
Abstract
Understanding the perspectives of people with dementia is crucial for providing person-centred care. Self-experience practices in caregiver training could foster empathy by simulating conditions individuals may encounter. This European study examines the potential contribution of self-experience practices to improving understanding and empathy towards people with dementia. A qualitative approach within the interpretative paradigm was employed to investigate perspectives on self-experience practices in dementia care through focus groups and individual interviews. Participants were people with dementia, informal caregivers, and professionals with experience in simulation-based dementia training and/or communication tools. Transcripts from Germany, Ireland, Italy, and the Netherlands underwent qualitative content analysis and thematic synthesis. Six analytical themes emerged across all target groups and countries, indicating the possibility of enhancing dementia care through self-experience. Themes cover the rationale and impact of these practices, required content and strategies, training procedures, target groups, implementation issues, and barriers and facilitators. Tailoring the training and supportive environment are crucial, but ethical and implementation issues must also be considered to ensure effectiveness and integrity. Integration of self-experience practices suggests benefits in skill acquisition, care strategies, and theoretical understanding. Further research is needed to reach an international consensus for self-experience dementia training practices.
Introduction
The progression of dementia profoundly affects the lives of people with dementia and their social environment, particularly their families and significant others. This process often involves various changes, affecting not only cognitive functioning but also behaviour, social interaction, and other aspects of daily life. While physiological changes in the brain may contribute to the observed behaviours, it is evident that numerous environmental, psychological, and social factors are also involved (Cerejeira et al., 2012; Cho et al., 2021; Fratiglioni et al., 2020; Kales et al., 2015). These factors shape the experience of people with dementia, and extend their influence on relatives, significant others, and the professional care environment (Cerejeira et al., 2012; Chekani et al., 2021; Kim et al., 2021).
Social isolation and the loss of autonomy represent significant challenges, exacerbated by societal stigma towards people with dementia (Alzheimer’s Association, 2019; World Health Organization, 2017). Common labels, such as “Behavioural and Psychological Symptoms of Dementia” (BPSD), can contribute to this stigma by neglecting the thoughts and emotions of people with dementia (Cunningham et al., 2019; Warren, 2022). Research suggests that emotional reactions, behaviours, or communication attempts may be pathologised by the diagnosis of BPSD (Warren, 2022). Many of these behaviours classified as BPSD are valid responses to inappropriate external circumstances and relational approaches (Kitwood & Bredin, 1992).
To strengthen successful social interactions in dementia care, it is essential to address the various factors influencing both people with dementia and their formal and informal caregivers. Effective social interactions are vital for meeting the needs of individuals with dementia but can be hindered by challenges such as difficulties with communication (Birt et al., 2020; Feast et al., 2016), experiences of stigma and inappropriate treatment (Lindeza et al., 2020). Similarly, caregivers encounter difficulties such as high levels of responsibility and increasing demands of care as dementia progresses (Lindeza et al., 2020).
Self-experience practices in dementia care involve experiential learning aimed at changing the perspectives of training participants, providing them with a deeper understanding of the needs and daily challenges of people with dementia (Kolb, 1984). These practices are driven by the rationale of achieving person-centred care that respects the individual requirements and values of each person living with dementia. Person-centred care emphasises the subjective experiences of individuals, focusing on their uniqueness rather than solely their underlying disease (Kitwood, 1997; McCormack & McCance, 2016). Integrating self-experience practices into dementia training programmes for caregivers may heighten awareness of the challenges faced by people with dementia, and may help reduce stigmatisation.
Trying to understand the subjective experiences of people with dementia is essential, as these experiences offer valuable insights into their emotional world and daily challenges (van Wijngaarden et al., 2019; Zwijsen et al., 2016). People with dementia are capable of expressing their thoughts and feelings, which are often overlooked in clinical settings (Eriksen et al., 2020; Machiels et al., 2017). By incorporating these lived experiences, practitioners can develop more empathetic and effective approaches to care that address the needs and preferences of people with dementia.
Self-experience practices comprise activities such as virtual simulations (Adefila et al., 2016; Torrence et al., 2022), role-play (Haugland & Reime, 2018; Maharaj, 2015), or film interventions (Baillie et al., 2016; Prins et al., 2019), which enable participants to gain insights into the physical, cognitive, and emotional challenges faced by people with dementia. Through these tangible experiences, training participants can enhance their own understanding and subsequently derive actions from it. An up-to-date review indicates a range of self-experience practices, from non-technological to high-tech solutions. Most studies focused on immediate reactions and knowledge assessments, while impacts on behaviour and caregiving practices were less explored (Wittmann et al., 2024).
While evidence suggests that the use of self-experience practices can lead to changes in practice and improvements in the quality of care (Slater et al., 2019), their specific role in dementia care remains unclear. This includes their potential to influence understanding and awareness of lived experience of dementia, as well as the empathetic response of caregivers towards people with dementia. Furthermore, it is unclear how these practices can address the needs and experiences of different parties (Heward et al., 2021).
The aim of our study is to examine how self-experience practices could contribute to enhancing awareness, empathetic response, and understanding of the perspective of people with dementia within the context of person-centred care. Consequently, the perceived needs and experiences associated with dementia-specific self-experience practices will be explored with three participant groups: people with dementia, informal caregivers, and health and social care professionals.
Materials and Methods
We followed the “Standards for Reporting Qualitative Research” Synthesis (SRQR; checklist provided in supplemental material; (O’Brien et al., 2014)) to structure this report.
