
Abstract
Keywords
Background
Dementia is a growing global public health challenge, with prevalence rising rapidly as populations age and life expectancy increases worldwide. In the absence of effective disease-modifying therapies, prevention strategies have increasingly focused on identifying modifiable risk factors that may reduce dementia burden at the population level (Norton et al., 2014). Among these, hearing loss has emerged as one of the most prominent and potentially preventable contributors to cognitive decline and dementia (Lin et al., 2011).
At the individual level, extensive evidence from longitudinal cohort studies and meta-analyses demonstrates that hearing loss is associated with increased risk of incident dementia, accelerated cognitive decline, and adverse structural and functional brain changes (Deal et al., 2015; Lin et al., 2011; Loughrey et al., 2018). Proposed mechanisms include increased cognitive load resulting from degraded auditory input, sensory deprivation, social isolation, and shared neuropathological or vascular pathways (Peelle, 2018; Pichora‐Fuller et al., 1995; Tun et al., 2009). On the basis of this evidence, hearing loss has been identified in major dementia prevention frameworks as a leading modifiable risk factor across the life course (WHO, 2019; WHO, 2021).
Despite this growing body of individual-level evidence, most existing studies have been conducted in cohorts of adults, often in high-income settings (Readman et al., 2025; Yu et al., 2024). Considerably less is known about whether the hearing loss-dementia association is expressed at the population level across diverse socioeconomic, demographic, and epidemiological contexts. Country-level ecological analyses cannot infer individual risk, but they provide a complementary perspective by examining whether national hearing loss prevalence aligns with national dementia prevalence after accounting for broader contextual factors (Greenland, 2001; Morgenstern, 1995; Readman et al., 2025).
Sex is relevant to this question because dementia prevalence, longevity, health behaviours, occupational exposures, and access to healthcare differ between females and males (Huque et al., 2023; LaPlume et al., 2022). However, sex-stratified ecological analyses should not be interpreted as evidence of sex differences unless formal effect-modification testing is undertaken (Altman & Bland, 2003; Greenland & Morgenstern, 1989; Knol & VanderWeele, 2012). In this study, sex stratification was used primarily to describe whether country-level patterns are broadly similar or divergent between females and males, with formal comparison added to avoid overinterpreting parallel models.
Interpretation of population-level associations is additionally challenged by the close interrelationship between hearing loss prevalence and broader macro-level conditions (Haile et al., 2021; Scholes et al., 2018). Economic development, urbanisation, increased longevity, and reduced biological selection pressures may be associated with both hearing loss and dementia prevalence (Mollalo et al., 2025; You et al., 2022; You et al., 2025). Consequently, observed correlations may reflect shared structural determinants rather than a distinct association between hearing loss and dementia (Greenland, 2001). Analytical approaches that account for these interdependencies are therefore essential for assessing the independent explanatory contribution of hearing loss within a broader socioeconomic and demographic framework (Morgenstern, 1995; Vatcheva et al., 2016).
Against this background, the present study uses global country-level data to examine sex-stratified associations between hearing loss prevalence and dementia prevalence. The specific aims were to: (1) characterise the country-level association between hearing loss prevalence and dementia prevalence in females and males; (2) assess whether this association persists after adjustment for socioeconomic development, urbanisation, the Henneberg Index, and longevity; and (3) formally assess whether the adjusted hearing-loss coefficient differs between female and male models. The main contribution is the extension of established individual-level evidence to a global ecological framework, rather than the claim of a new individual-level risk pathway or strong sex-specific divergence.
Methods
Data Sources
Sex-specific national prevalence estimates for dementia and hearing loss were obtained from the Global Burden of Disease (GBD) Study produced by the Institute for Health Metrics and Evaluation, University of Washington, USA (IHME, 2024). Dementia prevalence estimates for 2023, including Alzheimer’s disease and other dementias, were generated separately for females and males using standard GBD modelling frameworks that integrate data from cohort studies, health surveys, hospital and outpatient records, administrative claims, and mortality registries, with case definitions based on International Classification of Diseases (ICD) criteria (IHME, 2024; Nichols et al., 2022).
Hearing loss prevalence estimates for 2023 were also derived from the GBD database using established statistical modelling approaches based on population registries, epidemiological surveys, vital registration systems, and hospital records (IHME, 2023). Dementia and hearing loss were expressed as age-inclusive prevalence rates per 100,000 population and were log10-transformed prior to analysis to improve linearity and cross-national comparability.
Macro-structural indicators were sourced from internationally recognised databases. Economic development was measured using GDP per capita (PPP; constant 2020 US dollars) and urbanisation as the proportion of the population living in urban areas, both from the World Bank World Development Indicators (World Bank, 2022); Population ageing was indexed using sex-specific life expectancy at age 60 (e60; 2020) from the World Health Organization (WHO) Global Health Observatory (WHO, 2020). Population-level exposure to relaxed natural selection was assessed using the Henneberg Index (Biological State Index, Ibs) derived from published mortality and fertility estimates (You & Henneberg, 2017, 2026).
Countries were classified using multiple international frameworks to support stratified analyses, including World Bank income groups, United Nations development status, and the six WHO regions. Additional geopolitical groupings (e.g., APEC, OECD, European Union, Arab World, Latin America and the Caribbean, Southern African Development Community, Shanghai Cooperation Organisation, and English-speaking countries) were included to capture broader contextual variation. Depending on data availability, analyses included up to 204 countries.
