
Abstract
Background
Parents with dementia require emotional, physical, psychological and financial support from their child caregivers to continue living at home. Daughter caregivers have been shown to be more involved in self-care and household tasks and to experience higher levels of distress than son caregivers.
Objective
The aim of this study was to investigate the experience of daughter caregivers who provide informal care for a parent with dementia living in their own home.
Method
Semi-structured interviews were conducted with 11 daughter caregivers of a parent with Alzheimer’s disease. Interviews were analysed using Interpretative Phenomenological Analysis.
Results
Three axes emerged from the analyses: [1] the before conditions the after: the quality of the previous relationship with the parent with Alzheimer’s disease is a determining factor and allows the identification of three profiles of daughter caregivers: ‘the grateful’, ‘the resentful’ and ‘the ambivalent’, [2] when the relationship protects against the sense of burden: the feeling of being invaded by the caregiving situation is influenced by the quality of the relationship with the parent with Alzheimer’s disease, and [3] alone or almost: the support network is desired when it is absent but kept at arm’s length when it is present.
Discussion
The results underline the importance of assessing the quality of attachment and supporting the relationship with the parent (especially when the relationship prior to the disease was difficult). Daughter caregivers should also be encouraged to delegate tasks and refocus their actions related to their values. Family mediation sessions may be planned to improve the organisation of care and set up an efficient collaboration.
Keywords
Introduction
Supporting parents with dementia to help them continue living in their own home requires a significant emotional, physical, psychological and financial investment from child caregivers (Barca et al., 2014; Shim et al., 2011; Van der Lee et al., 2014). With the progressive loss of cognitive and executive functions, child caregivers have to take on various tasks (e.g., help with transportation, housekeeping, mobility assistance, hygiene, etc.), which leads them to focus increasingly on their parents with dementia (Chiao et al., 2015; Huang et al., 2015; Kjällman-Alm et al., 2013). This level of involvement is even more burdensome as they have to juggle their own marital, parental and professional obligations (Kjällman-Alm et al., 2013; Vinas-Diez et al., 2017). Helping their parent thus becomes an additional task to assume in their daily routine (Wawrziczny et al., 2020), which needs to be readjusted to meet the needs of the parent with dementia (Habermann et al., 2013).
Previous studies have shown that various individual, relational and social factors may affect the experience of the caregiving situation and the level of distress of child caregivers. Health problems (depression, high blood pressure and heart problems) are major predictors of distress in child caregivers (Holland et al., 2011; Wawrziczny et al., 2020, 2021). Furthermore, helping one’s parent can become a source of stress when it is motivated by a sense of obligation, duty or loyalty (extrinsic motivations), thus leading to the feeling of being forced into the caregiving role (Conde-Sala et al., 2010; Dombestein et al., 2020; Ducharme et al., 2011; Pinquart & Sörensen, 2011). Intrinsic motivations such as reciprocity of parental love and care during childhood are associated with greater satisfaction (Pinquart & Sörensen, 2011). Raccichini et al. (2009) also showed that child caregivers living in with their parent with dementia felt a greater sense of burden than those who did not. However, the latter felt more guilty about not doing enough and showed more depressive symptoms, especially when they lived far away or when they had received love, support, care, and devotion from their parent during childhood (Conde-Sala et al., 2010; Li et al., 2019; Wawrziczny et al., 2021).
The involvement and experience of child caregivers may be predicted by the quality of the past and present relationship with the parent with dementia. A positive relationship during childhood is associated with a better perception of the present relationship, fewer feelings of being overwhelmed or distressed about the caregiving situation, greater motivation to take care of the parent with dementia and better communication with them (Habermann et al., 2013; Smith & Rodham, 2022). A good present relationship also limits the sense of burden and encourages continued caregiving (Shim et al., 2011). Conversely, child caregivers who felt little affection in their childhood may experience more distress and pressure in their caregiving role with their parent with dementia (Daire, 2002; Habermann et al., 2013; Quinn et al., 2009).
