
Abstract
Keywords
Introduction
More than 55 million people are living with dementia globally, and the number is estimated to triple by 2050 (GBD 2019 Dementia Forecasting Collaborators, 2022). In the United States, more than 6 million Americans live with Alzheimer’s disease and related dementias (Alzheimer’s Association, 2022). The timely diagnosis of dementia is a healthcare priority and a goal of the United States National Plan to Address Alzheimer’s Disease (Alzheimer’s Association National Plan Care and Support Milestone Workgroup et al., 2016). For patients with dementia, studies reveal the benefits of receiving a timely and comprehensive diagnosis, including access to medical and social services, opportunities to discuss disease-modifying therapies (if appropriate), and engagement in advance care planning (Anantapong & Davies, 2021; Burgdorf & Amjad, 2023; Dubois et al., 2016). Despite the benefits, more than half (58.7%) of adults aged ≥65 with probable dementia from the US National Health and Aging Trends Study are undiagnosed or unaware of the diagnosis (Amjad et al., 2018). Furthermore, the diagnosis of dementia is often delayed beyond the early stages, in particular for individuals from racial and ethnic marginalized communities who are less likely to receive a timely and comprehensive diagnosis (Chrisp et al., 2011; Lin et al., 2021; Woods et al., 2019).
Clinician barriers to communicating a dementia diagnosis contribute to missed or delayed diagnoses and to negative experiences for patients and caregivers (Bradford et al., 2009; Low et al., 2019; Yates et al., 2021). The professional background of clinicians who deliver a dementia diagnosis varies within and between countries. In the European Union, for example, diagnoses are often given by psychiatrists or geriatricians in Sweden, whereas dementia diagnoses may be conducted and communicated by neurologists or geriatricians in France (Hlavka et al., 2018). Within the United States, one study of Medicare beneficiaries demonstrated that nearly 85% of initial dementia diagnoses were made by a non-dementia specialist (majority were primary care/family medicine) (Drabo et al., 2019). A different study using electronic health record data revealed that about two-thirds of patients received a diagnosis from dementia specialists (neurology, geriatrics, geriatric psychiatry) (Nguyen et al., 2022).
Regardless of professional background, clinicians report challenges with disclosing a dementia diagnosis. Fewer than one third of primary care physicians report feeling highly confident in making and communicating a dementia diagnosis (Bernstein et al., 2019). Dementia specialists (e.g., neurology, geriatric psychiatry) describe challenges with delivering difficult news and communicating prognosis and uncertainty (Milby et al., 2017; Wollney et al., 2022a; Yates et al., 2021). In addition, clinician fear of emotionally harming patients or uncertainty about the diagnosis contribute to avoidance of, or hesitation in, directly disclosing a diagnosis to patients and the use of ambiguous terminology in some instances (Bailey et al., 2019; Caruana-Pulpan & Scerri, 2014; Kaduszkiewicz et al., 2008; Nielsen et al., 2020; Segers, 2009; Vince et al., 2017). Furthermore, patients and caregivers describe unmet needs at the time of a dementia diagnosis, including inadequate anticipatory guidance and inattention to the emotional impact of the diagnosis (Byszewski et al., 2007; Jennings et al., 2015; Shafir et al., 2022). Variation in patient cognitive capacity to retain and process information, and the underlying stigma that accompanies dementia, add additional complexity to diagnostic communication (Parker et al., 2020; Sagbakken et al., 2018).
Most clinicians have not received formal training in disclosing this or other serious diagnoses to patients and caregivers (Caruana-Pulpan & Scerri, 2014; Yates et al., 2021). While there are national clinical guidelines about diagnostic disclosure communication in different countries (Alpinar-Sencan & Schicktanz, 2020; Armstrong et al., 2024; NICE Guideline, 2018), few evidence-based, structured interventions for person-centered diagnostic disclosure conversations for dementia target clinician communication skills. We aimed to investigate specific clinician communication skills, strategies, and challenges with diagnostic disclosure of dementia as an initial step in our goal of co-designing a structured communication intervention with patients, caregivers, and clinicians. The overall objective is to design and test a structured intervention that improves communication quality and patient and caregiver experience and outcomes at the time of a dementia diagnosis.
Methods
Study design
We conducted a qualitative study using semi-structured interviews with healthcare professionals in neurology, geriatrics, geriatric psychiatry, neuropsychology, primary care and family medicine. The Mass General Brigham Institutional Review Board approved this study (Protocol #: 2023P000181). All participants provided informed consent to participate.
Population and recruitment
We recruited a convenience sample of clinicians at 3 sites in the U.S. using an email study invitation that included a study fact sheet. Sites included two academic medical centers in Massachusetts and one academic medical center that has federally qualified health centers in New York. These sites were chosen due to existing serious illness communication quality improvement efforts and to capture clinician experiences across healthcare institutions that serve racially, ethnically, and socioeconomically diverse patient populations. Clinicians were included if they were health professionals employed at one of the three institutions and practiced in specialties involved in communicating a diagnosis of dementia to patients, including primary care, family medicine, geriatrics, neurology, geriatric psychiatry and neuropsychology.
Data collection and analysis
The study team developed the semi-structured interview guide based on conceptual frameworks for person-centered serious illness communication that address the following domains: patient-clinician relationships, sharing information, eliciting information, responding to emotions, and engaging in decision-making and care planning (Sanders et al., 2018; Street et al., 2009). JP (female palliative care researcher) conducted the interviews with participants via video conference using Zoom which lasted 45–60 minutes. JP did not have prior existing relationships with most participants. Participants did not receive remuneration. JP obtained verbal informed consent from participants before the start of the interview, which was documented by the study team. During the consent process, the study team reviewed the fact sheet with participants, including: a) the goal of the study; b) that participation is voluntary and they could withdraw at any time; c) risks and benefits; and d) procedures related to data privacy and confidentiality. Interviews were audio-recorded, transcribed, and de-identified.
