
Abstract
Despite increasing dementia prevalence among minority ethnic populations in the UK, culturally appropriate post-diagnostic support remains limited. South Asian ethnic groups face distinct barriers in accessing care, including a lack of tailored arts, heritage, and cultural interventions that could support engagement, wellbeing, and social connection. This study explored how people living with dementia from South Asian ethnic groups and their carers in an ethnically diverse part of London, experience dementia services and perceive the potential value of creative health and culturally rooted approaches. Ten qualitative interviews were conducted with 22 participants (10 people living with dementia and 12 carers) of South Asian heritage, in 2024. Participants were recruited via community dementia services and included inpatients and outpatients aged 65–85, and carers aged 35–80. Interviews (40–90 min) explored experiences of dementia care, service access, and the role of arts, heritage, and cultural interventions. Reflexive thematic analysis was used to generate themes. Five key themes were identified: (1) Cultural Disconnect in Dementia Services; (2) Underuse of Cultural and Creative Resources; (3) Relational Continuity and Trust in Home-Based Dementia Services; (4) Gaps in Information and Dementia Healthcare System Navigation; and (5) Intersectional Barriers to Dementia Care Access. Participants described trusted relationships with home-based dementia teams, but strain in navigating wider care systems. Carers—particularly women—reported emotional exhaustion and limited capacity to engage with arts-based or cultural activities. Participants preferred culturally familiar, faith-sensitive, and home-delivered creative interventions. Dementia care for ethnically diverse groups must address the intersecting pressures of structural inequality, cultural identity, and caregiving. Co-produced, home-based arts and heritage interventions — embedded within trusted dementia care relationships — show promise in improving culturally relevant support. Embedding intersectionality and creativity in post-diagnostic dementia services can improve access, equity, and quality of life for both those with dementia and their carers.
Keywords
Background
Dementia represents one of the leading causes of disability and dependency among older adults globally. In the UK, approximately 885,000 people live with dementia, and this number is expected to rise significantly over the coming years (Alzheimer’s Society, 2022). London is the most ethnically diverse region in England, with just under two-thirds of its population identifying as ethnically minoritised groups (ONS, 2022a). Among these, South Asian groups represent one of the largest and fastest-growing ethnic groups, reflecting broader national trends (ONS, 2022b).
Despite this, dementia care for Asian ethnic minoritised groups remains under-resourced and poorly understood. The Alzheimer’s Society (2022) estimates that 25,000 people with dementia in the UK are from minority ethnic backgrounds, with this number projected to double by 2026. South Asian ethnic minoritised groups are particularly affected by higher rates of dementia-related risk factors such as Type 2 diabetes and cardiovascular disease (Mukadam et al., 2023). However, they often face significant barriers to diagnosis, treatment, and support, including language barriers, stigma, and inadequate service adaptation to cultural and religious needs (Herat-Gunaratne et al., 2020; Nielsen et al., 2021).
As of February 2025, the NHS Northwest London Integrated Care Board (ICB) estimated that 19,858 individuals aged 65 and over were living with dementia. Of these, 12,883 had received a formal diagnosis and were included in the dementia register, resulting in an Estimated Dementia Diagnosis Rate (EDDR) of 64.9% (Office for Health Improvement and Disparities (OHID) 2024). Hounslow, one of London’s most ethnically and culturally diverse boroughs, has among the highest rates of emergency hospital admissions for people living with dementia in the city (Hounslow Health and Care Partnership, 2023). Despite this, culturally tailored approaches to support and care remain limited. Within Hounslow, approximately 2,157 people are estimated to live with dementia, with around 31% identifying as being from South Asian backgrounds. A significant proportion remains undiagnosed or lacks access to timely, culturally appropriate support (Hounslow Health and Care Partnership, 2023; NIHR, 2020).
The Role of Creative and Cultural Interventions
Dementia care that includes culturally responsive, community-embedded interventions—such as arts, heritage and cultural activities—has shown promise in enhancing mood, attention, memory, and communication, allowing capacities for thought and creativity (Fancourt & Finn, 2019; Letrondo et al., 2023; Wyatt & Boddington, 2025). However, most studies have been conducted within White British or Western populations, with minimal exploration of how such interventions are received by South Asian ethnic minoritised groups. There is also a lack of access to creative health activities for people from culturally and ethnically diverse backgrounds and minoritised groups (The Baring Foundation, 2021). According to the National Centre for Creative Health, despite the expansion of the creative health sector, there remains significant challenges in relation to equity, diversity and inclusion (EDI), both in participation and workforce representation (Kanber, 2024).