Qualitative Approach and Research Paradigm
The study focused on exploring and gaining a profound understanding of the perspectives and experiences of interview participants regarding the role of self-experience practices in enhancing person-centred care for people with dementia. A qualitative approach was chosen because it enables the exploration of complex social phenomena by capturing participants’ subjective interpretations of their experiences. The research interest situates our study within the interpretative paradigm, which is suited for exploring human experiences by considering the meanings individuals attribute to their social and cultural contexts (Merriam & Tisdell, 2016). This paradigm highlights the importance of understanding complex social phenomena, such as the role of self-experience practices in enhancing person-centred care, through the integration of diverse perspectives. By integrating the views of people with dementia, informal caregivers, and professionals, the study reflects the interpretative paradigm’s focus on capturing the multifaceted and context-dependent nature of lived experiences. These groups were selected to provide complementary insights into the challenges and opportunities associated with implementing self-experience practices, highlighting their potential to address specific needs and promote person-centred care.
Context
Our study was part of the international Erasmus+ funded project “Improving demeNtia care Through Self-Experience” (INTenSE, 2021), including collaborators from Germany (DE), Ireland (IE), Italy (IT), and the Netherlands (NL). INTenSE aimed to develop an innovative self-experience toolkit to enhance the knowledge and skills of health and social care professionals in providing person-centred care for people living with dementia. By incorporating self-experience practices as pedagogical approaches, the project aimed to facilitate a deeper understanding of the realities experienced by people with dementia among its participants.
Researcher Characteristics and Reflexivity
Team members from project countries were experienced in conducting qualitative research. Due to their expertise in dementia studies, the researchers were able to establish trusting relationships with the interview participants. Throughout the study, the team engaged in critical reflection, questioning their preconceptions and assumptions, particularly those influenced by their backgrounds in dementia research. Regular online meetings and in-person workshops facilitated active discussion and collaboration, helping researchers identify and address biases to ensure comprehensive data collection and analysis.
Sampling Strategy
Interview participants were selected based on predefined inclusion and exclusion criteria to ensure a diverse representation of perspectives and backgrounds. Purposive sampling was chosen as the recruitment strategy to involve individuals with knowledge or experience (in the field) of dementia and related self-experience practices or health communication tools. Recruitment was supported by key parties, for instance, from national organisations (e.g., dementia self-help groups, peer support networks, advocacy groups, local dementia networks, or Alzheimer societies), as well as through project partners’ networks.
Recruitment of interview participants proved to be challenging due to their high workload within the SARS-CoV-2-pandemic as well as their personal barrier to using online communication tools.
Data Collection
To meet the objective of the study, our aim was to capture and interpret the documented verbal expressions of individuals participating in interviews. Conducting focus groups was deemed appropriate to comprehensively explore the research interest, as this methodological approach facilitates the dynamic interaction among participants, enabling an exploration of their perspectives (Krueger & Casey, 2015). We aimed for five to eight participants per group. Some participants encountered challenges in engaging within group settings, particularly in online interviews due to the SARS-CoV-2-pandemic. Therefore, both focus groups and individual interviews were conducted, starting with focus groups because of their interactive nature, followed by individual interviews taking participants’ needs into account.
In total, we conducted 14 focus groups with two to eight participants (average duration: 87 min) and 11 individual interviews (average duration: 46 min) between March and May 2021. Amidst the SARS-CoV-2-pandemic, focus groups and individual interviews were conducted either online or in person, depending on country-specific regulations. The interviews were audio- or video-recorded (in accordance with country-specific regulations) and transcribed verbatim. Two researchers, one being the moderator and the other responsible for taking field notes, conducted focus groups and interviews.
The interview guides for each group of participants were drafted and piloted by the German partner and subsequently utilised in all participating countries (Helfferich, 2011; Krueger & Casey, 2015). The draft and final versions of the interview guides underwent a comprehensive review by the project partners. Additionally, a person with dementia revised the respective version of the interview guide tailored for people with dementia. The final questioning routes in English were translated into the national languages.
The interview guides served as a framework for conducting both the focus groups and individual interviews, enabling adaptation to the changing circumstances of data collection. To address the different groups, it was necessary to customise the guides for the interview participants. Specifically, these guides were designed to explore participants’ perspectives on the significance of self-experience practices in person-centred care, with a particular focus on identifying how such practices could contribute to improving the understanding and care of people with dementia. One of the key questions for the group of professionals, for example, was: “In what ways do you think interventions might be useful to understand what the person with dementia is feeling and what he/she needs?” In terms of content, the guides aimed to gather insights into the potential use, benefits, and challenges of implementing these practices in everyday care settings (see supplemental material).
Participants
A total of 75 participants took part in the study: six people with dementia, 37 informal caregivers, and 32 professionals. Not all of the countries were able to recruit people with dementia.
The persistence of memory problems among the participants with dementia was assessed through self-report and pertained to a relatively short period of 5 years, on average. Four out of six people with dementia participated in the interviews alongside their informal caregiver, who was the primary caregiver. Among the professionals, half were from the healthcare sector, with the majority being nurses.