We used a stepwise approach to thematic analysis (Braun & Clarke, 2006; Vaismoradi et al., 2013) with a hybrid deductive-inductive method for coding. The primary analytic team included JP and HCG, a female clinical research coordinator. JP and HCG reviewed the first four transcripts and used deductive coding to develop an initial codebook based on the interview guide, which aligned with a conceptual framework on the domains of high quality serious illness communication (Tarbi et al., 2022). Deductive codes, for example, included domains such as therapeutic relationships; assessing illness understanding and information preferences; responding to emotions; sharing information; engaging in care planning. JP and HCG coded the remaining transcripts and met every five interviews to revise and add codes (inductive), resolving differences by consensus. JP and HCG met regularly to review data, discuss, and reclassify codes as appropriate. In the relationship domain, inductive codes included, for example, ‘acknowledging and honoring patient strengths’ to establish connection and rapport. We identified preliminary themes and sub-themes related to communication strategies and challenges within each communication domain through review and discussion of coded results. JP and HCG engaged two additional researchers to refine themes and sub-themes: CR (female geriatrics and palliative care physician researcher) and AS (female medical anthropologist and health policy researcher focused on dementia care). After analyzing 17 interviews, no major additional themes emerged. After conducting an additional 6 interviews, we ceased data collection as we determined that we had reached thematic saturation. The supplemental table includes themes and codes with definitions and illustrative quotes.
Findings
Participants
Clinician characteristics.
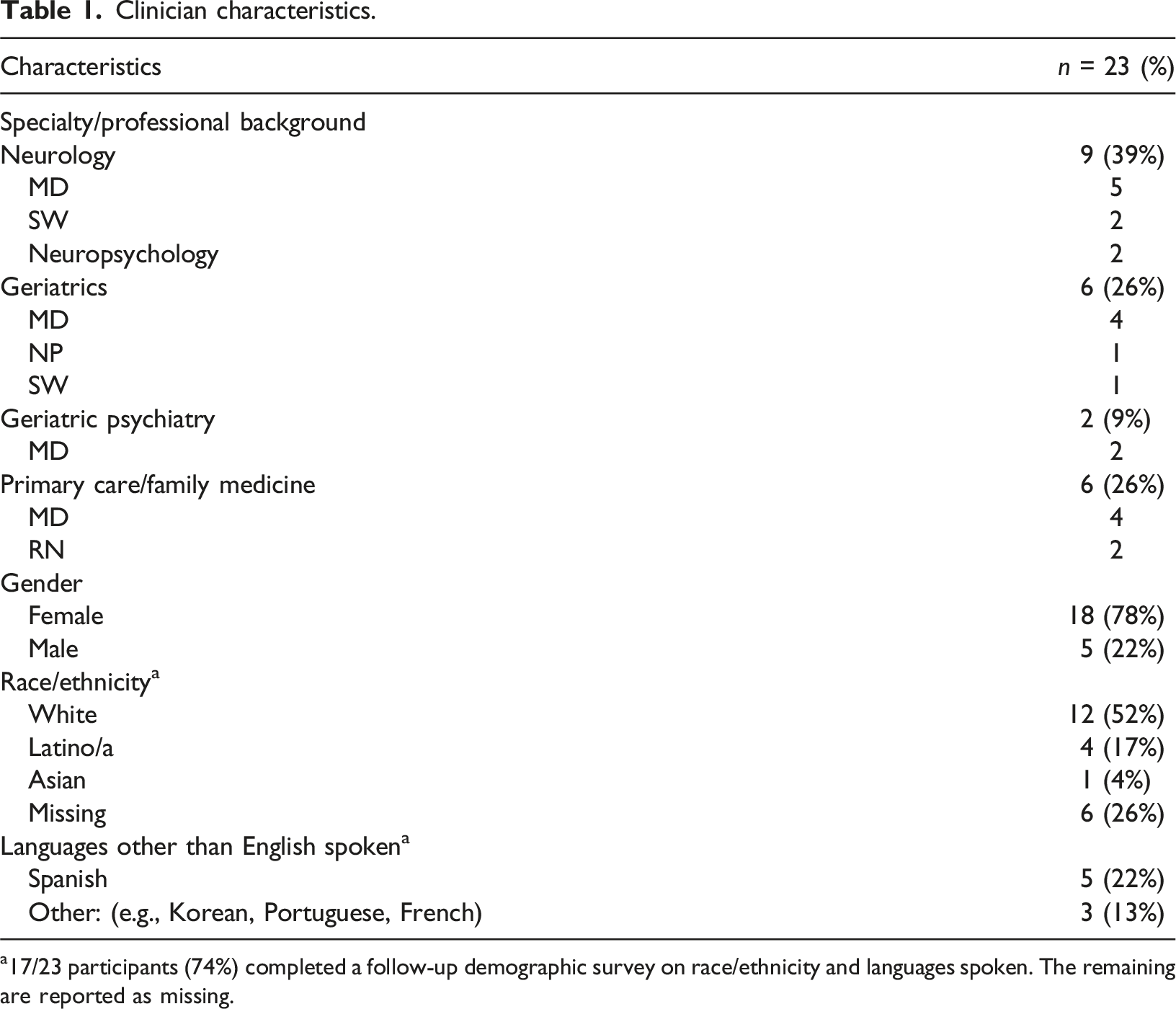
a17/23 participants (74%) completed a follow-up demographic survey on race/ethnicity and languages spoken. The remaining are reported as missing.
