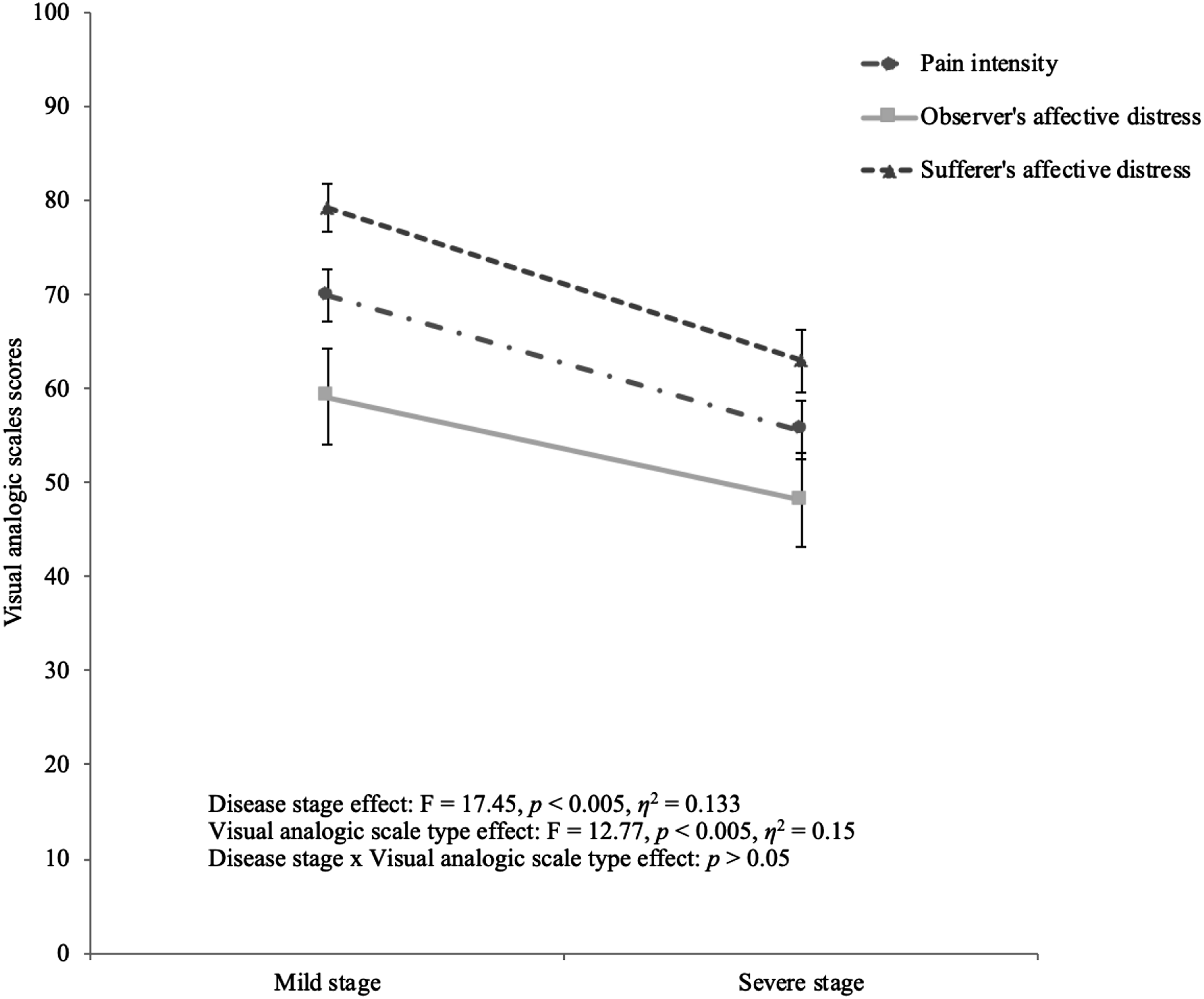
There was also a significant large-sized effect of the VAS type (F = 12.77, p < 0.005, η2 = 0.15). Contrast analyses revealed that participants had lower scores on the observer’s affective distress VAS compared to pain intensity (p < 0.001) and Jeanine’s affective distress scales (p < 0.001). No significant difference was found between the pain intensity and Jeanine’s affective distress VAS (p = 0.09).
