
Abstract
Patches Paediatrics is a specialised private multidisciplinary service in Western Australia (WA), offering a range of developmental diagnostic assessments such as foetal alcohol spectrum disorder (FASD). Many FASD assessments occur in children and youth who are engaged with the justice system in WA and the Northern Territory (NT). There are currently no studies outlining the types of clinical recommendations and management strategies made or implemented by clinicians for this clinical population within Australia. This study outlines therapeutic recommendations made as part of the youth justice FASD diagnostic process within Patches Paediatrics to ultimately refine recommendations to inform therapeutic strategies. This was a retrospective cross-sectional descriptive study of those aged 10 years to 17 years 11 months (N = 64) who were diagnosed with FASD within Patches Paediatrics; and referred from the youth justice system in WA and the NT between January 2017 and February 2019. Information on FASD recommendations was gathered by reviewing participants’ source documents, such as FASD diagnostic reports. ‘FASD recommendations’ categories were divided into subdomains: medical, mental health, developmental, lifestyle, future goals and others. In the various categories of recommendations, the most prominent were referral for National Disability Insurance Scheme (NDIS) funding (75%) followed by education support (67.2%), occupational therapy (56.3%), and drug and alcohol services (45.3%). Significant correlations between impaired neurocognitive domains and recommendations were also observed. Similarly, there were significant correlations between comorbidities and recommendations. Our study highlighted gaps in recommendations for those with comorbid attention-deficit/hyperactivity disorder (ADHD), rural communities and access to NDIS, therapeutic rehabilitation programmes as well as community work programmes. Other gaps included making adequate recommendations for speech/language therapy, education support, life skills advice and staff/clinician education. This study was the first to describe therapeutic recommendations for the youth cohort assessed by Patches Paediatrics in WA and the NT. It also showed significant correlations between the neurocognitive/comorbidity profile and clinical recommendations. This highlights areas within the recommendations that can be individualised as well as ways to improve community integration. A discussion of limitations and suggestions for future research is also provided.
Keywords
Highlights
Youth justice assessments at Patches Paediatrics in WA and the NT
Fetal alcohol spectrum disorder therapeutic recommendations in youth justice
Findings highlight recommendations need to be location specific and culturally appropriate
Forms the basis of future research avenues for establishing clinical guidelines
Introduction
The term foetal alcohol syndrome was first used in 1973 to describe children with poor prenatal care and/or growth and characteristic facial features who were born to mothers who were ‘alcohol dependent’ (Jones and Smith, 1973). It was not until 2000, that foetal alcohol spectrum disorder (FASD) was coined after recognition that alcohol exposure in utero results in neurodevelopmental problems with or without facial/physical features (Sokol et al., 2003). Currently to be diagnosed with FASD within Australia an ‘individual must have prenatal alcohol exposure (PAE) and severe neurodevelopmental impairment in at least three of ten specified domains of the central nervous system structure or function’ (Bower and Elliot; On behalf of the Steering Group, 2016). The Australian Guide to the Diagnosis of FASD categorises this into two diagnostic entities – FASD with three sentinel facial features and FASD without three sentinel facial features (Bower and Elliot; On behalf of the Steering Group, 2016).
Patches Paediatrics is a community-based multidisciplinary team, offering child development, disability, therapy and early intervention services in many locations including Western Australia (WA) and the Northern Territory (NT). The Patches Paediatrics team specialise in the diagnosis and therapy management of children and adolescents with FASD among other developmental concerns. The cohort that are referred receive assessments for FASD to aid in justice proceedings and management. Connor et al. (2020) described the demographic, neurocognitive and comorbidity profile of the first 199 individuals who received a FASD diagnosis in Patches Paediatrics clinics. This study highlighted the importance of how understanding the nature of neurodevelopmental impairments further facilitates both the diagnostic process and providing targeted therapy and management strategies. In the community, Reid et al. (2017) assessed 37 children between 2014 and 2015 as part of the first Australian public FASD diagnostic service. It was found that 84 per cent had a comorbid diagnosis, in particular: 61 per cent attention-deficit/hyperactivity disorder (ADHD) and a majority had no significant facial features.
The Australian Institute of Health and Welfare report 2018–2019 describes the different kinds of supervision in the youth justice system. Unsentenced supervision can be either on bail (community-based) or remanded in custody (detention). Sentenced supervision can be parole/supervision release/ suspended detention (community-based) or sentenced to detention (detention) (Australian Institute of Health and Welfare (AIHW), 2020). On an average day in 2018–2019, those between 10 and 17 years of age, 28 per 10,000 in WA and 61 per 10,000 in the NT were in supervision. Out of this, 5 per 10,000 in WA and 14 per 10,000 in the NT were primarily in detention (remanded in custody or sentenced to detention) (AIHW, 2020). Banksia Hill Detention Centre (BHDC) is the only detention facility for children and young people aged 10–17 years (Commissioner for Children and Young People WA, 2020; Office of the Inspector of Custodial Services, 2018). Bower et al. (2018) was the first Australian study in any justice setting to estimate the prevalence of FASD in youth. This study was conducted in the BHDC cohort, which showed that 36 per cent of this cohort (13–17 years) had FASD. Of this, the majority had a severe impairment in the academic (86%), executive functioning (78%), attention (72%), language (69%) and memory (56%) domains. Approximately 42 per cent of those with FASD were assessed to have an impaired IQ score at or below 70. Research in rural communities shows impairment in similar domains (Fitzpatrick et al., 2017), keeping in line with international studies (May et al., 2013).