Qualitative findings
Communication strategies and challenges. a
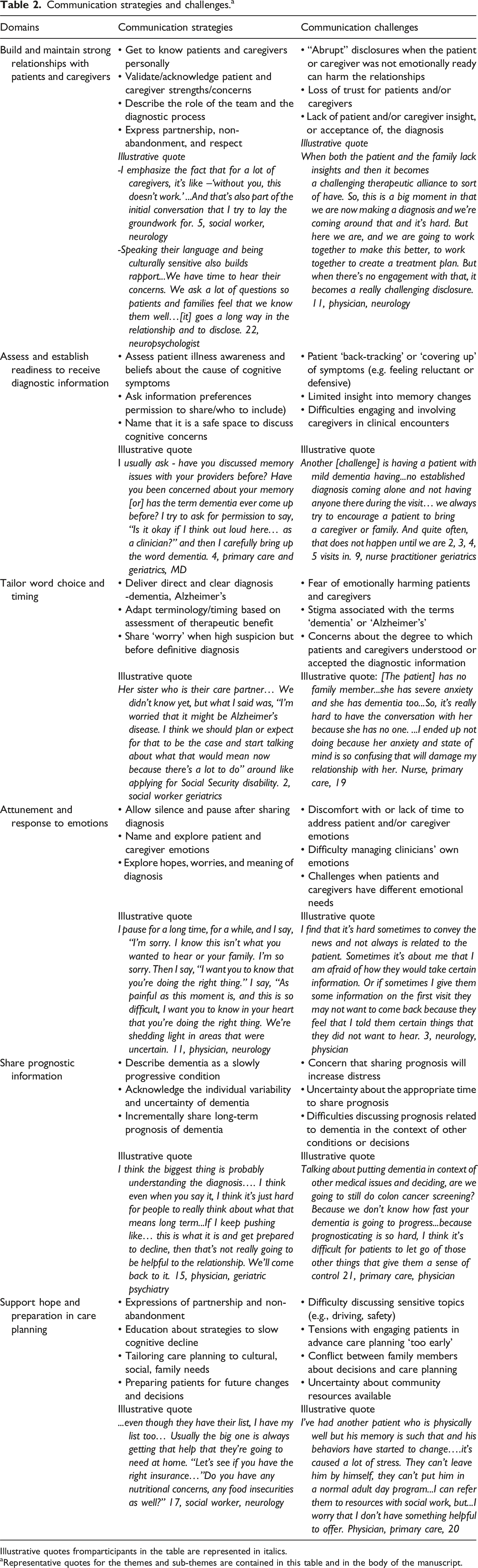
Illustrative quotes fromparticipants in the table are represented in italics.
aRepresentative quotes for the themes and sub-themes are contained in this table and in the body of the manuscript.
Theme 1: Building and maintaining strong relationships with patients and caregivers
Clinicians across professional backgrounds described their use of incremental communication strategies to establish and/or maintain strong relationships with patients and caregivers to build trust and a sense of partnership throughout the diagnostic process. First, clinicians established rapport and emotional connection by getting to know people personally and acknowledging and honoring their strengths. Second, language-concordant communication, when possible, was noted to enhance authentic connection when discussing cognitive concerns. Third, by naming what to expect with the diagnostic process and expressing non-abandonment, clinicians tried to help patients and caregivers navigate uncertainty and feel less alone in the process. Fourth, strategies demonstrating respect for both patients and caregivers deepened connection and laid the groundwork for relationships with both patients and caregivers during disclosure. …because I went really slow and we had built this relationship, it was our third visit…this was our visit to come and have this discussion…And we re-did his MoCA and it was horrible…He is this person, all these beautiful things. So, you have to really reflect those. You have to humanize it before the disclosure part because if I’m like ‘oh this is [dementia],’ they’re left absolutely destroyed and crushed. 8, MD, geriatrics I think the diagnostic disclosures when I do it in [patient’s language], they are so grateful. I find they connect with me in the sense that they see me like they are. So sometimes they tell me more intimate things. They say- ‘thank you for explaining that to us. No one had explained it in that way’…I see that and feel that connection. 3, neurology, MD I’ll give a discussion about what our role is, what we need, all the different little puzzle pieces…to put together. And it’s not going to be done today, but we will work on this together, and we talk about next steps. So if it’s imaging, you know what, let me give you a call again next week…it’s just establishing that relationship and that trust. 9, NP, geriatrics
Clinicians described instances in which the disclosure of a dementia diagnosis resulted in harm to the therapeutic relationship. Harm occurred because some disclosures were perceived to be insensitive or abrupt in that the patient was unable to develop insight into their diagnosis (anosognosia) and/or was not emotionally ready to hear the information. In other instances, the patient did not want to return to see the clinician after diagnostic disclosure, or a traumatic disclosure occurred by a different clinician which reduced overall trust in care. Clinicians described challenges with using an incremental process to build trust during the disclosure process when patients present with safety concerns (e.g., driving). … the patient refused to acknowledge or just doesn't have the ability to acknowledge that these things were happening. Then the [doctor]…made the decision to report the patient to the RMV [registry of motor vehicles] and then their license was taken away…This is very accomplished immigrant who strongly identified as having been …successful…So now it’s really hard to support the family because the family doesn’t feel that they can go behind the person’s back and get the support they need because there’s just no trust there from the patient. 2, SW, geriatrics
Theme 2: Assessing and establishing readiness to discuss diagnosis over multiple visits
Clinicians used an incremental approach to emotionally prepare patients and families and to tailor the diagnostic discussion to their needs. These strategies included: a) asking patients and caregivers to share their beliefs about what may be causing the cognitive changes, b) assessing information preferences to ensure that patients have control over the information they receive, c) naming that it is a safe space to talk about cognitive concerns, especially for patients from racial or ethnic communities in which there is enhanced stigma associated with cognitive issues, and d) ‘softening’ the diagnosis by presenting their worry that it may be a memory condition before having a definitive diagnosis. Clinicians also tailored when and with whom they shared diagnostic information based on these assessments. For example, suppose the patient had insight into the possibility that their symptoms were related to dementia. In that case, clinicians felt more comfortable sharing a direct diagnosis with patients. In contrast, information may be shared with the caregiver if there was concern that the patient could not retain diagnostic information. I often will start the conversation…[as part of] cognitive testing. What are your thoughts? Does that match up with what you’ve been experiencing? And for a lot of the time people will say, yeah, it does. So if they were that insightful in the beginning, they’re like, ‘yeah, I’ve noticed I’ve had some of these issues.’ Then…more often than not, I will have a frank discussion about diagnosis. 15, MD, geriatric psychiatry …there’s shame and stigma around admitting that there’s cognitive decline, especially in Latino communities, African-American communities. I had a lot of older adults who will pull me to the side and tell me, “I’ve been noticing... that my mind hasn’t been the same for the past year.” ... we would hear “In my culture, we don’t believe in that. We don’t speak our business outside of the family.’...I have had to kind of walk them through and say, “It’s a safe space for you to treat what you’re dealing with.” And I see it because I’m from [country] myself. 17, SW, neurology