The interaction between disease stage condition and VAS effects was not significant (p = 0.33).
Relation between dependent variables and association with the questionnaires scores
In the mild condition, the pain intensity VAS and Jeanine’s affective distress VAS scores were moderately and positively related (r = 0.40). The observer’s affective distress VAS and the empathic concern dimension of the IRI were moderately and positively related (r = 0.43). No other relation was found.
In the severe condition, the pain intensity VAS and the observer’s affective distress VAS were strongly and positively related (r = 0.65) and both were moderately to strongly negatively correlated with the personal distress dimension of the IRI (respectively, r = −0.67 and, r = −0.43). Jeanine’s affective distress VAS scores and the PDQ total scores were strongly and positively related (r = 0.55). No other relation was found.
Discussion
The objective of this study was to analyze the influence of AD related stigma on pain assessment behaviors of certified nursing assistants in nursing homes by manipulating the diagnosis label (study 1) and description about the stage of the disease (study 2). The interest of studying the stigma associated with AD through the evaluation of pain is two-fold. First, participants’ answers are less likely to suffer the desirability bias compared to self-report attitudes questionnaires (Tait & Chibnall, 2014) especially in an inter-subject design. Second, the focus is made on a crucial issue in dementia care. Thus, the results of this research are both theoretical and clinical.
The main findings of this study were that the information about the presence of the AD diagnosis did not impact the pain assessment behaviors and empathic reactions of the certified nursing assistants. Contrariwise, the stage of the disease had an important impact on the participants’ assessment behaviors. Indeed, the participants assigned less pain intensity and affective distress to the person in pain when she was described as severely ill. The participants also displayed less empathic reaction in this condition.
This results contradict the basis statements of the most popular stigma research in the field of mental illness (Corrigan, 2007; Link et al., 1989) which claim that stereotypes may arise as soon as the diagnosis label is disclosed. But they confirmed and refined results of Johnson et al’s. (2015) study which focused on the stigmatization process in the context of early diagnosis strategies