
Abstract
This study explored the experiences of people living with dementia and their care partners attending a nurse practitioner-led, community-based, multicomponent memory clinic in regional Australia. Guided by Nussbaum’s Central Human Capabilities, a qualitative descriptive design was used to examine how the model of post-diagnostic dementia care supported living a life of dignity. Emotional touchpoint interviews were conducted between January and May 2025 with people who had attended the clinic for six months or more. Fourteen interviews were completed with people living with dementia (n = 8) and care partners (n = 6), and analysed thematically. Four themes were generated: emotional safety in a predictable, respectful group; relational autonomy and everyday choice; feeling truly known, respected, and connected; and meaningful engagement through accessible challenge and play. People with dementia described the value of familiar routines, social connection, physical exercise, cognitive stimulation, creativity, humour, and supported choice. These experiences promoted feelings of safety, confidence, enjoyment, belonging, autonomy, and meaningful contribution. Care partners reinforced these experiences, highlighting the importance of predictability, emotional safety, individualised support, and being genuinely known within the group. The findings suggest that post-diagnostic dementia care can move beyond biomedical models focused on diagnosis, treatment, loss, and decline. Nurse practitioner-led, community-based models can support dignity when they create relational and emotional conditions in which people living with dementia can feel safe, make choices, express emotion, remain connected, and experience themselves as capable. This study highlights the potential of capability focused, nurse-led dementia care in promoting accessible, person-centred, and emotionally safe post-diagnostic support.
Keywords
Background
Dementia is often framed in terms of decline and loss, contributing to a deficit-based understanding of people living with the condition. Yet a diagnosis of dementia does not negate personhood, relationships, meaning, or the possibility of living well. As dementia prevalence grows globally, there is increasing urgency to provide post-diagnostic care responsive to cognitive and physical changes, but that also addresses emotional and social care needs of people living with dementia (Department of Health and Aged Care, 2024; Low et al., 2021; World Health Organization [WHO], 2025). Although two-thirds of Australians with dementia live in the community, post-diagnostic support is limited, and where support does exist, it rarely promotes wellbeing, inclusion, hope, or a sense of purpose (Department of Health and Aged Care, 2024; Pavković et al., 2024). There remains an opportunity for post-diagnostic care to better support people with dementia to live lives of dignity and meaning.
Current models of post-diagnostic dementia care continue to focus on information about diagnosis and pharmacological treatment (Naismith et al., 2022; Pavković et al., 2024, 2025), despite limited long-term benefits of pharmacological interventions alone (Dyer et al., 2018; Reuben et al., 2024). In contrast, growing evidence identifies social and non-pharmacological approaches can increase a sense of purpose and wellbeing for people with dementia (Desai et al., 2024; Low et al., 2021; Pavković et al., 2025; Woods et al., 2023). Cognitive stimulation is one such approach, with evidence supporting its role in improving cognition, communication, mood and quality of life for people with mild to moderate dementia (Woods et al., 2023). There is also growing interest in multicomponent models that combine cognitive, physical, creative, and social activity delivered by multidisciplinary teams (D’Cunha et al., 2025; Woods et al., 2023). These models recognise the person beyond physical symptoms of dementia, and create opportunities for engagement and enjoyment.
Nurses are well placed to lead such models of care. Nurse-led multidisciplinary clinics facilitate continuity, coordination, accessibility, and person-centred care across a range of conditions and care settings (Australian College of Nursing, 2024; Department of Health Disability and Ageing, 2025; Terry et al., 2024). However, evidence specific to nurse practitioner-led dementia care is limited (Luck & Doucet, 2021). Nurse practitioner-led, community-based models may offer one way to respond to the complex and evolving needs of people living with dementia after diagnosis, particularly when care needs extend beyond biomedical assessment and treatment to include social, emotional, cognitive, and relational support.
Nussbaum’s theory of Central Human Capabilities provides a framework for understanding what it means to live well with dementia. Nussbaum argues that a life of dignity is one in which people have genuine opportunities to develop and exercise capabilities; to do and be what they have reason to value (Nussbaum, 2000, 2010, 2011). These capabilities include being able to experience emotions, form meaningful relationships, engage in thought and creativity, participate in choices affecting one’s life, and enjoy play and recreation (Nussbaum, 2011). A capabilities approach is particularly relevant to dementia care because it does not make dignity, moral worth, or personhood dependent on rationality, and therefore offers a way to recognise the continuing personhood of people living with dementia. This approach recognises that all people, including those with cognitive disability, require social and care conditions that enable capability, affiliation, expression, and flourishing (Nussbaum, 2000, 2011). This approach shifts attention from deficit and dependency to consider how everyday care practices may support or limit experiences of dignity for people living with dementia.
Existing evidence offers limited accounts from people with dementia themselves about their experiences of post-diagnostic care, despite international and national policy advocating for inclusivity (Department of Health and Aged Care, 2024; WHO, 2025). This qualitative study is part of a larger evaluation of a nurse practitioner-led, community based, multicomponent memory clinic and its impact on cognition, psychological wellbeing, and quality of life for people living with dementia and their care partners (Beattie et al., 2025). The aim of this study was to explore experiences of participation in the clinic. The research questions were: (1) In what ways does participation in the clinic support living a life of dignity for people with dementia? and (2) How do people with dementia perceive their experience within a nurse practitioner-led model of dementia care?
Methodology and Methods
Research Design
This study used a qualitative descriptive design to explore how people with dementia experienced participation in a nurse practitioner-led, community-based multicomponent memory clinic. Qualitative description is suited to studies seeking to stay close to participants’ accounts and generate findings meaningful to practice, policy and service development (Tisdell et al., 2025). Nussbaum’s (2011) Central Human Capabilities provided an orienting framework. Reporting followed Tong et al.’s (2007) Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist, with reflexivity and theoretical positioning informed by Braun and Clarke’s (2025) Big Q Qualitative Reporting Guidelines to promote transparency and trustworthiness of the study (Guba & Lincoln, 1989).
Setting
The study was undertaken in a nurse practitioner-led, community-based multicomponent memory clinic in a major regional centre in New South Wales, Australia. The clinic opened in September 2022 to address a local gap in post-diagnostic dementia care. The clinic was developed through consultation with people living with dementia, geriatricians, aged care clinical nurse consultations, exercise physiologists, and academics.