Studies suggest that cultural identity, language, and religious practices play an important role in how dementia is experienced and managed within families (Jutlla, 2015). In many cultures, there is a strong tradition of informal caregiving, often undertake by women, which can obscure formal care needs and mask unmet support requirements (Greenwood et al., 2015), with evidence that female caregivers experience greater psychological burden (Pillemer et al., 2018). Lack of cultural appropriateness, stigma, fear of institutionalisation, and poor service alignment further discourage families from accessing support (Armstrong et al., 2022; Giebel et al., 2015).
Despite the evidence base supporting arts in dementia care, the cultural and contextual relevance of interventions remains a significant gap. There is little published research on arts and creative health- based models that are co-produced with, or designed specifically for, South Asian carers and patients with dementia in the UK. The absence of such work is especially concerning in ethnically diverse areas, where South Asian groups and communities form a substantial proportion of the population with dementia.
This study investigates how South Asian patients with dementia and their carers experience the care system in an ethnically diverse area in London, and whether there is an unmet need for culturally aligned arts, heritage, and culture-based and creative health interventions. The overall aim of this study was to explore the experiences of health inequalities for South Asian patients with dementia and their carers, with a focus on cultural inclusion in care and the relevance of arts, heritage, and cultural engagement. Specific objectives were to: • Explore experiences of accessing dementia-related healthcare services and information. • Examine current or past use of arts/heritage and cultural interventions in post-diagnosis support. • Identify barriers to culturally responsive care. • Investigate how intersecting social identities (e.g. gender, ethnicity, language) influence service access and use.
Methods
Study Design
A qualitative study using semi-structured interviews was conducted to capture in-depth experiences of South Asian people with dementia and their carers in one culturally and ethnically diverse area. Ethical approval was obtained from West Midlands - Black Country Research Ethics Committee (8/12/2023) Ref: 23/WM/0143.
Sampling and Recruitment
Purposive sampling was used to recruit participants through the Hounslow and Richmond Community Healthcare NHS Foundation Trust, with referrals facilitated by EDCS (Enhanced Dementia Care Service) specialist nurses. Eligible participants self-identified as South Asian patients aged 65–85 with a clinical diagnosis of dementia or were unpaid carers. The EDCS specialist nurse acted gatekeepers into the research study by suggesting participants who were eligible to take part.
Participants were contacted via email, phone, and in person by the specialist nurses, and provided with participant information sheets, and consent forms for carers. Participants were invited to express their interest to take part, and informed consent was taken by the EDCS specialist nurse in line with the Mental Capacity Act 2005. Where patients lacked capacity, their carers were invited to participate alone to reflect on caregiving experiences.
Participant descriptors are presented using gender, and self-identified ethnicity or national background, and faith where disclosed. Where participants did not provide specific details, only the available identifiers are reported.