of AD. In their protocol, based on labels manipulation and declarative measures, it was not the AD diagnosis itself that elicits stigma but, instead, the expectations of worsening impairments. The authors argued that the evolution of the disease model, due to new diagnosis techniques, expanded the AD spectrum from a stage where there is a complete absence of observable cognitive or behavioral symptoms, to later stages marked by behavioral changes, loss of awareness, and difficulty with activities of daily living. Indeed, the AD representation has shifted from a terminal to a chronic condition (Rosin et al., 2020; Stites et al., 2018). Thus, it may create a new way of how to react to persons diagnosed with AD and diagnosis label alone may not automatically conveys stereotypes of the most severe form of the disease.
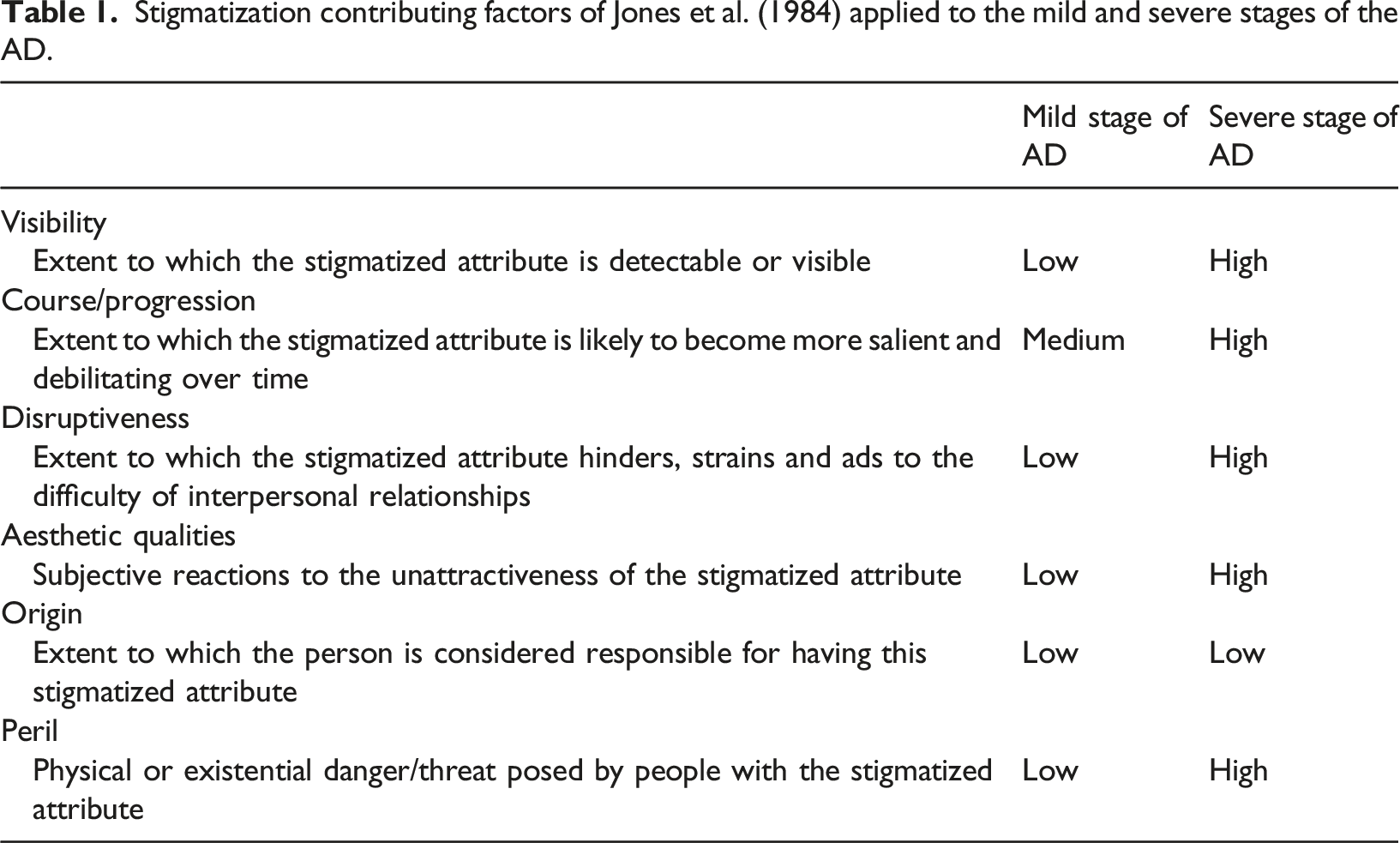
Stigmatization contributing factors of Jones et al. (1984) applied to the mild and severe stages of the AD.
Another sobering result of this study is that certified nursing assistants in nursing homes who are constantly in contact with people with AD are clearly endorsing stigma about the disease and displaying discriminating attitudes and behaviors in their care practice. It may come as a surprise as personal contact is deemed to be one of the most efficient ways to prevent the stigmatization process to unfold (Mukadam & Livingston, 2012). But, this phenomenon has already been observed in many healthcare professions dealing with dementia (Gove et al., 2016; Piver et al., 2013; Shinan-Altman et al., 2014; Werner, 2007; Werner & Giveon, 2008) and may be seen as a consequence of the type of contact they have with the people with AD. Indeed, these professionals are often interacting with people with AD when they are at the acute stage of the illness (Corrigan, 2007); namely, when their level of dependence or their behavioral disorders prevent them to stay at home. The illness perception of certified nursing assistants in nursing homes may therefore be biased by their work environment. It is also noteworthy that caring for people living with dementia at a severe stage of the disease is often challenging and represents a significant risk factor of burnout (Kandelman et al., 2018; Narme, 2018). Thus stigmatizing beliefs of the staff may be related to their level of burnout (Kane et al., 2020; Mantzorou et al., 2020). This association has not been found in our study, but it may depend on the type of beliefs that have been focused on.
