
Abstract
India is the world’s second-most populous country and there are about 5.3 million people with dementia in India. Only one out of ten people living with dementia in India ever gets a diagnosis, care or treatment. There are various obstacles to deliver dementia care and support to people living with dementia and their carers. Furthermore, there is inadequate understanding of dementia in the general public and within the health care professionals. Studies in India indicate that people with dementia experience stigmatisation in society as well as neglect from their families. Social prejudice associated with dementia makes it a challenging experience, in addition, it makes the persons with dementia and carers feel isolated and stigmatised. Focus groups and individual interviews were used to explore perceptions, beliefs and experiences of dementia across a number of stakeholders in India, with an effort to understand stigma towards people with dementia. Participants were recruited in two diverse cities of India (Chennai and Delhi), and were comprised of a range of key stakeholders, including persons with dementia (n = 8), caregivers (n = 19), health care professionals (n = 16) and the general public (n = 15). Following a thematic analysis, we identified three overachieving themes; (1) Poor awareness, (2) Stigma and (3) Barriers to accessing care. These all occurred within the context of socio-cultural beliefs. Whilst each stakeholder group had different experiences of dementia, it was common for all participant groups to use stigmatising language associated with dementia. In many cases, stigmatising beliefs and poor understanding of dementia resulted in poor care. There is an apparent need to raise awareness of dementia in India across all stakeholder groups; the fact that participants were able to self-identify that they had a lacked awareness of the condition may indicate that these groups are receptive to learning more about dementia.
Introduction
India is the second-most populous country in the world, with a total population of 1.3 billion. Approximately 104 million (8.6% of the population), are aged 60 years and above (Borah et al., 2016), with numbers expected to continue to rise significantly with increases in life expectancy. Dementia is most common among older people, with the mean age of presentation reported as 66.3 years in India (Alladi et al., 2011). Currently, it is estimated that there are 5.29 million people living with dementia (Alzheimer’s & Related Disorders Society of India [ARDSI], 2010) in the country, and is projected to rise to 7.61 million by 2030 and 14.32 million by 2050. Despite the rising burden of dementia, only 10% of people with dementia receive any care, diagnosis or treatment in many lower-middle-income countries (LMICs).
Stigma towards people with dementia is seen as universal problem, as it results in people not seeking diagnosis or support, and can leave people socially isolated (Alzheimer’s Disease International [ADI], 2019). Goffman (1963) defines stigma as ‘an attribute that is deeply discrediting’ that diminishes an individual ‘from a whole and usual person to a tainted, discounted one’ (p. 3). Further Goffman states that individuals who are stigmatised are perceived as having a ‘spoiled identity’ (Goffman, 1963, p. 3). Dudley (2000) describes stigma as stereotypes or negative outlooks credited to a person or a group of people when their characteristics or behaviours are viewed as different from or inferior to societal norms. Defined as disgrace and discredit, stigma is considered to be an unwelcome characteristic by society (Byrne, 2000). Poor awareness, misinformation and misconceptions can also contribute to stigma (Stangl et al., 2019). For example in India a large proportion of nursing home staff hold misconceptions and stigmatising beliefs about dementia (Strøm et al., 2019). Caregivers of people with dementia also had limited knowledge of dementia, having not heard of the term dementia or AD, and were unable to differentiate it from normal ageing (Shaji et al., 2003). Cultural values related with different religions emphasise the significance of family values, duties and obligations contributing to complex characteristics of Indian society and culture. Although in the last few decades there has been a growth of geriatricians in India and growing awareness of dementia is still overlooked and the concept of ageing is neglected. In India, stigma was related to psychological and behaviours challenges associated with dementia resulting in neglect and sometimes abuse of the person with dementia Cohen (1998) identified Sathiyana as ‘gone sixtyish’ term used predominantly in North India. Chinnan (childishness) in southern parts of India where people speak Malayalam (Iype et al., 2006) and Nerva Frakese (tired brain) in Konkani (Patel & Prince, 2001) are also used to refer to dementia. These local idioms highlight how the understanding of dementia is rooted socially rather than in medical pathology. These terms also reflect the healthcare gap in raising awareness and facilitating early diagnosis (Brijnath, 2014).
The overarching aim of this study was to understand attitudes and perceptions concerning people living with dementia residing in India from two diverse metropolitan cities, Delhi and Chennai. We explored views from three important, yet distinct, stakeholder groups: the general public, healthcare providers, people living with dementia and carers.
Methods
Between October 2019 and November 2019, we carried out a series of six focus group discussions across the stakeholder groups and two individual interviews with persons with dementia. To increase feasibility and comfort for participants, we also offered people with dementia an opportunity to participate via individual interviews to reduce any potential distress and improve their research experience. From both sites, one person with dementia was selected and was interviewed; their primary caregiver (spouse) was allowed to accompany them at the interviews with their consent to make them feel comfortable.
Alzheimer’s and Related Disorders Society of India (ARDSI) is a national organisation which was the primary gatekeeper in recruiting participants for the focus group discussions. ARDSI has 22 chapters spread over 22 cities providing a network of volunteers and working closely with medical professionals, running dementia services to provide care and support to families and people with dementia. The chapters are better established in some cities like in Chennai and Delhi. These chapters have been well established since 1994. Both these chapters have working memory clinics, and the board members of these chapters are associated with renowned hospitals in the respective cities. These chapters also provide services to family (unpaid carers) of person with dementias including counselling, referrals and training. In addition, the Delhi chapter has a fulltime dementia daycare centre.
