
Abstract
Korsakoff’s syndrome (KS) is a neurocognitive disorder characterized by executive dysfunction, behavioral symptoms, and impaired awareness. In the Netherlands, people with KS and other alcohol-related brain disorders are cared for in specialized long-term care facilities (LTCFs). However, little is known about how formal caregivers working with people with KS in LTCF guide residents in daily practice. An ethnographic study was conducted over six months in two LTCFs. Using an apprenticeship-inspired approach, a partially participating researcher observed caregivers (nursing assistants, nurses and social workers) during work shifts, with informal interviews complementing observations. Through thematic analysis conducted by three researchers, three guiding patterns were identified. Behavior-centered guidance (1) aims to promote desired behavior through clear rules and direct communication. Caregivers following this approach value being firm and consistent as a way to support residents’ independence and overall quality of life. Person-centered guidance (2) focuses on building connections through care by getting to know residents and working together with them. Caregivers in this pattern value attending to and understanding residents, treating them as individuals rather than defining them by their disease. Care-task-centered guidance (3) aims to keep things on track by prioritizing the completion of household and care tasks. Caregivers following this approach are practical and rational, adjusting their methods to prioritize task flow rather than resident interaction. Although caregivers had a preferred guiding pattern, they shifted between patterns depending on the resident and varying circumstances. These findings contribute to a deeper understanding of caregiving dynamics and offers opportunities for reflection and team development within LTCFs.
Keywords
Introduction
Korsakoff’s syndrome (KS) is a neurocognitive disorder arising from thiamine deficiency, most often due to malnutrition associated with alcohol misuse (Kopelman et al., 2009). People with KS typically have cognitive impairments, particularly amnesia, often accompanied by executive dysfunction, while general intelligence remains preserved (Brion et al., 2014; Van Oort & Kessels, 2009). Because individuals with KS and other alcohol-related cognitive disorders require specialized support, care in the Netherlands is often delivered in specialized long-term care facilities (LTCFs). In these LTCFs behavioral symptoms—such as irritability, agitation and disinhibition—are common in residents, and more than half of the residents have a psychiatric comorbid condition (Gerridzen et al., 2018; Gerridzen & Goossensen, 2014). Moreover, 70% of people with KS living in LTCFs have impaired awareness of their functioning and 71% of all residents receive psychotropic drugs (Gerridzen et al., 2019). These characteristics shape the everyday context in which formal caregivers interact with residents, highlighting the importance of understanding how guidance of people with KS takes place. In this study, “guidance” refers to caregivers’ actions that encompass both direct care and supportive interactions, including assisting with daily activities, promoting independence, and providing instruction or coaching (Botana Gronek et al., 2025).
Given the complex care context, caregivers require effective strategies to guide people with KS, as highlighted in previous qualitative studies with formal caregivers. In a focus group study on impaired awareness, caregivers reported adapting their caregiving strategies to residents depending on the situation and their knowledge of each resident’s characteristics (de Groot et al., 2026). Additionally, an interview study explored caregivers’ perceptions of what constitutes good care and how caregiving approaches were implemented in daily practice. The study identified three distinct perspectives on good care: making daily life a joint effort, being steadfast, and treating residents with respect (Gerridzen et al., 2021). To support caregivers, a specific training program in empathetic–directive guidance has been developed, which trains caregivers to provide clear, goal-directed guidance to residents in an empathetic manner (Van Noppen et al., 2008). However, although caregivers receive training and their descriptions and feelings about providing guidance have been explored, little is known about how they actually interact with and guide people with KS in daily practice.
To address this gap, the present study uses ethnographic field research to examine how caregivers guide residents in daily practice, capturing both their beliefs and actions within the real-world context in which they occur (Savage, 2000). While this method has previously been used in dementia research to explore person-centered care (Doyle & Rubinstein, 2014; Stokke et al., 2023), relational care (Sandvoll et al., 2012; Ward et al., 2008; Watson, 2019), and trust-building (Thorsen & Nielsen, 2023) it has not previously been used in KS research.
Methods
Study Design
This short-term ethnographic field study examined how formal caregivers provide guidance and interact with residents in specialized LTCFs for people with Korsakoff’s syndrome (KS) or other alcohol-related brain disorders (Pink & Morgan, 2013). We adopted an interpretivist–constructivist epistemology, viewing knowledge of caregiver practices as emerging both from participants’ perspectives and through the researcher’s reflexive engagement with the field (Green, 2009).
Over a six-month period between 2024-2025, caregivers in two LTCFs were primarily observed during day shifts, with additional observations in the evening, and on weekends to capture variation in daily routines. Data were gathered until data saturation occurred, defined as the point at which additional caregiver observations no longer generated new codes or guiding-related insights, as assessed by the researchers (EG, MD, MB, IG). The primary researcher (EG), a female elderly care specialist in training and PhD-student with prior training in qualitative research and experience as a care assistant and physician in LTCFs for people with dementia and KS, performed participatory observations by assisting caregivers. This apprenticeship-like positioning (Pink, 2015) involved performing small supportive tasks, such as handing over items or helping residents with dressing, in line with ethical standards given her prior training. Such practices enabled close collaboration with caregivers, built rapport, and allowed observation not only in communal living areas but also, with consent, in residents’ private rooms. Observations during team meetings and breaks provided insight into collective thought processes and team dynamics, while strengthening relationships with caregivers. Informal interviews were conducted throughout the observation period to clarify observed practices and explore caregivers’ underlying motives.