The relationship between stigmatizing beliefs and pain treatment decisions of health care staff in the context of advanced dementia has been explored in a previous study (Hunter et al., 2013). Their results showed that the more negative the beliefs of the participants were about personhood of people with AD status, the more likely they were to recommend anxiolytic treatments to reduce pain-related behaviors in people in pain described as having AD. Thus, the stigmatization process may elicit discrimination in care practice through misdiagnosis and mistreatment of pain. This phenomenon is supported by a descriptive longitudinal study which shows a clear association between pain and antipsychotic use in individuals with dementia (Rajkumar et al., 2017). Our research brings further elements by showing that the stigmatization process may not only influence the pain treatment decision but also the evaluative step of the pain management procedure leading to lower assessment scores. These findings are consistent with the main argument of Hunter et al. (2013) who related this discriminatory behaviors to the dehumanization process of people with Alzheimer’s disease, who gradually lose their individual status in the eyes of others and are no longer considered “subjects” of their own painful experience (Kitwood & Bredin, 1992; Malloy & Hadjistavropoulos, 2004). Our additional analyses corroborated this explanation since in the severe stage condition, the estimation of the older adult woman’s affective distress by the certified nursing assistants was no longer related to the intensity of pain (as in the mild stage condition) but, instead, with participant’s personal beliefs about personhood in dementia (PDQ scores). The more negative the beliefs were, the lower the level of emotional distress attributed to the person with AD in pain.
Our additional analyses gave also potential clues about the role of affective empathic disposition in the context of pain assessment of people with AD. In the mild stage condition, the pain intensity assessments of the participants were driven by the comprehension of other’s emotion (Jeanine’s affective distress) and their ability to feel compassion for another (empathic concern dimension of the IRI) while in the severe stage condition the pain intensity assessments of the participants were more driven by self-oriented emotions and negatively related to the personal distress score of the IRI. These findings are in line with a recent research study (Starr & Magan, 2020) that promote a model of empathic pain assessment for people with dementia. The authors argued that for the self-oriented clinician, observing pain may produce emotions such as distress or fear, which may prompt behaviors (e.g., denial of pain severity) to avoid unpleasant emotions associated with pain. Conversely, for other-oriented clinicians, observing pain may rouse emotional resonance leading to a desire to relieve pain through treatment that links to the behavioral response of pain treatment. Moreover, authors acknowledged that such orientation (self or other) may be influenced by bias (Starr & Magan, 2020). Surprisingly, no relation was found in our study between pain assessment and cognitive empathy (perspective taking dimension of the IRI) as if, in the context of dementia, affective reactions were hindering cognitive appraisal of pain. Further research may be conducted to test this hypothesis.
Finally, it should be noted that neither the diagnosis label nor the stage of the disease had an influence on the Algoplus scale scores. This lack of effect suggests that the use of such tool could protect pain assessment from the influence of stigma, even though stigmatizing attitudes would be present among observers. This result is consistent as this kind of observational grid is considered to be more objective than VAS or other non-standardized tools (Apinis et al., 2014). Indeed, using the Algoplus, the observer is asked to report explicit behaviors that can signal the presence of pain thus limiting the influence of subjective impression. Then, the high inter-rater variability found in the Algoplus scores in both part of this research and in previous works (Vitou et al., 2021) may more originate in the difficulty of assessing pain on the base of facial expressions than in the influence of personal beliefs and experience (Lautenbacher et al., 2013).
Limitations
Several limitations and methodological choices should be taken into consideration. Firstly, the important workload and burden of this population prevent us from recruiting a large number of participants. We decided therefore to conduct two independent studies instead of one 2 × 2 × 3 factorial design (stage of the disease condition × label condition × VAS type) to preserve statistical power of the analysis. But we are aware that this later methodology would have better fulfil our objectives. Second, we chose to recruit only female participants in order to avoid gender bias as 90% of the certified nursing assistants in French nursing homes are female, but further studies should explore the gender impact on stigmatizing attitudes in pain assessment. Third, we acknowledge that the pain intensity VAS is not a valid tool for a proxy-report of pain in people with severe dementia in a clinical context, but this tool has been chosen for analyze purpose as pain intensity VAS is a sensitive measure often used in research to explore observer’s pain assessment behaviors and bias (Prkachin et al., 2007; Seers et al., 2018). Fourth, the lack of control condition showing pain-free behavior of the older adult woman may have increased the variability of the pain assessment scores. Finally, we favored an experimental design with a video clip which may have dampened the empathic reaction of the observers. We deliberately chose to videotape an actress depicting simulated pain. This choice was based on ethical issues as vulnerable older adults with moderate-to-severe dementia are unable to provide fully informed consent. Such method has already been used in scientifically sound studies: validation of an observational assessment tool for dementia population (Snow, Weber, et al., 2004), evaluation of the ability of laypeople to use observational pain assessment tools (Ammaturo et al., 2016). Moreover, other studies have shown the inability of healthcare professionals to distinguish genuine and posed expression of pain, even with adequate training (Williams, 2002). Some facial expressions are more frequent in posed pain than in genuine pain but they are not specific (Galin & Thorn, 1993). In addition, more intense expressions may also reflect a greater pain experience (Lints-Martindale et al., 2007).