Data Collection
Demographic Characteristics of Participants
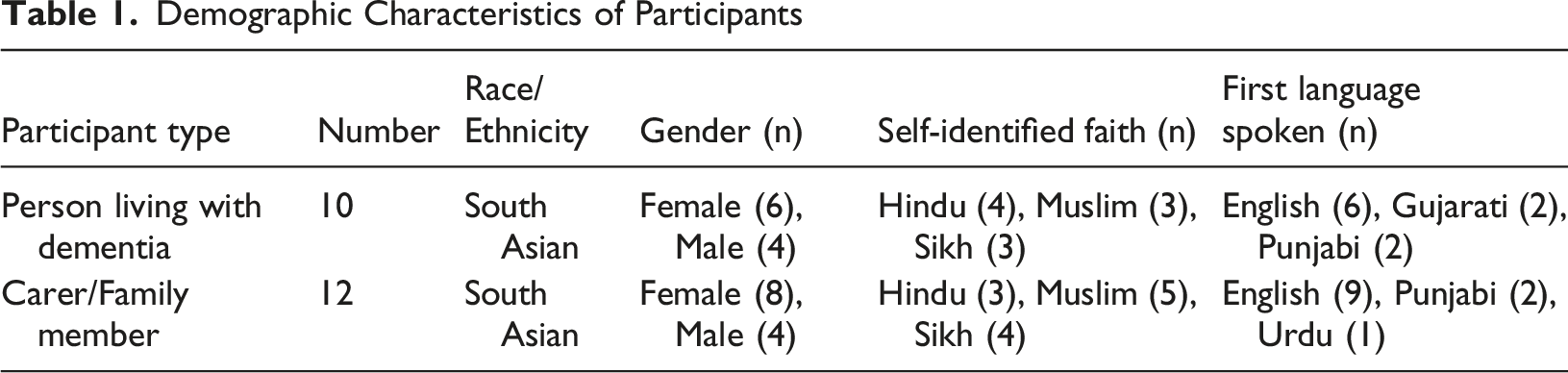
Interviews lasted 40–90 min and were conducted using Microsoft Teams or in person, based on participant preference. All interviews were conducted in English. While some participants spoke additional languages (see Table 1), interviews were carried out in English based on participant preference and ability to communicate. Language support was available if needed but was not required for this study. A £50 voucher was provided in appreciation of participant time. Topic guides explored diagnosis experiences, barriers to care, cultural adaptation, use of arts or heritage activities, and caregiving impacts. The interviews were audio recorded on an HRCH Trust encrypted laptop using MS teams. Transcription was completed using this recording by the researchers. Audio recordings and transcribed data were saved on the trust network drive securely and access was limited to authorised staff. Audio-recordings were deleted after transcription.
Subject Position Statement
The authors are five researchers with distinct social, cultural, and disciplinary identities: three self-identify as African, one as a African-Caribbean and one is White British. Our professional backgrounds span nursing, psychology, public health, and the arts. These intersecting identities, alongside our epistemological, ontological, and axiological commitments, shaped the research process, from framing the research questions to interpretating participants’ narratives. The work is grounded in a relativist ontology. We understand experiences of dementia not as singular, fixed phenomena, but as socially, culturally, and relationally constructed. It is recognised that dementia is lived and understood differently across communities, shaped by migration histories, intergenerational dynamics, spirituality, language, and experiences of racism and structural inequality in the UK. We approached participants’ accounts as valid, situated realities rather than objective representations of a universal condition. Epistemologically, the work is aligned with a social constructionist and interpretivist perspective. We view knowledge as co-produced between researchers and participants, emerging through dialogue, trust-building, and reflexive engagement. As researchers who do not share the same cultural background as the participants, we were attentive to the ways insider–outsider dynamics influenced rapport, disclosure, and interpretation. The African identities of some of the team, provided lived experience of racialisation and minoritisation within the UK context, and experience of delivering creative health programmes, which fostered sensitivity to structural inequities and cultural nuance. Our disciplinary training further shaped our epistemological lenses. The psychologist on the team brought expertise in cognitive and emotional processes and was attentive to meaning-making, coping, and identity in the context of dementia. The public health researcher foregrounded structural determinants of health, including access to services, socioeconomic conditions, and policy contexts. The artist contributed a sensitivity to narrative, embodiment, and non-verbal forms of expression, encouraging attention to affect, silence, metaphor, and aesthetics within participants’ accounts. The nurses foregrounded patient lived experiences, narratives, and meanings.
Together, these perspectives supported interpretation that moved beyond deficit-based dementia models. The team are committed to social justice, equity in health and social care, and the amplification of voices that are often marginalised within dementia research and service design. We recognise that South Asian elders in London may experience intersecting forms of marginalisation related to age, ethnicity, language, migration status, and disability. Our intention was not only to document experiences but to challenge dominant narratives that may render minoritised communities invisible.
Data Analysis and Procedures
To analyse the data, we followed Braun and Clarke’s (2022) approach to reflexive thematic analysis, which involves a dynamic and recursive process of familiarisation, coding, theme development, and interpretation. The analysis was interpretive and iterative, allowing meaning to emerge from the data through continuous engagement with participants’ narratives.
The lead researcher conducted open coding of all transcripts, adding descriptive notes and analytic reflections. After reviewing the first 3–4 interviews, an initial set of codes was shared with the wider research team. Through iterative discussion, an analytic framework was developed and refined. This framework was used to guide the review of subsequent transcripts, with codes and sub-themes revised as new insights emerged. Transcripts were revisited multiple times to allow for theme consolidation and deeper interpretive layering.