Study Design and Variable Specification
A sex-stratified ecological, cross-national design was used. Dementia prevalence was specified as the outcome variable, and hearing loss prevalence was specified as the primary explanatory variable. Analyses were conducted separately for females and males to describe within-sex country-level patterns.
Because parallel sex-specific models do not, by themselves, provide a formal test of sex differences, the adjusted hearing loss coefficients were compared using a coefficient-difference test based on the unstandardised coefficients and standard errors from comparable fully adjusted female and male models. A pooled sex-by-hearing interaction model was not used because the dataset comprised sex-specific country-level prevalence estimates with separate female and male dementia outcomes. The coefficient-difference test was therefore used to directly assess whether the adjusted hearing loss–dementia association differed between the sex-specific models.
This specification was guided by life-course considerations, as hearing loss is commonly identified earlier in adulthood, whereas dementia predominantly occurs in later life. Sex stratification was used to determine whether the population-level association was evident in both females and males, rather than to assume a priori that the association differed by sex.
Except for the Henneberg Index, which was obtained from a single published source, the study variables showed strong and stable country-level correlations across 2009–2023, indicating enduring national patterns. This temporal stability suggests that the use of a single reference year was unlikely to materially affect the observed ecological associations.
Data Preparation
Data from multiple international sources were harmonised into a country-level dataset. Prevalence measures and macro-structural indicators (economic development, urbanisation, Henneberg Index, and ageing) were aligned by country and standardised.
Countries with missing data for variables required in a given analysis were excluded using listwise deletion. Analytic sample sizes are therefore reported for each major analysis. All prevalence and macro-structural variables were log10-transformed in the primary correlation, PCA, partial correlation, and regression analyses to reduce skewness, stabilise variance, and improve linearity.
Multicollinearity was assessed separately in female and male regression models using tolerance and variance inflation factor (VIF) statistics. All models met conventional thresholds (tolerance ≥ 0.10; VIF ≤ 10), indicating no problematic multicollinearity.