Socio-demographic characteristics of participants.
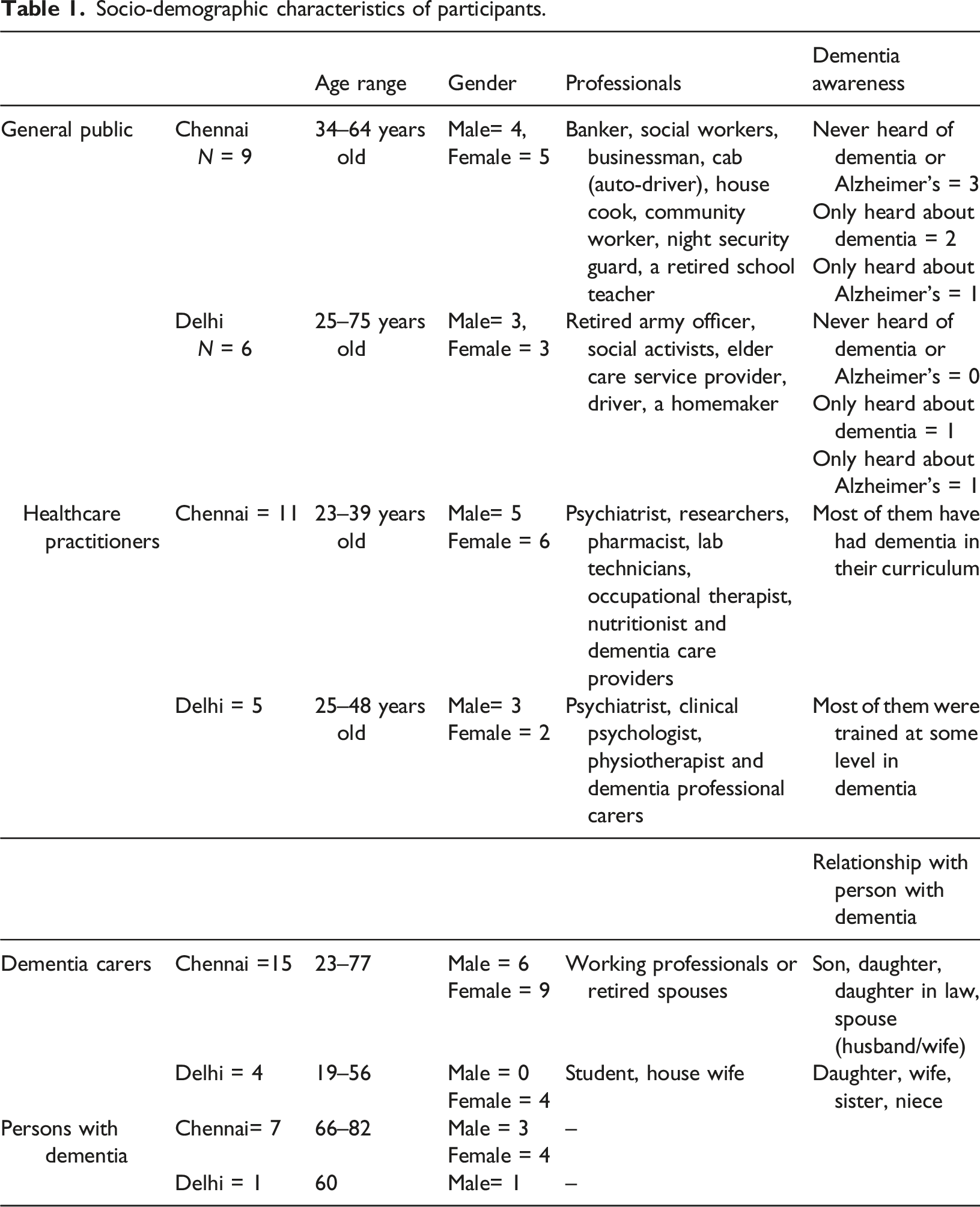
Participants
Participants were recruited separately in two metropolitan cities – Chennai and Delhi. The sites were selected due to their diversity in demographic and cultural factors. Delhi is situated in North India, whereas Chennai is the southernmost metropolitan city of India. The availability of ARDSI chapters in these cities facilitated recruitment across different participant groups, using different strategies.
General public: In Chennai, this category of general public was identified by ARDSI Chennai chapter with the aid of advertisements and word of mouth; some of the participants were recruited by local researchers as well. In Delhi, participants were recruited by the ARDSI Delhi chapter via word of mouth. All participants were required to be over the age of 18 and not formally identify themselves as having or caring for someone with dementia.