Comparing the prevalence of 36 per cent of the BHDC study with international studies, Pei et al. (2018) found that the prevalence of FASD varied significantly between studies. For example, a US study found that 60 per cent of both adults and adolescents had justice involvement, whereas Swedish studies showed that justice involvement was similar in proportion for those adults with or without FASD (Pei et al., 2018). Similarly, other studies varied from 11 to 23 per cent of youth justice involvement (Pei et al., 2018). This is supported by local research which explored the prevalence of FASD in Australia in comparison to international settings and found this to be difficult due to different diagnostic criteria and different study designs (Fitzpatrick et al., 2015).
Harvey (2019) describes various neurodevelopment domains and their assessment. Cognitive performance is a concept encompassing various domains of functioning ranging from basic sensory processes to more complex executive functioning (Harvey, 2019). Executive functions are higher-order cognitive functions required for adaptive goal-directed behaviours such as those skills required for planning, reasoning and problem-solving (Harvey, 2019; Salehinejad et al., 2021). Motor skills are both fine motor abilities such as dexterity, speed, reaction time as well as global abilities requiring gross motor skills such as balance (Harvey, 2019). Adaptive functioning relates to activities of daily living that require conceptual skills (numbers, money, time), social skills (rules, laws, understanding motivation) and practical life skills (feeding, dressing) (Oakland and Daley, 2013). Affect regulation is the ability of an individual to modulate their emotional state to meet requirements of situations they are in (Harvey, 2019).
Due to impairments in one or multiple neurodevelopmental domains, young people with FASD have a range of difficulties that can impact and contribute to their involvement with the justice system (Bower et al., 2018). They have difficulties in understanding the concept of ‘cause and effect’, associating past experiences with current behaviours, which in turn leads to poor decision making. This means, these individuals have problems with employment, poor school engagement, substance abuse and engagement with the law (Barnert et al., 2016; Borschmann et al., 2020; Bower et al., 2018; Education and Health Standing Committee, 2012; Mutch, 2013; Reid et al., 2017). In the youth justice cohort, these difficulties have significant forensic implications. For example, not understanding why their behaviours were wrong, comprehending their legal rights or making possible incriminating statements and resisting arrest. They can demonstrate a lack of understanding about the need to testify, becoming aggressive due to sensory overload and the inability to organise thoughts or processing information in written language (Barnert et al., 2016; Borschmann et al., 2020; Mutch, 2013; Patel et al., 2020).
As such, Bower et al. (2018) emphasised that identifying reasons which contribute to offending behaviour is vital to understand their involvement within the justice system. They suggest recommendations need to involve a full comprehensive needs assessment and support planning – including a formal neurodevelopmental assessment for comorbid conditions. Identifying therapy recommendations are vital to the physical, mental, education, learning and family needs of this cohort to reduce offending behaviour (Bower and Elliott; On behalf of the Steering Group, 2016; Bower et al., 2018; Education and Health Standing Committee, 2012; Mutch, 2013). The outcome of such recommendation has the ability to influence their trial outcome and what support they will receive. Appropriate services are vital and include medical management of additional diagnosis, mental health follow-up, treatment of substance abuse, vocational training, life skills training, mentoring and advocacy (Education and Health Standing Committee, 2012; Golzari et al., 2006; Mutch, 2013; Patel et al., 2020).
The UN Convention on the Rights of Persons with Disabilities (UNCRPD) paragraph 28 states that Children with developmental delays or neurodevelopmental disorders or disabilities . . . should not be in the child justice system at all, even if they have reached the minimum age of criminal responsibility . . . If not automatically excluded, such children should be individually assessed. (Hughes et al., 2020a)
There are arguements that incarceration should be the last resort in children and rehabilitation frameworks are far more appropriate, particularly those with a trauma background (Brinkley-Rubinstein et al., 2020). However, more research is needed to optimise methods to increase the nature and efficacy of these programmes. One of the main reasons for this is the known high risks of physical and mental health harms associated with detention, especially if children are also in centres with adult detainees (Brinkley-Rubinstein et al., 2020). Other recommendations suggest the need for health assessment teams to be listed on the FASD Hub for consumers to actively access a potential list of clinicians/ service providers (Webster et al., 2020).