Statistical Analysis
Exploratory scatterplots of untransformed rates were examined to assess distributions and visual patterns. Polynomial trend lines in Figure 1 were retained as descriptive visual summaries only and were not used for statistical inference. Primary analyses were based on log10-transformed variables and linear modelling. Associations between hearing loss prevalence and dementia prevalence were evaluated using Pearson and Spearman correlations, both globally and within predefined country groupings. Differences in correlation strength across income levels and development status were tested using Fisher’s r-to-z transformation.
Principal component analysis (PCA) was conducted separately for females and males to assess whether hearing loss prevalence clustered with indicators of population ageing and socioeconomic context, including economic development, urbanisation, the Henneberg Index, and ageing (e60). Sampling adequacy was assessed using the Kaiser–Meyer–Olkin (KMO) statistic and Bartlett’s test of sphericity, and components with eigenvalues greater than one were retained.
Multivariable linear regression models were fitted separately for females and males using the enter method. These theory-informed models were treated as the primary adjusted analyses. Standardised regression coefficients (beta), unstandardised coefficients (B), standard errors, adjusted R2 values, and F-statistics were reported. A coefficient-difference test was then used to formally evaluate whether the adjusted hearing-loss coefficient differed between the female and male models. Partial correlations were retained as sequential robustness checks and reported in the supplementary material to show how the hearing loss-dementia association changed after progressive covariate adjustment. Stepwise regression analyses were moved to the supplementary material and treated as exploratory sensitivity analyses only.
Except for exploratory scatterplots generated using Microsoft Excel 2016, all variables were log10-transformed prior to analysis. Statistical analyses were conducted using IBM SPSS Statistics, version 31 (IBM Corp., 2023). Findings are interpreted at the population level and do not imply causality or individual-level risk.
Results
Sample Description and Analytic Samples
Analytic Sample Sizes and Data Availability Across Major Analyses
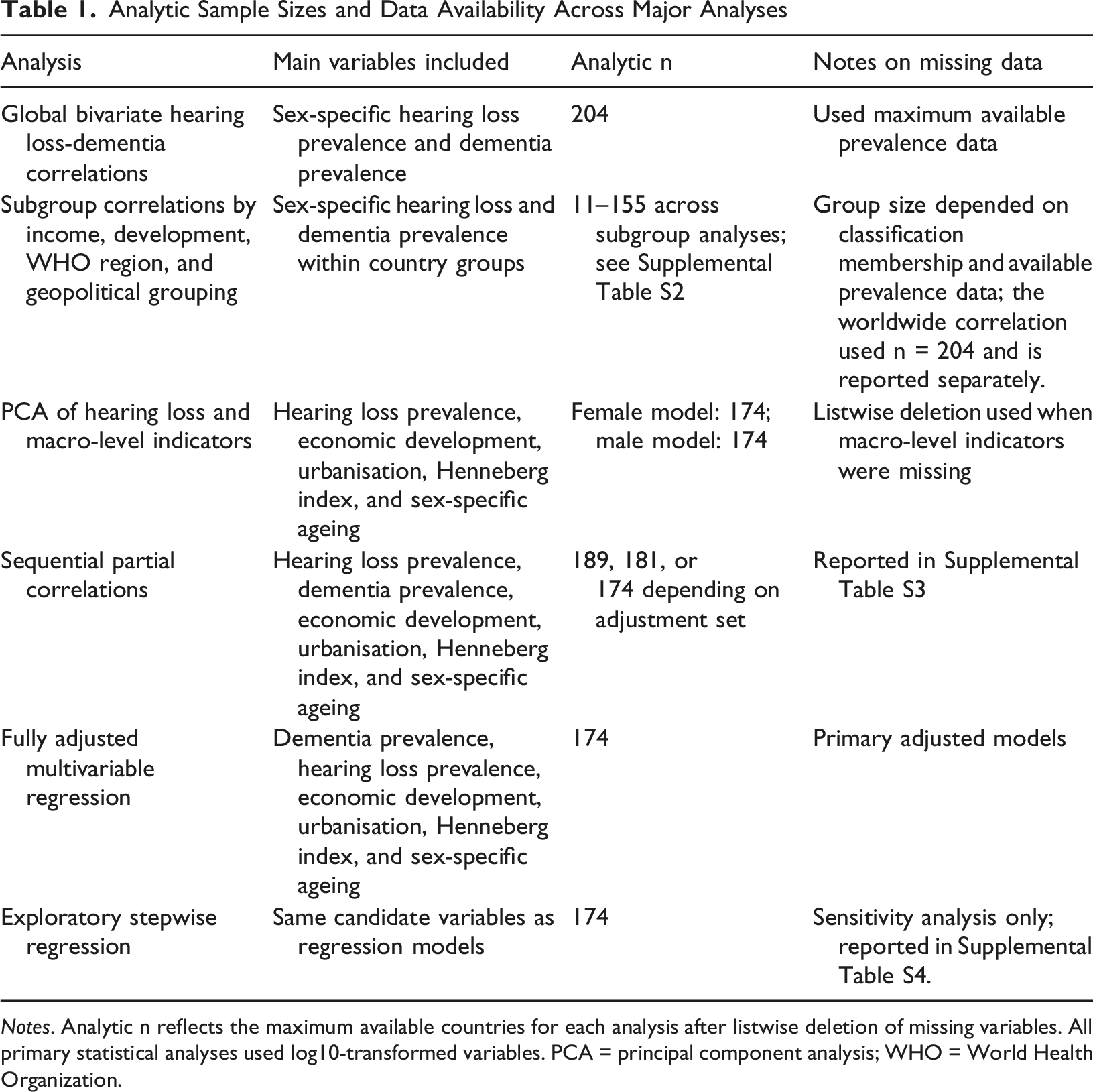