Implications and conclusion
In French nursing homes, a large majority of the residents are living with AD (or other forms of dementia) but not all have been formally diagnosed (Helmer et al., 2006). Moreover, the healthcare staff and especially the certified nursing assistants may not be aware of the diagnosis of the residents they care for (Snow, O’Malley, et al., 2004). They rather deal with the disease symptoms and their evolution. Unfortunately, as shown in our study, the stage of the disease may also be the designated stigmatization trigger. However, our findings put on the trail of solutions to support certified nursing assistants improving the detection of pain in people with dementia. Empathy may play a crucial role as it influences all the components of the clinician–patient relationship (Starr & Magan, 2020). Empathy has also been outlined as a core concept to understand stigmatization and struggle against its consequences (Álvarez-Castillo et al., 2018; Farmer & Maister, 2017; Vanman, 2016). Therefore, pain management training of certified nursing assistants may focus on empathic abilities in order to enhance awareness and interpretation of nonverbal communication and to weaken the influence of stigmatizing beliefs.
Despite international recommendations, the use of observational assessment tools in nursing homes is still low (Zwakhalen et al., 2018). Further efforts must be undertaken to promote their use in daily care practice as they guide attention to valid pain-related expressions and provide more objective assessments. The development of electronic assessment tools offers also promising perspectives for the improvement of pain management in people with dementia (Atee et al., 2017).
Future research would interestingly focus on other healthcare population (e.g., nurses, general practitioner) to acknowledge if their pain assessment and empathic reaction undergo the same biases. The same type of research protocol could also be used to study the effectiveness of anti-stigma interventions.
In conclusion, pain management in people with severe dementia is a challenging issue that needs to be manage with a global approach as it deals with experience, attitudes and behaviors of the staff. It also involves guidance of the care practice. Nursing homes organizations and training programs need to address these different topics and promote person-centered care in order to effectively improve the quality of care of people living with dementia.
Supplemental Material
Supplemental Material—The influence of Alzheimer’s disease stigma on pain assessment in older persons
Supplementary Material for The influence of Alzheimer’s disease stigma on pain assessment in older persons by Valérie Vitou, Marie-Christine Gély-Nargeot, Claude Jeandel and Sophie Bayard in Dementia
Supplemental Material
Footnotes
Author Contributions
VV: Conceptualization, Data collection and treatment, Writing—Original draft preparation. M-CG-N: Conceptualization, Supervision, Validation. CJ: Supervision, Validation. SB: Conceptualization, Data Analyzes validation, Reviewing and Editing.
Acknowledgement
The authors thank the health care professionals of the “Fondation Partage et Vie” who voluntarily participated in this study to advance scientific knowledge and improve the care of people with dementia.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was financed by the “Fondation Partage et Vie.”
Sponsor’s role
The funding source had no influence on the conduct and design of the study, neither on the data collection, analysis, the interpretation of the data, the approval of the manuscript or in the decision to submit the article for publication.
Ethical approval
The study was conducted in accordance with the Declaration of Helsinki (World Medical Association, 2013) and was approved by the ethics committee of the Paul Valéry University.
Supplemental Material
Supplemental material for this article is available online.
Appendix A: Mild stage of the disease condition vignette
Jeanine is 80 years old. She has just been diagnosed with Alzheimer’s disease. For some time now, she has been having memory problems. She may forget recent events such as what she ate for lunch or a phone call she received. Sometimes she is searching for her words or the names of people she knows. Occasionally she loses things like her wallet or keys. She has some difficulty managing her appointments. She is becoming less and less active. She often feels down because she is aware of her difficulties.
Appendix B: Severe stage of the disease condition vignette
Jeanine is 80 years old. She was diagnosed with Alzheimer’s disease five years ago. Most of the time she does not recognize her husband and children. She no longer takes part in conversations, but answers questions with a smile or a few words, which are often inappropriate. At night, she is agitated and anxious, and she asks continuously the same questions. Sometimes she becomes aggressive. She can no longer go out alone because she gets lost. She often wanders around at night. She has to be solicited and assisted to wash herself.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.