Child caregivers are rarely prepared for their parent’s dependence on care. Caring for a parent with dementia involves responsibilities that go beyond what is socially expected of them (Conde-Sala et al., 2010; Habermann et al., 2013). Roles become inverted and children have to act on behalf of their parent with dementia (Kjällman-Alm et al., 2013). They may also feel frustrated by the poor consideration of their own needs by health institutions (Barca et al., 2014; Kjällman-Alm et al., 2013). They often lack information about the disease and its treatment to understand their parent’s behaviours and needs, and do not feel competent enough to manage the situation (Fowler & Fisher, 2009; Kjällman-Alm et al., 2013). Tolkacheva et al. (2011) also showed that disruptions and coordination problems within the network may cause additional stress, whereas a functional care network can potentially reduce the burden on child caregivers. Preparing in advance may help child caregivers to feel better prepared and more efficient, and parents to reduce their depression and anxiety (Fowler & Fisher, 2009). Child caregivers may also feel neglected by their families (Barca et al., 2014; Kjällman-Alm et al., 2013), as they may face family conflicts related to sharing their role with their siblings (Kwak et al., 2012; Ngangana et al., 2016; Tatangelo et al., 2018). These conflicts may be exacerbated by difficult family dynamics prior to the parent’s disease, but they are also a significant source of interpersonal stress for children, thus impacting their ability to cope with the demands of their parent with dementia (Tatangelo et al., 2018).
Among these studies, most are quantitative and the few qualitative studies investigate the experience of son and daughter caregivers indiscriminately (Barca et al., 2014; Dombestein et al., 2020; Habermann et al., 2013; Kjallman-Alm et al., 2013; Tatangelo et al., 2018; Zimmermann, 2013). However, previous studies showed that daughter caregivers experience higher levels of distress, exhibit stronger correlations between burden and mental health (anxiety, depressive symptoms and difficulties in social relationships), are more involved in self-care and household tasks and receive less professional support to help them than son caregivers (Chumbler et al., 2003; Conde-Sala et al., 2010; Yee & Schulz, 2000). Until now, only three qualitative studies have focused on the experiences of daughter caregivers (Day et al., 2014; Legault & Ducharme, 2009; Smith & Rodham, 2022), two of which involved the parent with dementia