Notes. Analytic n reflects the maximum available countries for each analysis after listwise deletion of missing variables. All primary statistical analyses used log10-transformed variables. PCA = principal component analysis; WHO = World Health Organization.
Descriptive statistics for the key country-level variables are provided in Supplemental Table S1. This table summarises the available sample size, minimum, maximum, mean, and standard deviation for sex-specific hearing loss prevalence, sex-specific dementia prevalence, economic development, urbanisation, the Henneberg Index, and sex-specific life expectancy at age 60.
Sex-Stratified Association Between Hearing Loss and Dementia Prevalence
Figure 1 presents sex-stratified scatterplots of hearing loss prevalence and dementia prevalence across countries using untransformed rates. In both panels, higher hearing loss prevalence was associated with higher dementia prevalence. The overlaid polynomial curves are descriptive visual summaries of the raw-scale data and were not used for primary inference.
The visual pattern is consistent with the correlation and regression analyses conducted on log10-transformed variables. Because non-linearity was not the focus of the primary statistical framework, inferential interpretation is based on the log10-linear correlation, partial correlation, and multivariable regression models reported below and in the supplementary material.
Overall, Figure 1 provides descriptive visual support for a positive country-level association between hearing loss prevalence and dementia prevalence in both females and males, without implying causal inference or formally tested non-linear effects. Association between hearing loss prevalence and dementia prevalence across countries by sex. Panel A shows females and Panel B shows males.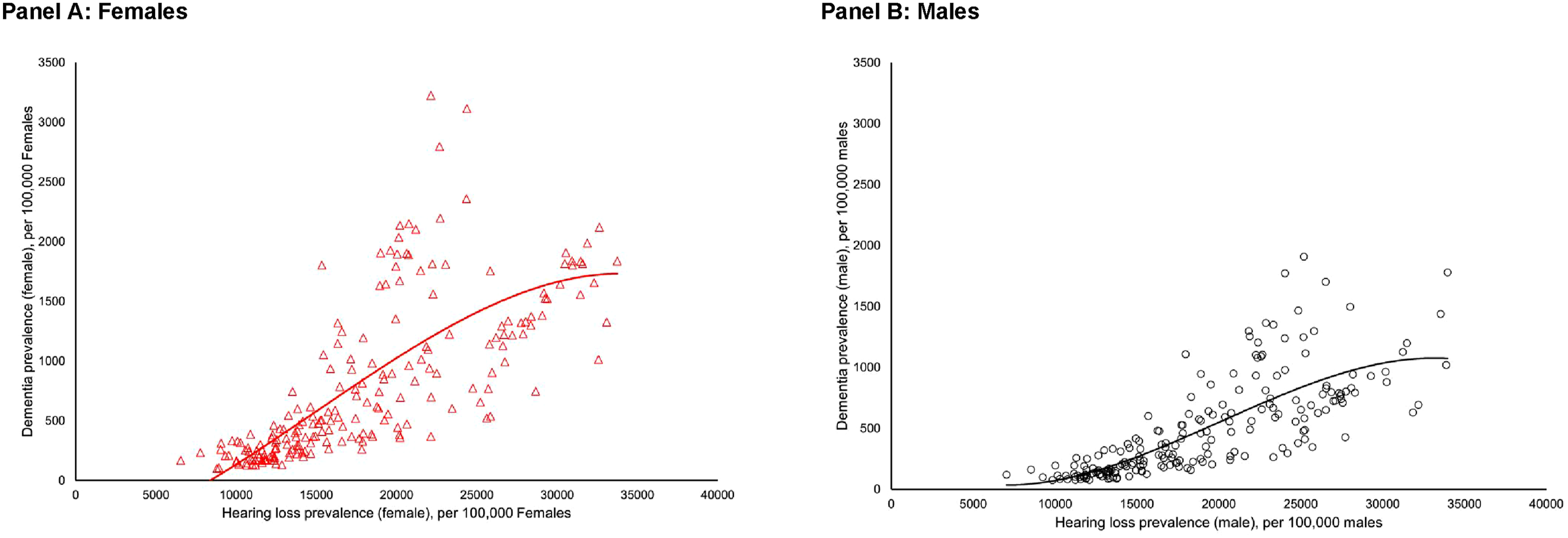
Country-level Correlations Between Hearing Loss and Dementia Prevalence
Pearson and Spearman Correlations Among Hearing Loss, Dementia, Socioeconomic, Demographic, and Ageing Indicators (log10-Transformed)
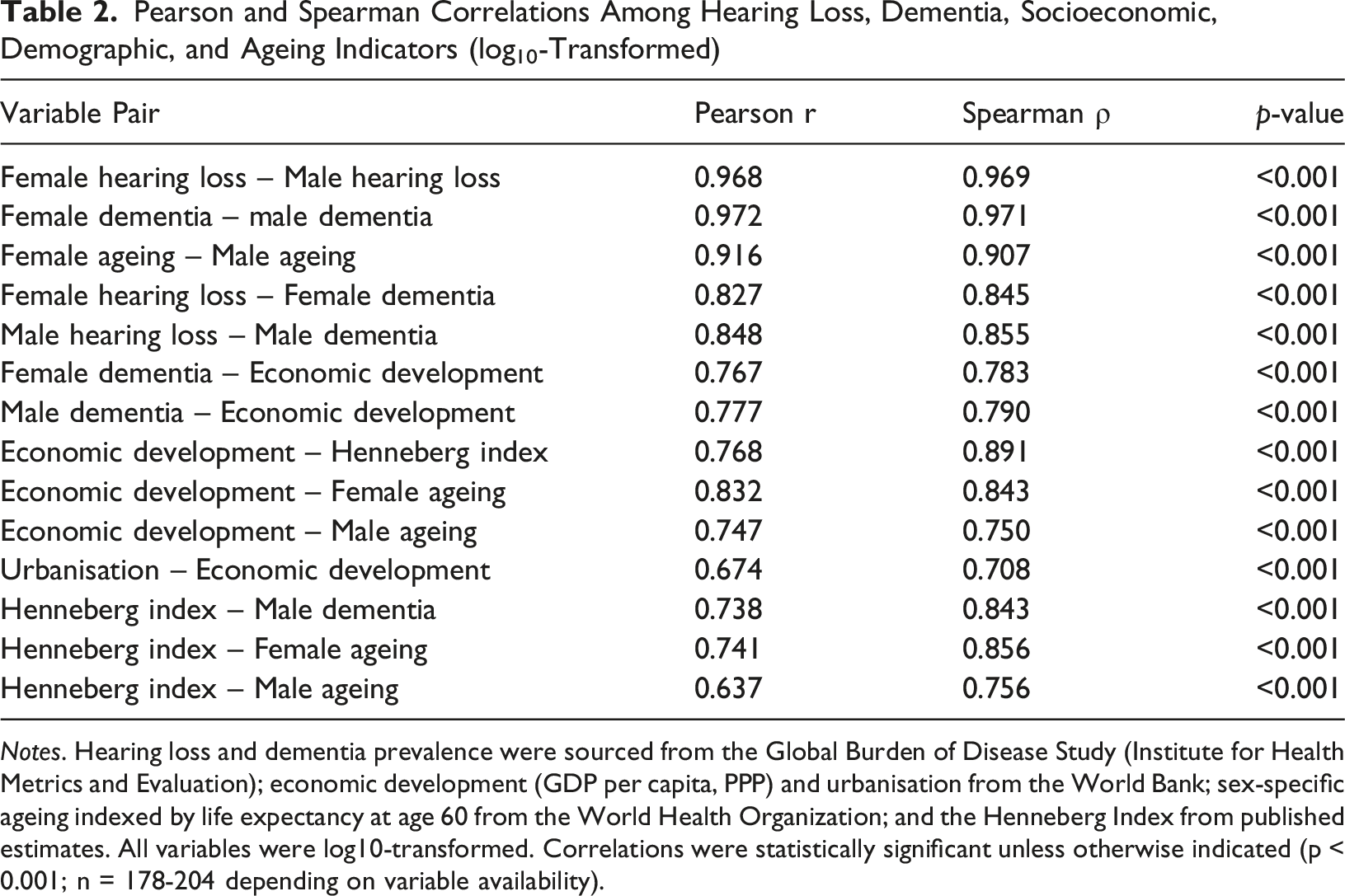
Notes. Hearing loss and dementia prevalence were sourced from the Global Burden of Disease Study (Institute for Health Metrics and Evaluation); economic development (GDP per capita, PPP) and urbanisation from the World Bank; sex-specific ageing indexed by life expectancy at age 60 from the World Health Organization; and the Henneberg Index from published estimates. All variables were log10-transformed. Correlations were statistically significant unless otherwise indicated (p < 0.001; n = 178-204 depending on variable availability).