Clinicians described challenges that arise during the assessment phase. When caregivers initiated discussions about cognitive concerns (vs. patients who initiate because of their own concerns), clinicians reported examples of patient ‘defensiveness’ or reluctance to engage in cognitive testing. Existing cultural beliefs that cognitive symptoms were related to normal aging were also noted to create barriers to assessment and diagnosis. Patient refusal to involve caregivers, or difficulties engaging caregivers, contributed to delays in making and communicating a diagnosis. Finally, caregivers responding for patients during clinical assessments caused patients to feel marginalized or frustrated, which was reportedly difficult to manage for some clinicians. I had a recent case of a daughter who brought in her mother and the mother was very dismissive of the daughter’s report and very angry at the daughter. And that was obvious when we went through the history separately, the patient told me, ‘don’t listen to her. She just is exaggerating’ and the patient in fact already had a positive amyloid pet scan…. It doesn’t come up that often, but there are times where it becomes very clear, very early that I'm not getting their best effort that they are too angry that they are there to participate. 23, neuropsychology Culturally…the notion that people have memory problems just because they’re growing older, that normal aging associated with memory decline, it can be so pervasive, it can interfere with early diagnosis. It’s almost like – you already expect that older family members will be needing help, people do take pride in that, caring for mom, caring for dad, it’s also like a cultural expectation that older family members will move in and may already be living with them. Neuropsychologist, 22 …if you know that someone’s memory isn’t the greatest and you’re trying to elicit symptoms and, not just for memory issues but for another problem and then their partner or their child is answering for them and you can see that they’re getting frustrated, it feels challenging to navigate that situation. MD, primary care, 20
Theme 3: Tailoring diagnostic disclosure word choice and timing
Different views emerged about use of the term ‘dementia’ or ‘Alzheimer’s’ when sharing a diagnosis with patients and caregivers. Some clinicians, especially dementia specialists, described that it is their professional duty to be forthcoming by relaying specific details about the diagnosis (if known) to enhance illness understanding and to enable the development of a tailored medical plan. Other clinicians, especially within primary care and geriatrics, did not typically use the term ‘dementia’ or did not use the term in specific instances, such as when the family was coping well without it being explicitly named or when there continued to be uncertainty about the diagnosis. Some clinicians also described incrementally introducing terms to enhance patient and caregiver comfort with receiving the news. I had a Spanish family and I felt like they dealt with [dementia] so beautiful and in such a different way...I’ll call her Grandma…it was getting to the point where then she wasn’t…engaging anymore. The family just kind of acknowledged that… more people moved into the house and they all took a rotation of taking care of Grandma. So in the end, she died peacefully at home…we didn’t even need to use the word dementia…It was just …woven into…the big arc of life. 13, MD, family medicine For the most part, I don’t use the word dementia unless it’s like, you walked in the room and you knew they had it because it’s so sensitive and devastating to hear you have dementia. Mild cognitive impairment people can deal with. 1, MD, geriatrics I’ll ask – ‘Have you seen the biomarker results yet?” Because it’s a little bit helpful to know if they know something or not. I’d say it’s about 50/50 they’ve either looked and they know, but they want to talk to me about what it means or they haven’t looked at it yet. I don’t beat around the bush. I just say, “So, your spinal fluid shows that you indeed have evidence of Alzheimer, or your symptoms are caused by Alzheimer’s disease.” And I pause for a long time.” 11, neurology, MD
Most participants, even those who regularly reported using the terms ‘Alzheimer’s’ or ‘dementia’ during disclosure, felt conflicted about the terms because of the emotional weight and stigma. For example: In some instances, even if there is a strong suspicion for Alzheimer’s, patient anxiety prompted clinicians to avoid or delay using the term until there is further confirmatory work-up. Furthermore, after sharing diagnostic information, clinicians expressed concerns about the degree to which patients and caregivers understood or accepted the information. For example, some patients and caregivers have been more inclined to attribute symptoms to co-occurring mental health disorders (e.g., anxiety, depression). Clinicians also described struggles when caregivers did not want the patient to hear diagnostic information as well as challenges with distinguishing between inadequate patient illness understanding due to anosognosia, limited health literacy, language barriers, or difficulties accepting the diagnosis. So I try to be really careful…I struggle with myself and I wonder if I’m being sadistic by bringing up the word dementia when I could just keep calling it a memory issue. We also have a lot of families who are like- ‘I need to discuss a lot of details but not in front of Dad because he’ll get upset.’ So, we’re doing a 90-minute visit but inevitably it means two or three other phone calls and the family meeting with Dad there and without Dad there. 4, MD, primary care/geriatrics So when I think about that for people who are not highly educated white patients that I see… and the…disclosure is often different, because it’s through interpreters…but also just where to start, what’s the understanding, where are they, how do I meet them where they are?…I don’t wanna be a different doctor for those patients. MD, neurology, 18 I gauge where the patient is and if they’re not anywhere near ready to hear that or they’re suffering from terrible anxiety about this, I let the other studies happen before, because I would hate to be wrong and have them be very anxious and given how long other appointments take to happen. I have an appointment with a patient who is incredibly anxious and I have a very high suspicion that she has Alzheimer’s disease, but I don’t think she can hear that right now. 23, neuropsychology