In Chennai, focus group discussions were advertised on the notice board of the Psychiatric Department at a renowned medical university associated with the ARDSI Chennai chapter. The gatekeepers at the university recruited health care professionals via word of mouth. In Delhi, participants were recruited and identified by Delhi ARDSI chapter. All the healthcare professionals recruited from this site were associated with dementia care in some way. The poster was posted in the psychiatric department of the medical hospital associated with ARDSI Chennai chapter for 10 days before the focus group discussions. This recruitment targeted mainly health care professionals working in the medical hospital. Out of the 11 healthcare professionals in Chennai, eight participants came after seeing the poster and the other three were approached via word of mouth. All people who showed interest were selected and included in the focus group discussions. The venue of the focus group discussions in Chennai was at this medical institute. In Delhi, the venue of the focus group discussions was in a meeting hall of a pre-booked public social institute, which is generally used by social researchers and organisations for meeting purposes. This venue was far from the medical hospital where the poster was displayed. In Delhi, the poster was displayed in the psychiatric department of the hospital connected to the ARDSI Delhi. ARDSI members are connected to these respective hospitals where they were able to recruit the sample. Information on the participants’ educational background was gathered.
In Chennai, persons with dementia and their caregivers were recruited by the local chapter of ARDSI Chennai and the associated medical university. The local researchers working with both these organisations recruited participants from the list of people with dementia and their caregivers who were frequent service users at these organisations. A total of 14 family carers were approached for the focus group discussion, of which eight were expected to come on the actual day of the interview, as it was anticipated that many of them might drop out due to situational reasons. In Chennai, we selected 14 caregivers and reached out to them to participate in the focus group discussions. Six caregivers responded ‘not sure’ to the focus group discussions innovation, and said they might not be able to make it on the particular day due to various reasons (e.g. the person with dementias may not cooperate, they may not have someone else to look after the person with dementia if they have to leave them back at home or some said they may have difficulty getting a transport to the venue as they have to bring the person with dementia along). However, on the day of FGD focus group discussions all 14 caregivers came and were involved in the focus group discussions. Most of the caregivers came specifically with the impression that they might learn more about dementia through these focus group discussions. This was expressed in the group discussions by participants from the caregivers’ group.
Recruitment of persons with dementia was based on identification through ARDSI data, which included careful selection of person with dementia who fit the criteria of coherence, communication and severity of dementia. Dementia severity was assessed through the medical professional assigned at the ARDSI Chapter. As part of recruitment at both sites, challenges were faced to identify a person with dementia in early stages who could understand and respond to the interview questions, as most of the persons with dementia were in moderate to severe stages. This also reflects the delayed diagnosis or approach to seek healthcare support in the later stages of the condition.
Some ethical issues that were observed at the time of recruitment of persons with dementia was that capacity of consent from the person with dementia seemed to be uncertain. Consent from the person with dementia was sought and in the case that the person with dementia was unable to provide informed consent (this was judged by the research team, which consisted of a dementia psychologist), proxy consent was taken from the family member that accompanied them. During the interviews with people with dementia, the caregiver was present (Chandra et al., 2021).
Procedure
Eventually, all caregivers who were approached attended the focus group discussions. Along with their family members with dementia and other family carers, in total this resulted in 21 participants (please refer Table 1). SH, MP and RN conducted the focus group discussions who had experience working with persons with dementia. The team was very conscious of the possible needs of all participants. Prior to the discussion, basic instructions were given to the group such as only one person to talk at a time and other to wait for their turn, to keep phones on silent whereas they were allowed to take calls outside the hall, they were informed and cued for restrooms and were told that they are free to walk out of the hall in middle of the discussion if needed. One person from the team (SH) moderated the group, whilst MP and RN being more familiar with the local language and culture facilitated the discussions. The group was given a break after an hour for 15 min where they were served coffee and refreshments. The local gatekeeper sat outside the hall throughout the discussion in case there is any need for support, for example like a person with dementia getting restless.
In Delhi, participants were recruited through ARDSI Delhi chapter gatekeepers. For both the sites, the inclusion criteria were (1) Persons with dementia with a confirmed diagnosis; (2) Persons with mild to moderate dementia, who were able to communicate and engage with the research activities. There was no formal cognitive testing; (3) Primary caregiver of persons with dementia should be aged 18 and above. Paid carers were excluded from the study.
Information sheets were provided to potential participants and informed consent was obtained. Socio-demographic characteristics (e.g. gender, age, profession) and knowledge about the terms ‘Alzheimer’s Disease’ and ‘dementia’ were collected prior to interviews collected through a questionnaire. The facilitator introduced the focus group discussion (or interview) and set the ground rules. Topic guides were tailored for each of the stakeholder groups. The types of questions asked in the focus group discussions are reported in the topic guide in the Supplementary Document. On average, the focus group discussions lasted between 40 and 60 min, whereas the large group of carers and people with dementia lasted for over 2 h with a break in between. In Chennai, the focus group discussions were conducted primarily in Tamil, whilst in Delhi they were predominantly in Hindi. Across both sites, English was intermittently used based on the comfort and preference of participants. The study aimed to conduct one individual interview with the person with dementia in each site, with the set of questionnaires that was developed for this study and adapted for persons with dementia (please refer to Supplementary Document for the questionnaires). At the ARDSI Delhi chapter only one person with dementia was recruited through purposive selection method for the requirement of person with dementia with mild to moderate stage, cognitive and communication abilities to be coherent for the interview. At Chennai chapter, the other persons with dementia were not selected, as they were either in severe stages or were unable to communicate for the individual interview.