living at home (Day et al., 2014; Smith & Rodham, 2022). These two studies explored risk factors for compassion fatigue in the daughter caregivers (Day et al., 2014), as well as identity and relationship changes related to role reversal, competing demands of multiple roles and difficulties in seeking support (Smith & Rodham, 2022). Using a qualitative approach, the present study thus aims to expand the knowledge about the experiences of adult daughter caregivers who provide informal care for a parent with dementia living in their own home.
Method
Participants
Participants were recruited over a two-year period on a respite platform and in day care centres in the Hauts-de-France region. The inclusion criteria were to be a daughter who was the main caregiver of a parent with Alzheimer’s disease. The latter had to live in their own home. We focused on Alzheimer’s disease to homogenize our sample as it is the most common form of dementia. The interviews were conducted and analysed using the Interpretive Phenomenological Analysis (IPA) method developed by Smith et al. (2009). Since IPA involves an in-depth understanding of participant’s experience of a given phenomenon, a small and homogeneous sample is recommended (i.e., between 1 and 20 participants) (Antoine & Smith, 2017; Smith & Nizza, 2022).
Characteristics of the daughter caregivers.
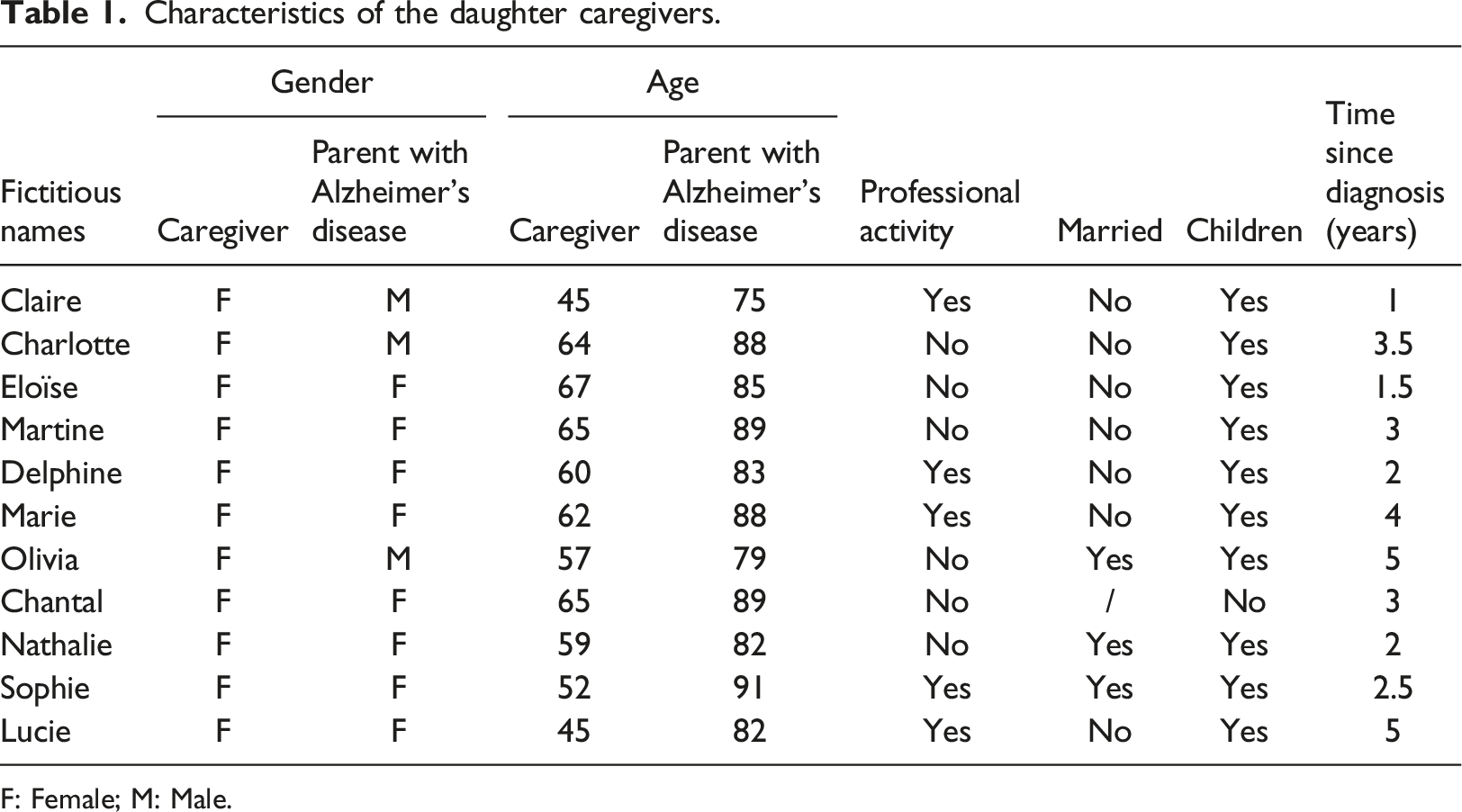
F: Female; M: Male.
Procedure and ethical issues
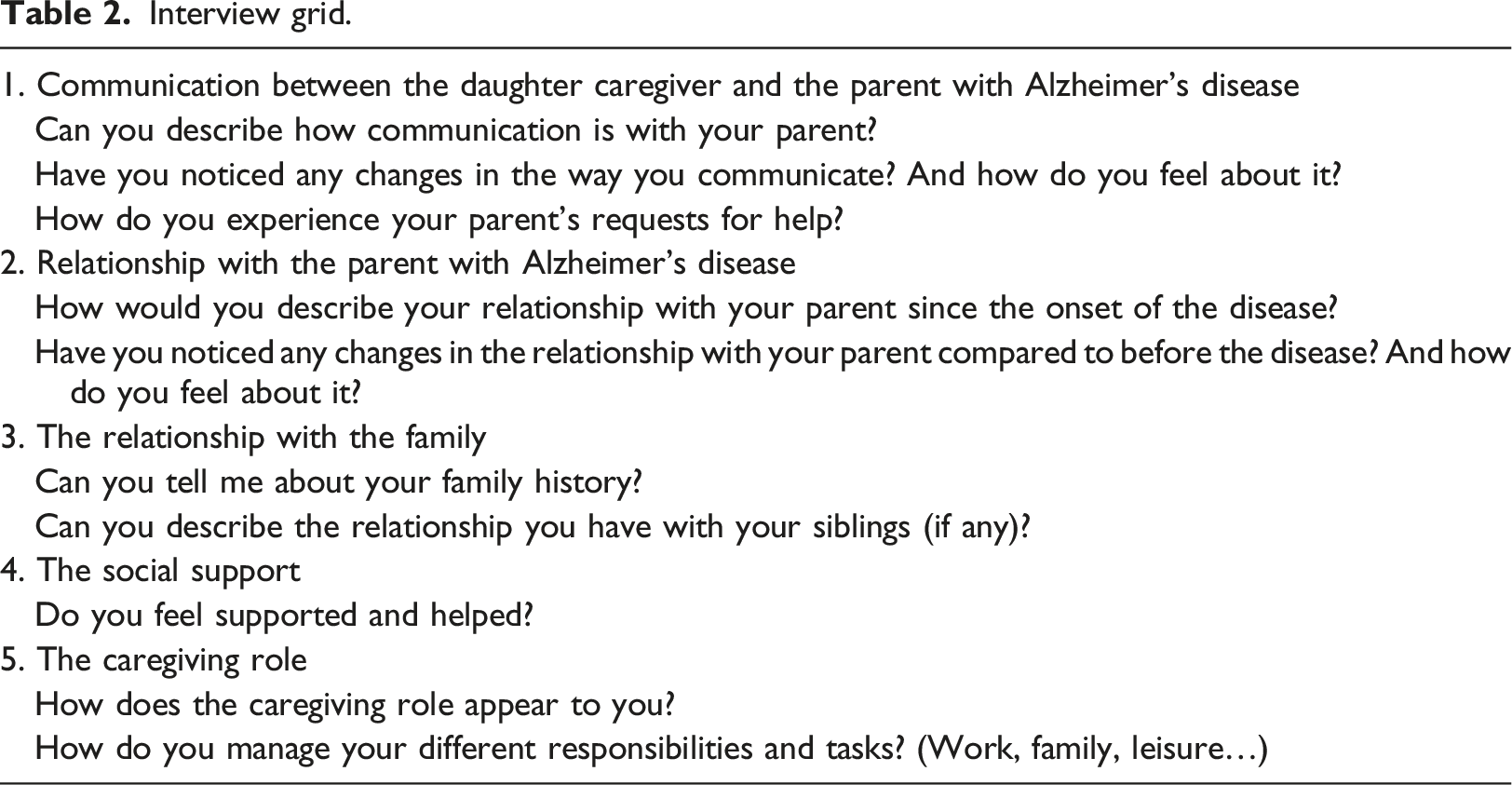
Interview grid.
Data analysis
The purpose of this study was to report the experience of daughter caregivers of a parent with Alzheimer’s disease, using an Interpretative Phenomenological Analysis (Smith et al., 2009). IPA is an experiential method developed for a detailed understanding of people’s experience with phenomenological, hermeneutic and idiographic theoretical underpinnings (Smith et al., 2009). Phenomenology is a philosophical approach used to understand the subjective experience of a given phenomenon. It involves double hermeneutics, which relies on the theory of interpretation and involves a co-construction of meaning by both the researcher and the participant. The researcher interprets the participant’s interpretation of their experience, prompting him to delve deeper into the participant’s discourse while putting aside his presuppositions about the participant’s experience. IPA is also idiographic as each interview is analysed as a case, focusing on how a specific phenomenon is experienced and understood by a particular person in a particular context (Smith et al., 2009).