Theme 4: Attunement and response to patient and caregiver emotions
Clinicians across professional backgrounds were highly attuned to the emotional experience of a dementia diagnosis for patients and caregivers. Participants described the sense of validation and relief that can come from naming the diagnosis and validating people’s experiences. Clinicians also discussed examples of patient and caregiver sadness, anxiety, shock, and disbelief after disclosure. Some clinicians routinely allowed silence or explored emotions after disclosure to create space for patients and caregivers to process the news. These strategies were perceived to enhance connection, information retention, and exploration of the meaning of the diagnosis. Because when we do these diagnostic disclosure discussions, we don’t want to overload people. –[I ask] what are your hopes and worries and how can we support that…. Again, it comes back to the time and space thing really being present with people and understanding the gravity of the information you’re relaying, just knowing that and honoring that fact is really important and that gets missed a lot too. 3, neurology, MD Depending on the emotional reaction…where I might spend the entire time just with containment, meaning that there’s a lot of emotional expression and my job is to stabilize. You can’t push forward with disease education while somebody is sobbing openly…you have to join with them in the moment and that’s where I think my work becomes the most, I would say, human. 5, SW, neurology
Participants also acknowledged their challenges in responding to the emotions of patients and caregivers. For example, some clinicians moved directly from disclosure to reassurance and planning without pausing to respond to emotions because of their own discomfort, lack of time, or strong desire to preserve hope. Some participants also described their own experiences of feeling overwhelmed by the emotional weight of these discussions. Transference responses, such as identification or protectiveness, have arisen from the clinician’s own distress, which can lead to them ‘teetering around’ the diagnosis. I think that when it comes to most other diagnoses, I kind of say what it is and then just kind of leave space for response. And this is an area where I don’t, it…s here…s a diagnosis and here’s how we’re going to hold you in this new space… There are things that we can do to work with you and with the family to make sure that everything is safe and that you…re as independent as possible. 13, MD, family medicine The other complicated ones are [a] transference I develop where I’m uncomfortable using ‘Alzheimer’s.’ I’ve set it up in a way where I’m teetering around it or I know that it’s not gonna be easy…I have this one early case…a patient at age 46…I think it’s really hard to disclose early onset Alzheimer’s no matter what, however you steal yourself to disclose that information…I lost a lot of sleep over disclosing that information. 18, neurology, MD
Theme 5: Variation in prognostic communication
Clinicians shared that many patients and/or caregivers ask about prognosis after diagnostic disclosure, yet practice variation in prognostic communication emerged. Some clinicians focused on the individual variability and uncertainty that accompanies the trajectory of dementia. Others described the prognosis of dementia as a ‘slowly progressive condition’ for which there is no cure. Sometimes prognostic information is delivered incrementally and includes anticipatory guidance about the likelihood that the patient’s memory and/or function will continue to decline over the course of years and that new symptoms may arise that need to be addressed. I often say –‘we don’t have a specific timeline,’ and everything is kind of tailored to each person individually....I said, “We don’t know an exact time for things, but what we do know is the things that can kind of help support them and you along the way.” 9, geriatrics, NP In terms of discussions about prognosis, a lot of times I will paint it as this slowly progressive condition where things that are currently an issue such as memory will become more of an issue as time goes by…Then there will, as time goes by, the other things that come up that would be new symptoms that you’re not having now that you’ll develop and over time those will also get worse. 6, Neurology, MD