Female hearing loss prevalence was strongly correlated with female dementia prevalence (Pearson r = 0.827; Spearman rho = 0.845; p < 0.001). Male hearing loss prevalence was also strongly correlated with male dementia prevalence (Pearson r = 0.848; Spearman rho = 0.855; p < 0.001). The similar coefficients indicate that the country-level association was evident in both sexes, while formal sex comparison is addressed in the regression section below.
Across sex-specific comparisons, Pearson and Spearman coefficients were concordant and statistically significant, supporting the robustness of the bivariate association (Table 2).
Sex-stratified correlations across income levels, development status, WHO regions, and selected geopolitical groupings are presented in Supplemental Table S2. At the global level, associations were strong in both females (Pearson r = 0.827; Spearman rho = 0.845) and males (Pearson r = 0.848; Spearman rho = 0.855).
Correlation strength varied primarily by socioeconomic context rather than sex. Associations were modest in low-income countries but strong in lower-middle- and upper-middle-income countries for both sexes, while correlations in high-income countries remained positive but attenuated. When grouped as LMICs versus high-income countries, correlations were significantly stronger in LMICs for both females and males. Similar patterns were observed across WHO regions and geopolitical groupings, with no region demonstrating a strong association in only one sex.
Overall, variation in correlation strength was driven more by income level, development status, and regional context than by sex, reinforcing the interpretation that the hearing loss-dementia association is broadly similar in females and males at the population level.
Principal Component Structure of Hearing Loss and Structural Indicators by Sex
Sex-stratified principal component analyses were conducted to assess whether hearing loss prevalence clustered with socioeconomic, demographic, and longevity-related indicators. Sampling adequacy was high in both models (females: KMO = 0.839; males: KMO = 0.829), and Bartlett’s tests of sphericity were significant (both p < 0.001), confirming suitability for factor analysis.
In both sexes, a single component (eigenvalue > 1) was retained, explaining 70.86% of total variance in females and 70.24% in males. All variables loaded positively and strongly on the component. Among females, the highest loadings were observed for economic development (0.933), ageing (0.903), Henneberg index (0.880), and hearing loss prevalence (0.762). A comparable pattern was evident in males, with strong loadings for affluence (0.939), Henneberg index (0.873), ageing (0.824), and hearing loss prevalence (0.821).
Principal Component Analysis of Hearing Loss, Socioeconomic, Demographic, and Ageing Indicators by Sex
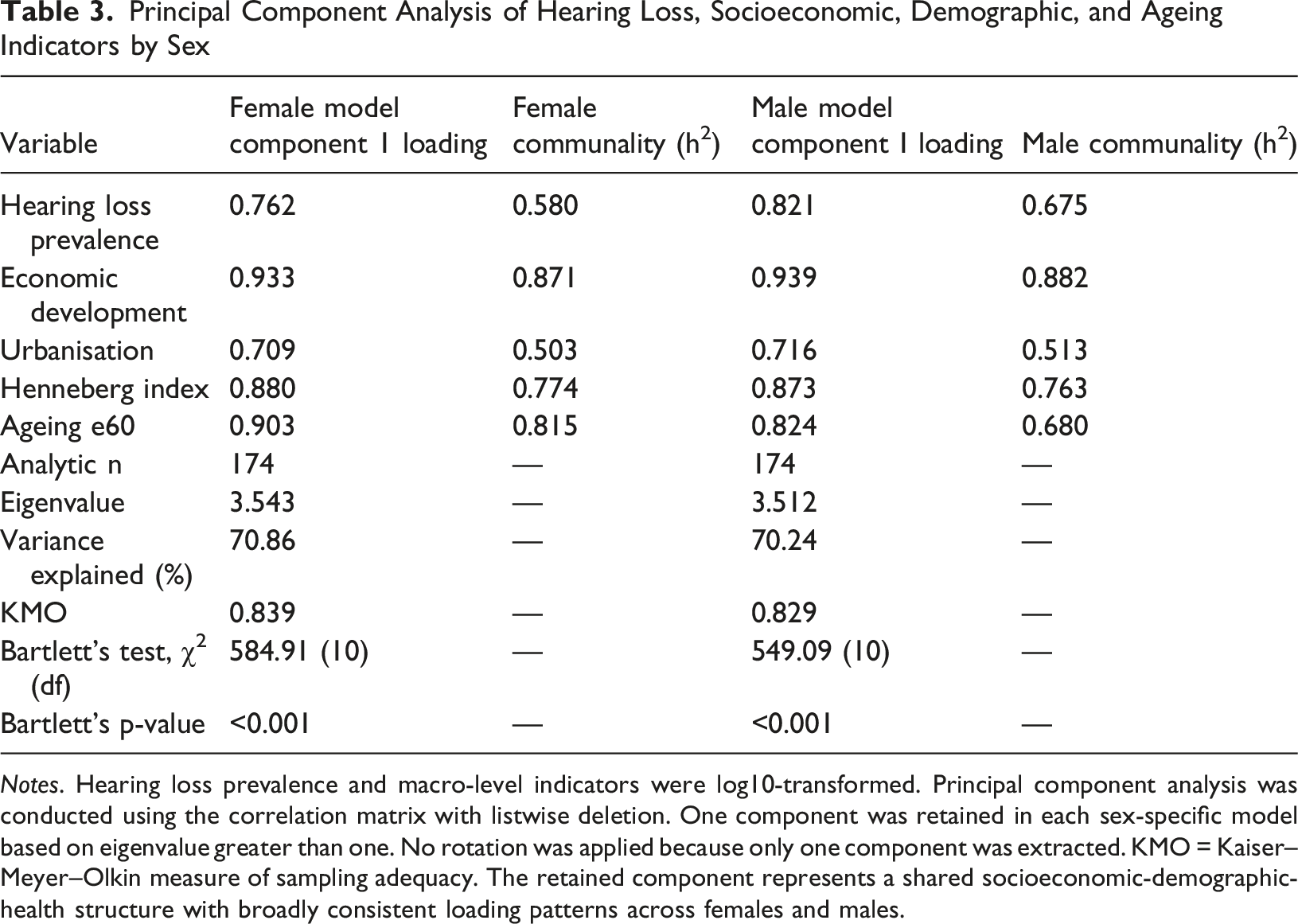
Notes. Hearing loss prevalence and macro-level indicators were log10-transformed. Principal component analysis was conducted using the correlation matrix with listwise deletion. One component was retained in each sex-specific model based on eigenvalue greater than one. No rotation was applied because only one component was extracted. KMO = Kaiser–Meyer–Olkin measure of sampling adequacy. The retained component represents a shared socioeconomic-demographic-health structure with broadly consistent loading patterns across females and males.