Data analysis
We adopted an inductive thematic analysis approach (Braun & Clarke, 2006). After repeated reading of the transcripts to familiarise ourselves with the data, a member of the research team, SH, independently coded the transcripts. SH developed a coding framework, which was presented and discussed among the wider research team. The research team met regularly to refine the coding framework iteratively to reach consensus on the definition and content of the themes. The framework was further refined by merging similar themes, removing extraneous themes and exploring the interrelationships between themes. All focus group discussions and interviews were audio-recorded and transcribed verbatim. They were then entered into QSR NVivo 12 for Windows.
Reflexivity and rigour
The focus group discussions were carried out by the ARDSI team of MP, RN and SH. MP hailing from South India has a strong grasp of written and spoken Tamil. She has vast experience working with people living with dementia; she is currently serving as ARDSI chairperson. RN a former caregiver, works as Executive Director at ARDSI and is fluent in Tamil, Hindi and English. SH, has worked as a psychologist in the field of dementia for 8 years, is fluent in English and Hindi. MP based in Chennai and RN in Delhi, made it easier as they are associated with the local chapters. This facilitated recruitment of the sample and enabled this recruitment to occur as per the pre-identified criteria of this study for the required target groups. As there are ARDSI chapters across the country affiliated with different medical organisations, it was more feasible to recruit from these chapters; once ethical approval was received from the affiliated organisations.
All individuals involved in the focus group discussions and coding received the same standardised training on the process, irrespective of prior experiences. All transcripts were transcribed in the language in which the interviews occurred (Tamil or Hindi), and then translated into English. The wording was kept as close to the original phrasing whenever possible. SH was involved in the initial focus group discussions and transcription and was also responsible for coding; this provided familiarity with the topic and content. Due to the education and qualification backgrounds of the researchers, there is the possibility that participants were less likely to speak freely on certain issues. To reflect the process of coding, frequent discussions were held with an independent researcher not involved in the data collection or transcription (SEL or NF). The reflection on the coding by senior researchers (SEL and NF) may have been biased by their experiences of dementia within a western context. In addition, the coding framework was presented to the wider Strengthening Responses to Dementia in Developing Countries (STRiDE) group, to stimulate discussion and reflection. STRiDE (www.stride-dementia.org) is a multi-national project led by a wide team of researchers from and related field of dementias, which aims to understand the impact of dementia in social, economic and cultural contexts in order to strength planning, implementations and evaluations on dementia plan in India. This study was conducted as part of the wider STRiDE project. The aim of these discussions was not to achieve a unified theme across India to understand the attitudes and perceptions of the various focus group discussions and persons with dementia, but to capture different themes that emerged.
Findings