Clinicians described discomfort and challenges with sharing prognostic information. The discomfort has emerged from the uncertainty of prognosis in dementia (rate of progression, in particular), difficulties distinguishing between prognosis related to dementia versus other co-morbid conditions, and lack of clarity about when and how to share prognostic information given the long-term trajectory of illness. This discomfort caused feelings of inadequacy in some clinicians, prompting them to discuss prognosis only if ‘pushed,’ or causing clinicians to deflect prognostic conversations by transitioning quickly to reassurance and education. Some clinicians also described the need to help individuals emotionally process prognostic information incrementally to avoid harm to the therapeutic relationship. If they really push me, I’ll say typically the disease is very variable the Alzheimer’s, but we see anywhere from… eight to 20 years of disease decline. We don’t know exactly where you are, but then I, because of my own uncertainty, I shift to an uncomfortability with it. I shift to something like, but here we are, we have some tools to do everything we can to try to keep you where you are…18, neurology, MD [Prognosis] is always inevitably is actually one of the first questions that comes up…So when we get to that part of the conversation, I find myself actually struggling conveying the prognosis part because it’s part explaining the uncertainty. Because I feel that sometimes people want to hear how many years I’m going to be in this stage… or when is that I’m not going to be able to stand up or care for myself. And trying to explain that to patients for me is personally hard because sometimes it makes me feel like inadequate, like, am I being a good doctor? Why don't I know these things?… 3, neurology, MD
Theme 6: Supporting ‘hope’ and ‘preparation’ in care planning
After disclosure, clinicians described offering hope and reassurance by discussing a plan. Communication strategies included: 1) Reaffirming non-abandonment; 2) Strategies to slow cognitive decline, such as exercise, diet, social engagement, controlling risk factors, and medications (including anti-amyloid therapies, if appropriate); 2) Asking what is important to the patient and caregiver to enhance quality of life; 3) Assessing social factors, including food, housing, insurance, and caregiver supports; 4) Connecting patients and families with resources. In addition, clinicians described discussions about preparation for the future, which often occurred in subsequent meetings. Preparation included discussions of advance care planning as well as safety and financial risks. Some participants adapted care planning to cultural needs. For example, families from some cultural communities may be more inclined to provide care in the home, and clinicians started working with families early to establish supports in the community. I just try to be as reassuring as possible that they are not alone. Try to make that as true as possible. Because in my experience, that’s a person’s greatest worry…And so… how do…we manage this together…? And how we live life for as long as possible with the highest quality of life possible?…Well, let’s make sure you’re taking your antihypertensives…go for the daily walks, stay socially engaged…And making sure we’re taking care of the …family system. 7, MD, geriatric psychiatry I talk about, let’s identify and try to control any modifiable factors…And then …let’s think about ways to strengthen your brain health…And then finally, I come back to disease modifying therapies. And that’s been a really nice conversation because there’s a lot of hope there and optimism around that. MD, neurology, 11 So at the [xx], this is a very heavily Spanish-speaking and immigrant population and I think culturally, a lot of Latina families want to keep people at home…And so when I make the dementia diagnosis....it usually does to a very different path in terms of management… let’s make sure you’re getting the maximum amount of services at home. Do you have siblings that you want to invite to the next visit so we could all talk about this diagnosis together…? 4, primary care/geriatrics, MD
Clinicians shared communication challenges with engaging patients and families in care planning. These included, for example, conversations about sensitive issues (e.g., driving) that signal loss of independence. Clinicians created psychological safety by using a ‘no decisions necessary today’ framework to prepare patients and families for future difficult decisions. While clinicians noted the importance of decisions related to advance care planning (ACP) to capture the patient’s voice before loss of cognitive capacity, they also described caution about when to begin discussing ACP because values and priorities change. In instances in which decisions were needed (e.g., increasing care in the home), conflict has arisen when numerous family members were involved in decision-making or when structural challenges existed which interfered with the ability to get enough support in the home (e.g., insurance limitations). We always talk about… the financial piece with all the scams and all the problems. So, we’ll bring that up and say...”Okay, so let’s kind of keep an eye on these things.” Driving is always the hardest… And we put little bugs in these are things we’re going to be checking in about. NP, 9 geriatrics Talking about advanced directives and code status…I think is really tricky, because...when they imagine themselves…unable to do things for themselves, unable to recognize family members…[they] imagine that as a terrible way to live and they would never want to live that way. But I think the fact of the matter is the brain changes over time…because their whole brain is different, they’re different. So I think making predictions about things like code status… that’s just really hard. Primary care, MD, 21 …if I have one caregiver who’s having communication challenges with the family. So then I often have to step in to kind of moderate what’s going on because…the other siblings are not on board with what this sibling may be trying to do with the mom or the dad…so that’s when it’s hard for me because I’m trying to bring everyone together so that we can all be on the same page. So it often has to be a family meeting 17, SW, neurology
Discussion
