
Abstract
Evidence supports that older adults with cognitive impairment can reliably communicate their values and choices, even as cognition may decline. Shared decision-making, including the patient, family members, and healthcare providers, is critical to patient-centered care. The aim of this scoping review was to synthesize what is known about shared decision-making in persons living with dementia. A scoping review was completed in PubMed, CINAHL, and Web of Science. Keywords included content areas of dementia and shared decision-making. Inclusion criteria were as follows: description of shared or cooperative decision making, cognitively impaired patient population, adult patient, and original research. Review articles were excluded, as well as those for which the formal healthcare provider was the only team member involved in the decision-making (e.g., physician), and/or the patient sample was not cognitively impaired. Systematically extracted data were organized in a table, compared, and synthesized. The search yielded 263 non-duplicate articles that were screened by title and abstract. Ninety-three articles remained, and the full text was reviewed; 32 articles were eligible for this review. Studies were from across Europe (n = 23), North America (n = 7), and Australia (n = 2). The majority of the articles used a qualitative study design, and 10 used a quantitative study design. Categories of similar shared decision-making topics emerged, including health promotion, end-of-life, advanced care planning, and housing decisions. The majority of articles focused on shared decision-making regarding health promotion for the patient (n = 16). Findings illustrate that shared decision-making requires deliberate effort and is preferred among family members, healthcare providers, and patients with dementia. Future research should include more robust efficacy testing of decision-making tools, incorporation of evidence-based shared decisionmaking approaches based on cognitive status/diagnosis, and consideration of geographical/cultural differences in healthcare delivery systems.
Keywords
Introduction
Dementia describes a group of symptoms that include cognitive impairment and an individual’s inability to perform activities of daily living (Hebert et al., 2013). Alzheimer’s disease and related dementias describe the group of conditions that cause symptoms referred to as dementia. Brain lesions found in Alzheimer’s disease cause difficulties with memory, language, problem-solving, and other cognitive skills (Fazio et al., 2018; Mantzavinos & Alexiou, 2017), which may contribute to difficulty communicating by and with people living with dementia. However, evidence supports that older adults with cognitive impairment can reliably communicate their values and choices, even as cognition may decline (Feinberg & Whitlatch, 2001). Unfortunately, adults living with dementia’s decision-making capacity is often overlooked or revoked by family members or healthcare professionals due to the communication barriers that present with the disease. Caregivers and healthcare providers are frequently tasked with making decisions for these individuals. As a result, people living with dementia may experience a loss of individuality and dignity due to this communication barrier.
Shared decision-making in dementia refers to the practice of working with patients, caregivers, and/or providers to choose how to proceed in issues related to healthcare based on at least two persons’ preferences, values, and health trajectory (Van der Flier et al., 2017). The Alzheimer’s Association presents Dementia Care Practice Recommendations with patient-centered care as a focus, and these guidelines include the use of communication systems to facilitate the delivery of care (Fazio et al., 2018). However, the guidelines do not outline what these communication systems are or define shared decision-making as one of them. Similarly, in the past decade, legislation has been passed to recognize patients with dementia should participate in the decision-making process, but there is limited evidence on how to incorporate and respect patient preferences of persons with varying cognitive impairment (Daly et al., 2018).
There is inadequate evidence regarding best practices for maintaining the dignity and independence in patients with AD regarding decision making. One challenge to best practice may be that family care partners and long-term care staff underestimate Alzheimer’s patients’ desire and ability to participate in decision-making (Daly et al., 2018). Previous reviews of decision-making in dementia focused solely on a long-term care population (Daly et al., 2018), which limits generalizability of findings to the majority of decision-making that occurs outside of institutionalized, long-term care settings. Changes are being made slowly to give patients with dementia more dignity in day-to-day decision-making, but the current evidence around shared decision-making for older adults with dementia has not been sufficiently explored. Using the enhanced scoping review methodology presented by Daudt et al (2013) and original approach by Arksey and O’Malley’ (2005), the aim of this scoping review was to synthesize what is known about shared-decision making (SDM) in older adults living with dementia. The research question was purposely broad to capture the extent, range and nature of research activity (Daudt et al, 2013).