From a reflexive perspective, the researcher’s background as a physician facilitated access and rapport but may also have shaped observations and interpretations. To enhance reflexivity, field notes included reflections on assumptions, and interpretations were discussed within a multidisciplinary research team (including expertise from psychology, physiotherapy, movement science, elderly care medicine and philosophy) to challenge potential biases. Preliminary findings were shared with participating caregivers to refine interpretations before finalizing the results. A topic guide was intentionally not used, allowing guiding-related topics to emerge inductively during data collection. This study followed the COREQ guidelines (Appendix 1) to ensure comprehensive and transparent reporting of the research process (Tong et al., 2007).
Recruitment and Ethics
The Dutch Korsakoff Knowledge Centre (KKC) awarded a grant to IG for this study, which was then embedded in LTCF1. The research coordinator (YZ) and local managers of LTCF1 selected a ward with caregivers interested in participating. LTCF 2, also affiliated with the KKC, was invited to participate, with management recommending the observed ward. Study information, including the observation method and research question, was shared internally with caregivers prior to the observer’s (EG) introduction.
The observer (EG) was briefly introduced to caregivers during shift changes at the participating ward of LTCF1 and during a coffee break at LTCF2. Initially, caregivers were included based on interest. Subsequently, participants were included based on variation in age, professional background, and caregiving experience. Caregivers included were nursing assistants, vocational nurses, secondary vocational nurses, registered nurses, and in LTCF1, social workers with equivalent caregiving roles, all employed by the LTCF. After verbal and written informed consent was obtained observation schedules were then planned with the participating caregivers.
As the aim of this study was to explore guidance from the perspective of caregivers, residents were not included as participants, as including both perspectives could have biased researchers’ interpretation and was beyond the scope of the study. To safeguard resident privacy, an opt-out procedure was applied: residents and their representatives were informed about the study and could decline observation at any time. At the beginning of the study, information was provided by both caregivers and the observer. During observations, residents could always decline the observer’s presence in their private rooms. The observer, together with caregivers, monitored residents’ comfort and left immediately if a resident expressed refusal or showed signs of agitation or distress. The names of caregivers and residents were pseudonymized, and caregivers’ ages were reported in ranges to prevent traceability and safeguard privacy. The medical ethics review committee of the Amsterdam University Medical Center approved the study protocol (file no. 2024.0424) and confirmed that the Medical Research Involving Human Subjects Act (WMO) did not apply.
Study Setting
Demographics of the Long Term Care Facilities and Wards
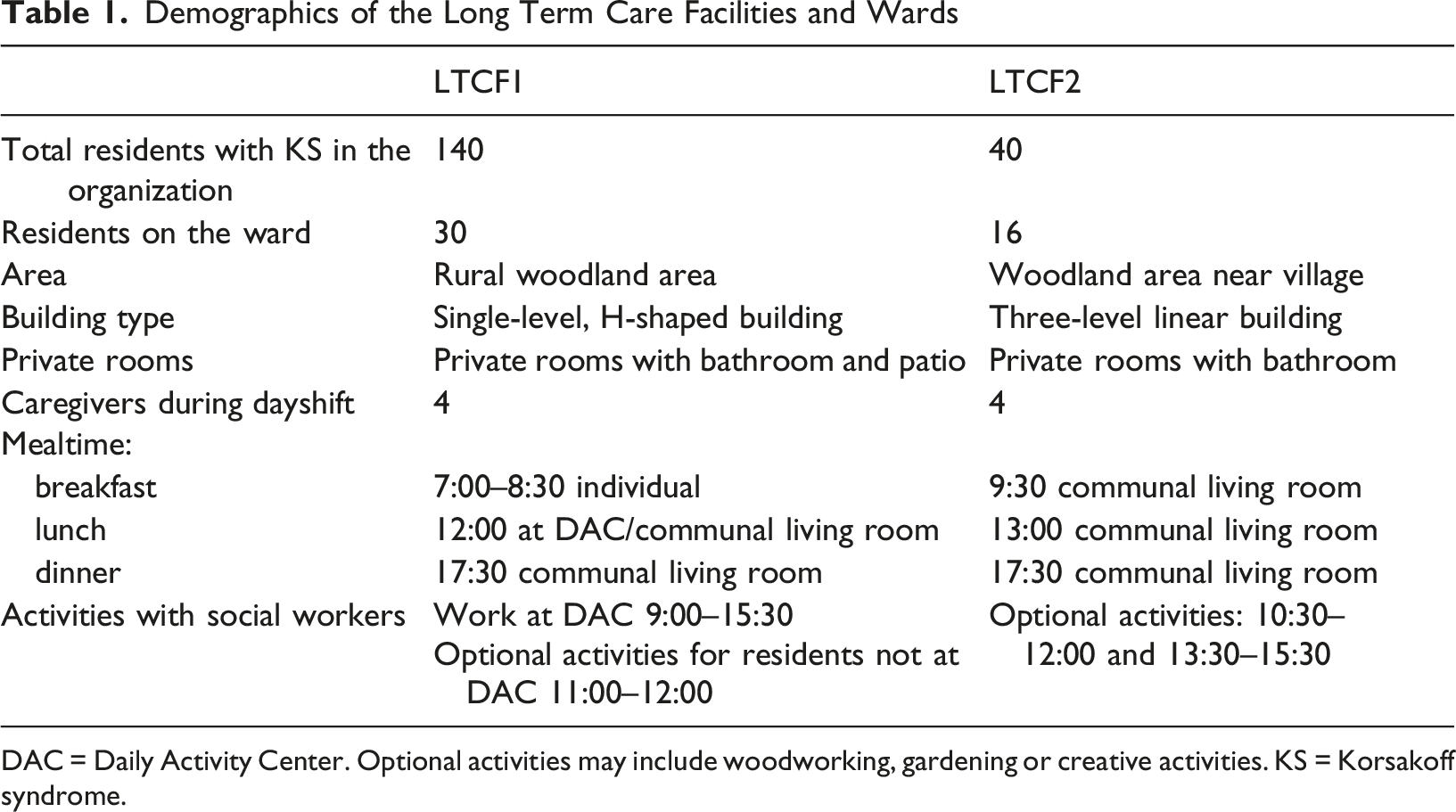
DAC = Daily Activity Center. Optional activities may include woodworking, gardening or creative activities. KS = Korsakoff syndrome.