The perspective of people with dementia regarding their individual situation was considered essential to creating a basis for enhanced awareness and understanding, and should therefore be included in the development of self-experience practices to enhance their effectiveness in person-centred care. Focus groups and interviews aimed to identify specific situations in the daily lives of people with dementia that are often misunderstood by others, as well as approaches to improve understanding and interaction. Participants with mild to moderate dementia were deliberately selected, as this group typically retains sufficient communicative abilities to articulate their experiences in a nuanced manner (Banovic et al., 2018). Mild to moderate dementia served as a general inclusion criterion, while the individual ability to participate in an interview was assessed by gatekeepers (e.g., self-help group leaders, advocacy representatives) through clinical judgment. Individuals with severe dementia or acute psychiatric or medical conditions that could interfere with participation were excluded. If desired by the person with dementia, an informal caregiver could actively participate in the interview.
To cover diverse perspectives, informal caregivers of different ages and relationships with the person with dementia (e.g., spouse, children, and friends) were recruited. Inclusion criteria for caregivers were (1) an existing caregiving relationship with the person with dementia and (2) the ability and willingness to reflect on caregiving experiences. Informal caregivers were asked to identify techniques and interventions to enhance understanding of the situations of people with dementia and to assess barriers and facilitators for the development and implementation of (self-experience) practices.
Inclusion criteria for professionals were (1) professional experience or work in the field of learning with dementia-specific self-experience or simulation practices and/or (2) involvement in the use or development of health-related information and communication tools (e.g., communication apps, decision aids). These criteria were selected to ensure that participants had practical experience with reflective learning processes in dementia care and communication. Their applied knowledge of how communication strategies influence understanding and awareness was considered valuable for informing the development of self-experience practices.
All eligible participants received detailed verbal and written information about the INTenSE project before providing their informed consent.
Data Processing and Analysis
National Data Analysis
In the initial step, a target-group-specific qualitative content analysis with inductive coding (Kuckartz & Rädiker, 2022) was conducted in each country based on the transcripts. An open coding method was applied, wherein categories were derived directly from the material. Researchers in each country analysed the data by developing an initial set of codes. Inter-rater reliability was examined by cross-comparing the sets of codes developed by two researchers on the same team, i.e., at a national level. Disagreement was discussed until consensus was reached, and a final category system was developed. Using the final category system, the remaining transcripts were analysed. The national results were translated into English and summarised in a country-specific report.
Cross-Country Analysis
In a second step, the “thematic synthesis” was conducted following the approach proposed by Thomas and Harden (2008), which involved synthesising the findings of the qualitative primary research from the available country-specific reports, i.e., the first step of the data analysis, using techniques to formalise the development of themes (Thomas & Harden, 2008). We selected this method because it allows for the synthesis of existing data by systematically identifying, analysing and integrating themes across multiple qualitative primary research reports, while ensuring that the context and complexity of the original information are preserved. Furthermore, the methodological approach of a cross-national analysis of interview data has proven to be feasible and valid in an earlier study of project partners (Stephan et al., 2018).
Within this second step of analysis, two researchers (JW, AB) independently coded line-by-line the results of one national research team (IE) and discussed the resulting target-group-specific coding system in a consensus-oriented manner. The remaining country-specific results were subsequently analysed, using the inductively derived descriptive codes which were supplemented as needed. The researchers searched for commonalities and differences among the codes identified a priori and grouped them into a hierarchical structure. Based on the results, we produced country-specific as well as cross-country summaries for each descriptive code, which remained close to the material, thus deriving a common conclusion from the results. These were discussed with the project partners. For data synthesis of national results, we identified analytical themes and were able to derive similarities and differences between the three perspectives based on descriptive codes. The analysis was performed using MAXQDA software (version 2018.2).
Techniques to Enhance Trustworthiness
In line with established quality criteria in qualitative research (Lincoln & Guba, 1985; Sim & Sharp, 1998), we applied several strategies to enhance the trustworthiness of our study. Lincoln and Guba’s framework (1985) provided the theoretical basis for defining trustworthiness criteria, while Sim and Sharp (1998) offered complementary practical guidance. Building on these foundations, we ensured credibility, transferability, and reflexivity through systematic procedures and team-based validation. To identify and address potential biases that could have influenced our perception and interpretation of the data, we engaged in continuous reflection. The systematic and multi-stage data analysis was supported by a jointly developed study protocol and online team meetings, which helped standardise the process and ensured that all research team members were familiar with the procedure and consistently adhered to it. To ensure the transferability of the results, the national findings were summarised in reports and discussed in an international context, identifying differences and similarities between the countries. To ensure the credibility of the results, all coding and synthesis were reviewed multiple times, and there was ongoing discussion about the validity of the conclusions.
Ethical Issues
Ethical approval was obtained from the responsible authorities in each country, in accordance with national regulations and international ethical principles (DE: Ethics committee of the Medical Faculty, Martin Luther University Halle-Wittenberg (2020-234); IE: Dublin City University Research Ethics Committee (DCUREC/2021/016); IT: Clinical Research Ethics Committee of the Servizi Pastorali Educativi Sociali (SPES) Group after consultation with trade union representatives; NL: Maastricht University Ethics Committee (FHML-REC/2021/009).
Particular attention was paid to the process of obtaining informed consent, which was secured prior to data collection. This was especially important in the case of participants with dementia, while also recognising the vulnerability of all participants. Both the study information and consent forms were designed to be easily understandable and specifically tailored to individuals with dementia.