The clinic was nurse practitioner-led, with the nurse practitioner providing initial assessment, clinical oversight, care coordination, review, and referral. At entry, people with dementia and their care partners attended an initial nurse practitioner consultation to discuss medical and life history, functional abilities, interests, goals, and current support needs. Participants then chose a weekly individualised program from the available components in consultation with the multidisciplinary team members. These components included cognitive stimulation, art and creative activities, low-intensity yoga, and exercise sessions (Figure 1). Cognitive stimulation included activities such as puzzles, games, and Lego® model building, and art sessions included painting, clay, craft, and drawing; both were facilitated by registered nurses. Exercise sessions were facilitated by an exercise physiologist, and low-intensity yoga was facilitated by a trained instructor and offered to people with dementia and their care partners. Programs were reviewed every eight to 12 weeks and adjusted in response to changing capabilities, feedback, goals, and availability. Additional nurse practitioner appointments were available to discuss health and wellbeing concerns, coordinate care, or facilitate referrals as required. A monthly support group was also offered to care partners by a mental health registered nurse. Clinic activity program choices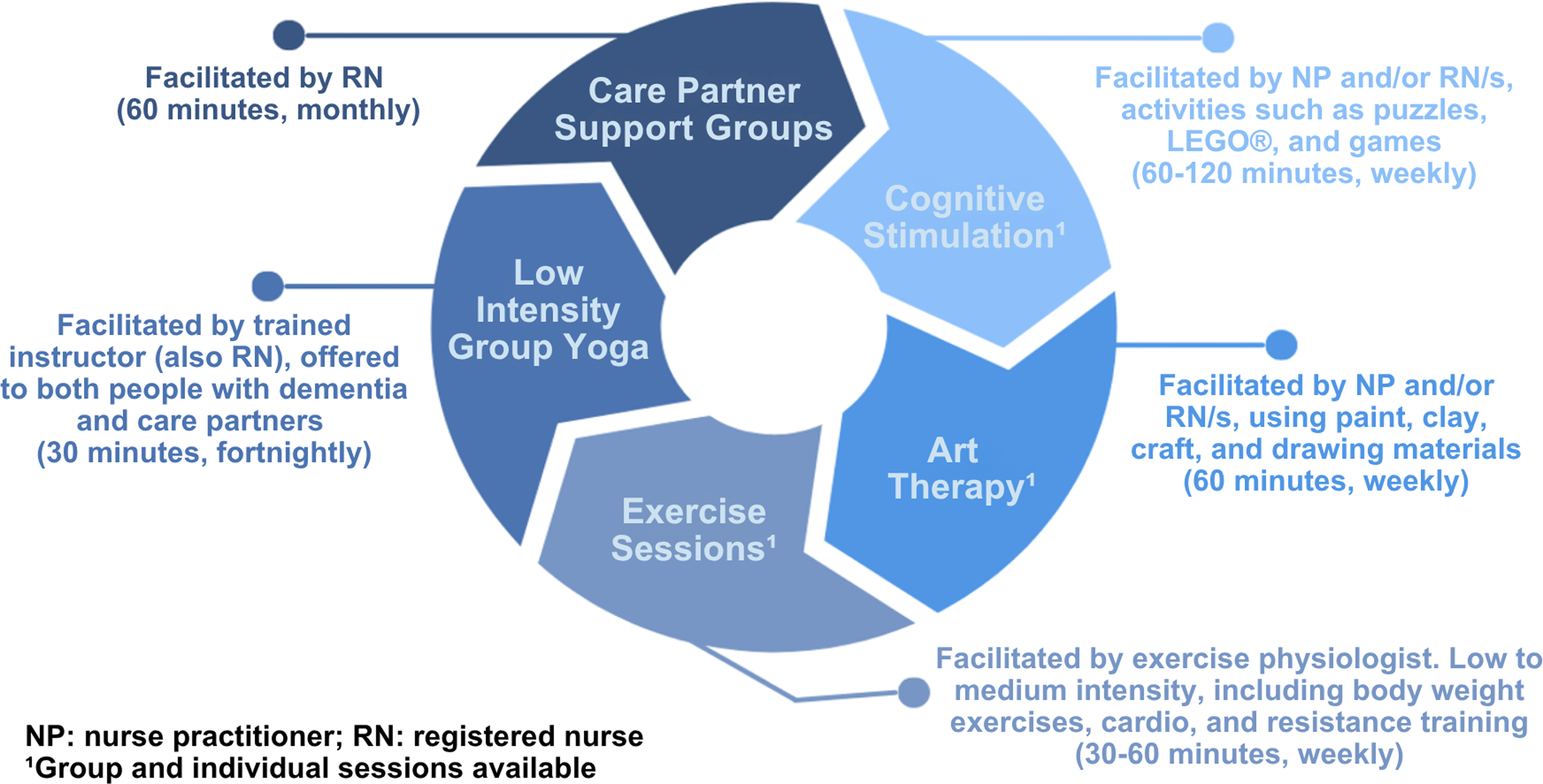
Participants
Participants were eligible if they had a diagnosis of early to moderate dementia, spoke and understood English, and had attended the clinic for at least six months. Care partners were also invited to offer complementary perspectives. Study information sheets were distributed to eligible participants, followed by email invitations. Invitations stated participation was voluntary, and would not impact ongoing involvement in the clinic.
Data Collection
Data were collected through emotional touchpoint interviews. This structured interviewing approach enables people with communication or cognitive difficulties to share perspectives by identifying and describing emotions about an experience (Alzheimer’s Society, n.d; Dewar et al., 2010). The Interview guide was developed by the first and last authors, informed by the study aims and emotional touchpoint method (Dewar et al., 2010). Questions focused on key moments in the clinic experience, including arrival, participation in activities, leaving the clinic, and perceived changes over time. Questions were piloted and minor wording refinements were made before interviews commenced.