Sequential partial correlations are reported in Supplemental Table S3 as robustness checks. These analyses showed that the hearing loss-dementia association remained positive and statistically significant after progressive adjustment for economic development, urbanisation, Henneberg Index, and sex-specific ageing.
Theory-informed Multivariable Regression and Formal Sex Comparison
Multivariable Linear Regression Models Predicting Dementia Prevalence by Sex
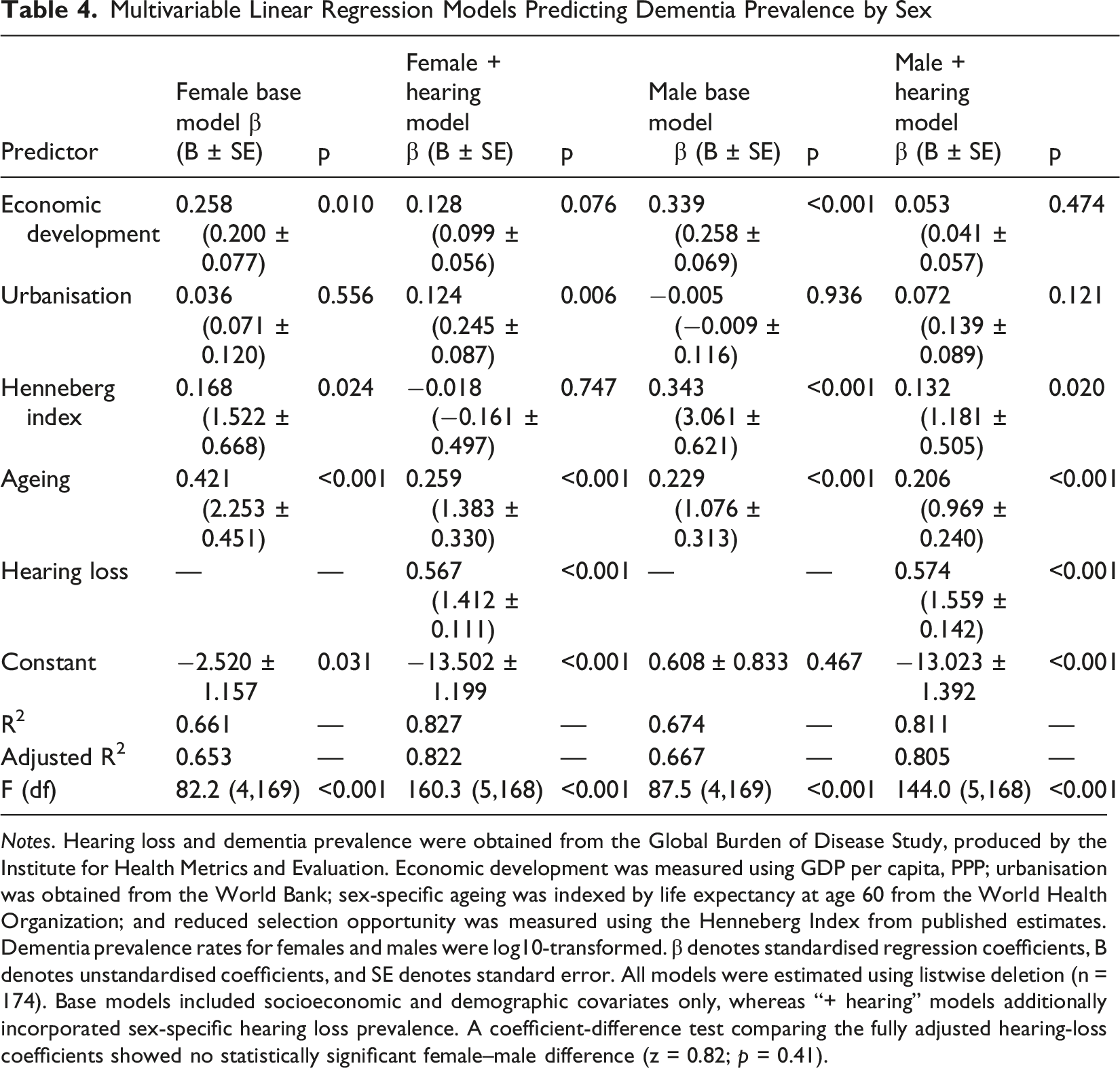
Notes. Hearing loss and dementia prevalence were obtained from the Global Burden of Disease Study, produced by the Institute for Health Metrics and Evaluation. Economic development was measured using GDP per capita, PPP; urbanisation was obtained from the World Bank; sex-specific ageing was indexed by life expectancy at age 60 from the World Health Organization; and reduced selection opportunity was measured using the Henneberg Index from published estimates. Dementia prevalence rates for females and males were log10-transformed. β denotes standardised regression coefficients, B denotes unstandardised coefficients, and SE denotes standard error. All models were estimated using listwise deletion (n = 174). Base models included socioeconomic and demographic covariates only, whereas “+ hearing” models additionally incorporated sex-specific hearing loss prevalence. A coefficient-difference test comparing the fully adjusted hearing-loss coefficients showed no statistically significant female–male difference (z = 0.82; p = 0.41).