Methods
The literature search was developed under the guidance of a professional medical librarian (DW). Once the project team agreed on the keywords and controlled vocabulary, the librarian performed the search in PubMed, CINAHL, and Web of Science in July 2021. English language was the only search limit used across the databases. The PubMed search consisted of the MeSH terms and keywords listed below. Searches in the CINAHL and Web of Sciences databases were performed using keywords and phrases from the PubMed search: (“cooperative decision making” OR “decision making, shared”[mesh] OR “shared decision making”) AND (Alzheimer OR “Alzheimer disease”[mesh] OR “mild cognitive impairment” OR “cognitive dysfunction”[mesh] OR dementia OR “dementia”[mesh] OR “Parkinson’s disease dementia” OR “Lewy body disease” OR “Lewy body disease”[mesh] OR “Corticobasal syndrome” OR “posterior cortical atrophy” OR “frontotemporal degeneration” OR “frontotemporal dementia”[mesh] OR “vascular dementia” OR “dementia, vascular”[mesh] AND (English[Filter]). After the initial search across the three databases, all results were exported into the citation manager, Sciwheel, where duplicates were removed. The remaining unique citations were then exported into Covidence to facilitate the screening process.
Title/Abstract Screening
A small, interdisciplinary team was assembled to develop the research question and to ensure comprehensive review, rigor, and reproducibility (Daudt et al, 2013). All the articles were screened using the following inclusion criteria: studies that focused on (1) shared decision making or cooperative decision making, (2) some kind of cognitive impairment, and (3) adult patients. All the articles were jointly assessed by two authors, and disagreements were resolved by the consensus of three authors (MM, JG, & IW) based on the recommended approach of Levac et al (2010).
Full-Text Screening
The full text of the articles was then attached to the articles that made it through the initial screening process. All the articles were jointly assessed by two authors, and a final decision was made by consensus of the three authors who reviewed the articles (MM, JG, & IW).
Data Extraction and Analysis
After completing the final article list, the team created a table summarizing the findings for each article using the following headings: Covidence study number; author, date, title; country; aims or purpose; study design; setting; sample description; decision-making groups represented; the decision of interest; decision-making measures; primary outcome or study variable of interest; SDM findings; and limitations. The research team organized the data based on Arksey and O’Malley’s (2005) approach to sorting by theme and issues that emerged during the review process. Specifically, articles with shared categories of interest (e.g., qualitative study design) were described and presented in individual tables based on the decision of interest. To enhance our approach, we used Excel for visualization and organization based on Daudt et al’s (2013) framework. 