People with dementia were asked questions such as “How do you feel when you arrive at your clinic session?”, “How do you feel about participating in the activities in the clinic?”, and “How do you feel after your clinic session?”. Care partners were asked questions such as “How do you feel about the person you care for attending the clinic?” and “Have you noticed any changes in the person you care for since attending the clinic?”. Participants chose one or more printed emotion cards, with blank cards available for emotions not represented (Figure 2), and invited to explain why they chose each emotion. Emotions were understood to be evaluative rather than inherently positive or negative (Nussbaum, 2011). Emotional touchpoint cards used during interviews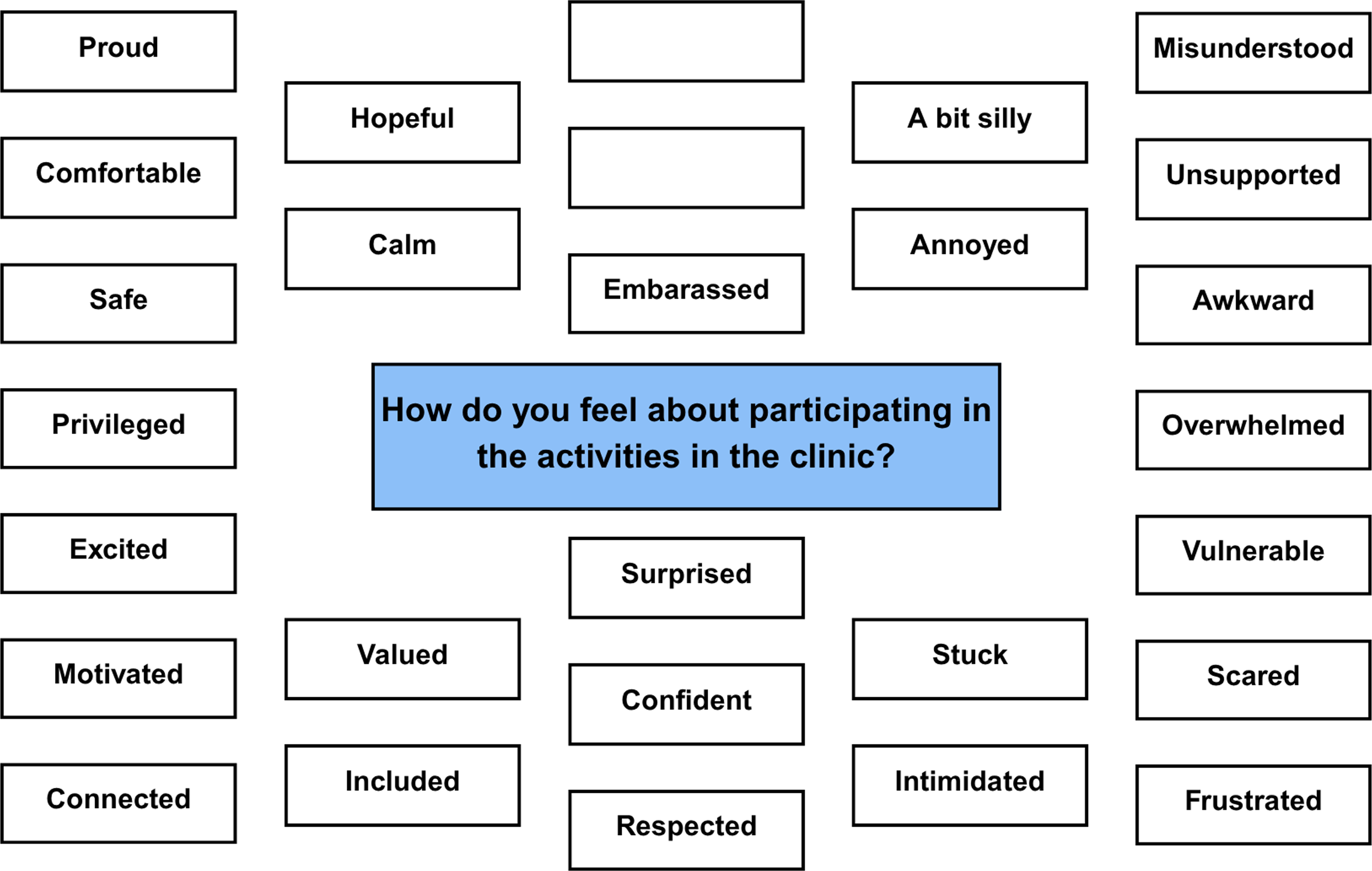
Eight people with dementia and six care partners were interviewed (n = 14). Participants had attended the clinic for an average of 16.5 months (range: seven to 32 months). Some people with dementia chose to have their care partner present during interview, and vice versa. Interviews were conducted in the clinic between January and May 2025 by the first and last authors, both experienced qualitative interviewers. Interviews lasted 11 to 63 min (mean 27 min), were audio-recorded and professionally transcribed. Participants were given the opportunity to review transcripts, make changes, or withdraw before analysis. All transcripts were de-identified with participant-chosen pseudonyms.
Data Analysis
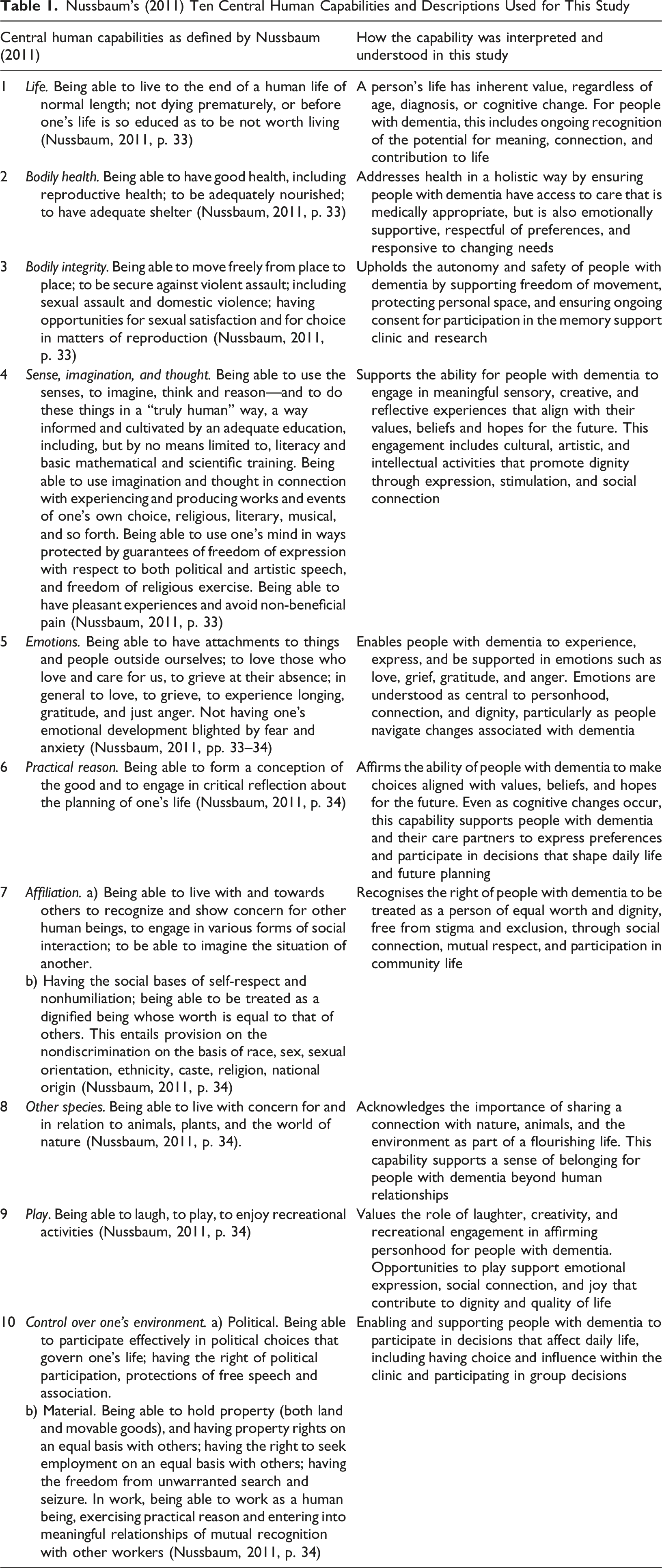
Nussbaum’s (2011) Ten Central Human Capabilities and Descriptions Used for This Study
Transcripts from people with dementia and care partners were analysed separately. The first and second authors focused on interviews with people with dementia, while the third and last authors focused on care partner interviews. This approach enabled the voices of the people with dementia to be privileged, while recognising care partners’ perspectives as a meaningful, yet different. Coding was undertaken in a shared Microsoft Excel spreadsheet, with regular team discussions to refine interpretations and ensure themes reflected participants’ accounts, emotional experiences, clinic context, and the research questions. Regular team discussions supported credibility and dependability through the analysis process (Guba & Lincoln, 1989).
Ethical Considerations
Ethical approval was obtained from the University of Wollongong Human Research Ethics Committee (2022/082) before commencing recruitment and information collection. Informed written consent was obtained before participation. Research involving people with dementia raises specific ethical considerations regarding capacity and consent. This study utilised Dewing’s (2007, 2008) process consent, viewing decision capacity as contextual and changeable over time, rather than a fixed state. Consent was an ongoing ethical practice, with interviewers monitoring assent, dissent, or signs of discomfort in participants. This approach aligns with person-centred research principles and a relational view of autonomy, where decision making is supported through trusted relationships (Dewing, 2008; Jacobs et al., 2017). To protect confidentiality and personhood, participants chose pseudonyms to avoid dehumanising means of identification, such as with a number (Braun & Clarke, 2025).
Rigour and Reflexivity
The first and last authors were nurse leaders of the memory clinic and had established relationships with participants through the clinic. This familiarity supported trust and contextual understanding during interviews, consistent with relational, person-centred qualitative research (Dewing, 2007; Jacobs et al., 2017); but also created potential power dynamics. In particular, participants may have felt reluctant to express any negative feedback about the service or practitioners involved in their care.