The Australian Institute of Health and Welfare (AIHW, 2020) reported that in 2018–2019, 38 per cent of Australian Aboriginal young people under supervision were first supervised when aged 10–13 years, compared with about 15 per cent of non-Australian Aboriginal young people. The Australian Aboriginal population is often over-represented in the justice system, and this group is most intensely researched population since the British settlement (Hamilton, 2020a). Alcohol use in pregnancy occurs in both Australian Aboriginal and non-Australian Aboriginal communities; however, certain communities especially those in rural/remote area have high alcohol consumptions (Fitzpatrick et al., 2015). In addition to this, there are complex, cultural, social, economic and behavioural reasons, which have led to Australian Aboriginals being over-represented in the youth justice system (Blagg et al., 2021; Blagg and Tulich, 2018; Bower et al., 2018; Hamilton, 2019; Hamilton et al., 2020c). Blagg et al. (2021) highlight the need for a ‘declonising’ approach, the importance of diversion, community-based cultural programmes and cultural training of custodial officers to support vulnerable youth who are in contact with the mainstream justice system, especially youth with FASD (Blagg et al., 2021). Given the limited number of health professionals who can diagnose FASD, there is a need to upskill allied health staff, paediatricians, Aboriginal Health Care providers and general practitioners (GP) especially in rural and remote areas, which are areas of need (Reid et al., 2020b; Webster et al., 2020). This is vital to be able to deliver NDIS and other clinical services, which need to be location specific and culturally appropriate, creating a challenge for target populations needing this service.
The best approach would be the placement of a multidisciplinary model of care focussing on neuropsychological approaches with FASD prevention, diagnosis and therapy (Fitzpatrick and Pestell, 2017). Research has indicated that the challenge lies in determining a standardised, collaborative response that lines with known international data and study protocols (Fitzpatrick and Pestell, 2017). It is recommended that following diagnosis, early intervention is vital and incorporating psychoeducation and support of patients as well as caregivers (Olson and Montague, 2011). A study in the United States developed a framework for therapy approaches that support the need for a strong patient- and family-centred approach (Bertrand, 2009). In particular, providing parent education/ training and teaching children specific skills and integration into existing models of care is vital for ongoing management by school, social services and mental health providers (Bertrand, 2009).
Blagg and Tulich (2018) documented the first study of providing diversionary strategies for youth with FASD in three Australian Aboriginal communities in the West Kimberley region of WA. They suggested the best approach was diversion into ‘owned and managed structures’ to offer a ‘secure environment’ and the need for a strong Australian Aboriginal community involvement (Blagg and Tulich, 2018). An appropriate model of therapy needs to engage the Indigenous population by understanding their cultural needs, way of life and connection with the land (Blagg et al., 2019). It was also recommended that an emphasis be placed on being aware of cultural factors that will influence implementation for FASD strategies internationally (Petrenko and Alto, 2017). The only way of doing so is to continue research based on evidence for FASD interventions specific to the area of need and in different regions within a country or in different countries. This will enable an educated decision, generate a mechanism of change and meet the needs of the given cohort the best (Petrenko and Alto, 2017). Furthermore, as discussed in Hamilton (2019) there appears to be a need for ongoing skills education for detention centre staff to manage those with FASD to provide consistent through-care (Blagg et al., 2021; Hamilton et al., 2019). A recent survey of custodial officers in the WA youth detention centres showed that they lacked the knowledge and training needed for caring both people with FASD and other neurodevelopmental impairments while in custody (Passmore et al., 2018a). Currently, Passmore et al. (2020) is the only study in Australia which outlines interventions for supporting detention officers in a local setting.
The forensic implications of a FASD diagnosis highlight the importance of an effective collaboration between health and justice professionals to enable a platform to provide greater opportunities for training, education and employment (Reid et al., 2020a). The Commissioner for Children and Young People in WA outlined a ‘toolkit’ for domains such as education, well-being, promoting rights and future opportunities for Australian Aboriginal children and young people in the youth justice cohort (Commissioner for Children and Young People WA, 2020). Currently, to our knowledge, there are no studies in WA or the NT that identify recommended therapy and management strategies by clinicians for FASD youth justice cohort. A national guideline for FASD recommendations specific for this cohort is also not available in Australia for community clinics, and this study hopes to inform such a guide.
Aims
For individuals diagnosed with FASD, and referred from the justice system in WA and the NT, within Patches Paediatrics clinics, we will aim to
I. Describe the demographic, neurocognitive and comorbidity profile of this cohort.
II. Describe the therapeutic recommendations made by categorising into the following domains: medical, development, mental health, lifestyle, future planning and others.
III. Describe associations between their neurocognitive profile and comorbidities with FASD recommendations.
Method
Sampling design
This study utilised a retrospective cross-sectional descriptive study design. Approximately 88 FASD assessments were conducted between January 2017 and February 2019 as referred from the justice system (this included both children and adults) at Patches Paediatrics. Participants were either on remand in the communities or in the detention centre. They were only included only if they received a FASD diagnosis according to the Australian FASD diagnostic criteria (Bower and Elliot; On behalf of the Steering Group, 2016). Of the 88 candidates, only 64 were aged between 10 years and 17 years 11 months and were included in this study to capture the paediatric and young adolescent profile relevant to the scope of this study.