The interviewer was trained in interviewing and qualitative analysis and was familiar with caregiving in neurodegenerative diseases. During the entire study, the interviewer, who was aware of the significant impact of subjectivity in IPA, adopted a reflexive attitude. The interviewer was particularly careful to set aside her knowledge on the matter and any presuppositions about the participant’s experience (Smith & Nizza, 2022). Following the recommendations of Nizza et al. (2021), each interview was analysed and interpreted by two researchers, first individually and then conjointly. They analysed the experience of each daughter caregiver line by line. By paying particular attention to the vocabulary and expressions used to describe their experience and the associated feelings and emotions, researchers gained access to the meaning of the caregivers’ experience and to the psychological mechanisms. The identified processes and salient elements were schematized, thus allowing the researchers to discuss their interpretations and densify their analysis. As they were aware of the potential bias of their own opinions and feelings, the discussion between them was also a way to share their perceptions of the interviews and ensure reflexivity.
Each case was analysed following the same process. All the analyses were then compared to identify the similarities and differences in the way the participants’ experiences were expressed. The researchers finally produced a general synthesis of the identified processes underlying the daughter caregivers’ experiences, which helped to define themes.
Results
Three themes were identified: ‘The before conditions the after’, ‘When the relationship protects against the sense of burden’, ‘Alone, or almost’. The first theme described different profiles of daughter caregivers. The second one explored the objective and subjective aspects of the daughter caregivers’ feeling of burden. Finally, the third theme illustrated the difficult adjustment with relatives. These themes are detailed and supported by examples from the interviews.
The before conditions the after
The pre-disease relationship with the parent with Alzheimer’s disease was found to condition the way the caregiving relationship is perceived and experienced, the involvement and motivations in the caregiving role and the level of adjustment and communication. Three profiles of daughter caregivers emerged regarding the quality of the relationship with the parent prior to the disease: ‘the grateful’, ‘the ambivalent’ and ‘the resentful’.