Several strategies supported the credibility of data generation (Guba & Lincoln, 1989). Study invitations detailed that participation was voluntary and would not affect ongoing involvement in the clinic. Participants were offered an alternative interviewer, although all preferred to speak with someone familiar. Emotional touchpoint cards included positive, negative, and ambivalent emotions, with blank cards available, encouraging participants to identify a range of experiences. Interviewers invited elaboration on all emotions chosen, and prompted participants to consider whether any feelings or experiences had been missed. Reflexivity was embedded in the analysis process, where the research team discussed how existing relationships may have shaped both what was shared and how accounts were interpreted. Authors with different relationships to the clinic contributed to analysis, and regular team discussions were used to question interpretations and consider if positive participant accounts were overly influencing theme development. These reflexive and collaborative strategies supported the credibility, dependability, and confirmability of the analysis, contributing to the overall trustworthiness and rigour of the study (Guba & Lincoln, 1989).
Findings
The findings of this study are presented in four themes: (1) emotional safety in a predictable, respectful group; (2) relational autonomy and everyday choice; (3) feeling truly known, respected, and connected; and (4) meaningful engagement through accessible challenge and play. Figure 3 provides a summary of the themes and links with the clinic components and Nussbaum’s (2011) central human capabilities. In presenting the themes, the voices of people with dementia are centred, with care partner perspectives included to deepen interpretation. Participant characteristics (such as age, gender, and dementia type) have not been included to uphold confidentiality. These characteristics were also not relevant to the aim of the study and did not meaningfully contribute to participants’ experiences. Creating capabilities within a nurse practitioner-led model of dementia care to enable living a life of dignity (flourishing) for people living with dementia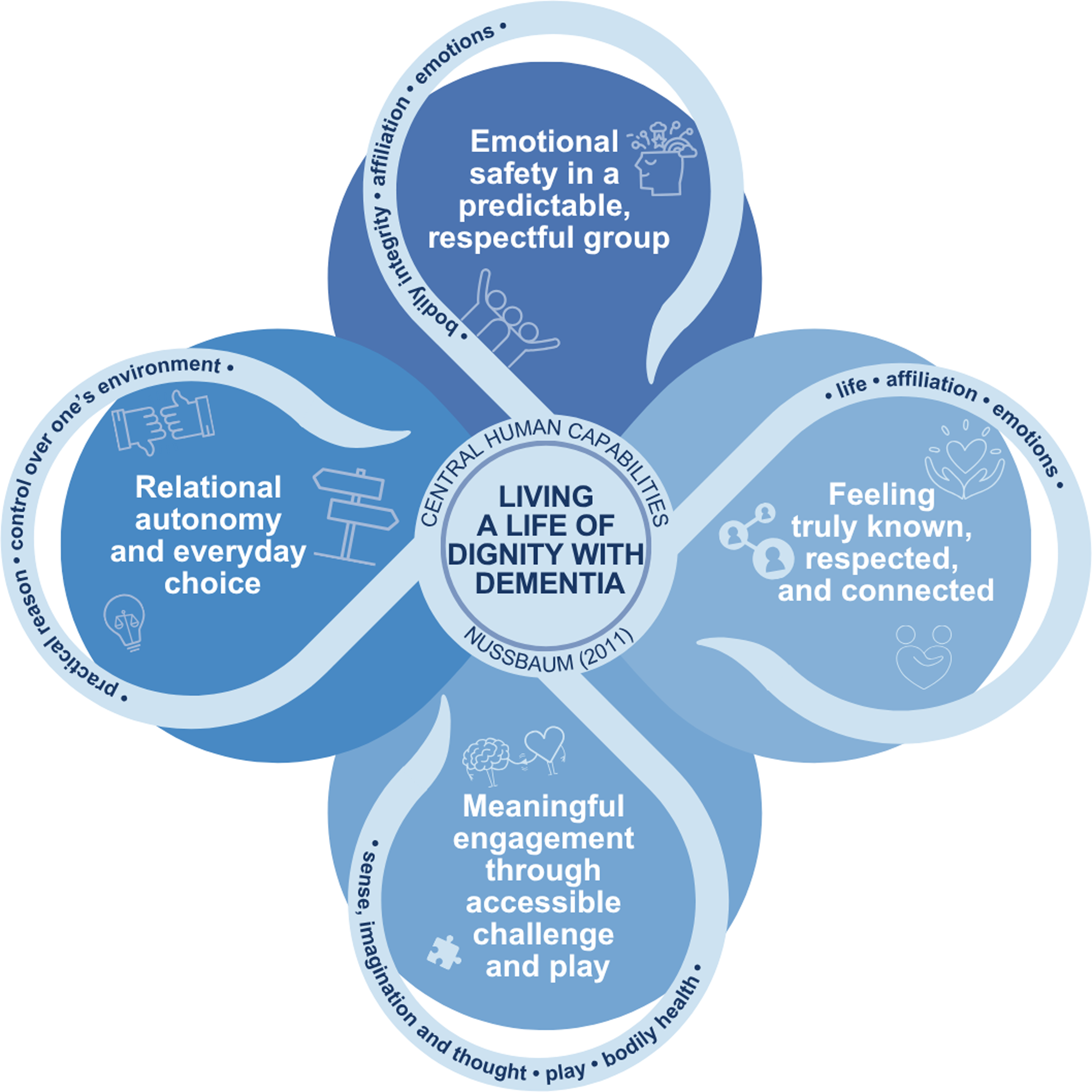
Emotional Safety in a Predictable, Respectful Group
(Linked with capabilities: bodily integrity; affiliation; emotions)
Participants consistently described the clinic as a place where they felt safe and comfortable. These feelings were linked to predictable routines, familiar people, and respectful interactions. Ken stated, “Yes, I feel comfortable… reassured,” and Al, Dave, and Jeff also described feeling comfortable. Birdie said, “I feel safe,” and elaborated “because I’ve connected by the time I leave, well I feel safer.” Recognition on arrival contributed to this sense of safety. Smokey described, “There’s the lovely lady at the front. Always greets us. Friendly, warm smile,” and Jeff said, “When I walk in there, ‘I know that person.’ And you feel comfortable.” These accounts illustrate how ordinary acts of recognition and familiarity supported emotional safety.
The clinic also provided a space where people with dementia could express emotion without judgement. Dave described an “easy” feeling in expressing emotions and Rosie described group conversations were an outlet for her emotions. For some, activities and interactions also surfaced frustration, grief, and awareness of change. Jim explained difficulty finding words during sessions, “Yes, yes. And that’s what’s [messed] up, you know?” He later added, “everybody knows everybody,” suggesting the familiarity within the group helped to make frustration be expressed without judgement. Birdie described grief during activities; “I feel frustrated that once upon a time I could have done that. And I think that’s what the—the feeling around that was grief.” Her account shows that meaningful activity could bring attention to both enjoyment and changing abilities, and that the clinic was a space where these emotions could be expressed and supported in a familiar and respectful environment.