Final themes and sub-themes were applied to all transcripts using NVivo software. The thematic framework was also structured and presented in a Thematic Analysis Table (see Supplemental File 1 for a sample of the quotes) which includes each theme, its sub-themes, and illustrative quotes.
For instance, the theme “Cultural Disconnect in Dementia Services” included sub-themes such as “Lack of culturally appropriate support,” “Absence of faith-specific guidance,” and “Language barriers.” One participant illustrated this point, stating: “We haven’t received any culturally specific resources or support, such as guidance tailored to our Hindu faith or Sri Lankan heritage.” (Carer – Female, Sri Lankan, Hindu).
To enhance trustworthiness, we adhered to the four principles of qualitative rigour: credibility, dependability, confirmability, and transferability (Lincoln & Guba, 1985). These were ensured through strategies such as maintaining an audit trail of analytic decisions, peer debriefing across the research team, and reflexive discussions throughout. Additionally, an independent qualitative researcher reviewed the coding and thematic structure to enhance transparency and intercoder reliability. Themes are reported as a descriptive narrative in the results section, supported by direct participant quotations to illustrate depth and diversity of experiences.
Findings
The following five key themes were identified: (1) Cultural Disconnect in Dementia Services, (2) Limited Use of Cultural and Creative Resources Amidst the Burden of Caregiving, (3) Relational Continuity and Trust in Home-Based Dementia Services, (4) Gaps in Information and Dementia Healthcare System Navigation and (5) Intersectional Barriers in Dementia Care Access.
Cultural Disconnect in Dementia Services
Participants described a persistent mismatch between dementia services and the cultural and religious needs of South Asian families. This included a lack of culturally appropriate support, limited availability of faith-specific guidance, language barriers, and reluctance to access unfamiliar services that lacked cultural resonance. “We haven’t received any culturally-specific resources or support, such as guidance tailored to our Hindu faith or Sri Lankan heritage. Nothing about fasting, prayers, or how it might impact her condition.” (Carer – Female, Hindu) “We’ve tried so many times to arrange day centres. They do one for Punjabis, okay, even with a pickup and a drop-off service. Oh yeah, that’s great. But every time she just shuts it down — wants to stay home.” (Carer – Female, Sikh)
People living with dementia also described difficulties making sense of unfamiliar environments and experiences, which could be heightened in contexts that were not linguistically or culturally familiar. This uncertainty influenced their willingness to engage with settings that felt unfamiliar or lacked cultural and relational familiarity. This was echoed elsewhere in the data, where participants expressed a preference for familiar, language-concordant social environments. “I see people… and hear things… sometimes I don’t understand what’s happening.” (Person living with dementia – Female, Sikh)
Participants also expressed concern about language barriers, noting that linguistically matched staff—such as Gujarati-speaking practitioners—were essential for effective engagement. “Yes, if it’s definitely something home-based will be helpful. The problem is with dementia, so much of it, she will understand, yeah, and how much we will then have to keep comforting her to make her understand. If she’s with like-minded people in terms of language, then I’m sure she can talk to them and that will be easy for her to communicate.” (Carer – Male, Muslim) “Lack of Gujarati-speaking healthcare professionals, particularly physiotherapists, severely limits rehabilitation support. I end up interpreting for her, and it’s exhausting.” (Carer – Male, Sikh)
Limited Use of Cultural and Creative Resources Amidst the Burden of Caregiving
Carers consistently described how opportunities to engage with cultural, creative, or arts-based interventions were either absent or inaccessible within dementia care pathways. This underutilisation was not due to lack of interest; rather, it was compounded by the overwhelming demands of unpaid caregiving, physical limitations of the person living with dementia, and a general lack of service visibility. Many carers had not heard of creative or cultural offers tailored for people with dementia. When asked directly, some expressed interest, but stressed that any intervention would need to be delivered at home and sensitively tailored to language, faith, and the cognitive stage of their relative. “We’ve not heard of anything useful. If there is something like that which would work specifically for her, then yes — that would be useful.” (Carer – Female, Sikh) “She used to love doing things like knitting, making pickles… She was very hands-on. So maybe art and craft would help her — like sticking things. The only thing I’d worry about is anything with needles or scissors… with dementia, you just don’t know.” (Carer – Female, Sikh)
People living with dementia also described a loss of previously meaningful cultural and social activities, particularly those connected to faith and community engagement. For some, declining health limited their ability to participate in practices that had previously structured daily life and social interaction. “I used to go and pray with others… now I can’t go anymore.” (Person living with dementia – Female, Muslim)