Ethics
This study was approved by the Human Ethics Committee from the University of Western Australia and the Western Australian Aboriginal Health Ethics Committee (HREC Approval Number: 901).
Procedure
Electronic data were stored on a password protected client record management system within Patches Paediatrics that was only accessible by authorised personnel. A pre-existing database collected by Connor et al. (2020) was used to obtain information about demographics – including Accessibility and Remoteness Index of Australia (ARIA) and socioeconomic status (SES), neurocognitive profiles and comorbidities for each participant. Additional information related to FASD recommendations was added to this database, which incorporated a review of the FASD multidisciplinary diagnostic reports for each participant. The recommendations made from each Patches clinician in the report were categorised and described. Fidelity was maintained by utilising the same structured approach across all participants.
Statistical analysis
Data were analysed using SPSS-22. Descriptive statistics to determine demographic, neurocognitive and comorbidity profiles were generated. Those who did not have a recommendation were coded as ‘0’ in the database and there was no missing data. To analyse associations between neurocognitive impaired domains and recommendations – a series of chi-square tests were employed. The results were deemed significant if the p-value was less than 0.05. Similarly, chi-square analyses were conducted to investigate the relationship between comorbidities and recommendations. A Cramer’s V test was further conducted for those variables with statistical significance to assess the strength of this correlation. A value > 0.25 suggested a very strong correlation (Cohen, 1988).