The safe and respectful culture of the clinic supported ongoing attendance. When asked if he ever did not want to attend, Jim said, “No, I don’t do that, no” and Rosie said, “No. No. No” when asked if she felt anxious about attending. Smokey described “lots of positive encouragement, reinforcement. No-one sort of belittled at all,” and Dave noticed the group members as “easy to talk to.” These accounts suggest that emotional safety was created through repeated, respectful interactions that made participation feel possible and worthwhile.
Care partners also recognised the emotional safety of the clinic. Alexandra felt comfort knowing “he’s in somebody’s good care … He seems to be comfortable.” Robyn stated, “He really enjoys it… he goes, ‘The girls are so nice.’” Erica compared the clinic with other programs that created worry: “he wants to take a pen with him. But when he comes here, he doesn’t … Other places, he’ll often say, ‘I’ve forgotten to bring this … I haven’t got that in my pocket.’ And he gets worried.” The experiences highlight how predictability and relational familiarity reduced anticipatory anxiety and supported bodily integrity as more than physical safety. Participants could arrive, move, interact, and express emotion in a setting experienced as respectful and safe.
Relational Autonomy and Everyday Choice
(Linked with capabilities: practical reason; control over one’s environment)
People with dementia described autonomy as something exercised through everyday preferences, adaptations, and choice about participation. Birdie offered a clear example when deciding whether to buy a puzzle: “I nearly bought it but then I thought, ‘No, I’m not going to do a thousand pieces.’ And I knew it would be difficult because of the colours … I’ve had to adjust my expectations, having dementia.” Her account shows practical reason in action; recognising changing capability while maintaining enjoyment and choice. Similarly, Rosie wanted to keep painting: “I’d like to do more … paint,” and used alternative painting methods, such as sponges, which accommodated her physical limitations; which she explained, “it helps.” These examples show how autonomy was supported by adapting activities so participation remained possible and meaningful.
Participants also described choosing how and when to engage socially. Smokey said, “I’m very comfortable doing my own thing. I do enjoy, depending on the activity, being able to mix with others,” identifying that group participation was about flexibility. Dave spoke about choice and engagement, “Look I’ve been doing this, and doing that, and doing something else and thinking, ‘I’ll do it. I’m going to do it.’” Jeff also offered he “never thought it was a waste of time.” These experiences highlight that ongoing attendance was not passive, and reflected participants’ own assessment and choice based on value, comfort, and interest.
Care partners reinforced these accounts by describing changes in confidence and initiative. Alexandra described how the person she supports initially resisted help but now chooses to attend, “He was just so unaccepting of any help that I was trying to organise… and he’s been going there, what, a year now, and he likes going and he comes back happy.” Alexandra’s reflections illustrate how preferences as to what is good and meaningful can evolve for a person with dementia following new experiences. Robyn described active choices to prepare to attend, “He goes ‘Well, I’ll need to have a shower then, won’t I?’” Erica shared the clinic’s support for both the person with dementia and care partners as creating “a synergy that you can’t really get from other places.” These accounts demonstrate relational autonomy as shared and supported, with choices made through trusted relationships, meaningful activities and changing confidence over time.