Although most participants were unaware of services such as arts by post, they showed interest in the concept, particularly as an accessible, low-pressure intervention that could be trialled at home. “No, we’ve never been offered anything like that. First time I’ve heard of arts at home [arts by post]. If something like that could be sent — art by post or craft stuff she could try — we might give it a go. But we just haven’t seen anything like that.” (Carer – Female, Muslim)
Verbal storytelling, music, and talking therapy were commonly mentioned as more culturally congruent forms of creative engagement — but again, participants stressed the need for home delivery and trusted practitioners. “When the memory nurse came, I told her — she loves talking. If she could get talking therapy, even once or twice a week, just someone to listen to her, I think that would help her a lot. She has a lot to say.” (Carer – Female, Muslim)
However, even when appropriate interventions existed, physical limitations, carer availability, and emotional strain made it difficult to engage. For some, mobility or cognitive decline made community-based services impractical without tailored transport and accompaniment. “She’s not confident by herself. She needs somebody with her. That's why I think she’s refused going to any centres. Even with pickup and drop-off, she still said no. She needs someone she knows to go with her, and we’re all working.” (Carer – Female, Muslim) “We haven’t accessed arts, heritage, or cultural activities to support my mum’s health and wellbeing, because of her declining mobility. She can’t go out now, and I don’t have the time. Who will care for her if I go… and be here for her to support her?” (Carer –Male, Sikh)
The caregiving burden — emotional, physical, and mental — was a persistent barrier. Participants described how they lacked time for self-care, let alone additional activity planning or service navigation. This strain made accessing cultural interventions not just unlikely, but often impossible without meaningful structural support. “Sometimes I cry because I don’t know what to do for him.” (Carer –Female, Pakistani, Muslim) “I can’t be bothered even now. Today I had an appointment for speaking therapy, about my stress, but I said look, I can’t be bothered today. I’m too stressed, and I had another call. Everything is piling up… I don’t know whether to be happy or sad anymore. I’m just tired.” (Carer –Female, Muslim) “You come into the kitchen, the sink’s full of dishes. Then I have to think what to cook. I feel guilty if I don’t make one proper meal. I’ve always liked to finish my work before I sit, but now the minute I sit, someone’s calling me, the doorbell rings, or I hear her calling. Even going out for a walk has become stressful.” (Carer – Female, Hindu)
Despite these pressures, carers acknowledged the value of cultural engagement — for themselves and their relatives — when they were able to access it. Periods of rest or cultural reconnection were described as essential to maintaining their ability to provide care. “I booked a trip with my daughter to Amsterdam. Just two days — and you won’t believe, I just slept. I didn’t wake up till 2pm. That’s how much my body needed rest. That’s the only time I could truly rest.” (Carer – Female, Muslim)
Relational Continuity and Trust in Home-Based Dementia Services
Despite frustrations with other parts of the care pathway, participants consistently praised the work of home-based dementia teams. They valued the familiarity, cultural sensitivity, and relational consistency of professionals who visited them at home. “The Dementia Care Team were amazing. They actually came to the house and spent time with her and with us. If it wasn’t for them, we wouldn’t have known mum had a UTI — we just thought she was more confused than usual. They caught it early.” (Carer – Female, Sikh) “The nurse from the memory clinic came to the house — she was the only one who explained everything clearly. She didn’t rush. She even spoke to mum in her own language a bit and gave us space to ask questions. That made such a difference. “(Carer –Female, Muslim) “When the doctor came for the assessment… there was an interpreter there. That’s brilliant. And on a couple of other occasions too — social services brought someone to help with the language.” (Carer –Male, Sikh) “They [dementia care team] were very good. Explained everything in a way that made sense to us. Not just the medical stuff, but in a way that showed they got how we live.” (Carer –Female, Sikh)
This stood in stark contrast to experiences with the wider NHS system, where fragmented services and rushed appointments left families feeling unsupported. “Everything else is a nightmare — GP, memory clinic, referrals. But they — the home dementia people — they actually listen. They’re the only part of the service that feels human.” (Carer –Male, Sri Lankan, Hindu)
Importantly, this trust enabled families to consider new types of engagement, including arts-based activities — but only if offered by a trusted professional. “She doesn’t go anywhere. She says no to the day centre and even to family gatherings. But if the nurse brought something like art — or if it was someone she knows — I think she might try it. She trusts her more.” (Carer –Female, Muslim)
Gaps in Information and Dementia Healthcare System Navigation
Participants reported significant confusion about how to navigate dementia services, particularly after diagnosis. Many described feeling left to “join the dots” across multiple fragmented services and unclear responsibilities. “I’m curious what stage she’s at, and what to expect in the future.” (Carer –Male, Muslim) “The process of diagnosis was very slow… we had to push our GP.” (Carer –Female, Sikh) “We have to call the GP, then the … team – it’s us chasing.” (Carer –Male, Sri Lankan, Hindu)
This lack of structured guidance created anxiety, and often placed the burden of system coordination on carers already stretched by daily responsibilities.