For this qualitative study on diagnostic disclosure communication, we interviewed 23 clinicians across specialties and professional backgrounds in three academic medical centers. This study revealed clinician perceptions of the specific communication skills and techniques they use to build relationships, tailor communication to patient/caregiver needs, and support emotional coping and care planning around the time of a dementia diagnosis (Figure 1, Discussing a Dementia Diagnosis with Patients and Caregivers). The findings also highlight practice variation and specific communication challenges that clinicians face, which provide opportunities for intervention development to enhance skills and communication quality. Discussing a dementia diagnosis with patients and caregivers.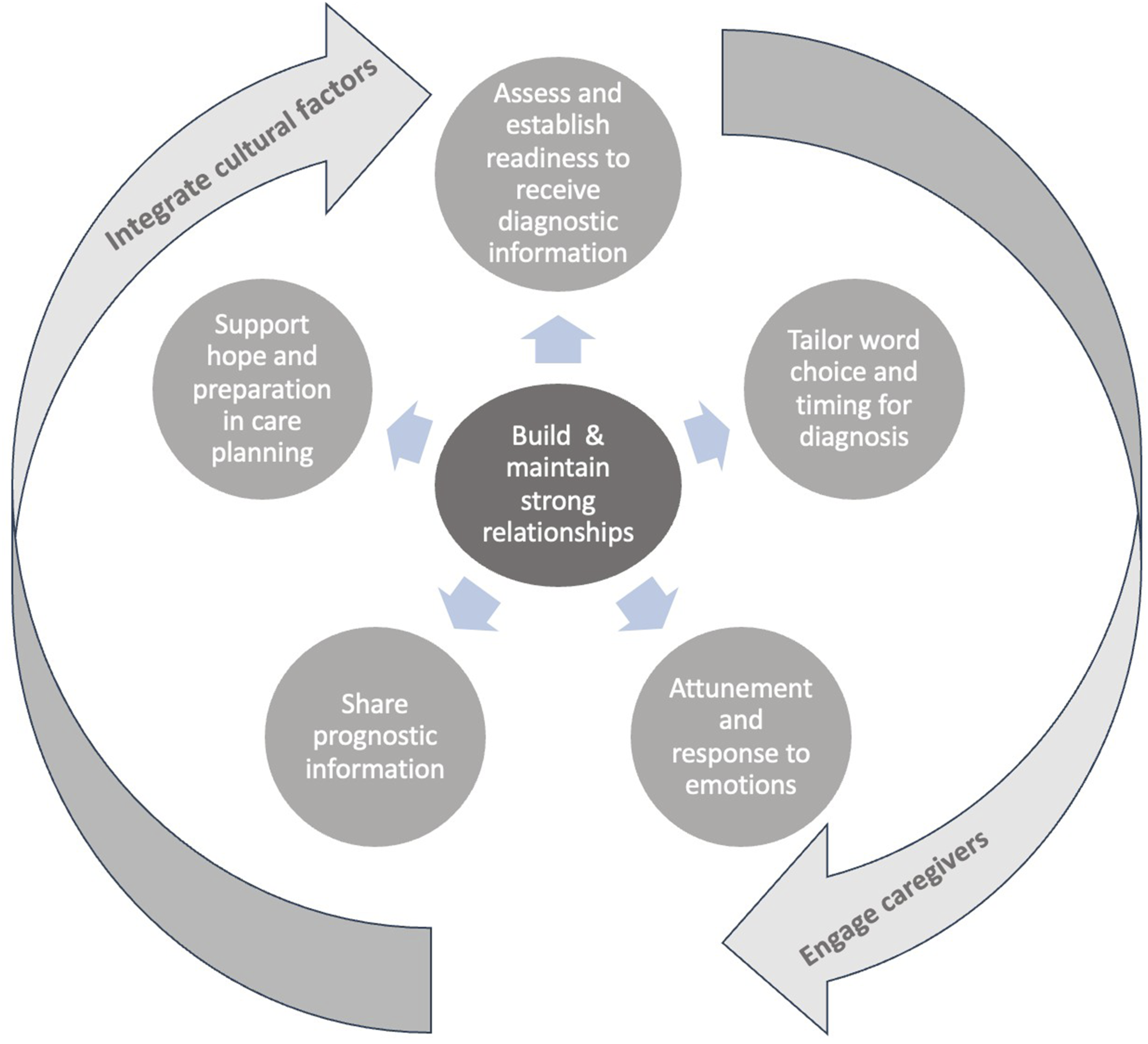
Clinicians described therapeutic relationships with patients and caregivers as a central aspect of person-centered diagnostic disclosure communication. Given the gravity of a dementia diagnosis, communication strategies to build authentic connection and rapport were perceived to be psychologically protective of patients and caregivers and to humanize the process of receiving difficult news that threatens identity and personhood. These findings align with other qualitative studies of clinician disclosure practices that have highlighted the importance of the therapeutic relationships with both patients and caregivers (McKenzie & Brown, 2021; Wollney, Bylund et al., 2022). Clinicians in our study identified specific communication strategies they use to build relationships, specifically for diagnosing dementia. These include, for example, getting to know people personally, validating fears or concerns, acknowledging and honoring strengths, and using an incremental and flexible approach to disclosure. Our study adds new knowledge about additional skills and strategies to foster relationships. Clinicians highlighted the importance of expressions of ‘non-abandonment’ (Quill & Cassel, 1995; Sep et al., 2014) (e.g., that they will have a continuous relationship with and active involvement in a patient’s care throughout the course) and ‘partnership’ (Wolf et al., 2017) (e.g., establishing a collaborative relationship for care planning and decision-making). Clinicians also identified language-concordant diagnostic disclosure, when possible, as an important trust-building strategy. The stigma associated with dementia, particularly in some cultural communities, requires additional strategies to create psychological safety for patients and caregivers, such as naming that it is a safe space to discuss cognitive concerns (Blinka et al., 2023; Ch’en et al., 2024; Johnson et al., 2020; Sagbakken et al., 2018). Furthermore, prior studies reveal that many individuals face a prolonged, uncertain, and fragmented path to diagnosis when undergoing evaluation for cognitive concerns (Wynn & Carpenter, 2019). In this study, clinicians highlighted the importance of explicitly ‘managing expectations’ for patients and caregivers by describing the role of different team members and discussing what to expect with the diagnostic process to build trust while navigating an uncertain journey. Taken together, these findings reveal the importance of reframing the primary goal of diagnostic disclosure from imparting medical information to a process of creating a trusting and holding environment to receive and adapt to difficult news of a dementia diagnosis.
Our study also reveals that diagnostic disclosure conversations are ‘serious illness conversations’ given the emotional weight of these discussions. The sensitivity with which clinicians approach diagnostic disclosure emerges from attunement to, and empathy for, the emotions that arise for patients and caregivers with a diagnosis; challenges with patient insight into their diagnosis due to cognitive limitations; struggles that some patients and caregivers have with psychologically accepting the diagnosis; and clinicians’ own emotions. Additional complexity arises when patients and caregivers have different levels of insight, emotional responses, and emotional support needs through the diagnostic process. These findings are similar to the results of a multi-stakeholder consensus process that highlighted the importance of tailoring diagnostic processes to patient and caregiver needs and clinician expressions of empathy (Armstrong et al., 2024). However, practice variation emerged that may be more related to clinicians’ own degree of comfort than to patient and caregiver needs. Findings from a systematic review demonstrated that patients with dementia and caregivers desire emotional support during and after diagnostic disclosure (von Kutzleben et al., 2012). While some clinicians in our study stated that they routinely integrate practices to validate and explore patient and caregiver emotions when sharing the news of a dementia diagnosis, other clinicians do not leave space for an emotional response after sharing a diagnosis and move quickly to reassurance and education. This variation accords with prior research of audio-recorded disclosure conversations, showing practice variation in the use of emotional rapport building strategies in dementia specialty clinics (Zaleta & Carpenter, 2010). There are numerous evidence-based training interventions to enhance clinician skills and comfort in responding to emotions when sharing difficult news (Baile et al., 2000; Peixoto et al., 2020). This study also adds to the literature by identifying the importance of attention to clinicians’ emotions as part of this process. Clinicians described feelings of uncertainty, inadequacy, and distress over difficult disclosures, and described altering their own practices based on personal discomfort. One implication of these findings is to provide space for clinicians to reflect on how their emotions relate to past experiences, future concerns, and how they may affect the way they care for the patient. Studies of serious illness communication interventions, for example, demonstrate that providing a safe space for clinicians to reflect on their challenges and emotional experiences (Alexander Cole et al., 2020; Paladino et al., 2022, 2023) can enhance comfort, confidence, and self-efficacy.