13 headings were used for data extraction were included in the Excel document, then summarized and sorted into categories by the study team. No hierarchy emerged when categories were created, although the categories that did emerge were chosen to promote adherence to answering the original research question. Two headings were excluded in the published table: (1) the Covidence study number and (2) decision-making measures. Decision-making measures were not included in the published table due to insufficient data extracted from the final article list. The descriptive analysis plan was determined a priori based on Arksey and O’Malley’s framework that uses a “descriptive numerical summary related to the general information collected and a thematic construction” (Daudt et al, 2013, S1) and went one step further to consider Levac et al (2010) recommendations to discuss implications for future research, practice and policy.
Results
The initial search retrieved 458 articles from the three databases (PubMed [170], CINAHL [130], and Web of Science [158]). All results were exported into the citation manager, Sciwheel, where 195 duplicates were removed. The 263 unique citations were then exported into Covidence to facilitate the screening process. Following the title/abstract screen, 170 articles were deemed not relevant. 60 articles were excluded using the following reasons: wrong patient population (n = 31), not original research (n = 20), not shared decision making as an outcome (n = 9), not in English (n = 1). The authors were satisfied with the results of the full-text screen, so no additional articles were included either through citation chaining or other sources. The total number of articles included was 32 (see Figure 1 for modified PRISMA Flow Diagram and Table 1 for Included Study Characteristics). PRISMA flow diagram. Subject Characteristics, Methods, and Outcomes of Included Studies.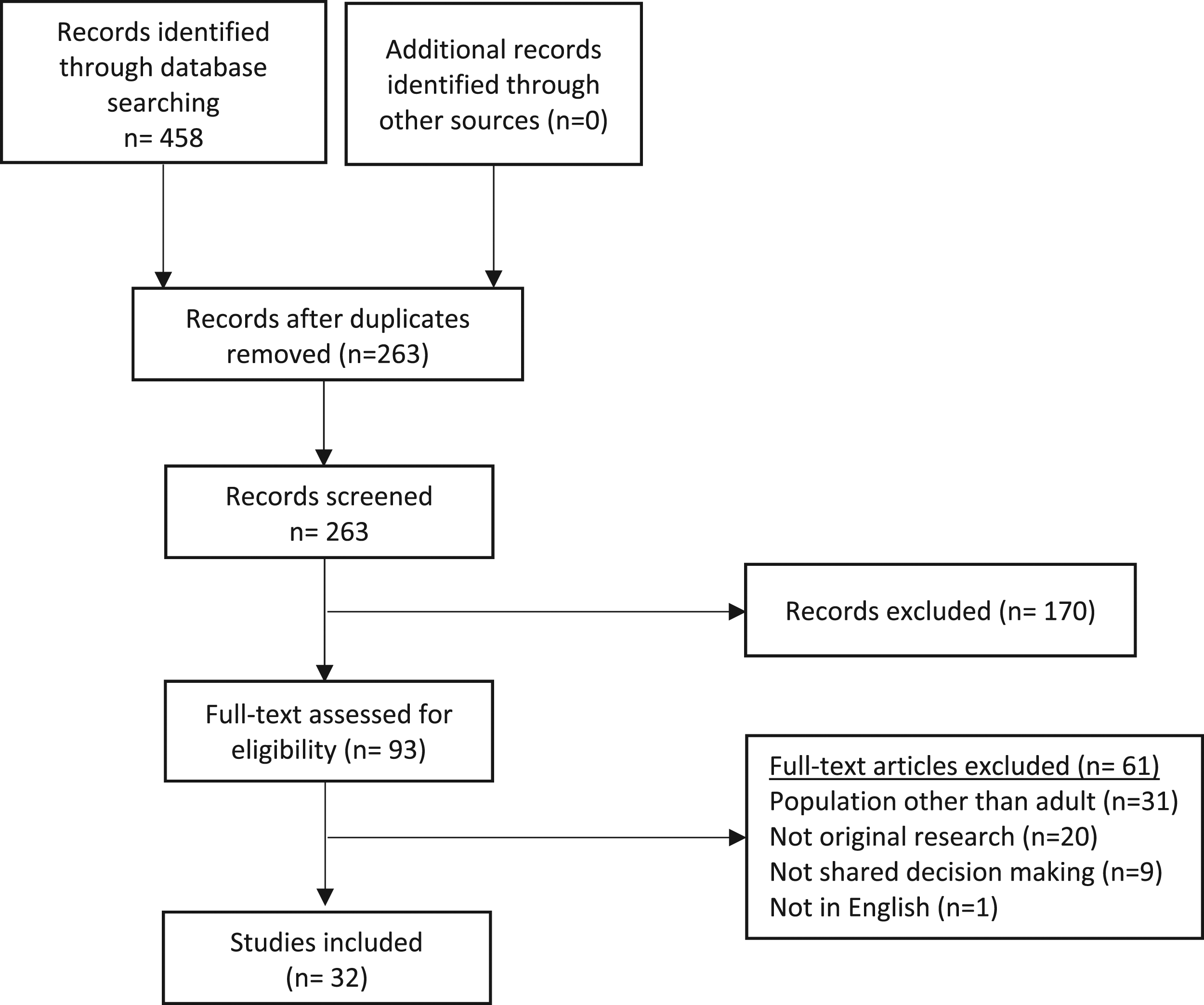

Of the 32 articles eligible for this review, studies were from across Europe (n = 23), North America (n = 7), and Australia (n = 2). In studies originating in Europe, 11 were from the Netherlands, one from the Netherlands and Italy, five from the UK, two from Belgium, one from Northern Ireland, one from Norway, one from Finland, and one from Germany. Articles from North America were comprised of four from Canada and three from the US.
The majority of the articles used a qualitative study design (n = 21; qualitative only, n = 13; mixed-methods, n = 9), and 10 used a quantitative study design (experimental, n = 1; quasi-experimental, n = 1; descriptive, n = 8). Of the 21 qualitative studies, 13 used qualitative methods only, and 9 used a mixed-methods approach. Of the 10 that used a quantitative study design, one was experimental, one was quasi-experimental, and eight were descriptive studies.
Study populations included patients with dementia (n = 24); caregiver, proxy, or relative (n = 30); and healthcare team members (n = 19). There were a range of cognitive evaluations and inclusion/exclusion criteria for each study for the patient population living with dementia. Participant cognitive status varied across and within individual studies, ranging from mild cognitive impairment to severe/advanced dementia.
Articles were summarized in tables and recategorized based on similarities in SDM topics that emerged through a review of the article and synthesis by three investigators (MM, JG, & IW). The categories included: health promotion (n = 11); advanced care planning (n = 6) and end-of-life (n = 3); development of a decision-making aid (n = 7); and housing (n = 4) and daycare (n = 1).