Autonomy was visible in small, everyday ways; choosing activities, adjusting expectations, preparing to attend, choosing when to join others, and continuing participation because it felt worthwhile. For some, control over one’s environment extended to the continuity in access to the clinic. Smokey noted, “Probably the only thing that I find a little bit frustrating is the eight-week blocks” suggesting that once the clinic had become meaningful, ongoing access to it was also experienced as a part of autonomy and dignity. The clinic supported people with dementia to reason, decide, and act in ways they felt they had control over, and participants recognised that autonomy was strengthened through relational and practical support.
Feeling Truly Known, Respected, and Connected
(Linked with capabilities: life; affiliation; emotions)
Participants described feeling known and valued within the clinic, which affirmed identity, purpose, and belonging. The clinic recognised the contributions and connections people with dementia can continue to make, despite changes in cognition and ability. Birdie described a renewed sense of self, stating “I do feel respected again for my contribution” and said the clinic “has enabled me to believe that there’ll always be something that I can do.” Similarly, Dave shared how being known is meaningful, “…it’s nice to have someone that wants to know me” and “I feel part of it.” For Jim, continuing to actively participate in life was important: “Well, you’ve got to go somewhere!” while Birdie described participation as connecting her “to the human experience.” These reflections demonstrate how being recognised and included supported personhood as ongoing, and not diminished by diagnosis.
Social connection was created through mutual respect, acceptance, and genuine interest in others. Rosie stated, “When I’m here, I love it. Every time … I love all of you.” For Al, the opportunity for social connection was important; “I like mixing with people… your clinic was particularly good at getting people to mix,” and described being “overwhelmed” by the respect shown to him. Jim and Jeff both talked about having made friends at the clinic, and Jeff described the group as “super” and added, “Everyone would help you if you asked for it.” For Jeff, connection was about genuine interest: “Talk to them properly and be friendly and talk to them about their family and things like that.” Ken found it reassuring to be part of a group who, “all seem to have the same sort of targets, aims.” Belonging, therefore, was active and reciprocal for participants and not just about being in the same room together. For some participants, the clinic contrasted with the loneliness felt outside it. Birdie said “I feel included. I feel part of something that’s good.” She further described, “it’s the place, it’s the people, it’s what happens here is quite special and unique … it’s like [the clinic] has been an antidote to the loneliness.” Her reflection highlights how connection was experienced through social contact, but more so through a renewed sense of place and value.
Care partners also described the clinic as supporting connection to life. Erica said the clinic created moments of familiarity, “… a bit like almost a glimpse of the person without the disease,” and explained connection with others enabled the person she supports to feel “still part of what’s going on in the world.” Mabel said, “I think she feels valued, too, coming here… she feels ‘heard’.” For Sue, she felt relieved “he’s got somewhere to go to and do something.” Robbo and Mabel identified the social aspect as one of the most important elements, and Robyn described the clinic as “a positive, and a social thing for him as well.”
Feeling truly known, respected, and connected came through ordinary and repeated acts of being listened to, recognised, included, and valued. These actions affirmed identity and contributed to a sense of continued place in the world for people with dementia. The clinic’s social group model fostered personhood through connection and belonging.
Meaningful Engagement Through Accessible Challenge and Play
(Linked with capabilities: sense, imagination and thought; play; bodily health)
Participants described the clinic activities as enjoyable and stimulating. Puzzles, games, craft, art, exercise, and humour created opportunities for play and engagement that were not experienced as tokenistic. Rosie shared, “Yes, we get some laughs and everything, yes,” and Smokey stated, “I’m really enjoying [the clinic] and mixing the exercise in with it … thoroughly enjoying myself.” Birdie described puzzles as calming: “There’s lots of feelings. Like great ones, really positive ones … I think doing the puzzles makes me feel calm… I enjoy those.” Dave said humour was a source of enjoyment and connection for him; “Joking to those things and that, that sort of thing. I just laugh at them.” Ken valued the exercise and cognitive stimulation components: “I look forward to doing the physical exercises and also the mental – yes … it’s very enjoyable.” These accounts suggest play and stimulation are important to wellbeing and dignity.
Activities also supported creativity, imagination, intellectual curiosity, and cognitive engagement when they were accessible and matched to participants’ interests. Rosie described feeling “good” about painting, and said the clinic was something she looked forward to: “I love it … it’s beautiful.” When engaging in Lego® model building, Al chose emotional touchpoint cards Encouraged, Comfortable, and Respected, indicating that creative activity affirmed self-worth. Jeff liked the intellectual engagement, stating, “There’s always something to learn, right?” Participants also recognised when activities were not accessible or scaffolded appropriately. Dave explained, “I don’t like it when people just give people a whole load of things … that they need to do this and work it out.” His account highlights that challenge was meaningful when it was accessible and not overwhelming.
Meaningful engagement also supported physical, emotional, and psychological wellbeing. Birdie described feeling “energised… physically and mentally,” and stated, “there’s enjoyment and it’s safe … I feel like I’ve been challenged.” Jeff said, “I’m proud that I can come here and I’m hopeful that something comes out of it,” and Smokey chose the emotional touchpoint cards Proud and Confident, elaborating, “it feels good that – achieving something.” These emotions suggest that challenge and achievement were important because they led participants to experience themselves as capable. The exercise component was also valued; Ken said, “It’s good for the brain,” while Rosie stated, “I’d like to do it more,” and laughed. Additionally, Birdie described, “I’m definitely more connected to my body from the exercise,” and “I feel motivated to do more exercise.”
Care partners observed similar effects. Robyn shared “He loves his table tennis and he’s happy to take his reading glasses, whereas normally he wouldn’t.” Mabel stated, “She really just wants to get in there.” Alexandra described how relational connectedness enabled participation: “I’ve tried doing crafty things with him and he’s not interested, but he does do them with you.” Mabel described the person she supports rediscovering painting; “I think [painting] makes her feel a little bit of power.” Erica thought the clinic enabled people with dementia to: “generate activity and feeling and emotions in other people,” and Robbo observed improvements in posture, grip strength, and fewer falls, while also stating: “She’s much happier.”