The grateful
Chantal, Martine, Olivia and Sophie explained that they always had a good relationship with their parent with Alzheimer’s disease and that they were grateful for it. They always felt supported. Martine said "They really supported me. Both morally and financially, they supported me”. This relationship was a strength on which the ‘grateful’ relied to manage their parent’s disease. Sophie even said that "the relationship is better than before, because I am really closer to her". The question of help thus came naturally as a fair return for what they had received. Sophie added: "It’s normal. When I was a little girl, I told her, ‘You take me for a walk in my pushchair, and when I’ll grow up, I’ll take you for a walk in the pushchair too'“. However, the disease was all the more difficult to live with because it triggered a succession of losses of what constituted the personality and identity of their beloved parent. Olivia explained: “You don’t understand what’s going on, it’s someone else, it’s not your daddy anymore”. However, they tried to adjust their communication while being attentive to the well-being of their parent with Alzheimer’s disease. “It’s not always easy, but you have to be able to tell him… but when are you going to tell him because there are times when Daddy is not very well.” (Olivia)
The ambivalent
Charlotte, Claire and Delphine described a better relationship with their parent with Alzheimer’s disease since the onset of the disease, even if communication became increasingly limited. The relationship evolved from an authoritarian and confrontational dynamic to a more uninhibited and joyful one, allowing each one to rediscover the other. Charlotte explained: “He got to know me, I like that”. However, they regretted not having experienced this relationship before. Claire said: “I feel it is too late because I am an adult. I mean, as a child, I would have liked to have a father like he is now”. This relational dynamic before the disease was very marked by the notion of the roles of parent and child. The parent’s progressive loss of autonomy and the increased responsibilities for the daughter caregivers were experienced as a role reversal, causing a disruption of identity markers. Charlotte said of her parent with Alzheimer’s disease: “He is more and more my child”. This perception of an authoritarian infallible parent was thus turned upside down by the disease. Delphine explained that “Our parents are the pillars in our lives, and we feel like these pillars are collapsing”. This challenged the deepest beliefs of the daughter caregivers, going as far as questioning what had previously defined them, their own identity: “It’s difficult for me because everything is being questioned: my education, my family life, my personal choices. I live alone with my daughter, I made personal choices that were guided by the education I received, which was quite authoritarian, etc. You build yourself by what you have received and now, suddenly, what I have received, I realise that my father, how can I put it… it’s as if it didn’t make sense (...) it’s as if I had believed in God and suddenly, I see that God doesn’t exist.” (Claire).
The resentful
Eloïse, Lucie, Marie and Nathalie described their relationship with their parent before the disease as conflictual. Lucie explained: “I was always in conflict with my mother.” Although they would have liked to escape the situation (Nathalie: “There was a period when I didn’t go there anymore”), they felt obliged to fulfil their role as caregivers because they were the only ones who could do so. The relationship with the parent with Alzheimer’s disease was described as mechanical and emotionally distant. They claimed not to expect anything in return, as if to protect themselves and avoid being disappointed. Eloïse said: “I have never had any recognition from my mother, I’m not going to get it today.” For some of these daughters, it was an opportunity to regain the upper hand in the relationship. While Eloïse sought to assert herself by saying “I’m not her kid who is being manipulated anymore,” Marie sought to take control with a devaluing behaviour tinged with rejection. “ I tell her to fuck off, I say listen you’ve always told me to fuck off, so I say I don’t need you […] I tell her she looks like a fool, so I say “you look like a fool! I’m going to take a photo of you.” And then I show her the picture” (Marie)
When the relationship protects against the sense of burden
All the daughter caregivers felt constantly preoccupied and invaded both mentally and physically by the caregiving situation, like Sophie who said she felt “overwhelmed.” This feeling could be amplified by the geographical distance and/or the health problems inherent, or not, to the caregiving situation. While Chantal reported that “driving is exhausting,” Claire and Eloïse described sleep disorders caused by their anxiety: “at night you have dreams, nightmares… the life of a caregiver really is horrible” (Eloïse). Martine’s doctor even diagnosed exhaustion in her.