Health Promotion
There were 11 studies that focused on health promotion related to SDM. Topics included SDM in general patient care (Aaltonen et al., 2021; Groen-van De Ven et al., 2017, 2018; Hamann et al., 2011), activities of daily living (Groen-van De Ven et al., 2017; Stevenson & Taylor, 2016), clinical appointments (Griffin et al., 2020; Groen-van De Ven et al., 2017), diagnostic testing (Visser et al., 2018), and medication use (Dooley et al., 2018; Mccabe et al., 2019). Of the 11 studies, five were qualitative (Aaltonen et al., 2021; Griffin et al., 2020; Groen-van De Ven et al., 2017, 2018; Stevenson & Taylor, 2016), two used mixed methods (Murphy & Oliver, 2012; Span et al., 2015; Visser et al., 2018), and three quantitative approaches (Dooley et al., 2018; Hamann et al., 2011; Mccabe et al., 2019).
The most common form of health promotion discussed as part of SDM among the articles was general patient care. In Aaltonen et al (2021), researchers described the limitations and range of influence of caregivers when discussing care of persons with dementia with formal healthcare providers. Groen-van de Ven et al (2017) asked about specific topics such as managing daily life with dementia, arranging care and support, living in society, and representing the persons with dementia. They explored how these decisions were made, when decisions occurred, and characteristic patterns in the sequence of decisions in the care networks, and ultimately found the patterns differed between people living alone and those with an informal caregiver living in the same home (Groen-van De Ven et al., 2017). In a secondary analysis of the same sample, researchers identified challenges to SDM, including adapting to diminishing independence, including shifting roles in SDM; tensions in network interactions; and timing decisions well (Groen-Van De Ven et al., 2018). In the only study focused on mild cognitive impairment and early-stage dementia, Hamann et al (2011) found that patients preferred to have the greatest say in social decision making and “want their relatives to have little influence on social or medical decisions.” This quantitative study measured patient confidence, and better decisional capacity and Mini Mental Status Examination scores were found to be predictors of stronger patient participation preferences (Hamann et al., 2011).
There were two studies that described the role of SDM when determining a patient’s activities of daily living. One qualitative study described how risk information was shared among family caregiver-care recipient-and healthcare professionals to better understand the SDM process (Stevenson & Taylor, 2016). Groen-van de Ven et al (2017) discussed managing daily life for persons with dementia and the importance of activities of daily living when arranging care and support (Groen-van De Ven et al., 2017).
There were two studies that discussed clinical appointments as an important topic to consider for SDM for persons with dementia (Griffin et al., 2020; Groen-van De Ven et al., 2017; Visser et al., 2018) Groen-van de Ven et al (2017) presented findings on SDM related to clinical appointments, and Griffin et al (2020) conducted online focus groups with persons with dementia and their caregivers to provide evidence on best practice for decision making. They found that participants thoughts healthcare providers should be trained in SDM, the importance and significance of family caregivers in the decision-making process, and how to resolve conflicts between or among multiple decision-makers (Griffin et al., 2020). Finally, a mixed-methods study on the ABIDE project presented findings on patient-clinician communication during the process of undergoing diagnostic testing (Visser et al., 2018).
Two studies addressed SDM regarding medication use in older adults with dementia (Dooley et al., 2018; Mccabe et al., 2019). In a study with persons with dementia and healthcare providers (Dooley et al., 2018), there was found to be no association between patient acceptance or resistance and whether a medication was prescribed. However, patients stated they were significantly less satisfied with patient-provider communication when they were not given a choice in taking the medication. McCabe et al (2019) examined the process of SDM when deciding to start anticholinesterase inhibitors across different types of dementia. The quantitative study used the decision-making subscale of the Autonomy Preference Index and Satisfaction with Decision Scale to measure SDM of patients and caregivers/companions. Lower SDM scores were found for patients compared to companions, and patients with mixed dementia were more involved in decision-making compared with AD alone.
Housing & Daycare
Four articles focused explicitly on housing decisions for persons with dementia (Adekpedjou et al., 2019; Boucher et al., 2019; Elidor et al., 2020; Garvelink et al., 2019). Three of the four articles focused primarily on caregiver outcomes, using quantitative/discrete measurements of caregiver preferences and perceptions. The fourth article used qualitative methods, including separate interviews with persons with dementia and their caregivers.