Meaningful engagement was created through activities that were enjoyable and appropriately challenging. Activities were neither infantilising, nor overwhelming, and were adapted to participants’ interest, capabilities, and goals. This approach in the clinic supported people with dementia to experience creativity, bodily confidence, achievement, pleasure, and contribution.
Discussion
This study explored how participation in a nurse practitioner-led, community-based, multicomponent memory clinic supported people with dementia to live a life of dignity. Using Nussbaum’s (2011) Central Human Capabilities as an interpretive lens, the findings show dignity was supported through everyday care practices that enabled emotional safety, relational autonomy, social connection, meaningful engagement, and accessible challenge. In addition to providing non-pharmacological activities, the clinic created relational and emotional conditions through which people with dementia could feel known, make choices, express emotion, participate, and experience themselves as capable.
Dignity Was Supported Through Emotional Safety, Recognition, and Meaningful Participation
A key finding was that people with dementia valued feeling safe, known, and connected within the clinic. Participants described comfort and reassurance through familiar routines, recognition on arrival, respectful interactions, and relationships with group members and staff. These experiences are important because post-diagnostic care is often framed through information, diagnosis, and treatment, and the emotional and relational dimensions of living with dementia are not addressed (Pavković et al., 2024, 2025). In this study, feelings of safety and comfort were central to how participants experienced the clinic as a place where participation was possible. The findings extend understandings of safety in dementia care. Through Nussbaum’s (2011) capabilities, bodily integrity can be understood to include the conditions that enable people to participate and express themselves without fear or humiliation. Participants’ accounts of feeling safe, comfortable, reassured, and able to express frustration or grief suggest that emotional safety supported capability. This support was particularly evident in activities where changing abilities were noticed by participants, and support was provided so emotions such as frustration and grief could be expressed, without being treated as failure.
Participants described autonomy as relational and practical. Choice and practical reason were evident in everyday acts such as preparing to attend, choosing activities, adjusting expectations, deciding when to participate with the group, and continuing participation because the clinic felt worthwhile. These findings align with relational understandings of autonomy, where agency is enabled through trusted relationships and practical support and not always in isolated and independent ways (Dewing, 2008; Jacobs et al., 2017). For people living with dementia, autonomy may be expressed through perceived small, situated choices that can be easily overlooked. The clinic supported practical reason and control over one’s environment by adapting activities to changing capabilities, interests, and goals.
Feeling known and connected also affirmed identity and personhood. Participants valued being recognised as persons with continuing interests, contributions, relationships, humour, and preferences. These findings challenge deficit-based dementia discourse by showing how people continued to learn, create, and contribute within a relational, non-pharmacological model of care. Similar recent evaluations of multicomponent post-diagnostic dementia care programs report that group-based participation can enhance confidence, social connection, and program engagement for people with dementia living in the community (D’Cunha et al., 2025). Participant accounts in this study add to this evidence by highlighting how emotional safety, recognition, and belonging can enable dignity in post-diagnostic care.
Meaningful engagement was also central to participants’ experiences. Cognitive stimulation, creative activities, physical exercise, humour, and play were valued when they were accessible and not infantilising. Participants’ emotions of enjoyment, pride, confidence, calm, and motivation suggest that activities created opportunities to experience their own capability. These findings support evidence for social and non-pharmacological approaches, including cognitive stimulation and multicomponent programs, in promoting wellbeing, mood, and quality of life for people with dementia (D’Cunha et al., 2025; Desai et al., 2024; Woods et al., 2023). In this study, accessible challenge was important to nurture strengths and enable achievement so that dignity is upheld.
Participants wanted what all people need: to know and be known by others. Yet people with dementia continue to experience stigma, discrimination, and exclusion in society (Department of Health and Aged Care, 2024; WHO, 2025). Recent work by Pavković et al. (2025) highlights that after diagnosis, people and care partners often receive empathetic communication but overwhelming or generic information, uncertain pathways, and prefer a single trusted contact to guide them through post-diagnostic support. The clinic responded to this need by centring relational and emotional connection, not only cognitive or functional support.
Nurse Practitioner-Led Care Enabled Continuity and Relational Knowledge
The nurse practitioner-led model in this study offered more than a program of activities. The clinic combined initial assessment, care coordination, review, referral, individualised activity programs, and care partner support. These elements enabled the clinic team to know participants over time and respond to changing capabilities, goals, preferences, and emotional responses. This approach is important in dementia care, where needs are evolving and post-diagnosis support pathways can be fragmented or uncertain (Naismith et al., 2022; Pavković et al., 2024, 2025).
Participants’ experiences in this study suggest that continuity and relational knowledge were important in post-diagnostic dementia care. While many other memory support or cognitive stimulation therapy programs operate within predetermined program durations (D’Cunha et al., 2025; Jeon et al., 2025; Woods et al., 2023), the clinic in this study was able to offer ongoing programs for participants. The ability to return to a familiar place, be recognised by familiar people, and participate in activities adapted to individual needs supported feelings of safety and belonging for people with dementia. Continuity is known to support quality of life and wellbeing in dementia care (Department of Health and Aged Care, 2024; Pavković et al., 2025). Although the clinic was offered on an ongoing basis, some participants’ frustration with enrolment occurring in successive eight-week blocks suggests that uncertainty about continued access to meaningful post-diagnostic care can influence their sense of autonomy, control over one’s environment, and dignity.
Nurse-led multidisciplinary care models have demonstrated value in improving access, continuity, and person-centred care across health contexts, as well as being sound economic investments (Australian College of Nursing, 2024; Luck & Doucet, 2021; Stewart et al., 2024; Terry et al., 2024). However, evidence specific to nurse practitioner-led dementia care remains limited (Luck & Doucet, 2021). This study contributes qualitative evidence from people with dementia and care partners about how a nurse practitioner-led multidisciplinary dementia care model may support dignity in practice. The findings suggest the value of nurse practitioner-led dementia care is in the clinical expertise, and also in the relational continuity, emotional safety, individualised and capability matched activities, and care partner support.
Strengths and Limitations
A strength of this study is the privileging of accounts from people living with dementia, supported by an interview method that enables emotional expression and accommodates communication and cognitive changes. The inclusion of care partners provided complementary perspectives. The use of Nussbaum’s (2011) Central Human Capabilities offered a coherent theoretical framework for interpreting dignity, capability, and flourishing in post-diagnostic dementia care. Additionally, the methodological congruence, transparent reporting, and reflexive team analysis promotes the credibility and overall trustworthiness of the study (Guba & Lincoln, 1989).