Intersectional Barriers in Dementia Care Access
Carers highlighted how overlapping experiences of ethnicity, gender norms, migration history, and socioeconomic position shaped their access to care. Cultural expectations around family responsibility often led carers to reject or avoid formal services — especially after negative past experiences. “She’s lived differently all her life… she’s not adapting to this lifestyle.”(Carer-Female, Muslim) “We had such a bad experience with a respite home during my son’s wedding. Mum’s clothes were soiled, hair undone, bruises. She was calling out at night like she was having nightmares. The police got involved. We will never send her back there. From our Indian background, we want to care for her at home till her last day.” (Carer –Female, Sikh)
Others described invisible sacrifices, often without recognition from services or financial compensation. “I do everything – the cleaning, washing, cooking, changing bed, meds. A care worker comes for the basic things, but everything else is on me. I even changed jobs so I could be at home more. Now I work flexible hours, send emails at 3am if needed. It’s changed the whole trajectory of my life.” (Carer –Male, Muslim)
The need for culturally safe, language-matched, and emotionally supportive interventions was repeatedly emphasised and seen as critical for both people living with dementia and their carers. Carers highlighted the importance of home-based, relational forms of support that could facilitate communication, emotional expression, and engagement within familiar environments. “If talking therapy is possible at home, she might open up more.” (Carer – Female, Muslim)
People living with dementia similarly described experiences of social isolation and expressed a desire for opportunities to engage with others in culturally and linguistically familiar contexts. The importance of shared language and cultural understanding was central to their willingness to participate in activities or social settings. “I want to go out… my son is here… but I’m all alone… I’d like to go out.” (Person living with dementia – Female, Sikh) “We can try. But the problem is the communication… unless I’m with people who speak the same language… like Punjabi… and understand the culture.” (Person living with dementia – Female, Muslim)
Discussion
This study explored the experiences of South Asian minoritised people living with dementia and their carers, with a specific focus on arts, cultural and creative care interventions. The findings reveal persistent structural inequalities, shaped by a combination of cultural disconnect, caregiving burden, limited culturally appropriate support, and intersectional barriers. While existing dementia care pathways in the borough include community-based and relational services that are highly valued, participants experienced these as exceptions in an otherwise fragmented and culturally misaligned system.
Cultural Dissonance and Service Avoidance
A key finding relates to the pervasive cultural disconnect between mainstream dementia services and the needs of South Asian families. Participants described a lack of faith-specific guidance, limited availability of language-matched staff, and services that did not align with their everyday cultural values and religious beliefs. These findings reinforce earlier work showing that cultural identity significantly influences dementia recognition, help-seeking behaviours, and acceptance of external support (Herat-Gunaratne et al., 2020; Jutlla, 2015).
Despite the presence of targeted services such as ethnic-specific day centres, uptake was low. Participants often perceived these offers as inadequate or unfamiliar, confirming previous research indicating that superficial ethnic matching does not guarantee meaningful engagement (Armstrong et al., 2022). This finding highlights the need for co-designed, culturally safe services that embed religious, linguistic, and intergenerational understandings of dementia.
Underutilisation of Cultural and Creative Health Interventions
Although research has demonstrated the positive impact of creative and arts-based interventions for people living with dementia (Fancourt & Finn, 2019; Letrondo et al., 2023), this study found little evidence of uptake or access within the South Asian population interviewed. Participants expressed interest in such interventions, especially those delivered at home, but most were unaware of their existence. Where awareness did exist, logistical, linguistic, and cultural relevance issues made participation unlikely.