Data from the focus group discussions and interviews revealed three overachieving themes; (1) Poor awareness, (2) Stigma and (3) Barriers to accessing care. All themes occurred within the context of socio-cultural aspects which typically framed discussions. The main themes and subthemes identified from the data are shown below in Figure 1. Key themes and subthemes identified across participant groups.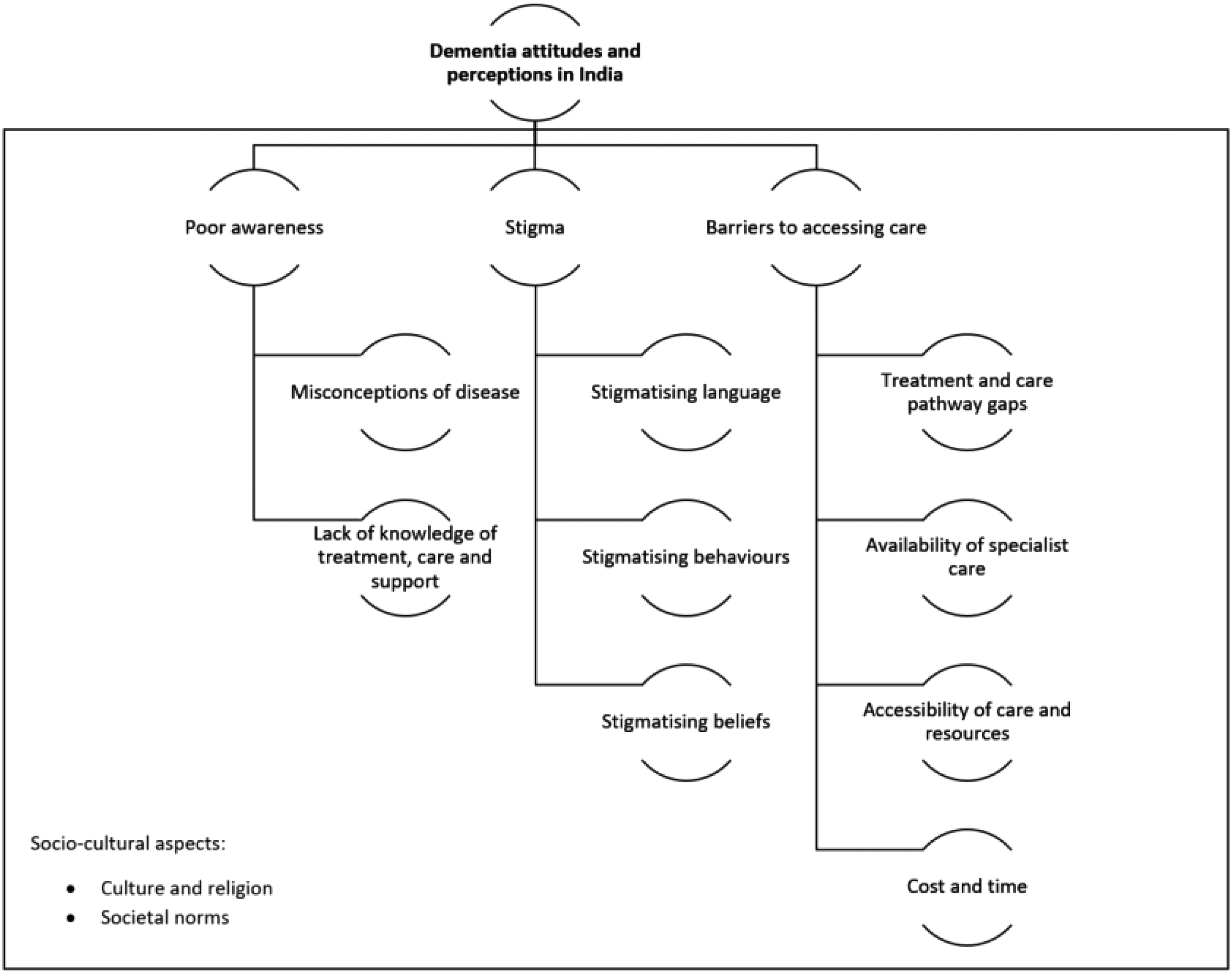
Theme 1: Poor awareness
The most common theme that emerged across participant groups was poor dementia awareness. This could be broadly split into lack of knowledge and misconceptions; the former represented a self-described absence of knowledge; the latter represented an incorrect understanding of dementia.
Participants, irrespective of site or stakeholder group had poor understanding and awareness of dementia; they also expressed being conscious of the fact that they have low dementia awareness. Most caregivers said they came to the focus group discussions in order to learn more about dementia. Caregivers brought their loved ones with dementia to the focus group discussion as they thought that it would benefit them. “Why I came here because, in India [we have] no awareness, we do not know where to go, we are totally confused” – PMS07, Male, Carers group, Chennai “…this group discussion happening here is also very helpful. When lot of people discuss this, I thought I would get some tips from this” – PM03, Male, Carers group, Chennai
Caregivers shared their experience of their confusion with receiving a dementia diagnosis and attributed it to failings of medical professional’s knowledge. In a one-on-one interview, a caregiver reported the impression from their physician after seeing the dementia diagnosis: ‘I know her because something happened to her suddenly, it will affect her, it is nothing to do with all these things (dementia). This is a joke and words (the diagnosis), kindly throw it out,’ – PMSHCG, Male, Carer, Chennai
Healthcare professionals trained in dementia and who theoretically had access to dementia resources also seemed to have a limited knowledge of the nature of the disease, cause and overall understanding of dementia. “(what causes dementia) …. is due to deficiency of vitamins, exactly I don't know what is the reason of it, some problem with nervous system also…” - PMCG003, Male, Healthcare professional, Delhi
Notably, there appeared to be a divergence in the dementia knowledge of healthcare professionals. Those who had experience working abroad tended to have greater expertise on the topic.
It also emerged from the discussion that dementia gets mislabelled. Across family carers and healthcare professionals focus group discussions, many participants referred to a gap within the healthcare system and poor training of medical practitioners in dementia care. Misdiagnosis was one concern that participants had spoken about. “They are misdiagnosed and treated for something else, they are treated for mental disorders, they are treated for OCD, obsessive-compulsive disorder for that they are given medicines.” – PMPt002, Male, healthcare professional, Delhi
Irrespective of different types of challenges faced such as misconception, stigma, mistreatment or lack of accessibility to treatment, most participants attributed these challenges towards a lack of dementia awareness. Throughout discussions among all the groups, a dire need to raise dementia awareness across all levels [HCP, GP, CG] was identified. “The most important thing is to educate the caregivers, spread awareness as there is not much treatment for dementia” - PMCG003, healthcare professional, Male, Delhi
Some participants believed that dementia awareness in urban areas is better, as there is some amount of awareness and access to services that provide dementia treatment.