Results
Overview of Interviews and Characteristics of Participants per Country. Values are Numbers Unless Stated Otherwise
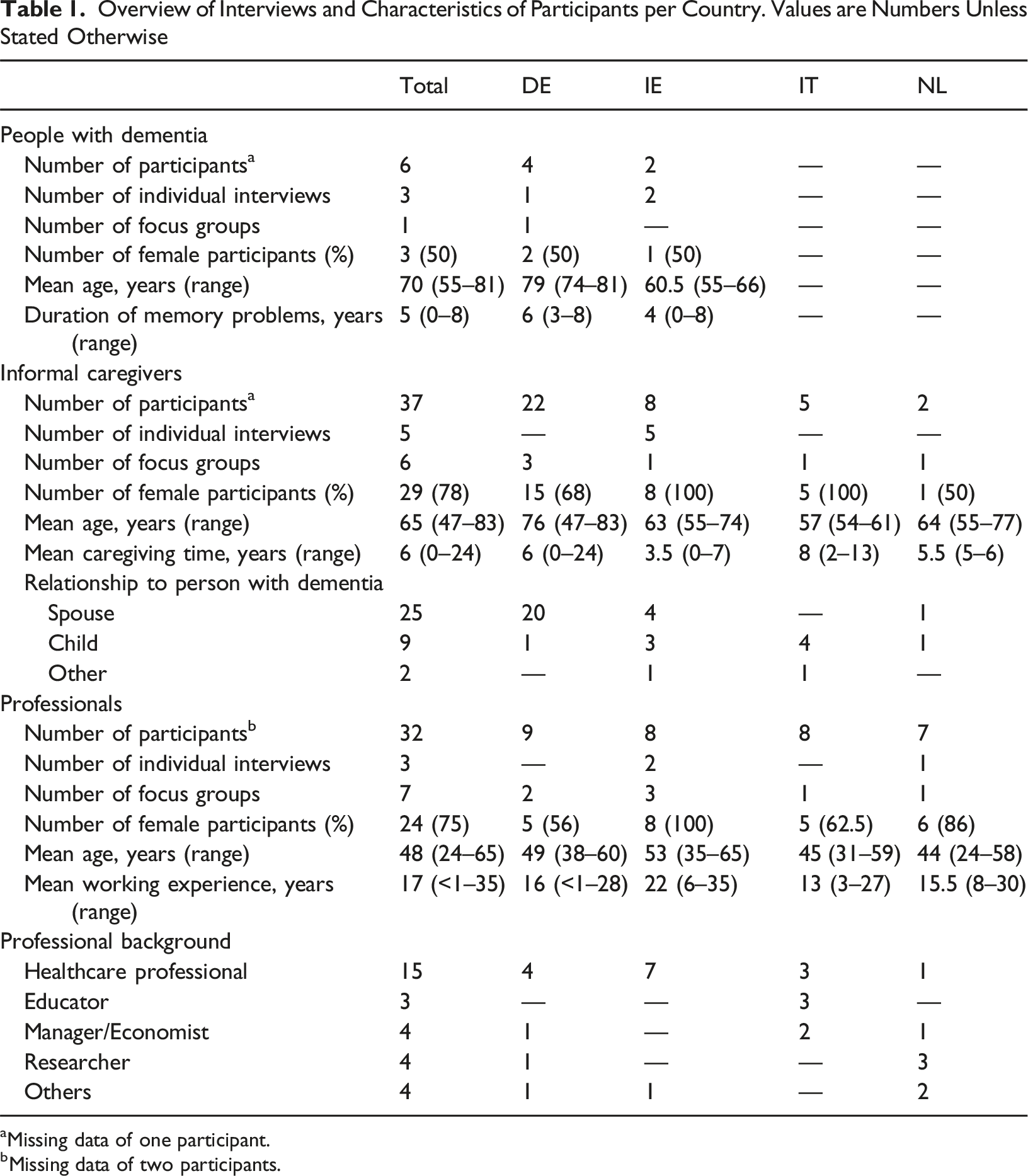
aMissing data of one participant.
bMissing data of two participants.