Data-Collection and Analyses
Fieldnotes were taken every 15–30 min during observations using a secure dictation application, recording keywords and conversations chronologically. Within 24 hr, these were elaborated into detailed reports combining descriptive accounts with reflections on the observer’s thoughts, feelings, and emerging ideas about caregiver guidance. Reports were read and re-read, by EG, MD, MB, and IG to facilitate data familiarization. Two researchers (EG and IG) independently coded the data, compared codes and discussed discrepancies to reach consensus and develop the codebook. Data were coded iteratively using MAXQDA Analytics Pro 2024 (VERBI Software, Berlin, Germany) during the observation period, revisiting earlier reports to ensure consistency and rigor, in line with Braun and Clarke’s (2006) approach to thematic analysis. Initial codes captured all aspects of guiding (e.g., events, resident behaviors, guiding approaches, caregiver motivations, and moods) which were iteratively reviewed and refined into candidate themes. Simultaneously, EG and MD summarized the guiding approach of each caregiver to understand the meaning of practices and motivations, informing theme development. Regular team discussions (EG, MD, MB, IG) ensured researcher triangulation, consensus, integration of findings, and reflection on the reports. This iterative cycle of observation, reflection, and analysis, consistent with an ethnographic–theoretical dialogue approach (Pink & Morgan, 2013), allowed themes—including the three final guidance patterns—to emerge inductively from the data.
Results
Participant Characteristics
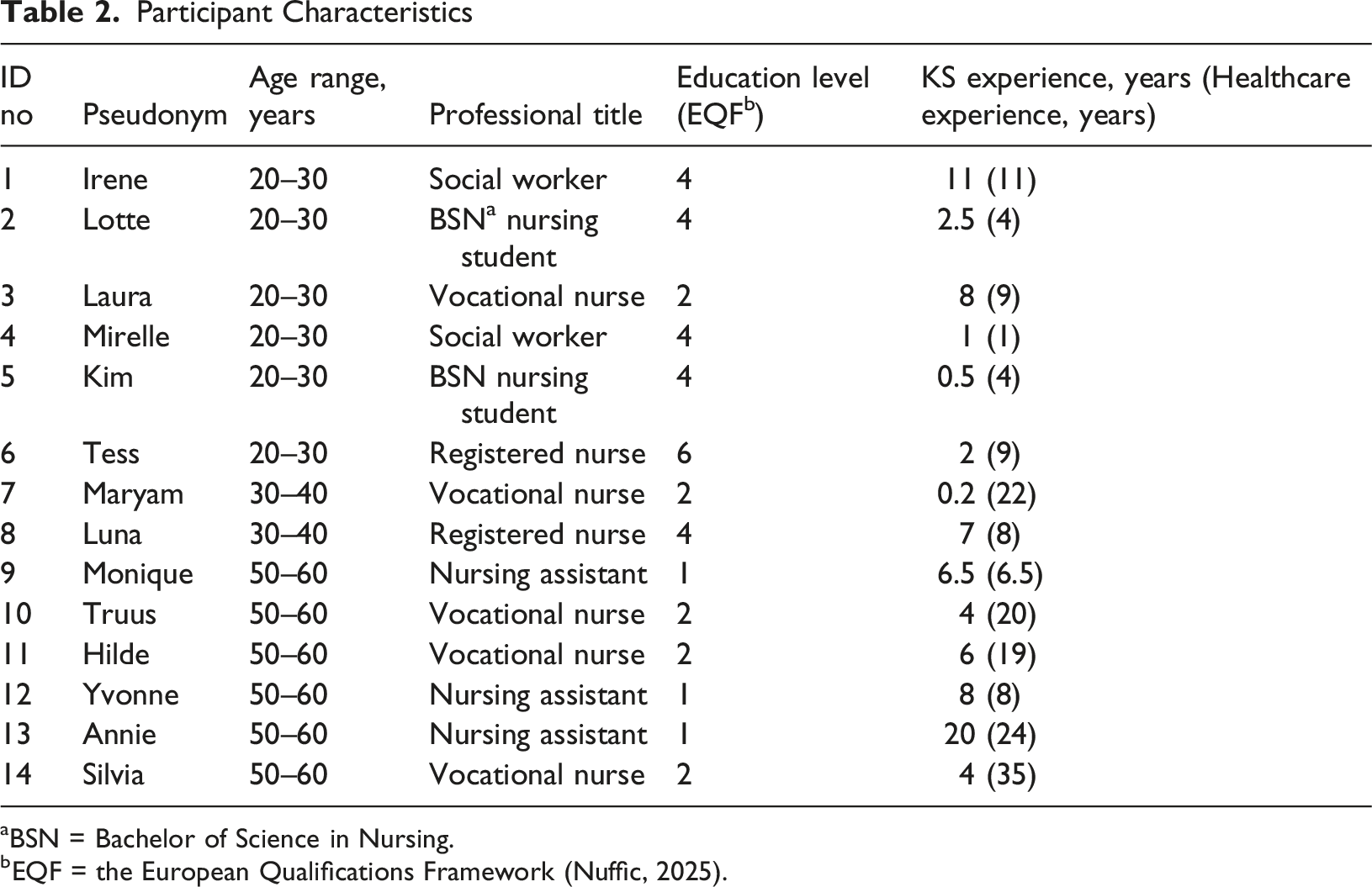
aBSN = Bachelor of Science in Nursing.
bEQF = the European Qualifications Framework (Nuffic, 2025).