In baseline models excluding hearing loss, socioeconomic and demographic covariates explained similar proportions of variance in dementia prevalence among females (R2 = 0.661) and males (R2 = 0.674). Ageing, economic development, and the Henneberg Index were retained as relevant macro-level covariates, whereas urbanisation was not consistently independently associated across baseline models.
After inclusion of sex-specific hearing loss prevalence, model explanatory power increased markedly for both females (R2 = 0.827) and males (R2 = 0.811). Hearing loss was the strongest correlate of dementia prevalence in both fully adjusted models (female: beta = 0.567, B = 1.412, SE = 0.111; male: beta = 0.574, B = 1.559, SE = 0.142; both p < 0.001).
Formal comparison of the unstandardised hearing-loss coefficients did not indicate a statistically significant difference between the female and male models (difference in B = 0.147; z = 0.82; p = 0.41). These results support a strong association in both sexes, while avoiding interpretation of small differences in parallel models as evidence of meaningful sex-based effect modification.
Exploratory stepwise regression sensitivity analyses are reported in Supplemental Table S4 and are not used as the basis for primary inference.
Discussion
This study adds global ecological evidence to the individual-level literature on hearing loss and dementia by examining whether the association is also evident at the country level. Using sex-stratified ecological data and complementary analytical approaches, the findings show that national hearing loss prevalence aligns closely with dementia prevalence in both females and males. This association persisted after adjustment for economic development, urbanisation, the Henneberg Index, and ageing, suggesting that hearing loss captures a population-level dimension of dementia burden not fully explained by the included macro-level covariates. These findings should be interpreted as ecological associations rather than evidence of individual-level risk or causality.
Population-level Relevance Beyond Individual Risk
At the individual level, hearing loss is well established as a risk factor for cognitive decline and dementia, supported by longitudinal cohorts, neuroimaging studies, and intervention trials (Lin et al., 2014; Loughrey et al., 2018; Mueller, 2024; Yu et al., 2024). The present study complements this evidence by showing that countries with higher hearing loss prevalence also tend to experience higher dementia prevalence, even when major macro-level determinants are considered. The ecological design means that these results cannot be translated directly to individual risk, but they do indicate that hearing health may be informative for population-level dementia surveillance and prevention planning.
The persistence of the association after adjustment challenges the interpretation that hearing loss prevalence merely reflects underlying socioeconomic development or population ageing (Liang et al., 2021; Nichols et al., 2022). While both hearing loss and dementia are shaped by demographic transition, the findings suggest that hearing loss prevalence captures an additional dimension of population-level vulnerability not fully explained by the covariates included in this analysis (Nichols et al., 2022; Alzheimer’s Disease International, 2025).
Structural Embedding Within Demographic and Socioeconomic Systems
These PCA and regression findings indicate that hearing loss prevalence is closely patterned within broader socioeconomic and demographic systems. Its alignment with economic development, urbanisation, longevity, and reduced selection opportunity suggests that hearing loss may function not only as a clinical condition, but also as a population-level marker of ageing, survival patterns, occupational and environmental exposures, and health-system capacity for detection and care (Emmett & Francis, 2015; Haile et al., 2021; Stevens et al., 2013; You & Henneberg, 2022; You et al., 2025). This structural patterning may help explain why hearing loss prevalence remains strongly associated with dementia prevalence across countries, even after adjustment for the included macro-level covariates (Krieger, 2024; Livingston et al., 2020; VanderWeele, 2019).
Rather than undermining the relevance of hearing loss, this contextual positioning strengthens its interpretability as a population-level indicator (WHO, 2021; VanderWeele, 2019). Hearing loss prevalence likely reflects cumulative exposure to multiple upstream influences across the life course, including prolonged survival into older age, diminished biological selection, environmental noise, occupational risk environments, and unequal access to hearing care (Basner et al., 2014; Man et al., 2021; Nelson et al., 2005). In this sense, hearing loss functions as an integrative marker linking biological vulnerability with social and environmental context, making it particularly informative for population-health analyses of dementia burden (Diez Roux, 2001; Peelle, 2018).
Sex-specific Patterns: Convergence Rather Than Divergence
Despite well-documented sex differences in dementia prevalence, longevity, and health trajectories, this study found broadly similar country-level hearing loss-dementia associations in females and males (Anstey, Peters et al., 2021; Huque et al., 2023). The sex-stratified models showed strong positive associations in both sexes, and formal comparison of the fully adjusted hearing-loss coefficients did not support a statistically significant female-male difference. Taken together, these findings support broad convergence between females and males rather than clear sex-based divergence in the country-level hearing loss–dementia association (Altman & Bland, 2003; Knol & VanderWeele, 2012).