Results
Demographic profile
In our study, the mean age was 14.7 years (SD 1.53, range 10–17), most were 13 years or above (n = 58, 90.6%), male (n = 52, 81.2%) and Australian Aboriginal (n = 54, 84.4%), the remainder being Caucasian (n = 10, 15.6%). A high proportion also had child protection involvement (n = 41, 64.1%). Participants were more commonly from major cities (n = 23, 35.9%) or very remote areas (n = 24, 37.5%). A histogram was generated to determine the cut-off for SES. The Index of Relative Socioeconomic Advantage and Disadvantage (IRSD) of 1–3 was classified as low SES and had just over half the participants (n = 33, 51.5%), IRSD of 4–7 was classified as medium SES (n = 22, 34.4%), while IRSD of 8–10 was classified as high SES (n = 9, 14.1%), as given in Table 1.
Demographics of individuals with FASD (N = 64).
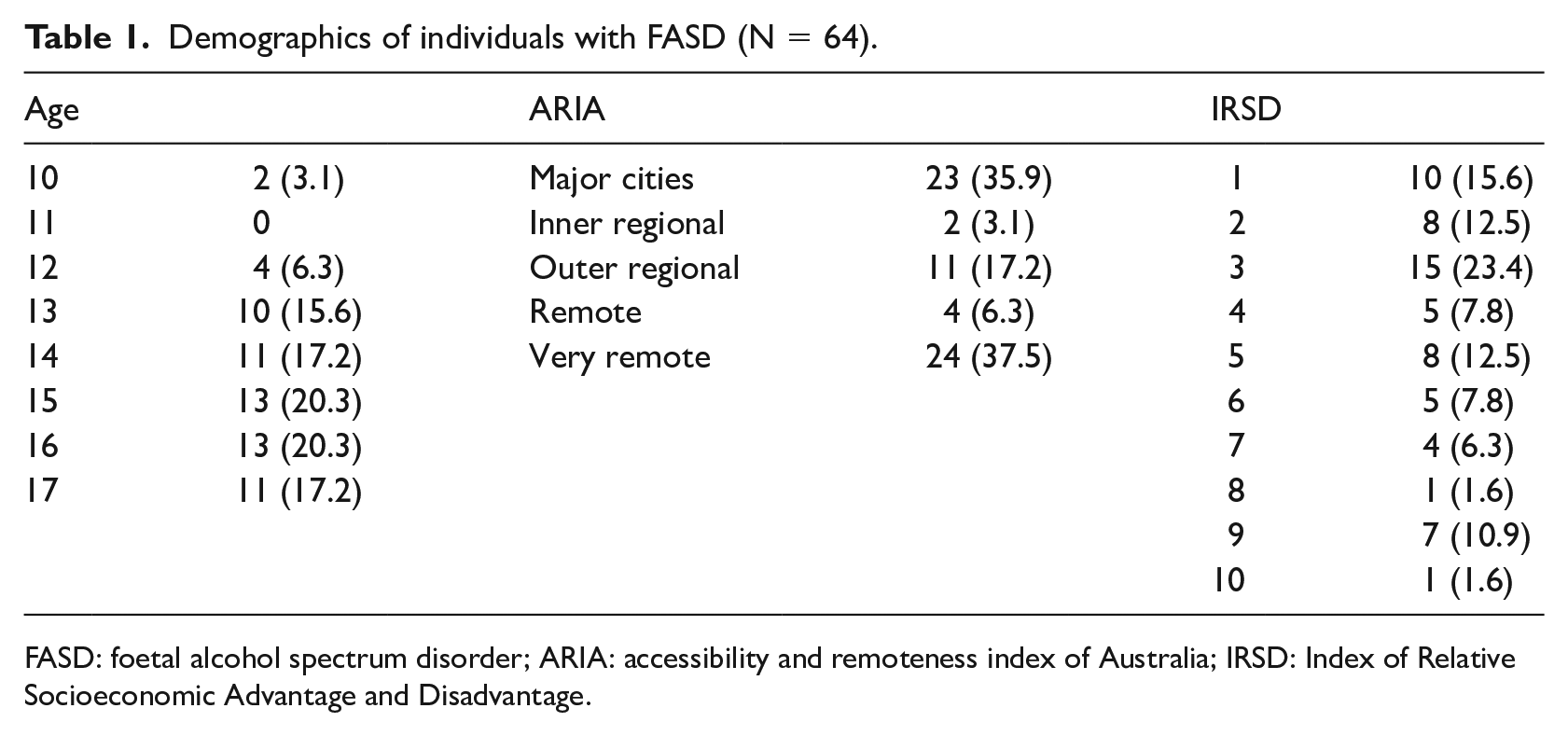
FASD: foetal alcohol spectrum disorder; ARIA: accessibility and remoteness index of Australia; IRSD: Index of Relative Socioeconomic Advantage and Disadvantage.
Neurocognitive profile and comorbidities
Most participants received a diagnosis of FASD with < 3 sentinel facial features (n = 59, 91.2%). There were challenges in obtaining information about prenatal alcohol consumption given most of the participants were in child protection or not living with family. Information was gathered from the case social worker, a parent directly (even if not currently under their care) or a known relative (older sibling, spouse or grandparent). Birth