This feeling of invasiveness was influenced by the number of tasks to be done and the amount of time spent helping, but also by the ability of the daughter caregivers to take time for themselves and delegate. Martine said: “I go three times a day, we don’t live very far from each other.” This level of commitment to the caregiving situation forced Claire, Eloïse and Martine to abandon personal projects or activities due to the lack of time. However, while Chantal, Claire, Delphine, Lucie, Martine, Nathalie and Olivia were able to delegate certain tasks when they needed to, Eloïse, Marie and Sophie were unable to do so. Eloïse’s mother refused to accept anyone else’s help, while Marie and Sophie did not want to entrust their parent to other people because they did not trust the quality of care and wanted to retain control. Unable to be constantly present, Sophie set up cameras in her parent’s home and watched the videos regularly, and Marie installed a GPS system on her mother’s keys to monitor her whereabouts. While these devices helped monitor the safety of the parent with Alzheimer’s disease, they also allowed permanent access to his or her privacy, which could be embarrassing for the parent. They also kept the daughter caregivers constantly connected to their parent with Alzheimer’s disease, thus reinforcing the feeling of invasiveness. “If I’m going away, I’ve got the camera and with my phone I can connect from anywhere...so it’s good because I can see her.” (Sophie) “I have a GPS on my mum’s keys so the good thing is that as soon as she leaves, if she leaves at night or at any time, I am warned.” (Marie)
This feeling of invasiveness was also influenced by the emotional burden of the caregiving situation and the quality of the relationship with the parent. For Eloïse, Lucie, Marie and Nathalie, a quick weekly visit to provide technical assistance was already experienced as burdensome. Marie confided: “After a while I get fed up! I feel like my life has no meaning. My life revolves around my mother and I can’t get out of it.” Providing help was thus experienced as a struggle, as an obligation in a negative relational context.
For Chantal, Charlotte, Claire, Delphine, Martine, Olivia and Sophie, their involvement was more frequent, even sometimes daily. In a more positive relational context, helping their parent with dementia was thus motivated by the desire to do well and to make the best possible adjustments. Chantal explained: “I can see that her daily activities are getting worse, so I have to invent new things.” Daughter caregivers felt valued and aware that their help was essential for allowing their parent to stay home.
« I reassure myself […] I think that if I hadn’t worked like that, she would have left a long time ago […] I tell myself that if I hadn’t done all of this… I’m proud of myself. She has reached this age thanks to me. » (Sophie)
Alone, or almost …
Chantal and Delphine received satisfactory support from their siblings in the continuity of the relationship prior to the disease, which kept building up as the disease progressed. Delphine explained that everyone contributed to the parent’s care in their own way: “With my brothers, it’s really great because we support each other. We don’t provide the same sort of support at all.” For Charlotte, Claire, Lucie, Olivia and Sophie, their siblings were more distant. Olivia said she suffered from this absence: “I felt abandoned and I was indeed,” like Sophie. Charlotte, Claire and Lucie voluntarily kept their siblings at a distance, either to protect them (cf. Claire below), or to avoid conflicts linked to care decisions and to preserve the sibling bond. Lucie explained: “I’m going to lose my brothers and then, when something happens to my mother, I’ll be all alone.” Whether desired or not, the absence of their siblings caused them to feel very lonely. « She (her sister) never had a good relationship with our father, so she is less inclined to be there. So at the moment she’s not there [...] I've talked to her (her sister) a lot about it, she’s very aware of it, she's very responsive, if I tell her to come she'll come.» (Claire)
Like Marie, who felt “supported,” Charlotte, Claire, Delphine, Lucie and Sophie explained that they found comfort in their friends or children. However, when they felt their anxiety, they avoided sharing too much or were careful about what they said. Sophie reported her daughter’s words: “We are afraid for you. You’re not careful enough about all this, you’re going a bit too far with grandma.”
Chantal and Olivia explained that they did not rely on other people, either to maintain the image of someone strong who can manage alone or for fear of disturbing people. Olivia explained that although she had people who loved her, “not everyone is able or willing to hear.” Nathalie, Olivia and Sophie also said that support was potentially an additional source of stress. They considered that they were not always understood and sometimes felt torn between their parent with Alzheimer’s disease and their own partner. As Olivia put it: “My husband went away for ten days in August and left me, he couldn’t stand it anymore. So, he left the house, he went to a hotel for about ten days. Everything collapsed.”
Discussion
The objective of this study was to explore the experience of daughter caregivers of a parent with Alzheimer’s disease to better understand their needs and difficulties. Three main results were found: [1] the quality of the relationship with the parent with dementia prior to the disease is decisive, [2] the quality of relationship with the parent with dementia impacts the perception of the burden, [3] their attitude towards their entourage is ambivalent.
The quality of the relationship with the parent with dementia prior to the disease is decisive
The findings of this study corroborated previous ones showing that the care relationship is affected by the relationship with the parent with dementia prior to the disease. The experience and the perception of the caregiving situation, as well as the involvement and the motivations to help, are also conditioned by this past relationship (Chen & Bailey, 2018; Daire, 2002; Pinquart & Sörensen, 2011; Shim et al., 2011). Merz et al. (2009) noted that the quality of the relationship was the strongest predictor of the well-being of the child caregiver and that of their parent with dementia. Quinn et al. (2009) added that a better understanding of the role of the quality of the previous relationship would help in developing more effective interventions for caregivers.