A SDM training intervention for home care teams increased the proportion of caregivers reporting an active role in decision-making and their preferred decision-making role regarding housing (Adekpedjou et al., 2019). For caregivers involved in housing decisions, a greater perception of a joint decision-making process was linked to a higher burden of care and less decision regret (Boucher et al., 2019; Elidor et al., 2020). Housing decision-making involving patients and caregivers tended to correspond with elements of the Interprofessional (IP)- SDM model (Légaré et al, 2011; Garvelink et al., 2019). Although patients and caregivers preferred for persons with dementia to remain at home as long as possible, cognitive decline typically made moving inevitable eventually (Garvelink et al., 2019). Finally, though not explicitly focused on housing decisions, an additional qualitative study found that persons with dementia had less autonomy in decisions related to moving/housing, as compared to less consequential decisions (e.g., daily activities; Smebye et al., 2012).
One article focused on decisions regarding daycare for persons with dementia, including data from qualitative interviews with persons with dementia and informal and professional caregivers (Groen-Van De Ven et al., 2018). The authors identified three critical points in the decision-making process that resulted in various decision trajectories (i.e., the decision to attend or not attend daycare). Critical issues included initial expectations, followed by negotiation and trying daycare.
End-of-Life & Advanced Care Planning
Studies focused on EOL primarily made decisions around the process of and experiences with care at the EOL (Bolt et al., 2019; Davies et al., 2021; Hill et al., 2017). For all three studies, the individuals who were part of the decision-making process included the family caregivers, persons with dementia, and bereaved caregivers. Of the three studies, two were qualitative (Bolt et al., 2019; Davies et al., 2021), and one study used mixed methods. Findings can be summarized around consensus building amongst decision-makers (Davies et al., 2021; Hill et al., 2017); challenges around “moral rightness” of their decisions or considering emotions (Bolt et al., 2019; Davies et al., 2021), and sharing and exchanging information (Davies et al., 2021; Hill et al., 2017). The small sample sizes in both qualitative and mixed-method studies limited generalizability, and these SDM studies did not include a healthcare provider.
Six articles focused on advanced care planning with a focus on the degree of involvement of families and the older adult in the process (Ampe et al., 2017; Goossens et al., 2020; Tilburgs et al., 2020), as well as the level of SDM by examining patient preferences in conjunction with those of their physicians (Goossens et al., 2020; Kwak et al., 2019; Mariani et al., 2018), the importance of shared-decision making (Goossens et al., 2020; Tilburgs et al., 2020), and preparedness of proxy to engage in shared-decision making (Kwak et al., 2019; Mariani et al., 2018). Of the six studies, three studies (Givens et al., 2018; Goossens et al., 2020; Kwak et al., 2019) used quantitative methods to examine SDM, while three studies used mixed methods (Ampe et al., 2017; Mariani et al., 2018; Tilburgs et al., 2020). Of the SDM instruments used across all studies, only one instrument was used in more than one study, the OPTION scale (Ampe et al., 2017; Goossens et al., 2020). There were two other studies (Kwak et al., 2019; Tilburgs et al., 2020) that also included whether or not the SDM process resulted in a completed advanced care planning or documented advanced care planning conversations. One study (Mariani et al., 2018) that focused on life care planning was not specific to advanced care planning. Still, it showed similar results of improvement of residents and family members in the SDM process. Overall, the results illustrated that SDM was important and preferred SDM among family members, physicians, and patients. Results also indicated that having SDM increased their acceptance of the patient’s illness (Ampe et al., 2017; Givens et al., 2018; Goossens et al., 2020; Kwak et al., 2019; Tilburgs et al., 2020). Areas for future research builds on the limitations, which included small sample sizes (Kwak et al., 2019; Mariani et al., 2018), using proxy accounts of the patient’s preferences (Givens et al., 2018; Kwak et al., 2019), not including a measure of cognitive decline of the older adult (Goossens et al., 2020), and differences between documentation of a completed advanced care planning versus just having a conversation (Tilburgs et al., 2020).