These findings reflect wider gaps in arts-in-health programming, where cultural tailoring remains underdeveloped. Notably, Tischler et al., 2022; Wyatt & Boddington, 2025 demonstrate that home-based cultural interventions can successfully support wellbeing and cognitive agency among people with dementia. Few studies have meaningfully involved ethnically diverse groups in the development or delivery of creative dementia interventions. Where they have, such as in Gilmore-Bykovskyi et al.’s (2020) work developing culturally relevant storytelling materials to engage African American communities in Alzheimer’s care, or Cheston et al.’s (2024) study on barriers to partnership working with South Asian communities in the UK, researchers have emphasised the importance of cultural fluency, co-production, and trust in increasing meaningful participation. These studies highlight how culturally grounded narratives, and collaborative design can help bridge access gaps in dementia support. Our findings similarly suggest that future creative offers must be co-produced with families and embedded within trusted care pathways to support both engagement and sustainability.
The Value of Relational, Community-Based Dementia Services
Participants consistently praised home-based dementia services for their cultural sensitivity, relational continuity, and emotional presence. These teams, often led by specialist memory nurses or community workers, were trusted and perceived as responsive. They played a critical role in enabling families to engage with the idea of creative, non-clinical interventions. This reflects earlier evidence on the value of continuity of care and relationship-centred practice in dementia services (Armstrong et al., 2022; Nielsen et al., 2021).
The relational aspect of these services enabled carers to reflect on needs beyond crisis management, including emotional support, communication, and quality of life. For example, carers were more open to discussing talking therapy or arts by post when introduced by someone known and culturally attuned. This finding underscores the importance of embedding social prescribing or cultural offers within pathways already perceived as culturally safe.
Caregiver Burden and Cultural Expectations
The theme on limited use of cultural resources amidst the burden of caregiving highlighted how structural pressures often eclipsed opportunities for enrichment, respite, or self-care. Women disproportionately carried the emotional and physical load of caregiving, a finding consistent with previous literature (NHS England, 2022). Participants described exhaustion, distress, and guilt — compounded by limited recognition of their role by formal services.
Our findings support work by Giebel (2024), which argues that addressing a single barrier — such as service awareness — is insufficient without also addressing the structural conditions that restrict access. Cultural expectations to ‘care for your own’, lack of paid respite, and household responsibilities were all major deterrents to engaging with support.
While services like Culture Box (Tischler et al., 2022) and Leicester’s Culture to You https://www.cultureleicestershire.co.uk/culture-to-you/ (Leicestershire County, 2025) demonstrate that home-based arts programmes are both viable and well-received, our findings suggest that future adaptations must more explicitly address caregiver time, capacity, and emotional readiness. For such interventions to be truly inclusive and sustainable, they must support not only the person living with dementia but also the wider family system that facilitates their care.
Intersectional Challenges in Access and Participation
The study also foregrounded intersectionality — particularly the interplay of gender, ethnicity, language, and migration status — as a major determinant of inequality in dementia care. These intersectional dynamics were evident in accounts of invisible care, service mistrust, and trauma linked to previous poor experiences. Such complexity cannot be addressed through generic services or “single-issue” interventions. Carers described how even when services were available, their uptake was undermined by shame, uncertainty, or fear of judgment. This finding aligns with Giebel’s Dementia Inequalities Model (2024), which emphasises that access barriers are mutually reinforcing. For example, a lack of linguistically appropriate services may intersect with caregiving fatigue and distrust of institutional care. Addressing only one barrier in isolation is therefore unlikely to improve engagement. Holistic, multi-level responses are required.
Strengths and Limitations
This study presents several strengths. It offers an in-depth qualitative account of the under-explored experiences of South Asian ethnic minoritised carers and people living with dementia in a London borough with one of the UK’s highest dementia-related hospital admission rates. The use of reflexive thematic analysis provided a flexible lens to explore intersecting cultural, social, and structural barriers. The study also foregrounds carer voices and captures highly contextualised lived experiences.