Guiding Patterns and Characteristics
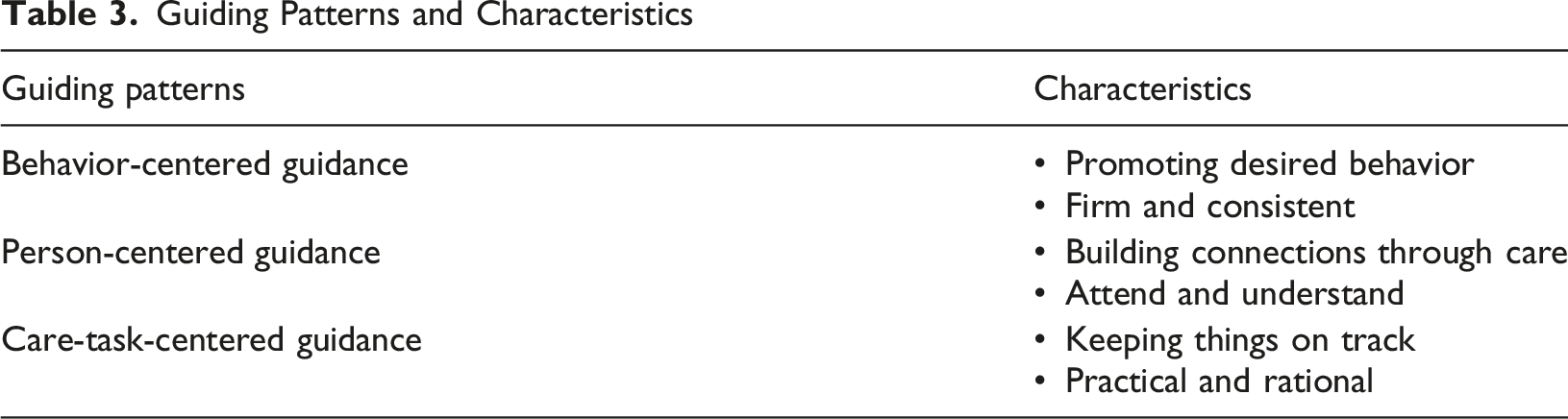
Behavior-Centered Guidance
The behavior-centered guidance pattern focuses on promoting desired behavior, using strategies, such as rules, rewards and humor. This pattern is grounded in the caregivers’ belief that being firm and consistent helps to create a predictable environment on the ward, supports responsibility among residents, and enhances quality of life. This approach was frequently described during team meetings as the standard on the ward, reflecting what most caregivers practiced and had learned during training. Caregivers noted that following this approach was expected and reinforced by colleagues, shaping routine practice.
Promoting Desired Behavior
Clear rules and structured routines, such as showering before breakfast, are maintained to shape residents’ behavior toward what caregivers consider appropriate. Cooperation among reluctant residents is further encouraged by rewarding them with everyday provisions, such as breakfast or cigarettes: resident Peter: “I feel like having a nice breakfast.” Caregiver Luna: “Yes, that’s fine, but first you need to shower.” Peter: “I don’t want to shower.” Luna: “Then just wash at the sink.” Peter: “Can I have a cigarette?” Luna: “Once you’ve washed.” Moreover, caregivers ensure that residents do not take advantage of one another and intervene when they fail to fulfill their own responsibilities or take over the tasks of other residents, as illustrated in this observation when most residents had finished their breakfast: Resident Vera stacks all the plates and cutlery from her table. Caregiver Monique notices the stack and says firmly: “Vera, how many times have we told you that everyone must clean up their own things?” Vera calmly replies: “Yes, but it prevents the kitchen from getting too crowded.” Monique, also calmly, responds: “Yes, but we have the agreement that everyone cleans up their own things.
Caregivers adopting this pattern aim to influence residents’ behavior by being direct in their communication and actively responding to residents’ inappropriate behavior to educate them. They do not shy away from confronting residents when needed, especially if it helps to set boundaries. Such interactions reflect a broader educational and corrective orientation in which caregivers see behavioral guidance as part of their professional role. For instance when caregiver Mirelle takes cigarettes from the cabinet to hand out to residents, she tells resident George in a neutral and friendly tone: “Go ahead, but put your coat on first.” George shouts angrily: “NO!” Mirelle responds firmly: “Come on, behave normally.” George, still angry but slightly quieter, asks: “Where is my coat?” Mirelle points behind him: “On the coat rack.” After that George and two other residents put on their coats.
Sometimes these interactions involve a playful yet strategic back-and-forth between the resident and caregiver, where the resident pushes back and the caregiver responds with increasing authority, as illustrated by the interaction between caregiver Irene and resident Robert: Irene cheerfully says to Robert, “Good morning, happy to see us?” He lets out a loud fart. Irene looks on, disgusted, clearly expecting this reaction. She walks over to him and says firmly in a commanding tone: “I’m putting on the support stockings,” at which Robert extends his leg. She calmly puts the stocking on using the aid. “Ouch!” Robert says angrily, glaring at Irene. “What ouch?!” Irene exclaims disapprovingly, then turns to me and jokes, “You wouldn’t think he played ice hockey and soccer.” These examples highlight how caregivers use a mix of directness, humor, and relational authority to steer residents toward desired behavior, with humor also serving to maintain behavioral expectations even when residents initially resist.