Development of Decision-Making Aid
Eight articles presented approaches or findings related to the development of a decision-making aid. Tools were developed for patients to use in discussions (Bilodeau et al., 2019; Groen-van De Ven et al., 2017; Murphy & Oliver, 2012; Reitz & Dalemans, 2016; Span et al., 2015; Stirling et al., 2012), providers to use with patients (Casey et al., 2015; Meyer et al., 2019; Stirling et al., 2012), and relatives to use with persons with dementia (Murphy & Oliver, 2012; Reitz & Dalemans, 2016). SDM tools were meant to be used for general SDM targeting persons with dementia (Bilodeau et al., 2019; Casey et al., 2015; Groen-van De Ven et al., 2017; Murphy & Oliver, 2012; Reitz & Dalemans, 2016; Span et al., 2015), fall prevention (Meyer et al., 2019), and caregiver respite services (Stirling et al., 2012). Three studies used a qualitative research design (Casey et al., 2015; Groen-van De Ven et al., 2017; Stirling et al., 2012), four used mixed methods (Bilodeau et al., 2019; Murphy & Oliver, 2012; Reitz & Dalemans, 2016; Span et al., 2015), and one quantitative intervention study (Meyer et al., 2019).
Three studies describing SDM tool development used a qualitative research design (Casey et al., 2015; Groen-van De Ven et al., 2017; Stirling et al., 2012). Casey et al (2015) examined social interactions among nursing home residents and identified competencies and attitudes that facilitate patient autonomy, making decisions over time, reciprocal information exchange, use of a step-wise approach to SDM, and shared responsibility for decision-making within the care network (Casey et al., 2015). In another qualitative study, a secondary analysis was performed to create a model of collaborative deliberation in dementia care networks to support SDM. They propose an enriched model that includes preparatory work, rational discussion, and coalitions (Groen-van De Ven et al., 2017). Another study described how SDM can aid in selecting community-based respite services (Stirling et al., 2012). In one of the few studies that did not include persons with dementia, researchers found that there were differences amongst healthcare providers regarding the “type of information they believed was appropriate to share” with caregivers (Stirling et al., 2012). Many participants felt that caregivers would benefit from the use of the decision aid, and some felt that the use of aid would be useful for healthcare providers to work with caregivers (Stirling et al., 2012).
Three studies used a mixed-method design to aid in decision-aid development. Span et al (2015) evaluated a SDM tool to make decisions focusing on patient preference and ease of use called DecideGuide. When using DecideGuide, participants felt more involved and shared more information about daily issues than they had done without a formal SDM tool. In Murphy and Oliver (2012)’s mixed-method study, they describe how couples (persons with dementia and family caregivers) discuss personal care, getting around, housework, and activities of daily living using a SDM aid called Talking Mats (Murphy & Oliver, 2012). The tool significantly increased feelings of involvement and overall satisfaction with the SDM process for participants. Bilodeau et al (2019) present persons with dementia and their caregiver’s feedback on a revised SDM tool trialed across three case studies. A Dutch version of Talking Mats was used in SDM discussions about daily activities and care (Reitz & Dalemans, 2016). Findings demonstrate the feasibility of use in a different language from the original design, and participants stated the tool made it possible to understand each other better (Reitz & Dalemans, 2016). The only quantitative study described the development of a “discussion tool” to help persons with dementia and their caregivers talk about fall prevention strategies (Meyer et al., 2019). The tool facilitated discussion and collaboration among persons with dementia, caregivers, and health professionals.