hospital records and other medical/health documents were also obtained where possible. In cases where this was difficult to ascertain, this was classified as ‘unknown’. However, as per the Australian FASD diagnostic guidelines, a child can still meet a diagnosis of FASD if they meet the neurodevelopmental criteria and have 3 sentinel facial features on medical examination (Bower and Elliott; On behalf of the Steering Group, 2016).
As seen in Table 2, executive functioning including impulse control and hyperactivity was the most impaired domain (n = 53, 82.8%). Those who were a ‘don’t know’ in having a comorbidity were counted as a ‘no’: executive functioning (n = 2), language (n = 11), memory (n = 7), academic achievement (n = 12), adaptive functioning (n = 6), attention (n = 4), cognition (n = 2), affect regulation (n = 10) and motor skills (n = 23). Most participants were impaired in at least four domains (n = 16, 25%) with only five (7.9%) having seven or eight impaired domains cumulatively (Figure 1). The comorbidities observed in individuals with FASD can be seen in Table 3 with sleep disturbance and ADHD being the most commonly observed comorbid conditions (n = 23, 35.9% each). Those with a ‘probable’ neurocognitive impairment were counted as a ‘no’: post-traumatic stress disorder (n = 8).
Impaired neurocognitive domains in individuals with FASD (N = 64).
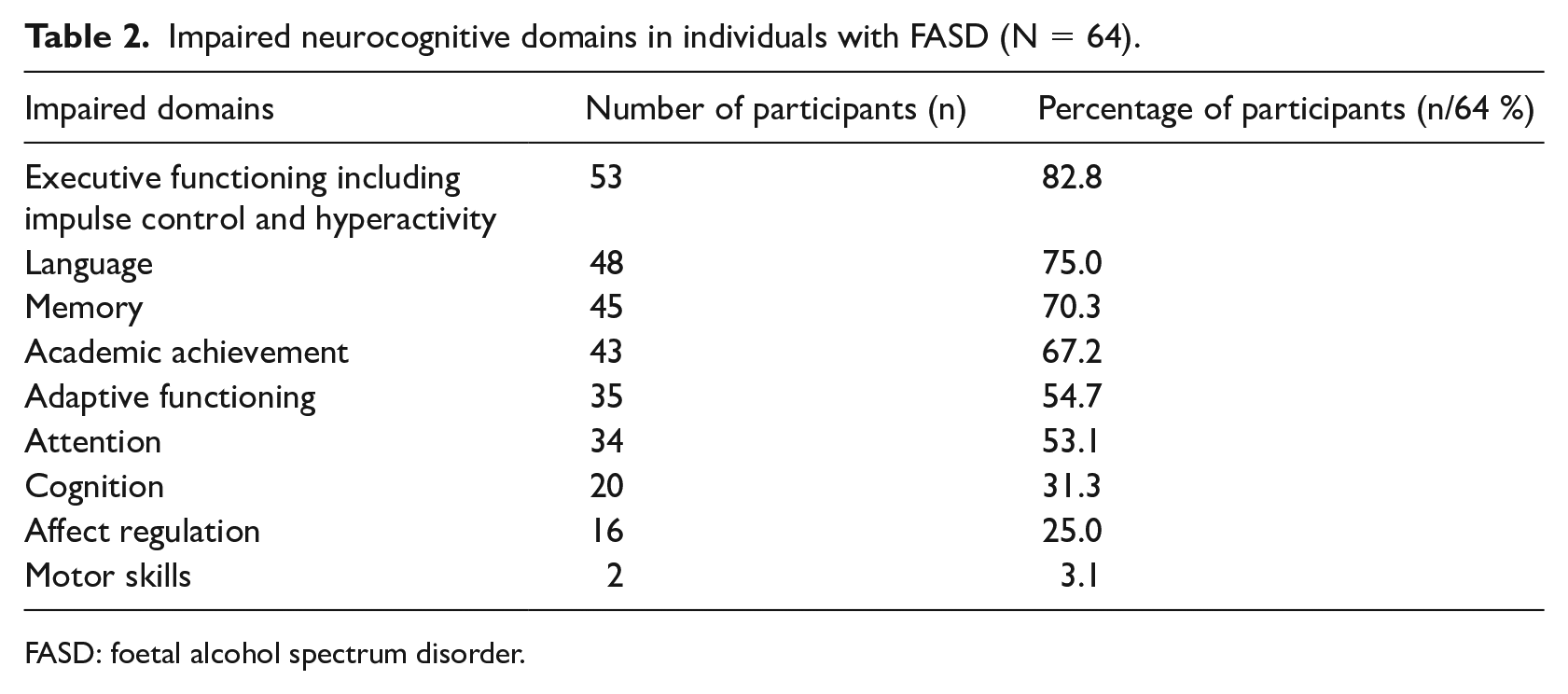
FASD: foetal alcohol spectrum disorder.
Comorbidities in individuals with FASD (N = 64).
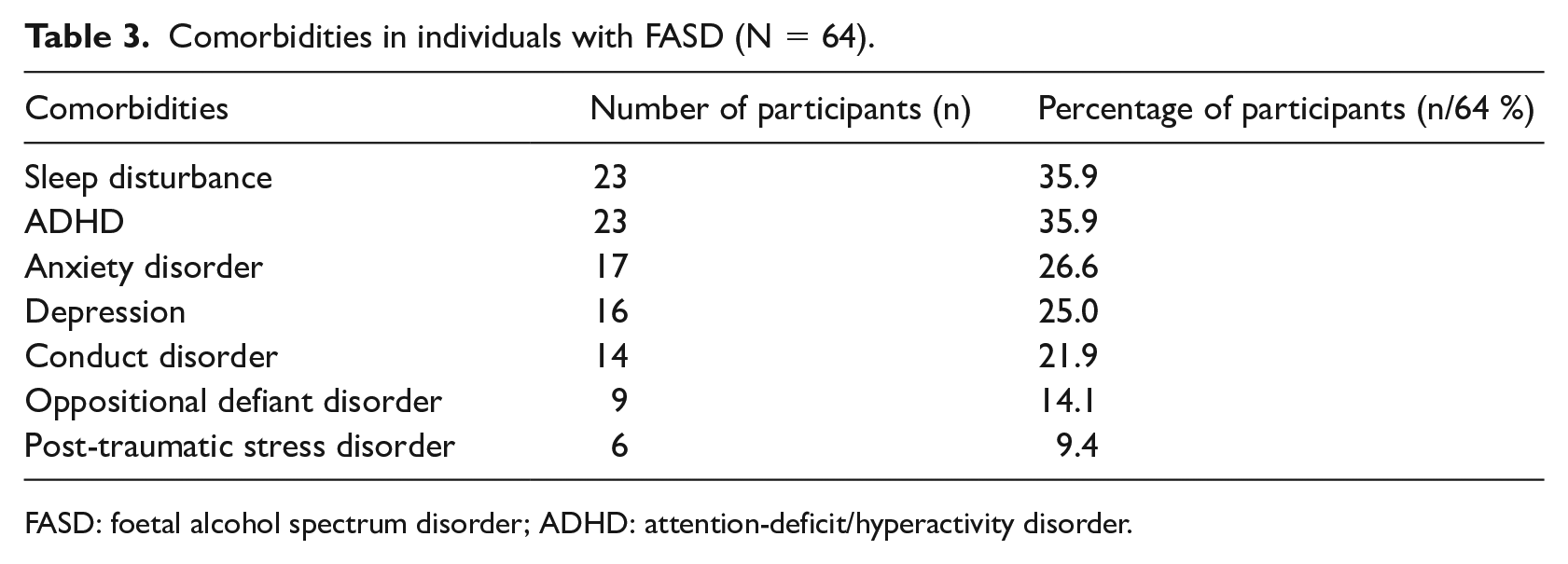
FASD: foetal alcohol spectrum disorder; ADHD: attention-deficit/hyperactivity disorder.