Clinicians in our study aimed to foster hope and empowerment while preparing patients and caregivers for future changes during and after dementia diagnosis. These findings are similar to prior studies of clinician-reported experiences with diagnostic disclosure (Vince et al., 2017; Wollney, Bylund et al., 2022). The ‘hope/prepare’ communication framework is a commonly used framework in serious illness communication (Campbell et al., 2010). In this study, clinicians transitioned quickly after disclosure to discussions about what patients can do to slow cognitive decline, including social engagement, diet, exercise, addressing modifiable risk factors, and medications, including emerging anti-amyloid therapies if appropriate. Additionally, clinicians connect patients and caregivers to community resources and assess caregiver and family needs as well as social factors, including food, housing, and insurance. Clinicians described these strategies as a means of supporting hope and empowering patients and caregivers to begin adapting to a dementia diagnosis. In addition to current planning, patients with dementia and caregivers often desire information about what to expect in the future (Jennings et al., 2015; Shafir et al., 2022). This study revealed clinician challenges with sharing prognostic information as an important aspect of anticipatory guidance. Many clinicians in our study framed prognosis in terms of individual variability or deflected the conversation, even when asked by patients and caregivers. Others reported that they would discuss a ‘big picture’ prognosis of dementia as a progressive condition for which there is no cure. In a qualitative study of audio-recorded discussions in memory clinics in England, prognosis was discussed in general terms rather than specifics, and the seriousness of the prognostic information shared was minimized by some clinicians (Dooley et al., 2018). Prior research in the United States demonstrates that expressions of prognostic ‘uncertainty’ are common in dementia diagnostic practice (Visser et al., 2020), yet few clinicians share long-term prognostic information regarding expected or likely changes to memory and function. In our study, clinicians described why they felt uncomfortable sharing prognostic information, which included uncertainty about the rate of progression; difficulties distinguishing between prognosis due to dementia versus other co-morbid conditions; and worries about harming relationships with patients by discussing long-term prognosis too early (since it can be too much for patients and families and there may be time to do this as the relationship grows.) Yet it is also important not to miss opportunities for this conversation, given that patients and caregivers want to prepare for changes and needs that arise with illness progression, such as cognitive and functional decline, financial planning, and advance care planning (Sanford et al., 2020). Identifying an opportunity to discuss sensitive prognostic issues in a tailored and emotionally supportive way is an important aspect of ongoing anticipatory guidance.
Our communication findings have implications for clinical practice, education, and research. First, interventions designed to improve diagnostic disclosure communication and care planning would benefit from the inclusion of communication skills training for interprofessional clinicians to enhance therapeutic relationships, support validation and exploration of the emotional needs of patients and caregivers, and enable hope and preparation for an uncertain future (McKenzie & Brown, 2021; Portacolone et al., 2020). Numerous evidence-based communication interventions (e.g., Serious Illness Care Program, Vital Talk) that include tools and clinician training that can be adapted for dementia diagnostic disclosure (Berry et al., 2023). Given the findings related to the clinician’s emotional experience, future interventions should consider pairing clinical tools and clinician training with support for clinicians that provides opportunities to reflect and recognize their own emotions and how they relate to their personal and clinical experience. Second, qualitative studies, clinical guidelines, and recent consensus processes have highlighted best practices in dementia diagnostic disclosure communication (Armstrong et al., 2024; Lecouturier et al., 2008; Wollney et al., 2022a, 2022). Translating these principles into clinical interventions that improve practice would benefit from the incorporation of human-centered intervention design (Göttgens & Oertelt-Prigione, 2021). For example: prior use of co-design methods with diverse patients, caregivers, and clinicians have facilitated the development of scalable, structured communication interventions that have contributed to improvements in clinician practice, patient and clinician experience, and patient outcomes (Bernacki et al., 2019; Curtis et al., 2018; Paladino et al., 2019, 2020; Sanders et al., 2023). Third, dementia diagnostic communication across languages and cultural backgrounds is critical to intervention development to address the unique challenges of dementia diagnostic disclosure. In fact, a recent survey of clinicians in memory clinics demonstrated that most (79%) would like to use tools, training, or both for communication strategies to enhance patients’ understanding of information and to engage patients and caregivers who speak a different language (Hendriksen et al., 2023). Fourth, we have an opportunity to consider the outcomes that matter at the time of diagnosis. While patient and caregiver knowledge and understanding of the diagnosis remains important, the degree to which individuals feel heard and understood (Edelen et al., 2022), sense of hope and resilience (Stoner et al., 2018), feeling respected and emotionally supported (McKenzie & Brown, 2021), and therapeutically connected (Baier et al., 2020; Pinto et al., 2012) may be meaningful measures to study in communication research.
Several limitations are noted. First, recruitment focused on clinicians working in cities in academic centers in the United States in Massachusetts and New York, and with an overrepresentation of specialists, which limits generalizability. Second, we focused on themes identified across specialties. We did not have a large enough qualitative sample to fully explore differences in disclosure practices and needs between dementia specialty clinicians in memory care settings compared to primary care and geriatrics, although our findings point toward both similarities and differences. Third, the settings and clinicians in this study specifically have a practice of diagnostic disclosure, even if they face challenges. Overall, many dementia diagnoses are not made or disclosed at all (Amjad et al., 2018; Connolly et al., 2011) or if they are shared, are not done using any specific framework. Thus, what we are describing here may not be reflective of typical communication practices, but these findings could contribute to the development of a structured intervention.
Conclusion
This study revealed clinician perceptions of communication challenges with diagnostic disclosure as well as specific communication skills and techniques they use to build relationships, tailor communication to patient/caregiver needs, and support emotional coping and care planning around the time of a dementia diagnosis. These findings reveal the importance of reframing the primary goal of diagnostic disclosure from imparting medical information to a process of creating a trusting and holding environment to receive and adapt to difficult news of a dementia diagnosis. Future research to co-design and test a customized, structured communication framework and training for clinicians may enhance the quality of diagnostic disclosure communication in dementia care.
Footnotes
Author contributions
JP: conceptualization, planning, methodology, data collection, analysis, data curation, writing—original draft, writing—review and editing, and reporting. AMV, DB, DR, SB, LRG, EL, CD: conceptualization, methodology, supervision, writing -- review and editing, and reporting. HCG: planning, data analysis, data curation, writing—review and editing. CR, ASB: conceptualization, methodology, data analysis, writing—review and editing, and reporting. All authors have contributed to the design, analysis and writing of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Jack Satter Foundation awarded to JP (230111). The funder did not contribute to the design, analysis or writing of this manuscript.