Discussion
This scoping review illustrates that SDM requires deliberate effort from caregivers and healthcare providers to discuss and understand patient preferences. Findings from this scoping review included identification of decision topics between or among persons with dementia, caregivers, and healthcare providers that focused on health promotion, advanced care planning, and housing. Shared decision-making was preferred among family members, healthcare providers, and persons with dementia (Dooley et al, 2018; Hamann et al, 2011; Hill et al, 2017; Kwak et al, 2019), and models that incorporate SDM were found to promote patient and family satisfaction (Garvelink et al, 2019; Murphy et al, 2012; Reitz & Dalemans, 2016; Span et al, 2015; Stirling et al., 2012; Tilburgs et al., 2020). Articles also discussed the role of healthcare providers in the decision-making process and how their roles should be trained in shared-decision making (Casey et al., 2015; Griffin et al., 2020; Groen-van De Ven et al., 2017), including communication and how to incorporate and respect patient and caregiver/family preferences. Study findings highlight a patient-centered approach to decision making, as supported by Alzheimer’s Association’s (AA) Dementia Care Practice Recommendations (see Figure 2). AA Recommendations focus on the person-centered delivery of care model, depicting individuals with dementia and their caregivers in the center model (see Figure 2). This scoping review presents evidence that shared decision-making can be used to address various topics across the dementia continuum, ranging from current preferences in medication use to long-term care planning. Situating study findings within the Model, promoting decision-making capacity within the individual with dementia-caregiver dyad has the potential to impact all areas of care and care coordination. Alzheimer’s Association person-centered delivery model.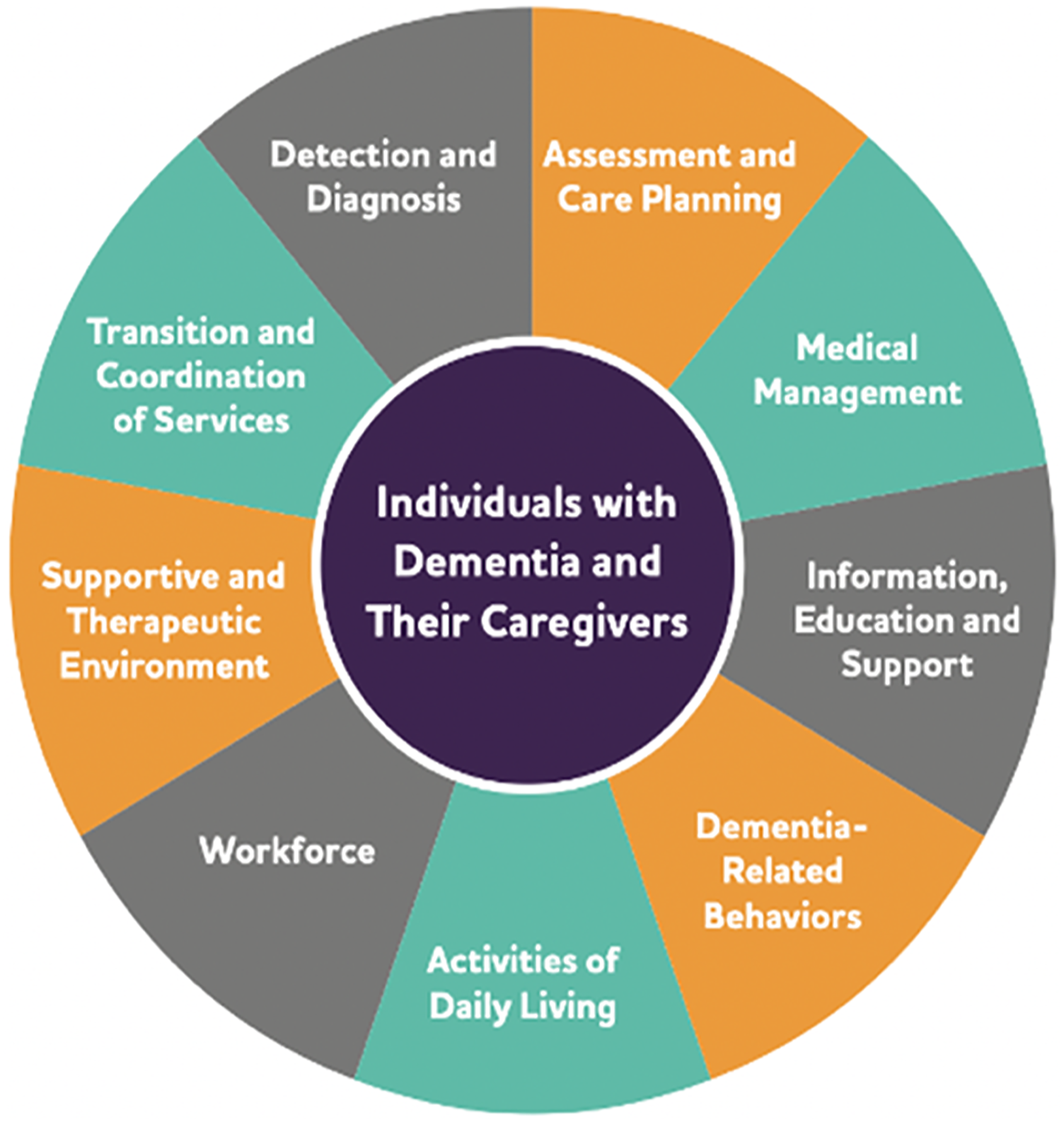
The majority of the articles identified in this scoping review used a qualitative study design. Qualitative articles across topics aimed to describe or understand patient, caregiver, and/or healthcare professional decision-making approaches and preferences to facilitate successful decision making. Researchers approached decision-making as a process requiring re-evaluation over time. This approach to decision-making was supported by the quantitative literature that identified patients’ decision-making capacity as a significant challenge to the decision-making process. Challenges to the determination of decision-making capacity were identified in studies with persons living with later-stage dementias and supported by a recent study by Sun et al (2020) that found decision-making ability “under risk” is only impaired in later-stage AD, not in MCI or normal cognition groups (Sun et al., 2020). In earlier stages of cognitive impairment, such as MCI, patients preferred to have greater input in social decision-making and wanted their relatives to have little influence on decisions. This was supported by Hamann et al. (2011), who found that better decisional capacity and cognitive status were found to be predictors of stronger patient decision-making participation preferences. This is an important consideration as there was significant study variation in inclusion and exclusion criteria for persons with dementia in this review, which may influence the generalizability of study findings to different dementia etiologies and staging. It is also possible that interventions or tools to improve decision-making may demonstrate varied efficacy.