The specificity of our results is to have identified three profiles according to the quality of this past relationship: the ‘grateful’, the ‘ambivalent’ and the ‘resentful’ daughter caregivers. For the ‘grateful’ daughter caregivers, a positive past relationship and gratitude towards their parent gave them the strength to manage the disease and maintain their motivation. They also experienced a form of closeness and the feeling of a reinforced affective bond with the time spent together. Previous studies also showed that some caregivers perceived advantages in the changes caused by the disease, such as a greater emotional and relational closeness, a strengthening of the bond and a richer relationship (Wawrziczny et al., 2016). Both past and present relationships thus serve as a protective resource in a caregiving context (Browne & Shlosberg, 2006; Nelis et al., 2014; Smith & Rodham, 2022).
For the ‘resentful’ daughter caregivers, a negative past relationship was a negative determinant of the caregiving relationship, which was seen as an obligation. Daire (2002) and Lee et al. (2018) showed that child caregivers who reported perceiving less affection and insecure attachment in their childhood tended to feel more distress and burden in their role as primary caregiver to their parent with dementia. Chen and Bailey (2018) also observed that a conflicted childhood relationship based on aggressiveness and intolerance could lead to a misperception of the emotions of the parent with dementia as being intentionally hostile. This could then have repercussions on the quality of the caregiving involvement, and cause relational conflicts, critical attitudes and tensions towards the parent with dementia. Our results also showed that tensions might arise when daughter caregivers felt in a position of strength or power regarding their dependent parent. Out of anger or revenge, they might resort to aggressive, hurtful or even violent language and behaviour towards their parent with dementia.
The ‘ambivalent’ daughter caregivers appeared as an intermediate profile. The disease impacted the capacities of their parent with dementia, but also attenuated their strong authoritarian personality. These changes led to both a disruption and reshaping of identity markers, but also laid the foundations for a new, more peaceful, positive relationship.
For all these profiles, the changes in the parent’s identity and role imposed by the disease had emotional and relational consequences. Wawrziczny et al. (2016) already showed that spouse caregivers and spouses with dementia no longer recognised each other and experienced a feeling of loss and nostalgia. In this study, the positive commitment in the caregiving relationship and the greater closeness to the parent with dementia of the ‘grateful’ daughter caregivers might have made it more difficult to accept losses, especially identity losses (no longer recognise the personality of their beloved parent). For the ‘ambivalent’ and the ‘resentful’ daughter caregivers, the loss of the parent with dementia’s capacities and dependence had an impact on the asymmetrical relationship that they previously had with their parent. For the ‘ambivalent’, the previously authoritarian yet respected parental image weakened by the disease gave way to a more positive relationship dynamic, while for the ‘resentful’, their parent’s decline offered an opportunity to take power and control over the relationship.
The quality of relationship with the parent with dementia impacts the perception of the burden
The results showed that daughter caregivers felt physically and psychologically invaded by the caregiving situation, which caused distress. For most of them, this feeling of being overwhelmed was directly related to the number of daily tasks and responsibilities that they had to manage at the expense of their personal life and leisure time. Their personal equilibrium was affected by the hours dedicated to caregiving (Kim et al., 2012; Liu et al., 2019) and by the constant worry towards the parent with dementia (Kjällman-Alm et al., 2013). Daughter caregivers divide their time between work, family life and supporting their loved one (Rigby et al., 2019). The additional responsibilities created by the caregiving situation strained an already complex set of relationships and demands on caregivers' time and energy, leading to a declining sense of control over their own environment and significantly affecting their physical and mental health (Cao & Yang, 2020; Seltzer & Li, 2000). They also found it difficult to delegate as they felt as if they were abandoning their parent by doing so or as if they were the only ones able to provide quality care. They thus became resistant to outside help. They never took a break and they gave up their leisure activities. This difficulty in letting go and their need to feel in control reinforced the physical and mental invasiveness of the caregiving situation in their daily lives.
Interestingly, this feeling of invasiveness might be moderated by the quality of the relationship. While some of them (mainly the ‘resentful’) felt a strong sense of invasiveness, the objective burden was low. Wawrziczny et al. (2017) already showed that the quality of the relationship could influence the severity of the symptoms as perceived by the caregiver: the poorer the quality of the relationship, the more the caregivers perceived the symptoms as severe. In the present study, a difficult relationship with the parent with dementia made the caregiving situation more burdensome and invasive than it objectively was. Help was underpinned by extrinsic motivations and experienced as a struggle. Conversely, the results underlined the potentially protective role of the parent/child relationship which, when positive, mitigated the negative impact of the daily burden. Daughter caregivers then felt recognition and a sense of usefulness that boosted their motivation to support their parent with dementia. This underlined the importance of considering the quality of the past relationship into account when assessing caregivers’ burden.