There was a prevailing view that dementia was a normal part of ageing and thus not a major health concern. “Whenever there is a cognitive deficiency in a cluster of family, what they think is, he is aged, it is common in this age.” PdR01, male, healthcare professional, Chennai
Across all groups, participants identified a range of potential causes of dementia; attributing dementia to depression, stress, older people living alone, poor nutrition or according to some, due to demons, spells or due to the person’s Karma. “I see a lot of reasons why it happens; it is correct that one main reason is because of stress, along with stress, in Indian culture we don’t have a proper diet in the first place” - CPF03HCp, Female, healthcare professional, Chennai,
One of the misconceptions that emerged from some participants was that in general, people thought that the disease will be passed on to the next generation through the family genes. “(If) There is someone in my house with this similar issue, and a girl is getting marriage proposal in my house, so they might think if you make the alliance here will this person get this disease due to heredity, in future if there is a kid the kid might have to you suffer all this” - PGp01, Female, general Public, Delhi,
As per socio-cultural norms, children are expected to care for their parents as they age. As a result of such norms, some participants perceived one cause of dementia to be older people living alone by themselves. “I feel because of this reason a lot of people get dementia issues other than this another major reason is the neglecting of parents (by their children) which leads them to depression they are not able to share the daily things with others.” – S003, Female, Delhi
People with dementia and their caregivers had some idea about existence of dementia memory clinics or other care services, as they were either associated with the hospital memory clinic or the dementia support services provided in these two cities. However, the general public participants perceived that there is no treatment, care or support available for dementia. “I don’t feel that till now there is any treatment for this, or there is any place where they provide counselling for this, or people get any information about this.”- PM2, Male, General public group, Delhi
Theme 2: Stigma
Most of the time participants felt that stigma occurred as a result of poor awareness of dementia in society. Participants were more comfortable discussing stigma in the third person plausibly creating distance in relation to the person with dementia. Most of the participants discussed that dementia is most commonly related to mental illness and this contributes to stigmatisation. Participants were hesitant to say the local idioms for dementia on their own, but when one initiated the conversation, the rest of the group followed breaking the ice, after which participants spoke at length.
For instance, in Hindi language some common terms used for dementia was expressed: “(Who toh sathya gaye hai, who mandhuddhi hai, pagal hai) He has gone senile, has gone cuckoo, mad. If there is an old man in a house who has gone senile, the whole family faces the stigma of it, people don’t want to marry off their daughters in such family’ – P03gP, Female, General public group, Delhi
Also, from the Tamil language it was observed that common idioms were used instead of the term dementia: ‘Dementia I don’t think (any one uses the term dementia), for all the conditions they are using the word, ‘(Paittiyam)’ Lunatic or ‘Mana noyali’ mentally ill.’ –P04H, Female, Health care professional, Chennai
It was very common for participants to refer to people with dementia in the same way that they would to small children, due to the poor cognitive and functional abilities associated with the condition. Even experts in dementia who attended the focus group discussions referred to persons with dementia as being childlike, without realising it diminishes the person. As the person with dementia experiences more cognitive challenges, they were described as ‘childlike’ which was considered to be reflective of their lower cognitive abilities, dependency on others or just acting ‘foolish or difficult’. “They (persons with dementia) are almost like child, you have to take care as (they are) a child, even a child doesn’t know anything, dementia person also doesn’t know anything.” – PM1, Healthcare professional, Chennai “(in villages people refer to persons with dementia and) decide that elderly has started behaving childlike” - PMPt002, Healthcare professional, Delhi
Participants described families’ and friends’ stigmatising behaviour towards the person with dementia. Many families perceived dementia as mental illness and behaved in a negative way towards the person with dementia. It was highlighted in most of the groups that the person with dementia was generally isolated by the family, as they feared how others would react to the condition. “I feel that it is the major issue, where you need to deal with the person as a normal person, give them the same position in the family, make them sit in the gathering, where the visitor is should I understand that this person is unwell and they should also deal well, not that this person is mad and we should avoid them.” – PF0o1 , Female, general public, Delhi
Healthcare workers who had experience dealing with families with persons with dementia reported that it is generally perceived that in rural areas there is limited awareness of dementia resulting in increased stigma and greater negative consequences like neglect and abuse. The Delhi healthcare professionals who visit rural areas as part of dementia campaigns for awareness and screenings had experienced and observed the attitudes of people towards people with dementia and shared similar experiences towards mental health conditions. A lot of people related to rural experiences from their own hometowns. “Villagers do not know what it is, in villages they throw stones (on persons with dementia), try to shoo them off, meaning (if) that helpless person (disabled/demented) is walking people will shoo or tease, the small kids, group of 4-5 kids, say teenagers (beat them) that is with stone or stick.” – PMPt002, Male, Healthcare professional, Delhi
Theme 3: Barriers in accessing care
Certainly, whilst misconceptions and poor awareness (above) were likely to act as a barrier to care, other physical barriers were also identified, including accessibility, affordability, family neglect and dependency of older people on their family for mobility. “When it comes to cost, there is both direct cost and indirect cost. Direct cost could be less compelling to indirect cost, so if there is a person is taking care of them he has to lose his one-day job and come and bring him here and transportation cost full and everything. That becomes again a second cost factor for the person” - CPm01h, Male, Healthcare professional group, Chennai.