This study was conducted in a single nurse practitioner-led clinic in regional Australia, and findings may not be transferable to all dementia care settings. Participants had attended the clinic for at least six months, and therefore the study reflects experiences of people who had remained engaged with the service over time. Participant accounts were largely positive, which may reflect the value participants placed on the clinic, but may also relate to existing relationships with the interviewers. Some interviews included both the person with dementia and their care partner, which may have shaped what was shared. However, participant choice about who was present in the interview was prioritised in the person-centred approach to the study. Finally, participant characteristics were not reported which may limit contextual detail.
Implications for Policy and Practice
This study provides evidence for nurse practitioner-led, community-based dementia care that complements biomedical models through relational, non-pharmacological, strengths-based approaches. In practice, the findings suggest that post-diagnostic care should attend to emotional safety, routine recognition, supported choice, accessible challenge, and opportunities for contribution and play. Emotional expressions should be understood as meaningful information about how people experience care, including whether activities feel safe, overwhelming, grief-inducing, enjoyable, or affirming.
The findings also have implications for service design and funding. The clinic aligned with national and international priorities for flexible, multidisciplinary, community-based dementia care that supports autonomy, wellbeing, inclusion, and care partners (Department of Health and Aged Care, 2024; Low et al., 2021; World Health Organization, 2025). However, supporting a model of care such as the one described in this study requires funding structures that recognise nurse practitioner-led coordination, cognitive stimulation, exercise, creative engagement, and care partner support, as important components of post-diagnostic dementia care. Investment in nurse-led models of multidisciplinary dementia care may help address current service gaps by enhancing continuity, accessibility, and person-centred practice for people living with dementia in the community.
Recommendations for Further Research
Nussbaum’s (2011) Central Human Capabilities show promise for evaluating dementia care. Future research could explore how the framework might inform co-design, or be adapted into a practical evaluative tool or set of indicators. Additionally, while most capabilities were strongly reflected in this study, the capability of other species was not; future research could explore if connection with animals and nature enables flourishing for people with dementia.
Future research is needed into the cost and economic value of nurse-led, multidisciplinary dementia care. Evidence of the cost-effectiveness and efficiency of nurse-led models is needed as calls for dementia care reform increase. This research could include how nurse-led models impact hospital admissions, transitions to residential aged care, and care partner wellbeing. Research is also needed into the emotional and relational dimensions of dementia care identified in this study, including how relational autonomy is created, navigated, and practiced by healthcare workers and people living with dementia. Additional studies of longer-term non-pharmacological dementia care programs are needed.
Conclusion
This study challenges dominant deficit and biomedical models of dementia care by examining an innovative community-based, multicomponent, nurse practitioner-led dementia clinic. The findings demonstrate that when post-diagnostic care models are built on emotional safety and relational autonomy, people with dementia are supported to live lives they value. A capabilities approach makes visible practices that support dignity and flourishing beyond narrow deficit-based views of dementia.
Footnotes
Acknowledgements
The authors extend our whole-hearted gratitude to the people living with dementia and their care partners who shared their time, stories, and experiences as part of this research. Your openness and generosity have made this work meaningful, and your contributions will help shape future conversations and care models for post-diagnostic dementia care around the world. This study was supported in part by a 2024 seed grant from University of Wollongong Advancement and Equity Grant Scheme for Research (AEGiS). Additionally, the Enhance Memory Clinic would not have been possible without the generous philanthropic donation made to the Illawarra Medical Research Institute and the University of Wollongong.
ORCID iDs
Ethical Considerations
This study involved research with human participants. Ethical approval for this research was obtained from the University of Wollongong Human Research Ethics Committee prior to commencing participant recruitment and information collection (Approval Number 2022/082).
Consent to Participate
All participants provided informed written consent prior to their participation in the study. Research involving people with dementia raises specific ethical considerations regarding capacity and consent. This study utilised Dewing’s (2007, ![]() process consent model, viewing decision capacity as relational, contextual, and changeable over time. Consent was an ongoing ethical practice, with verbal consent obtained prior to interview commencement and interviewers monitoring assent, dissent, or signs of discomfort in participants.
process consent model, viewing decision capacity as relational, contextual, and changeable over time. Consent was an ongoing ethical practice, with verbal consent obtained prior to interview commencement and interviewers monitoring assent, dissent, or signs of discomfort in participants.
Consent for Publication
No identifying information from participants is included in the manuscript. To protect confidentiality and personhood, participants chose pseudonyms for reporting and publications related to this study. Additionally, participant characteristics (such as age, gender, and dementia type) have not been included for risk of re-identification and uphold confidentiality. These characteristics were also not relevant to the aim of the study and did not meaningfully contribute to participants’ experiences.
Authors Contribution
All authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship, have approved the final manuscript, and agree to be accountable for all aspects of the work. CRediT (Contribution Roles Taxonomy) author statement; Kelly Marriott-Statham—conceptualisation; methodology; investigation; formal analysis; funding acquisition; project administration; supervision; visualisation; writing—original draft preparation; writing—review and editing. Asha Beattie: investigation; formal analysis; visualisation; writing—original draft preparation; writing—review and editing. Meg Kelly: investigation; formal analysis; writing—original draft preparation; writing—review and editing. Susie Seitaridis: project administration; writing—review and editing. Nathan D’Cunha: supervision; writing—review and editing. Luke Molloy: project administration; writing—review and editing. Wyatt Hampstead: project administration; writing—review and editing. Rebekkah Middleton: project administration; writing—review and editing. Amy Montgomery: conceptualisation; investigation; formal analysis; funding acquisition; project administration; supervision; writing—original draft preparation; writing—review and editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by a 2024 seed grant from University of Wollongong Advancement and Equity Grant Scheme for Research (AEGiS). Additionally, the Enhance Memory Clinic would not have been possible without the generous philanthropic donation made to the Illawarra Medical Research Institute and the University of Wollongong.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and analysed during the current study are not publicly available due to the sensitive and potentially identifiable nature of qualitative interview data involving people living with dementia and their care partners. Participants did not provide consent for full transcripts to be shared publicly and the ethical approvals governing this study prohibit open data release. De-identified data excerpts supporting the findings are included within the published article. Additional non-identifiable materials may be available from the corresponding author upon reasonable request, subject to ethical approval and in accordance with participant confidentiality requirements.