Firm and Consistent
Firmness involves maintaining boundaries and expecting respect from residents, reflecting the view that caregiving should not resemble service work, as Yvonne illustrated when a resident immediately demanded a sandwich, by stating: “I’m not going to drop everything for him right away, this isn’t a hotel.” Caregivers within this pattern encourage residents to take responsibility and perform tasks they are capable of, without unnecessary assistance or exploiting the helpfulness of fellow residents, as Monique explained regarding a resident who tended to take over others’ tasks: “Yes, everyone has a task, some more than others because they are able and enjoy it. But in this way, Vera takes over a lot, which isn’t fair to the others, and it’s not enjoyable for her either.” Caregivers emphasized the importance of team consistency, especially regarding rules and structured routines, to ensure coherent care practices. Accordingly, they valued individual care plans as tools to coordinate their approach, yet some caregivers expressed frustration with coworkers’ more lenient approaches, fearing that such leniency could undermine established rules and desired behaviors. The tension between firm and lenient approaches became apparent during discussions about dietary restrictions between coworkers Luna and Yvonne. Luna: “Did you give [resident] Peter chocolate spread on his bread?” Yvonne responds with: “No, he’s not allowed to have that. He has diabetes and eats without restraint.” Luna: “He’s allowed to have it once in a while.” Yvonne: “Yes, but we don’t have any right now. And if we give it to him, he’ll want it every day.” Additionally, this exchange illustrates how caregivers in this pattern frame decision-making as protective and preventive, prioritizing perceived long-term wellbeing over immediate preferences. Another motivation for using a firm and consistent approach is the caregivers’ believe that it enhances residents’ quality of life, as Irene describes why she uses this approach: “The residents often show little initiative, but once they start doing something or get out of bed, they do experience some enjoyment from it.” At times, this motivation to enhance the quality of life for residents led caregivers to overrule residents’ choices in everyday matters, as Monique demonstrated when discussing clothing options with resident Cornelia. Monique takes a blouse from the closet, holds it up in the air, and says cheerfully, “This black blouse?” Cornelia: “Yes.” Monique: “All fancy and stylish!” Cornelia looks at her skeptically, and says (annoyed): “Why does everything have to get washed? That’s not necessary.” Monique (in a neutral tone): “Well, sometimes you sleep in your top, and then it’s not very clean anymore. I’ll just look for a black undershirt…” Cornelia: “White is fine too, you know.” Monique: “White shows through.” Cornelia looks annoyed and says, “Well, I’ll just go to the toilet then.” Monique (laughing): “Good idea.” Monique later explained: “Cornelia believes it’s important to look neat, and she always has her nails polished.” In this case, Monique made decisions regarding clothing based on her own perception of Cornelia’s personal preferences. These examples reflect how caregivers within this pattern understand their role as actively supporting residents’ engagement and well-being, even when this involves guiding or structuring choices on their behalf.
Person-Centered Guidance
The person-centered guidance pattern focuses on building connections through care by finding moments of closeness in everyday activities. Caregivers apply this approach through strategies such as listening, affirming residents’ preferences, and engaging in shared activities. This pattern reflects the caregiver’s belief that they should attend to and understand residents as individuals rather than care recipients, emphasizing empathy, reciprocity, and relational equality. In contrast to the behavior-centered pattern, caregivers favoring a person-centered approach questioned the emphasis on firm and consistent communication as best practice and felt it did not align with their personal way of interacting.
Building Connections Through Care
In this guiding pattern, the caregivers’ aim is to “foster a sense of home for the residents”(Hilde). Caregivers learn about residents’ past lives and current preferences to better understand their needs and form meaningful connections. These connections are established by asking how residents are and, as caregiver Silvia shows, offering help: “Shall I braid your hair around 10:30?” Resident Victoria replies: “Thank you, if you have time, that would be great.” Silvia: “I know you like your braid neatly down your back. I’ll make time for you!” Across these moments, the emphasis lies on relating to residents as people first.
During interactions, caregivers listen attentively and respond affirmatively, using residents’ stories to build rapport and encourage cooperation with care routines: caregiver Annie walks to the door, knocks, peeks around the corner, and chuckles softly. With a playful tone, she asks, “Already back in bed?” Resident Cornelia looks up from her bed and laughs: “Yes, it’s cold and I wanted to sleep a bit longer.” Annie calmly encourages her: “Time for a shower.” Cornelia protests lightly, “I think that’s ridiculous. It doesn’t have to be every day.” Annie asks gently, “Did you do anything nice with your son on Friday?” Cornelia’s expression relaxes, and she slowly sits up: “My son is visiting today. He’s bringing my grandson.” Annie smiles: “How lovely!” She opens the bathroom door and says, “Come on, let’s go to the shower.” Cornelia rises and follows Annie with her walker. “Quickly, then,” she mutters, and Annie replies, “Yes, we will.” Here, emotional engagement and conversational continuity are used as means to support cooperation while maintaining relational closeness.
Care tasks, such as cleaning and cooking, are considered as opportunities for making social connections. For example, caregiver Laura shows how participation happens in a relaxed and supportive way when she stands by a resident and offers: “Shall I help you?” They then load the dishwasher together while chatting casually.” In these moments, tasks are also used to foster a sense of purpose and support residents in making their own decisions. This was illustrated by caregiver Hilde’s interaction with resident Edward, who was agitated and sad following his recent admission to the ward: Hilde takes some vegetables from the fridge and says, “Maybe we can ask Edward if he wants to help—he might enjoy that.” Later, during cooking, Hilde explains that the spices need to be added to the vegetables and asks Edward, “How do you usually do this? Dissolve in water first or put it straight in the pan and add some water?” Edward replies, “Straight in the pan.” Hilde hands him the spice packet, and he adds it to the pan.