Irrespective of experience with dementia, participants held the general view that there is a lack of specialised hospitals, especially in rural areas, which also applies to dementia care. ‘This care is available only in big hospitals. Small hospitals, Primary Health Care Centres don’t have this, and I think we need to make awareness in Primary Health centres about dementia. We need to talk about this to doctors in Health Care Centres too, they themselves don’t know this.’ '- Pf005N, Female, General Public group, Chennai
Even amongst healthcare professionals, there was a common impression that dementia care is specialised and only experts can provide such care, which may be lacking in rural areas. “Even the doctors there [rural areas] they also don’t have information because they are only MBBS (Bachelor of Medicine and Bachelor of Surgery), simple MBBS in rural areas, he does not know the neurology and they don’t even diagnose Alzheimer’s” – PPh02, Male, Healthcare professional group, Delhi
It was a common perception among all the participants that there is poor or no treatment available for dementia, even if a person gets a diagnosis. Generally, people did not trust private healthcare services as they think it is more of a commercial venture; with them trying to make money out of them. With respect to public health sector services, however, people were generally not happy with the services provided (free of cost). “…another factor is that since we are government institution, we do not charge for anything for consultation, most treatment is free, most (medical) investigations are also free, so the commercial motives cannot be imposed on.” - P001, Female, Healthcare Professional, Delhi
Families who received the diagnosis mentioned that it was not always possible to follow the recommended course of treatment as advised, due to accessibility and affordability of suggested therapies. “but we were not able to apply and follow occupation therapy in full-fledged manner, so it slowly it progressed... now 9- 10 years his family is taking care and is managed by daughter” – MCG, Male, Caregivers group, Chennai
Cross-cutting themes: Societal norms, culture and religion
Throughout the focus group discussions and interviews, it was apparent that societal norms, culture and religion played an important role in framing conversations and thought processes surrounding dementia and its care.
Participants highlighted cultural norms wherein older people tend to lose their family position, independence and increasingly needed support and assistance from others in their older age, especially after their retirement. “They are dependent on son or the daughter, they are taking care of them, they (elderly) are not independent in our culture” - PF002, Female, General Public, Chennai
Even for minor errands like visiting banks, grocery stores or hospitals, they needed assistance and could not perform simple tasks on their own. The dependency on others and the migration of younger population made them feel further helpless. All the groups conveyed that having older people living alone is not seen as a good practice in Indian society. “another major reason is the neglecting of parents (by their children) which leads them to depression they are not able to share the daily things with others.” – PF003, Female, General Public group, Delhi
It was observed that caring for older people is traditionally viewed as a family responsibility in the Indian context.
Most of the participants seem to have the belief that dementia is caused because of one’s bad Karma, yet they avoided speaking about this in the group. It was observed that they were afraid that others would judge them for their beliefs. “See that Karma theory is a different thing”- PM1, Male, General Public, Delhi. “(Yes, Karma is a cause of dementia) Its some stigma, as they have aged they have gone mad. People say like this generally.”- PF3, General Public, Delhi. “They also say (‘Upar ka prakop ho gaya’) it is a doing of Ghost or demons.”- PMCG003, Male, General Public group, Delhi
The role of faith and spirituality also formed beliefs about prognosis. In one circumstance a participant with dementia believed that she would be cured if it was God’s will. “Yes, I do think, at the mercy of the one above (God) and I will be cured” - PF01SH, Female, Person with dementia, Chennai.
However, it was observed that participants were hesitant to talk about their beliefs openly such as dementia is caused by Karma or magic. When prompted, they shared that others had such beliefs. “So people call these kinds of patients with a lot of names like he has gone mad, there is no proper diagnosis, everyone is calling the patient mad or is under the cast of Ghost, or someone has cast a magic spell.” - PMPt002, Male, Healthcare professional, Delhi
Social isolation of persons with dementia and their family caregivers were reported. The family avoided taking the person with dementia to social gatherings. This is because as the disease progresses, dependency on the caregiver increases and they eventually drop out from attending social functions and gatherings. In addition, when caregivers were not able to get the person with dementia outside the house for a social gathering and did not have anyone else to look after them at home, they also dropped out from socialising. “A person who was very involved (earlier) in meetings and family functions gets isolated, if you take this person to marriage what if the person starts misbehaving? I also feel impression that is made (by others) in my family is behaving like a mad person.” PF1, Female, General Public, Delhi “Though it is tough we don’t have a choice. Don’t take him to family functions. all people come and ask why it has happened. we should take them somewhere different, mixed along with public like beach.’’ PM05, Male, Caregiver, Chennai
Discussion
The principal aim of this study was to understand the perceptions, attitudes and beliefs of dementia in India from two diverse metropolitan cities, Delhi and Chennai. The study explored dementia-related insights and experiences in relation to people living with dementia among four stakeholder groups: the general public, healthcare providers, people living with dementia and carers. Explicitly, this study investigated existing knowledge, attitudes and behaviours towards people with dementia and carers; experiences of stigma and discrimination; local culture-specific idioms of stigma and discrimination, current practices to promote social inclusion and preferences about how to reduce stigma among the population.
Across all key stakeholder groups, there appeared to be a gap in knowledge surrounding dementia. Healthcare professionals shared that they did not have sufficient understanding of dementia, but this was due to not being taught about it in the medical curriculum, whilst also believing that they did not come across such patients on a regular basis. This supports previous quantitative research from India, in which gaps in knowledge were present amongst a group of doctors and nurses (Biswas et al., 2017) and nursing staff within nursing homes (Strøm et al., 2019), albeit to varying degrees. Caregivers supported the view that doctors had insufficient knowledge and training of dementia, as exemplified by an experience of a doctor denying diagnosis even in the presence of a brain scan. Raising awareness is seen as one of the key pathway to tackle stigma (Mukadam & Livingston, 2012), and as such, it is unsurprising that raising awareness of dementia is recommended in India (Dias & Patel, 2009; Emmatty et al., 2016).