Overview of Analytical Themes and Included Descriptive Codes per Group of Participants
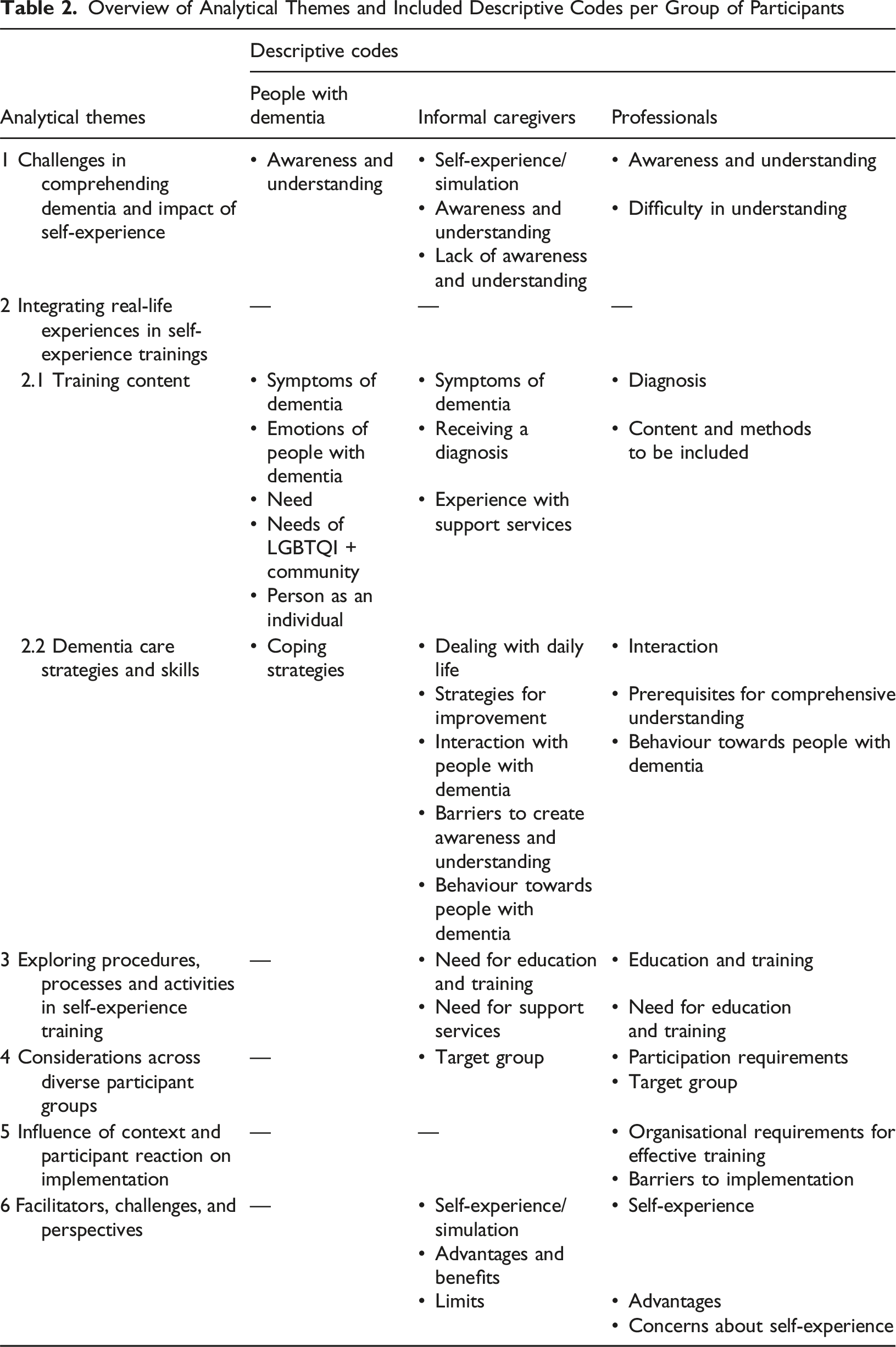
Theme 1: Challenges in Comprehending Dementia and Impact of Self-Experience
All participant groups affirmed a prevalent lack of awareness and understanding of (the person with) dementia among healthcare professionals, informal caregivers, and the general public. Participants highlighted the difficulty of relating to the experiences of people with dementia due to its heterogeneous and fluctuating symptoms, including non-cognitive symptoms. Participants emphasised the challenges of comprehending symptoms such as hallucinations and delusions. ‘So it’s one of the hardest for families to just understand as well.’ (Professional, IE)
According to informal caregivers and professionals, this lack of understanding may impede the early recognition of dementia signs by family members and healthcare professionals, contributing to stigmatisation and hindering the provision of person-centred care. ‘If you start with prejudices, you risk not being able to empathise with the patient because this aspect bothers you and you become unable to interact with this person.’ (Professional, IT)
Consequently, the need for education and increased awareness about dementia underscores the importance of integrating self-experience practices into training, as advocated by both informal caregivers and professionals. They believe such practices can enhance awareness, understanding, and provide insight into the world from the perspective of a person living with dementia. Interview participants emphasised that this improved understanding, when applied to person-centred care approaches, and could lead to more empathetic responses and tailored support for individuals with dementia.
Furthermore, people with dementia emphasised the significance of acceptance and understanding, acknowledging limitations of perspective-taking. ‘There are some situations that simply cannot be explained.’ (Person with dementia, DE)
Theme 2: Integrating Real-Life Experiences in Self-Experience Trainings
Sub-Theme: Training Content
All of the participants reported about personally relevant situations where others lacked understanding and awareness of dementia, e.g., during diagnosis, accessing health services, or encountering the emotions of people with dementia. These concrete experiences should be used as a basis for self-experience training, according to the interview participants. However, informal caregivers and professionals noted that providing universally applicable recommendations is challenging due to the diverse clinical presentations and the individuality of each person with dementia. Additionally, training must include both negative and positive experiences with dementia to avoid perpetuating negative stereotypes.