Caregivers sometimes find it challenging when residents do not cooperate with each other during tasks or activities, such as cleaning plates or playing a game, and may hesitate about whether to intervene. In such situations, these caregivers often try to lighten the mood or gently redirect attention to maintain a positive group dynamic. When residents do help each other and no one seems to mind, caregivers acknowledge and appreciate these moments of support: caregiver Maryam: “[resident] Willy, can you clear the table?” Willy: “No, I’m not doing anything.” Meanwhile, resident Vera has already stacked everything and is now wiping the table with a cloth. Maryam: “Ah, Vera has already done everything. Lucky you, Willy!” Willy: “Yes, Vera is so kind.” In this case, the caregivers’ positive acknowledgment of a resident’s helpfulness appeared to foster more meaningful social interactions.
Attend and Understand
Attending to residents involves standing with them and perceiving them as unique individuals, rather than defining them by their disease. By acknowledging residents’ perspectives, caregivers foster relational equality despite the inherent hierarchy in the LTCF. To support this equality, caregivers reflect on their own preferences and recognize that residents might feel similarly in comparable situations: Caregiver Tess: “Yes, and residents have to have whole-grain bread. What nonsense. If someone wants white bread, shouldn’t that be allowed too? It should be enjoyable. And another thing—it’s not like we’re supposed to be ‘raising’ the residents. Besides, we’re not that strict about what we eat ourselves.”
This effort to relate as equals is grounded in compassion, which becomes visible in everyday interactions, such as apologizing when appropriate, offering suggestions rather than instructions, and respecting residents’ decisions even when advice is declined: caregiver Annie, in a friendly tone: “Hey [resident] Cornelia, would you maybe like a different kind of bra?” Cornelia, in a neutral tone: “No, this one feels fine.” Annie: “Yes, but it’s always hard to get it on and off over your head, and it hurts your arm every time. With one of those clasp ones in the back, you wouldn’t have that problem.” Cornelia: “No, I’m fine with it like this.” Annie: “Okay, whatever works for you—but now you know it’s an option.” This reflects an underlying effort to position care as relational rather than directive, with equality and shared humanity as guiding principles.
This person-centered guidance pattern becomes even more apparent when caregivers have to work alongside colleagues who, for instance, follow a behavior-centered pattern to manage situations: resident Johan is angry: “I want bread!” caregiver Truus responds, “You know lunch is at 12:00. You should have come then.” Coworker Hilde walks over and says to Truus, in Johan’s presence, “A cookie is fine.” Hilde and Truus walk to the pantry, and Hilde takes out the cookies. Truus remarks, “We have set some rules; we need to stick to them.” Hilde replies, “I don’t like it when Johan is hungry.” Here, Hilde prioritizes the resident’s wish over strict adherence to routine, demonstrating the empathetic and flexible approach characteristic of person-centered guidance. To support this approach, individual care plans are consulted to understand and respect residents’ needs and wishes, in contrast to the behavior-centered pattern, where they were used primarily to ensure coherent care practices.
Care-Task-Centered Guidance
The main aim of the care-task–centered guidance pattern is to keep things on track, prioritizing the timely and proper completion of planned daily activities—such as washing, dressing, and administering medication. Caregivers who adopt this pattern are practical and rational, operating from their belief that continuity and efficient task completion are essential both for completing work within the shift and for maintaining residents’ physical well-being. This reflects an underlying logic of prioritization, in which care is organized around task completion as the primary condition for safe and reliable care delivery. Especially when understaffed or when additional tasks arise—such as meetings or writing reports—this approach becomes more prominent.
Keep Things on Track
To move things forward, residents are guided in a calm and gentle way, determined to complete all care tasks, even when residents resist. For example, caregiver Kim gently prompts resident David with “Were you sleeping comfortably?” and, in a slightly commanding but friendly tone, adds, “I have your medication here,” encouraging him to take it, while also guiding him to where he needs to be with “Okay, we’ll see you shortly in the living room.” Determination to keep things on track becomes particularly clear when caregiver Truus insists on proper hygiene, despite resistance: Truus picks up the dirty clothes and says, “This is dirty and needs to go in the laundry,” sticking to her decision even though resident Walter protests angrily, “NO, it’s CLEAN.” Truus responds gently but firmly, “Yes, it’s dirty,” before leaving the room with the laundry ignoring Walter’s wish to keep it. These interactions illustrate a guiding logic in which task completion is prioritized over negotiation of preferences when the two come into conflict.
This task-oriented perspective shapes how caregivers evaluate their coworkers’ contributions, with frustration particularly directed at those who fail to take initiative, as incomplete tasks can disrupt both the efficiency of the ward and the physical well-being of residents. As Truus explains about younger coworkers: “They leave a lot of things undone, like dishes still sitting on the counter. They don’t ask what they can do or take action on their own. Having to guide them and tell them what to do is tiresome.” Similarly, Mirelle notes: “It can be difficult sometimes. I might come to a client and notice that something hasn’t been done, like providing clean clothes. That really bothers me.” Here, effectiveness and continuity of care are not only practical concerns but also normative expectations that define “good” caregiving within this pattern.
Interpersonal conflicts among residents are usually not addressed when leaving them alone is the more practical option, allowing caregivers to focus on other tasks while disagreements settle naturally. Intervening in resident interactions typically occur only when broader consequences arise, such as escalating aggression or a running out of cigarettes. Caregiver Truus: “Don’t you have any tobacco?” resident Bart: “No, I’m smoking someone else’s.” Truus: “We’re not going to do that. Don’t give him any,” she tells the other residents. “Bart, you’ve got enough money to buy your own.” Later Truus explains: “I don’t think it’s okay that he smokes from others. Also, we wouldn’t have enough tobacco if that keeps happening.” This illustrates a pragmatic threshold for intervention, where relational issues are addressed primarily when they threaten order, fairness, or resource management.