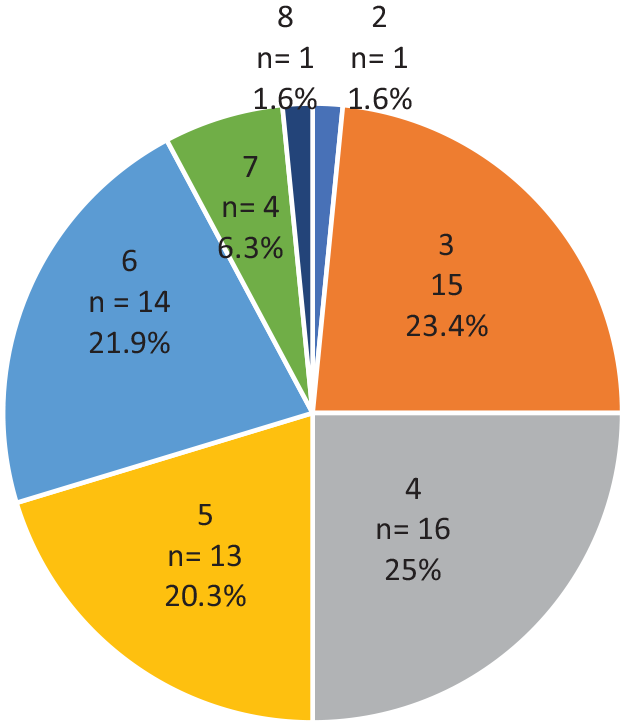
Number of impaired neurocognitive domains in individuals with FASD.
FASD recommendations
As outlined in Table 4, the most common recommendations in each category were: GP for management (n = 26, 40.6%), occupational therapy (OT) (n = 36, 56.3%), drug and alcohol services (n = 29, 45.3%), National Disability Insurance Scheme (NDIS) (n = 48, 75%) and educational support (n = 43, 67.2%). The ‘other’ category included recommendations that were less than 10 per cent and are listed in Table 4. Of these, the highest being for disability employment programme or an Aboriginal health worker (n = 6, 9.4% respectively). Recommendations for a ‘Psychiatrist’ also included Child and Adolescent Mental Health Service (CAMHS) referrals. The referral to the OT, specifically involved referring the participant to the ALERT programme for self-regulation, such as that offered by Patches Paediatrics. Recommendations for ‘Diversionary activities’ also involved recommendations to sports as a form of diversion therapy. ‘Family arrangements’ included recommending a change in family circumstances such as housing or relocation, future family planning, family carer support programme and care placement on release. ‘Sleep’ recommendations included referral for sleep apnoea testing as well as management strategies; and ‘Future sentencing’ recommendations included future community-based sentencing options or therapy/support options instead of detention.
FASD recommendations for individuals with FASD (N = 64).
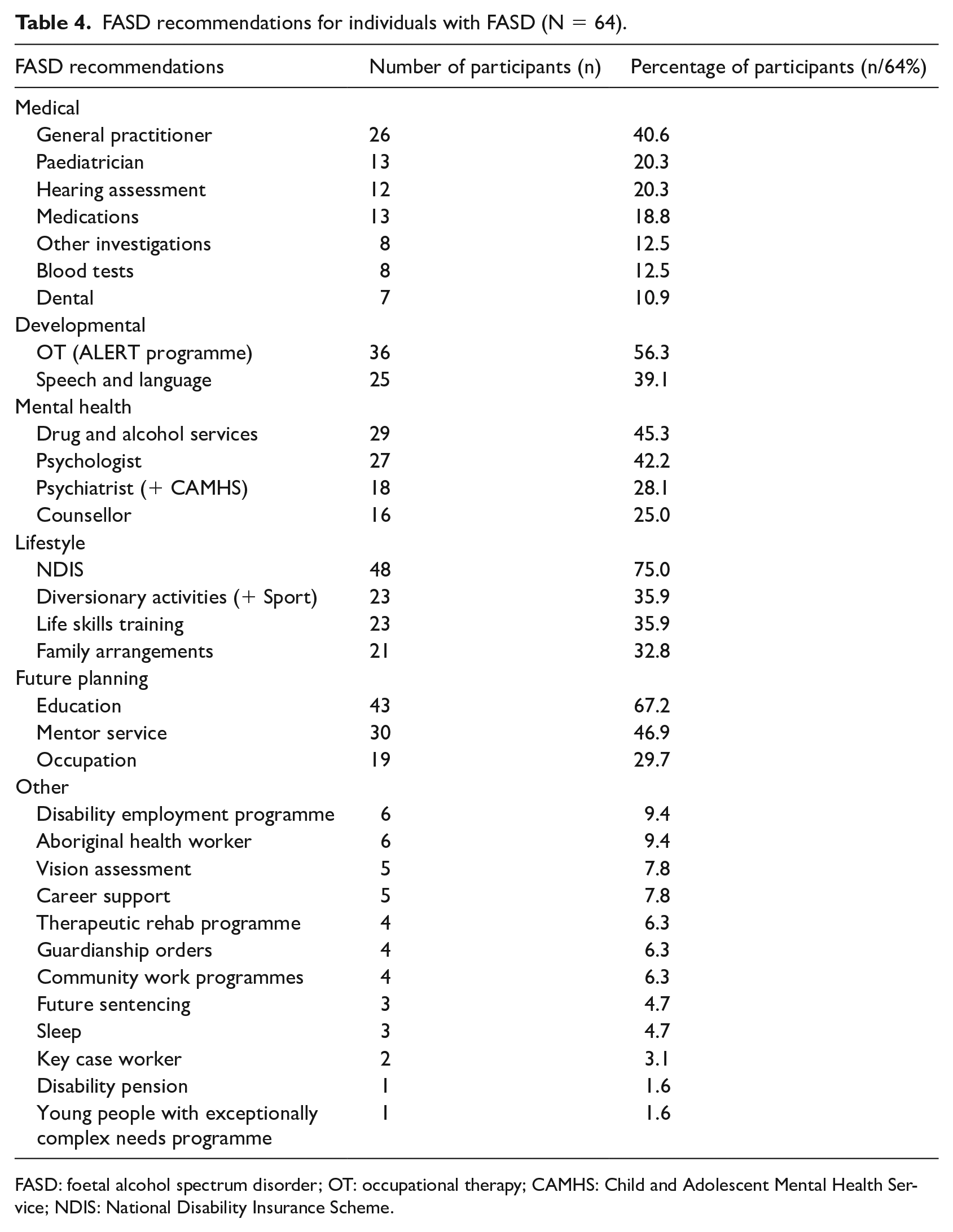
FASD: foetal alcohol spectrum disorder; OT: occupational therapy; CAMHS: Child and Adolescent Mental Health Service; NDIS: National Disability Insurance Scheme.
Domains impaired and its association with FASD recommendations
Significant and strong correlations were found between a range of impaired neurodevelopmental domains and specific clinical recommendations. This occurred between impairment in executive functioning and recommending family arrangements (χ2(2) = 5.704, p = 0.017, φC = 0.303); impairment in memory and recommending a speech/ language therapist (χ2(2) = 6.747, p = 0.009, φC = 0.344) as well as counselling services (χ2(2) = 4.491, p = 0.034, φC = 0.281). In addition, there