Participants across the three groups described the diagnostic process as crucial. Receiving a dementia diagnosis is profoundly shocking for those affected. Informal caregivers noted that diagnostic procedures mostly focus on forms of dementia with cognitive deficits. There is also a lack of general information about dementia and limited assistance in managing its impact on daily life. These deficiencies have been identified as affecting the manner in which people with dementia and their caregivers handle the diagnosis, according to both caregivers and professionals. The absence of adequate information at the outset of the diagnostic process may further impede the delivery of person-centred care. ‘Nobody really kind of guided them in terms of how it might appear in day-to-day life.’ (Professional, IE)
People with dementia and their informal caregivers identified challenges in accessing health services, particularly in acute settings. Examples provided by participants illustrate situations where accessing healthcare services exacerbated difficulties, such as feeling overlooked or misunderstood by healthcare professionals. Inadequate support and inappropriate care in hospitals underscored the urgent need for improved training and awareness among healthcare providers. Participants emphasised the need for training programs to be adaptable and responsive to the diverse needs and experiences of people with dementia. ‘And then, you know, they sent out an appointment for half 8 in the morning, even though you’ve told them “No, the public health nurse comes to help with insulin at half 9 we can’t be in the hospital at half 8.”.’ (Informal Caregiver, IE)
The emotional experiences of people with dementia were frequently discussed by interview participants. Self-experience training should integrate these sentiments to enable others to respond appropriately to the emotional aspects of living with dementia. People with dementia highlighted feelings of sadness and discomfort when cognitive symptoms manifested or when they attempted to conceal these vulnerabilities. They expect others to accept them as individual autonomous persons. Recognising the person beyond the dementia, a crucial prerequisite for person-centred care, was deemed important from their perspective. Participants emphasised that despite the challenges posed by the disease, people with dementia retain their unique identities, preferences, and emotions. ‘You kind of dodge around; try to hide it, especially from strangers who don’t know. I still do that, yes. But it’s not nice.’ (Person with dementia, DE)
Sub-Theme: Dementia Care Strategies and Skills
Participants described various strategies and skills for dealing with dementia that were suitable for teaching using innovative training methods.
Many participants stressed the need for training on collecting and using information about life history, preferences, and (residual) abilities in order to better understand and adapt care to the person with dementia. ‘Knowing my mother-in-law before she had dementia has helped hugely. And I knew what her personality was like, I knew what things she liked and didn’t like in very simple little things.’ (Informal Caregiver, IE)
Professionals experienced in the field of information technology or simulation learning noted that self-experience practices could facilitate empathy, compassion, respect, and open-mindedness. Additionally, according to informal caregivers and professionals, it is crucial to convey that the care of a person and their living environment can greatly influence the manifestation of symptoms. This underscores the significance of understanding how environmental and external factors influence the expression of dementia symptoms. ‘Even if they don't know who you are per se, but if you show the love or something like that, yes, then they react to that.’ (Informal Caregiver, NL)
People with dementia highlighted that others should adopt an attitude of seeking understanding rather than assuming knowledge towards people with dementia. ‘And I’m lucky enough not to be surrounded by people who think they all know about Alzheimer’s, and they tell you all about it.’ (Person with dementia, IE)
Consequently, professionals stressed the need for interactive and engaging dementia education, noting that traditional didactic teaching methods are outdated. In this context, all participants endorsed self-experience practices like roleplaying, augmented reality, gamification, virtual reality (VR), filming and theatre games.
Theme 3: Exploring Procedures, Processes and Activities in Self-Experience Training
Informal caregivers and professionals discussed training procedures, processes and activities related to self-experience practices.
They highlighted that understanding the lives of people with dementia is a continuous learning process influenced by personal experiences. Consequently, self-experience practices can provide participants with the necessary awareness and skills needed for constructive relationship building and person-centred care. ‘Working on oneself might be the starting point to reach the other person and create the relationship.’ (Professional, IT)
Participants stressed the importance of combining various techniques and strategies, using different tools, and changing perspectives for broad impact. Furthermore, they suggested that training should cover all types of dementia and aspects of care, including psychological, relational or practical, with sufficient time allocated.
Informal caregivers and professionals noted that self-experience practices can pose ethical challenges and overwhelm participants, especially in emotionally distressing situations. Thus, training programs should consider these factors and include safeguards to minimise potential distress. Participants emphasised the importance of reflection opportunities and highlighted that participants should be voluntary, with the option to withdraw at any time. ‘Although I must say and I think it might give it a bit of a negative perception of whatever you know, dementia is for everyone, but it’s good. It’s just ambiguous.’ (Professional, IE) ‘But I think there is always an ethical issue involved.’ (Professional, DE)
Theme 4: Considerations Across Diverse Participant Groups
Self-experience practices were deemed beneficial for various groups, including informal caregivers, health and social care professionals, students (e.g., from medical or nursing backgrounds), and the general population. Professionals and caregivers emphasised the training’s benefits for potential participants, group composition, adaption to target group, and personal prerequisites for participation in self-experience training. ‘I would love a training that really helps not only the person with dementia in the first place but the whole group, from the team, to the caregiver, to the family members who work in contact with the patient.’ (Professional, IT)
Participants highlighted the necessity of adapting the training to meet the specific needs of each target group, including content, timing and complexity. Consideration should be given to participants’ technology skills, particularly when involving different age groups. Younger participants could assist older ones, bridging the gap between different technological skill levels. ‘The young and the old generations of healthcare workers are very different in their way of thinking about IT tools; a connecting point has to be found because these two worlds are completely opposite.’ (Professional, IT)
Professionals emphasised the importance of a supportive learning environment; particularly as self-experience may evoke unwanted feelings or trauma. In this context, it is advisable that participants have sufficient knowledge and experience in dementia care, especially when using practices such as VR. ‘It may well be that someone is slightly traumatised by a self-experience because he may notice that he has made mistakes himself or perhaps, yes, that he feels he is involved in something.’ (Professional, DE)
Theme 5: Influence of Context and Participant Reaction on Implementation
Professionals pointed out the importance of considering specific conditions and equipment when conducting self-experience training. The effective implementation of such training presents a significant challenge due to various organisational, contextual and temporal factors. Therefore, self-experience training should be tailored to the particular setting or context, e.g., aligning with organisational goals. ‘So there’s another thing I suppose for anything that you do, it's having it there but it’s actually getting it implemented into practice is going to be the biggest challenge.’ (Professional, IE)
It is crucial to recognise and address the individual reactions and behaviours of participants during the implementation of self-experience training. The willingness of professionals to engage in training may be limited by their unfamiliarity with the technology, necessitating low-threshold access. Having a dedicated person within an institution to champion the training, providing technical, content-related and emotional support, seems to be essential. ‘Yes, and I think it should be easily accessible because if you have to put in a lot of energy to get it to the client, the time factor is really the limiting factor.’ (Professional, NL)
Theme 6: Facilitators, Challenges, and Perspectives
Interview participants discussed their views on self-experience training for dementia education, describing its perceived impacts and mechanisms.