However, there are also limitations to note. Firstly, although our sample size aligns with qualitative principles, findings are not generalisable to all diverse Asian ethnic groups, communities or other boroughs. Participants were recruited through community dementia nurses, potentially excluding those not currently in contact with health services. Despite offering options for remote participation, digital exclusion or care responsibilities may have deterred others. Additionally, interviews were conducted primarily in English, which may have excluded individuals with lower English proficiency or influenced how some participants expressed their experiences. Finally, although one additional independent qualitative researcher reviewed coding to support rigour, data interpretation was still shaped by researcher positionalities — a recognised feature of reflexive methodology.
Conclusion
This study highlights a critical opportunity to strengthen dementia care pathways by embedding cultural relevance, relational continuity, and carer inclusion for ethnically diverse populations. Through reflexive thematic analysis, we identified how South Asian families face intersecting structural, linguistic, and emotional barriers to accessing culturally appropriate dementia support — including creative and heritage-based interventions.
Participants described a care system that is often fragmented and difficult to navigate, placing disproportionate responsibility on unpaid carers, most often women. Despite the known benefits of creative and arts-based interventions in dementia care, these offers remain largely inaccessible unless they are home-based, co-designed, and introduced through trusted, culturally responsive professionals.
Community-based relational care teams emerged as key enablers of trust, understanding, and openness to creative engagement. Programmes such as Culture Box and Culture to You offer valuable models of outreach and culturally inclusive arts and creative health provision. Building on their success, further work is needed to extend these interventions into home environments, particularly to support multi-generational families and unpaid carers in community settings.
Future efforts should prioritise the co-production of dementia support with South Asian and other minoritised families, integrating culturally tailored care with social prescribing, creative wellbeing, and accessible, language-sensitive information. Without this shift, existing inequalities are likely to persist or deepen. By centring the voices of carers and recognising intersectional barriers to engagement, this study contributes critical evidence toward the design of more inclusive and equitable dementia care systems in the UK and beyond. Further research is needed to explore how culturally tailored creative interventions can be adapted and scaled across diverse communities, particularly in settings where formal service contact is low or fragmented.
Supplemental Material
Supplemental Material - Hounslow Health Inequalities in Dementia Care (HHIinD): Experiences of South Asian Ethnic Minority People Living With Dementia and Their Carers, and the Role of Arts, Heritage and Cultural Interventions
Supplemental Material for Hounslow Health Inequalities in Dementia Care (HHIinD): Experiences of South Asian Ethnic Minority People Living With Dementia and Their Carers, and the Role of Arts, Heritage and Cultural Interventions by Natalie Darko, Naomi Keyamo, Luki Obro, Errol Francis, and Victoria Tischler in Dementia
Footnotes
Acknowledgements
This research was supported by NHS England. ND is supported by the National Institute for Health and Care Research (NIHR) Leicester Biomedical Research Centre. The views expressed are those of the author(s) and not necessarily those of NHS England, the NIHR Leicester BRC, the NIHR or the Department of Health and Social Care. The authors thank the Hounslow and Richmond Community Healthcare NHS Foundation Trust, and particularly Shivani Khan, the Enhanced, Dementia, Care Services (EDCS) team and dementia care nurses, Research Governance lead, and Medical Director (Hounslow and Richmond Community Healthcare) HRCH, for supporting the study. We also gratefully acknowledge the participants and their families for sharing their experiences. This paper is dedicated to the memory of Dr John Omany.
Ethical Considerations
Ethical approval was granted by the Health Research Authority (HRA) and Health and Care Research Wales (HCRW) Social Care Research Ethics Committee, reference: RAS 318610 (HHIinD) Hounslow Health Inequalities in Dementia Care. Prior to participation in interviews, written informed consent was obtained from all participants, or, where applicable, from carers supporting individuals with impaired capacity, in accordance with the Mental Capacity Act (2005).
Author Contributions
VT and EF conceived and designed the study, with input from ND. ND led the data collection, supported by LO, SK, and NK. Thematic analysis was conducted by ND, VT, and an independent qualitative researcher. ND, EF and VT drafted the manuscript; all authors contributed to data interpretation, manuscript revisions, and final approval.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by NHS England. The funders had no role in the design of the study, data collection, analysis, interpretation of data, writing of the manuscript, or decision to publish.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
A sample of de-identified participant quotes is provided in the thematic analysis table (see Supplementary File 1). To protect participants’ privacy and anonymity, the complete set of interview transcripts is not publicly available.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.