In the AA Dementia Care Practice Recommendations, there is a considerable focus on the person-centered delivery of care model, depicting individuals with dementia and their caregivers in the center model (see Figure 2). This scoping review provides evidence that persons with dementia are recognized as important, if not vital, members of the care team, regardless of cognitive status. Most studies included in the review described persons with dementia across different stages of dementia with varying neuropsychological assessments or clinical diagnoses. As presented in the literature, guidelines for person-centered care should include communication systems to facilitate the delivery of care (Fazio et al., 2018). However, the AA guidelines do not provide characteristics of successful communication systems or approaches, nor does the AA define shared decision-making as an essential component of the Person-Centered Delivery Model. As presented in a recent review of SDM in long-term care facilities, there is limited evidence on incorporating and respecting patient preferences of persons with varying cognitive impairments (Daly et al., 2018).
Although SDM is not explicitly mentioned within the Model, the categories or topics that emerged from this review incorporating SDM are consistent with critical components of the Model. For example, the scoping review category of health promotion included topics including medical management (medication use), activities of daily living, and detection and diagnosis (diagnostic testing). There was overlap among Model categories of transition and coordination of services, assessment and care planning, and supportive and therapeutic environment with the review categories of advanced care planning and end-of-life care. The purpose of this review was not intended to create similar categories to those of the Model; however, it is interesting that the categories or topics that emerged from this review are consistent with the AA Person-Centered Delivery Model for persons living with dementia. This review provides evidence that there have been evidence-based attempts to use SDM for various topics of interest in the care of persons living with dementia. SDM can be a critical component in communication for person-centered care, as supported by SDM practices or approaches by patients, caregivers, and healthcare providers.
There is a general lack of experimental research on SDM for persons with dementia. Most of the articles retrieved were qualitative studies with small sample sizes, and mixed-method studies were likely to be pilot studies focused on instrument creation or program evaluation. Overall, limited evidence was available across any topic to provide generalizable findings outside of the individual study samples. SDM tools were created and used in eight articles, but none provided critical evidence of validity and reliability. Tools for SDM could provide the framework and guidance necessary for healthcare providers to provide options for persons with dementia and their families as well as increase family and provider confidence in decision making. There should be targeted efforts to develop and test evidence-based SDM tools or frameworks to ensure patient and family preferences are incorporated into the current care and future decisions.
Limitations
There are limitations to conducting a scoping review. Although we systematically searched the literature to answer the research question, the purpose of the review is limited to describing the current state of the science. Categories of similar decisions in this population and SDM approaches are presented, but as a scoping review, the intent was to have broader scope and “more expansive inclusion criteria” to describe what is currently known about SDM in dementia (Peters et al., 2020). Our diverse findings coupled with the overall purpose of the scoping review support the need for targeted future efforts to develop tools and use SDM for persons with dementia, families, and healthcare providers.
Conclusion
Our findings demonstrate a lack of validity and reliability in SDM tools and approaches to engage persons with dementia and caregivers in SDM. Although our review found that SDM in this population has spanned three continents, the variability in methodological approaches and outcome measures indicates the need for tools to promote patient communication of values and choices, even as cognition may decline. Our decision to place the person living with dementia at the center of all decision-making and finding similar categories emerged from the scoping review was consistent with the AA Person-Centered Delivery Model for persons living with dementia. Refining new tools and conducting psychometric studies addressing the same AA Model topics identified as the categories of the review are vital to person-centered care delivery in persons with dementia are critical to moving this field forward. Future research should include more robust efficacy testing of decision-making tools, incorporation of evidence-based SDM approaches based on cognitive status/diagnosis, and consideration of geographical/cultural differences in healthcare delivery systems. Clinicians should include persons with dementia, families, and healthcare providers in shared decision-making to promote patient and family satisfaction.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the National Institute on Aging of the National Institutes of Health under Award Number K76AG074942. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.