Informal caregivers and professionals regarded self-experience as a valuable tool for teaching how to understand dementia and the individual experiencing it, as well as for fostering empathy. Encouraging participants in self-experience training to cultivate openness, empathy, and self-reflection is essential, as it provides the opportunity to step back and reflect on the significance of the dementia experience. Self-experience can improve communication and enable individuals to respond appropriately in various situations, allowing participants to see different perspectives. ‘Because talking about it is not the same as seeing, experiencing.’ (Professional, NL)
However, self-experience might inadvertently reinforce a negative portrayal of dementia, leading to a pessimistic view among participants. There were also concerns about whether the challenges depicted accurately reflect all dementia experiences.
Facilitating factors, from the view of informal caregivers and professionals, included VR’s strong impact on empathy and understanding the deficits experienced by people with dementia, roleplaying for situational assessment, theatre for perspective-taking, and films for public awareness. ‘Putting yourself in the other’s shoes is now possible with virtual reality; the human brain tends to learn more by listening to images than listening to what we are talking about, so it has a greater impact.’ (Professional, IT)
Barriers mentioned included the risk of generalising dementia through simulations like movies, the potential of VR to cause nausea or balance issues, and the artificial feeling of VR due to the challenge of maintaining a realistic simulation of dementia experiences over time. ‘But in the long run it is not seen as being real.’ (Informal Caregiver, NL)
Discussion
Our study aimed to develop a comprehensive understanding of the role of self-experience practices in enhancing person-centred care for people with dementia by exploring the perceptions and experiences of three key participant groups: people with dementia, informal caregivers and professionals. By employing a qualitative research approach, we were able to capture the nuanced perspectives and subjective experiences of each group.
Our findings suggest that comprehending dementia is challenging for healthcare professionals, informal caregivers and the broader public. Interview participants view self-experience practices as a promising approach for enhancing awareness and promoting person-centred care, highlighting the need for tailored training programmes.
A key finding of our study is that both the content and the strategies to be taught should be grounded in the experiences and needs of people with dementia. Gaps in knowledge among healthcare professionals can lead to inadequate support and stigmatisation, highlighting the need for enhanced caregiver training for dignified, person-centred care.
Actively involving people with dementia in the research process enriches the study with first-hand perspectives, promoting a nuanced understanding of their experiences (Conway et al., 2023; Williams et al., 2020). Flexible interview techniques, familiar environments for data collection, and providing support to enable effective communication can address these challenges (Collins et al., 2022; Conway et al., 2023).
Approaching the lived experience proves to be both the objective of self-experience practices and, simultaneously, the most significant challenge due to factors such as the inconsistency and unpredictability of symptoms or the difficulties in interpreting nonverbal signals. Another obstacle lies in the effective implementation, influenced by factors such as group composition, ethical considerations, costs required to finance the tools and the careful selection of self-experience practices and procedures that align with the context in which the participant supports the person with dementia.
Despite these challenges, interview participants believe the expected positive impact of self-experience practices outweighs the difficulties. Enhancing awareness and understanding of dementia may contribute to achieving the goal of individualised, tailored care. However, individuals with dementia emphasise that understanding their lived experience is in a constant state of tension, as also indicated by the meta-synthesis conducted by Górska et al., 2018. While they highlight the importance of empathetic and supportive attitudes from others, people with dementia also caution against overly protective support, which may undermine their autonomy and potentially lead to social isolation (Górska et al., 2018). This assertion aligns with our findings, emphasising the importance of recognising people with dementia as autonomous individuals. Therefore, it is crucial to use tailored dementia training measures that not only impart strategies and skills but also foster successful interaction and communication through a cooperative approach.
Understanding the lived experience of people with dementia holds promise for long-term care improvement, acknowledging the dynamic and complex interrelationship. Both formal and informal caregivers need to contribute by bringing distinct competencies into the interaction. Self-experience practices may help foster these skills. Bearman et al. (2015) demonstrate that simulation promotes empathy in health profession students while offering the opportunity to step into another’s role, though the outcome depends on the didactic method used. Clear conclusions are challenging due to the complexity and heterogeneity of the practices (Bearman et al., 2015). Our research supports these findings, as study participants indicate that generalised statements in support of self-experience practices are limited.
Our qualitative study emphasises the significance of reflection in dementia-specific self-experience training. Interview participants suggest that structured reflection helps to process experiences, leading to more meaningful learning outcomes. A systematic review on debriefing in healthcare education indicates that effective skills teaching can result from integrating debriefing as an integral component of the simulation experience (Levett-Jones & Lapkin, 2014). Reflection is regarded as a valuable tool for educating about dementia and cultivating a deeper understanding of (people with) dementia in our study. General perspectives on simulation in healthcare (INACSL Standards Committee, Watts, et al., 2021) outline specific criteria and recommendations for the debriefing process. Reflection and debriefing may help learners identify knowledge gaps and reconcile discrepancies between their perceptions and practice (INACSL Standards Committee, Decker, et al., 2021).