There seems to be no standard word for dementia in the regional languages, and the focus group discussions highlighted multiple words used in different languages for dementia, out of which some words highlighted a stigmatising approach of addressing the person with dementia or the disease. In Tamil
Dementia, as reported by the participants, was associated with many different beliefs depending on an individual’s educational background, religious beliefs, societal and traditional norms. It was observed in the focus group discussion’s that dementia is one’s destiny, Gods will, Karma or evil doings. Caregivers reflected that dementia is a natural course of life and one’s destiny that cannot be altered. Whilst culturally distinct, we can observe some parallels with findings in Pakistan. Religion appears to be central in shaping attitudes amongst the general public (Farina et al., 2019), and family members perceived duty of care (Balouch et al., 2020). Whilst the heterogeneous religious population within India makes the importance of religion less clear, it is evident that filial piety still features heavily in the culture. The introduction of the Maintenance and Welfare of Parents and Senior Citizens Act of 2007, in which there is a statutory duty for adult children to support their parents who are unable to provide for themselves (Serrano et al., 2017), could be a symptom (and cause) of such attitudes of care provision of people with dementia. The Maintenance and Welfare of Parents and Senior Citizens Act was not explicitly asked in the focus group discussion, which limits these conclusions whereas this aspect can be explored in further studies. When combined with a perceived lack of adequate infrastructure and skilled workforce, it is likely that these barriers bolster attitudes of ‘keeping it in family’ and reluctance to place family members into long-term care facilities (Brijnath, 2012; Sharma & Marwah, 2017). Furthermore, awareness about institutional care, and subsequently, the demand for services like care homes or dementia assistive livings are much lower. Studies reported that older people prefer to live in their own home with family even if they lack emotional support or are subjected to verbal or physical abuse, neglect and disrespect from their children (Kumar et al., 2012) (Khurana, 2013). With the influence of multiple religions, cultures and traditions, the Indian society values family as the most important institution and like most of the eastern societies, is a collectivist society which emphasises on family integrity, loyalty and unity.
A key limitation of this study is that it is derived from a modest sample of key stakeholders in Delhi and Chennai. As such, it is important to not assume this is a representative sample of general public, healthcare professionals, caregivers or people with dementia. As dementia diagnosis rates are low and tend to happen late in India, this acted as a barrier to recruiting people with dementia that were cognitively able to engage with this research. In addition, those that did enrol in the research were likely to have some interest in the topic, therefore the views presented here might reflect those who in fact are more aware of dementia. Similarly, we should recognise that other regions of India, most notably more rural areas, are likely to have different attitudes of dementia, not least because of different education levels, service availability and cultural norms. Whilst lessons can be learnt from this study and applied to Indian communities living abroad, it should be done so cautiously due to structural and societal differences. The findings may, however, be more pertinent to first generation immigrants. Another key limitation of the study was that healthcare workers were identified from the hospitals associated with the respective chapters. In Chennai the healthcare professionals were a multi-disciplinary group, including nutritionist, pharmacists, researcher, physiotherapist but with no experience of working with dementia. In Delhi they were from different backgrounds like paid carer, physiotherapist, researcher but has had experience working with dementia. Due to the limitation of study design and resources it was more purposive and limited data collection.
Conclusions
The study provides further evidence of a lack of awareness and potentially stigmatising attitudes towards dementia in India. The study builds upon past literature by incorporating perspectives of different stakeholders who will interact with dementia within different capacities. In addition, recruitment of these stakeholders from different settings and languages, provides different perspectives from this multi-cultural country. It highlights the societal and cultural influence on dementia-related stigma, which contributes towards delay in accessing care. The study demonstrates the need for proper recognised terminology in various Indian languages, which may help to reduce stigma towards dementia. However, it is important to note that the use of stigmatising language is also reflective of culturally embedded aspects, which cannot be resolved with only simple changes in terminology. With the given demographics of dementia in India, it is essential to address these issues with anti-stigma campaigns at higher levels like in dementia national policy and/or strategy, which can help to educate and reach out to larger populations across different regions of India.
Supplemental Material
Supplemental Material – Understanding, experiences and attitudes of dementia in India: A qualitative study
Supplemental Material for Understanding, experiences and attitudes of dementia in India: A qualitative study by Saadiya Hurzuk, Nicolas Farina, Meera Pattabiraman, R Narendhar, Suvarna Alladi, Jayeeta Rajagopalan, Adelina Comas-Herrera, Priya Treesa Thomas and Sara Evans-Lacko in Dementia
Footnotes
Acknowledgements
The authors would like to thank all the participants for taking time out of their schedules to contribute in the focus group discussions and interviews. We would also like to express our gratitude towards Dr. Sathianathan Ramanathan and Mr. Stanley Vinoth from ARDSI Chennai Chapter and Dr. Manjari Tripathi and Col. Vinay Kumar Khanna from ARDSI Delhi chapter for their contribution towards this study. We grateful to the support and input from the wider STRiDE team.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the UK Research and Innovation Global Challenges Research Fund (ES/P010938/1).
Ethical approval
Ethical approval for this study was obtained from London School of Economics and Political Science Research Ethics Committee and National Institute of Mental Health and Neuro-Sciences Ethics committee (NIMHANS) (No. NIMHNAS/IEC (BS &NS DIV.)/18th MEETING/2019 Date: 07.05.2019)
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.