Practical and Rational
Caregivers following this pattern value a practical and straightforward approach, as caregiver Mirelle mentioned “All that fussing over residents isn’t really for me; I’m more practical.” Which is reflected in her routine of preparing plates with sandwiches in plastic wrap while commenting “In this living room everything is prepared in advance, because the residents always eat the same and they’re not able to prepare it themselves. To stay organized and focused on care tasks, these caregivers adhere to their own work routines: Annie “I like to do things my own way; otherwise, I get confused about what needs to be done.” Accordingly, unnecessary changes to routines on the ward are unwelcome, as Annie continues: “Some people, like new colleagues and management, want to change things on the ward, but if it’s working, it’s working, right?” When these caregivers do have to adapt their routines—for instance when time or staffing is limited—extras and personalized touches are often set aside. Mirelle explained during an understaffed shift “Normally we always cook eggs on Sundays, but it’s going to be hectic today, so I’m not going to do that now,” thereby skipping a non-essential ritual as they prioritize getting essential work done. Caregivers following this approach rely on their own experience and practical solutions rather than consulting individual care plans or coworkers, which can be time-consuming, as Sylvia notes, “I know what I am doing.” This reflects a focus on continuity and efficiency, with caregivers drawing primarily on their own routines and experience. Overall, this pattern reflects a form of situated pragmatism in which efficiency, predictability, and self-reliance function as organizing principles of care delivery.
Caregivers adopting the care-task-centered guidance pattern emphasized the importance of adjusting their approach based on the individual resident, as Luna reflected on differing guiding approaches: “You need to really know the resident to understand what works. When I started here a few years ago, I would just give up if someone didn’t want to get out of bed. Now I’ve learned that it’s important to adapt your approach and find what motivates each resident.” This illustrates that, although caregivers may have a preferred guidance pattern, they can learn to adapt their approach to meet the individual needs of each resident.”
Discussion
To our knowledge, this is the first ethnographic study examining how caregivers guide people with KS in daily work in LTCFs. Three guiding patterns were identified. The behavior-centered guiding pattern is characterized by a focus on promoting desired behavior using strategies such as rules, rewards, and humor. Caregivers following this pattern expressed the belief that being firm and consistent helps residents in their responsibility and quality of life. The person-centered guiding pattern emphasizes building connections through care, often by engaging in everyday activities together. These caregivers use listening, attending and understanding residents as key strategies and they view residents primarily as fellow human beings instead of patients with a specific disease. The care-task-centered guiding pattern focuses on keeping things on track, with caregivers adjusting their approach to achieve this goal. These caregivers describe themselves as practical and rational, prioritizing the completion of daily care activities over extended interactions with residents. While caregivers generally adhered to one predominant guiding pattern, the findings suggest they adapted depending on resident needs, situational context, and interactions with coworkers.
In the behavior-centered guidance pattern, caregiving primarily revolved around residents’ behaviors and the perceived implications of these behaviors. This orientation may reflect the longstanding emphasis on biomedical and behavioral approaches in the care of people with KS (Oudman et al., 2017). Care for people with KS was traditionally guided by the 4K-model, which emphasizes short, concrete, and concise communication alongside a structured daily routine. This model has evolved into the Empathic Directive Approach, a caregiver training program that incorporates principles of attentiveness (Klaver & Baart, 2011) to promote resident guidance through clear, goal-directed communication delivered with empathy (Van Noppen et al., 2008). Although this training offers a valuable practical framework developed by experienced caregivers, it is based primarily on practice and has not yet been empirically tested. Notably, while training programs emphasize empathy, the behavior-centered pattern identified in this study is more paternalistic, prioritizing control and directiveness over responsiveness to residents’ preferences. Although this approach may be effective in stimulating residents, it may also contribute to loss of autonomy and the processes of othering (Doyle & Rubinstein, 2014)—that is, viewing them primarily through the lens of their impairments or care needs rather than as individuals with their own perspectives, thereby limiting their sense of agency. It remains unclear whether this approach aligns with residents’ own wishes or genuinely serves their best interests.
In contrast to the behavior-centered guidance pattern, the person-centered guidance pattern is focused on the resident as a person, rather than allowing the disease and its symptoms to define them. The principles of the person-centered guidance pattern align closely with the concept of person-centered care, emphasizing support for individual identity, autonomy, and relationships to meet each residents’ needs (Kitwood, 1997; Sabat & Harré, 1992). Another related concept is relational care, which sees care not merely as completing tasks but as an ongoing, reciprocal process shaped by interpersonal relationships and the wider organizational and social context (Novy et al., 2023). In an ethnographic study on trust in interpersonal care, Thorsen and Nielsen (2023) showed that trust between people with dementia and their caregivers is fundamental to interpersonal care. Building trust goes beyond verbal communication, involving “primordial” emotional and relational aspects—such as the tone and mood set by caregivers—that influence whether individuals feel safe to accept care. As Thorsen and Nielsen note, the relational and social dimensions of caregiving are not separate from nursing tasks but form the foundation that makes these tasks possible. This perspective aligns with the principles of person-centered guidance, where attention to social and relational aspects is considered essential for effectively carrying out practical caregiving tasks for individuals with KS.
Interestingly, whereas the behavior-centered and person-centered guidance patterns focused on interaction with the resident, the care-task-centered guidance pattern focused primarily on physical well-being, such as care activities and household duties. Other ethnographic studies on dementia care showed that although caregivers strove to attend to the social aspects of caregiving, they were constrained by a rigid healthcare paradigm prioritizing residents’ physiological well-being and imposed strict time limits on tasks such as assisting with toilet visits (Stokke et al., 2023; Thorsen & Nielsen, 2023; Ward et al., 2008). These constraints were also experienced by caregivers in the current study and at times prompted a shift toward a care-task-centered pattern. However, the emphasis on physical well-being and household tasks seemed in some cases self-imposed, as caregivers who preferred this pattern derived a sense of fulfillment from completing care tasks and took pride in their practical approach. A similar practical orientation was reported by Sandvoll et al. (2012) in an ethnographic study on the implementation of new quality regulations in dementia care, where caregivers were primarily task-focused and relied on experiential knowledge in their daily work. Taken together, these findings suggest that while task-focused care can be practical and rewarding for caregivers, it may also limit opportunities to engage in more person-centered forms of guidance and, as Gilmore-Bykovskyi et al. (2015) found, may be associated with increased behavioral expressions when residents’ individual needs are overlooked.