Emphasising the importance of psychological safety and the effective management of participant distress in self-experience training is imperative, as discussed by former literature on nursing and healthcare education (Henricksen et al., 2017; Kostovich et al., 2020). Among others, these insights underscore the need for ongoing dialogue and a vigilant approach to address ethical concerns within training programs, thereby ensuring the upholding of ethical principles such as dignity, respect and autonomy for all involved (Lateef, 2020; Slater et al., 2020).
Established views exist on training caregivers of people with dementia (Pleasant et al., 2020; Spector et al., 2016; Surr et al., 2020), as well as general guidelines on simulation techniques (INACSL Standards Committee, Watts, et al., 2021). While the relevance of these views is confirmed by some of our results, insights into the perspectives of people with dementia are lacking. Our study addresses this gap by involving relevant parties and providing a comprehensive understanding of the needs and challenges in person-centred dementia care. Our participants highlighted specific training scenarios and dementia care strategies that should be included in training programs. The scenarios are directly based on experiences of people with dementia, informal caregivers and professionals, which the interviewees found highly relevant for the training content. This unique approach of incorporating concrete examples from those directly affected makes our study different from others.
We expand existing knowledge on training methodologies by exploring self-experience practices, which cover a broad spectrum of training methods, including simulation approaches. At the same time, we identify challenges and opportunities related to the implementation of these training strategies. Therefore, our study can contribute to the groundwork for the direction and practical application of dementia-specific self-experience practices to enhance care and support for people with dementia.
Further research on the development, implementation, and evaluation of self-experience training programs is crucial. Investigating these topics in depth can provide a comprehensive understanding of the role of self-experience training in improving dementia care and can lead to recommendations to ensure program continuity. Integrating our findings into practice and fostering a feedback loop between practice and research can enhance the effectiveness and relevance of these training programs.
Strengths and Limitations
To ensure that self-experience training programs are developed based on diverse insights, we incorporated perspectives from people with dementia, informal caregivers, and professionals. People with dementia participated in data collection and provided feedback on interview guides, a significant strength given their challenging involvement in qualitative research (Conway et al., 2023; Phillipson & Hammond, 2018).
However, difficulties arose in recruiting people with dementia, exacerbated by stress during the SARS-CoV-2-pandemic and limited social contacts available to support their participation. Furthermore, individuals with moderate to severe dementia are underrepresented. This limitation is significant as their experiences may differ from those with milder symptoms, meaning the training scenarios may not fully capture this subgroup’s experiences.
Despite efforts to diversify professional backgrounds, most participants were nurses with educational experience. Recruitment from outpatient, acute inpatient, or geriatric settings proved challenging due to pandemic-related workloads. However, due to the online format of data collection, a smaller number of participants was deemed appropriate (Bolin et al., 2023; Tuttas, 2015).
Conclusion
Self-experience practices offer valuable approaches to addressing the challenges of person-centred dementia care. Integrating self-experience into training programs can enhance competencies and understanding among professionals and caregivers.
For successful implementation, appropriate frameworks and target group-specific approaches are essential. Our findings indicate that self-experience practices should not replicate a singular experience of living with dementia but foster awareness of the diversity and subjectivity inherent in these experiences. Self-experience practices should therefore equip participants to appreciate and adapt to this individuality.
Our research forms the basis for the development, implementation, conduction, and evaluation of self-experience practices in dementia training. Further research is crucial to accompany and evaluate the development and implementation of dementia-specific self-experience practices and to establish consensus-based recommendation for their use.
Supplemental Material
Supplemental Material - Enhancing Person-Centred Dementia Care Through Self-Experience: European Perspectives From a Qualitative Study
Supplemental Material for Enhancing Person-Centred Dementia Care Through Self-Experience: European Perspectives From a Qualitative Study by Janina Wittmann, Gabriele Meyer, Fania C. M. Dassen, Kealan Forristal, Louise Hopper, Niels Janssen, Marianna Riello, Marjolein de Vugt, and Anja Bieber in Dementia
Footnotes
Acknowledgements
The authors thank the interview participants who generously gave their time. Furthermore, this work relied on the support of many individuals and organisations, for which we are grateful. Thanks also go to the participating colleagues at the institutes who actively supported us in this work. In addition, we would like to specifically thank Social IT (Trento, Italy) for applying for funding, designing and organising the INTenSE project.
ORCID iDs
Ethical Considerations
This study has been carried out in accordance with the Declaration of Helsinki and national guidelines for research ethics. Each country applied for ethical approval from the responsible authority: DE: Ethics committee of the Medical Faculty, Martin Luther University Halle-Wittenberg (2020-234), IE: Dublin City University Research Ethics Committee (DCUREC/2021/016), IT: Clinical Research Ethics Committee of the Servizi Pastorali Educativi Sociali (SPES) Group after consultation with trade union representatives, NL: Maastricht University Ethics Committee (FHML-REC/2021/009).
Consent to Participate
All participants provided informed written consent. National regulations for the assessment of informed consent, particularly with regard to informed consent for people with dementia, were respected.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by EU Erasmus+ under Grant 2020-1-IT01-KA202-008426. The funding organisation did not influence the design of the study, the collection, analysis and interpretation of data or the content of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data supporting the findings of this study can be made available from the corresponding author (JW), upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.