Their attitude towards their entourage is ambivalent
When relatives were absent
While a minority of the daughter caregivers in the study felt satisfied with the relationship with their siblings, most of them deplored the quality and quantity of the informal support they received and had an overall feeling of loneliness. While some siblings intentionally stayed away when it came to supporting the parent with dementia (Smith & Rodham, 2022), many daughter caregivers tended to isolate and to refuse help. This intentional distancing aimed at maintaining control over the care situation and preventing others from interfering in care decisions in the same way as spouse caregivers or not becoming a burden to others and disturbing them (Au et al., 2009; Peisah et al., 2006; Pinquart & Sörensen, 2006; Wawrziczny et al., 2020).
When family and friends were present
Daughter caregivers may have felt caught up in a loyalty conflict between their parent with Alzheimer’s disease and their own children and spouses, as caregiving often took place in the context of multiple family relationships (Gaugler et al., 2018). The feeling of burden was often linked to difficulties in balancing the demands of their caregiving role with their roles as mothers and wives (Kjällman-Alm et al., 2013; Smith & Rodham, 2022). Unlike Seltzer and Li (2000) who found that the relationships of daughter caregivers with their husbands and children remained unchanged during caring, our results showed that family and couple might become an additional source of tension.
Limitations
This research had several limitations. While other authors found gender differences in the experience of being a child caregiver, our sample was entirely composed of women due to the aim of the study. Indeed, a similar study is now required which focuses on the experience of sons. In addition, our daughter caregivers did not live with their parent, so it would be interesting to observe the impact of living with the parent. Finally, our results only reflected the subjective experience of one member of the parent/child dyad. It would be relevant to also study the experience of the parent with dementia.
Clinical implications
This study highlighted the uniqueness of the experience of daughters caring for a parent with dementia. First, the results demonstrated that the quality of relationship with the parent with dementia (prior to the disease and the caregiving relationship) was a determining factor of the caregiving experience and the perceived sense of burden. It would then be relevant to evaluate the quality of attachment of daughter caregivers with their parent with Alzheimer’s disease. Psychotherapy would also permit to identify the unconscious relational scripts of the daughters caregivers, and modify them to find internal security and work on the present bond with the parent with dementia. To encourage the best possible adaptation of the daughter caregiver/parent with Alzheimer’s disease dyad to the care needs associated with the progression of the disease, it would be useful to support them in a process of co-construction from an early stage, to prepare for the changes and the new relationship. The diagnosis period is a pivotal moment when caregivers and the relatives they care for can plan how they will organise future care (Robinson et al., 2005; Whitlatch & Feinberg, 2003).
Second, daughter caregivers should also be supported in their role transition with more preparation and knowledge to develop confidence and coping strategies (Meleis et al., 2000).
Third, the caregiving tasks become more numerous and varied as the disease evolves. They add up to family, professional and social tasks, particularly when the caregivers do not live with their parent and are women (Pinquart & Sörensen, 2006). Moreover, family caregivers sometimes feel that the offered support does not meet their needs (accessibility, location, costs, opening hours, etc.) (Mast, 2013). It is therefore essential to create the conditions to enable them to manage all these tasks with greater flexibility at work (e.g., flexibility in the number of hours worked, flexible working hours), better information on professional, community or peer support networks, a facilitated access to day care or respite services, financial aid and transportation to medical appointments. Daughter caregivers also need support based on Acceptance and Commitment Therapy (ACT) to ease up on control, become more flexible and identify their important values and needs, in order to accept help, delegate tasks and refocus their actions related to these values and needs (e.g., health needs) (Harris et al., 2012).
Fourth, daughter caregivers could explore the personal support available to them. Family mediation sessions could also be offered to help family members, especially siblings, to better understand the disease and re-allocate responsibilities.
Footnotes
Acknowledgements
We would like to thank all the caregivers who participated in this study, as well as the respite platforms and the day care centres in the region of Hauts-de-France for their help in this study. LabEx (Laboratory of Excellence) DISTALZ (Development of Innovative Strategies for a Transdisciplinary approach to Alzheimer’s disease) supported this research. Special thanks to Julie Naveaux, Vinciane Leduc, and Honorine Pourrier for their involvement in this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.