Small numerical differences between female and male estimates may reflect differences in occupational noise exposure, cardiovascular profiles, healthcare access, or ascertainment patterns (Gong, Harris et al., 2023; Kim et al., 2018; Wang et al., 2021). However, these differences were not the main finding and should not be overinterpreted. The stronger conclusion is that the association was present in both sexes, while heterogeneity across income levels, development status, and regions appeared more prominent than sex-based divergence.
Income and Development Gradients
The attenuation of associations in high-income and highly developed countries warrants careful interpretation. In these settings, widespread access to hearing aids, cochlear implants, and rehabilitative services may mitigate the functional and social consequences of hearing loss, while more comprehensive cognitive screening and diagnostic infrastructure may alter dementia ascertainment patterns (Lin et al., 2023; Mick et al., 2014; Shukla et al., 2020). In contrast, in low- and middle-income settings, untreated hearing impairment may exert a stronger population-level impact through pathways such as social isolation, communication barriers, delayed healthcare access, and reduced cognitive stimulation (Olusanya et al., 2014; Stern, 2012; World Health Organization, 2021).
An alternative explanation is saturation. In highly aged populations where both hearing loss and dementia prevalence are already elevated, between-country variability may be limited, reducing observable correlations (Bloom et al., 2015; Harper, 2014). Importantly, these income- and development-related gradients were similar for females and males, further supporting the interpretation that contextual factors, rather than sex, are the primary drivers of heterogeneity in association strength (Diez Roux, 2001; Krieger, 2024; You, 2025).
Implications for Dementia Prevention and Public Health
The findings have implications for dementia prevention and surveillance. While individual-level research has established hearing loss as a modifiable risk factor for cognitive decline and dementia, the present analysis shows that hearing loss prevalence is also a country-level correlate of dementia prevalence. This supports the inclusion of hearing health indicators in broader population-health approaches to cognitive ageing.
From a public health perspective, earlier identification of hearing impairment, improved access to affordable hearing technologies, and integration of hearing care into primary healthcare may be relevant for dementia prevention strategies, particularly in low- and middle-income settings where untreated hearing loss remains common. However, intervention effects cannot be inferred from the present ecological analysis.
The observed association should not be interpreted as evidence of direct causality. Hearing loss prevalence likely reflects cumulative biological, social, environmental, and structural influences shaping dementia risk across populations. Nevertheless, the consistency of the association suggests that hearing loss may function as a useful population-level indicator within dementia surveillance frameworks.
Effective prevention requires addressing upstream determinants, as hearing loss is embedded within demographic transition, requiring integrated clinical and policy responses.
Strengths and Limitations
This study has several strengths. It draws on a global dataset with wide geographic coverage, uses a sex-stratified ecological framework, and relies on harmonised international estimates. The use of multiple analytical approaches, together with formal coefficient comparison and relocation of stepwise analyses to the supplementary material, strengthens the transparency of the revised analysis while avoiding overreliance on data-driven model selection.
Several limitations should be acknowledged. As an ecological analysis, the findings cannot be interpreted as reflecting individual-level risk or causal relationships. Residual confounding may persist due to unmeasured or imperfectly captured factors such as education, cardiovascular disease burden, healthcare quality, hearing-aid uptake, diagnostic practice, or dementia ascertainment. Prevalence estimates for hearing loss and dementia are modelled estimates and may vary in precision across regions, particularly where primary data are sparse. Finally, the cross-sectional design precludes assessment of temporal sequencing or lagged effects between hearing loss exposure and subsequent dementia outcomes.
Future research integrating longitudinal population-level data, lagged exposure models, and multilevel designs linking individual and contextual data would help clarify underlying pathways and strengthen causal inference.
Conclusion
This study provides evidence that hearing loss prevalence is a strong and consistent country-level correlate of dementia prevalence worldwide in both females and males. Formal comparison did not support clear sex-based divergence in the adjusted hearing loss-dementia association. Overall, the findings position hearing loss as an important population-level indicator within the global dementia landscape, reflecting the combined influence of biological vulnerability and macro-level social and demographic context.
Supplemental Material
Supplemental Material - Hearing Loss and Dementia Prevalence Across Countries: Global Eco-logical Evidence in Females and Males
Supplemental Material for Hearing Loss and Dementia Prevalence Across Countries: Global Eco-logical Evidence in Females and Males by Wenpeng You in Dementia
Footnotes
Acknowledgements
The author acknowledges the international organisations that curate and maintain the publicly available datasets used in this study.
Ethical Considerations
Ethical approval was obtained from the Office of Research Ethics, Compliance and Integrity (ORECI), The University of Adelaide (Approval No. 36289).
Consent to Participate
Consent to participate was not applicable, as this study used publicly available, de-identified data.
Author Contributions
Wenpeng You: Conceptualization; Data curation; Formal analysis; Investigation; Methodology; Writing – original draft; Writing – review and editing.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data analysed in this study are described in the Methods section and were obtained from publicly available databases maintained by international organisations. As all datasets are openly accessible for non-commercial research use, no additional approvals were required, in accordance with the data access policies of the respective data providers.
GEN AI Use Statement
Generative AI or AI-assisted tools were not used in the creation, modification, or enhancement of any figures, images, artwork, or graphical materials in this manuscript. All visual elements were produced using standard statistical software based on the original study data. Generative AI did not contribute to the study design, analytical procedures, or methodological processes, and no AI-generated artwork, graphical abstracts, or cover images were included in this submission.
Supplemental Material
Supplemental material for this article is available online.
Author Biography
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.