Gerridzen et al. (2021) examined professional caregivers’ perspectives on good care for people with KS, identifying three views on good care—making daily life a joint effort, being steadfast, and treating residents with respect—which reflect core care values. The present study builds on this by showing how these values take shape in everyday caregiving practices through the guiding patterns used by caregivers. These guiding patterns show parallels with established care paradigms, such as person-centered and more biomedical or task-oriented approaches. Their contribution, however, lies in integrating these orientations into a single framework that captures how caregiving is enacted in practice for people with KS. This framework illustrates how caregivers navigate and balance resident needs, routines, and contextual constraints. It also offers a tool for reflection at both the individual and team level by making differences in approach more visible and open to discussion—an aspect caregivers in this study experienced as challenging. Although developed in the context of KS care, the patterns resonate with care paradigms described in dementia research, suggesting broader relevance for understanding caregiving practices in other long-term care settings.
Strengths and Limitations
A key strength of this study is its unique focus on the everyday interactions between care staff and KS-residents, enabled by a natural and participatory observational approach. This method provided valuable insights into real-life practices and in-the-moment reflections, avoiding the recall bias often associated with retrospective self-reports. However, this approach may have limited access to deeper perspectives, such as how staff members evaluate their workday, which might have emerged through the use of formal interviews.
Observation periods varied between participants, ranging from one to three days, which may have introduced some representation bias, as certain caregivers were captured in greater depth than others. To address this, additional informal conversations were held with staff during breaks and on non-observation days, helping to balance these differences. Observations were conducted across different shifts—day, evening, and weekend—enhancing the comprehensiveness of the data. However, most observations took place during day shifts. No observations were conducted during organized daytime activities, as the study focused on direct care rather than activity facilitation. Including observations during daytime activities in future research may provide valuable insights into different aspects of care.
A limitation of this study is the homogeneous sample, all caregivers were female, and only one had a different cultural background, limiting analysis of diversity as a factor in guidance. Finally, this study focused on care staff and did not include residents’ perspectives. Studying residents independently is essential, as including caregivers’ views simultaneously could overshadow or bias the interpretation of residents’ own experiences. Future research incorporating residents’ perspectives and structured observations could provide a more complete understanding of guidance in KS care and inform improvements in practice.
Conclusion
This study shows that behavior-centered, care-task-centered, and person-centered guidance patterns each play a role in caring for people with KS. The practical framework of these guiding strategies can help caregivers reflect on their approaches, discuss and reflect on them with the team, and align practices to provide tailored care. Future research should include residents’ and informal caregivers’ care experiences to provide a more complete picture of what constitutes good care.
Supplemental Material
Supplemental Material - Guiding People With Korsakoff’s Syndrome and Other Alcohol Related Cognitive Disorders in Long Term Care – An Ethnographic Study
Supplemental Material for Guiding People With Korsakoff’s Syndrome and Other Alcohol Related Cognitive Disorders in Long Term Care – An Ethnographic Study by Esther de Groot, Marja F. Depla, Ineke J. Gerridzen, Yvonne Zwaagstra, Cees M. P. M. Hertogh, Martin Smalbrugge and Marike E. de Boer in Dementia.
Footnotes
Acknowledgements
The authors would like to thank the professional caregivers from the specialized Korsakoff nursing homes who participated in this study, as well as the residents and management of the involved healthcare organizations for their support.
Ethical Considerations
The medical ethics review committee of the Amsterdam University Medical Center approved the study protocol (file no. 2024.0424) and confirmed that the Medical Research Involving Human Subjects Act (WMO) did not apply.
Consent to Participate
Participation was voluntary. Written and verbal informed consent was obtained from all participants after they were informed about the study.
Consent for Publication
All participants gave written consent for publication of the data in a scientific journal.
Authors Contributions
Conceptualization: I.G., M.D., C. H., E.G, M.B., M.S.
Methodology: E.G., M.D., M.B.
Data collection: E.G.
Formal analysis: E.G., M.D., I.G., M.B.
Writing-original draft: E.G.
Reviewing and editing original draft: E.G., M.D., I.G., M.B., M. S., Y. Z.
Project administration: Y. Z., I. G.
All authors have read and agreed to the published version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this research was funded by The Dutch Korsakoff Knowledge Centre (KKC).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The observation reports used and analyzed during the study are available from the corresponding author upon reasonable request.
AI Statement
Generative AI (ChatGPT, GPT-5) was used to assist in editing and improving the clarity, conciseness, and flow of the manuscript text. All content, ideas, and scientific interpretations were authored and verified by the research team. No data analysis or interpretation was performed by AI.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
Note on the Dutch elderly care physician (‘specialist ouderengeneeskunde’):
In the Netherlands, elderly care medicine is a recognized medical specialty dedicated to the care of older adults with complex, chronic conditions, predominantly within nursing home settings. Elderly care physicians provide comprehensive medical management for individuals with neurocognitive disorders—such as dementia, Huntington’s disease, and Korsakoff’s syndrome—alongside multiple comorbidities and neuropsychiatric syndromes. Their role integrates medical expertise with coordination of multidisciplinary teams, emphasizing person-centered care tailored to each individual’s needs.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.