was a significant association between language impairment and recommending NDIS (χ2(2) = 8.115, p = 0.004, φC = 0.392) as well as a key caseworker (χ2(2) = 4.003, p = 0.045, φC = 0.275). This was also the case between impairment in academic functioning and OT recommendations (χ2(2) = 4.077, p = 0.044, φC = 0.283) as well as to the disability employment programme (χ2(2) = 3.864, p = 0.049, φC = 0.275). A significant and strong correlation was also found between impairment in adaptive functioning and recommending a paediatrician (χ2(2) = 5.042, p = 0.025, φC = 0.298) as well as NDIS (χ2(2) = 5.168, p = 0.023, φC = 0.301). Similarly, significant correlations were found between impairment in attention and recommending medications (χ2(2) = 4.344, p = 0.037, φC = 0.269); as well as impairment in cognition and recommending a key caseworker (χ2(2) = 4.340, p = 0.037, φC = 0.265). Finally, significant correlations were found between impairment in affect regulation and recommending dental, (χ2(2) = 4.272, p = 0.039, φC = 0.284), OT (χ2(2) = 5.998, p = 0.014, φC = 0.336), drug and alcohol services (χ2(2) = 4.890, p = 0.027, φC = 0.304) as well as psychiatry (χ2(2) = 8.322, p = 0.004, φC = 0.396).
Comorbidities and its association with FASD recommendations
Further statistical analyses also highlighted significant correlations between certain comorbidities and particular FASD clinical recommendations. This was seen between sleep disturbance and recommending a paediatrician (χ2(2) = 4.644, p = 0.031, φC = 0.269), psychiatrist (χ2(2) = 4.187, p = 0.041, φC = 0.256), diversionary activities (χ2(2) = 4.591, p = 0.032, φC = 0.268) as well as sleep management (χ2(2) = 5.611, p = 0.018, φC = 0.296). This was also the case between ADHD and recommending family arrangements (χ2(2) = 4.323, p = 0.038, φC = 0.262); and between anxiety and recommending a psychiatrist (χ2(2) = 4.105, p = 0.045, φC = 0.253). Significant and strong correlations were also found between depression and recommending occupation support or advice (χ2(2) = 4.217, p = 0.040φ C = 0.257); between conduct disorder and recommending a psychologist (χ2(2) = 6.282, p = 0.012, φC = 0.313); and between oppositional defiant disorder and recommending education support (χ2(2) = 5.444, p = 0.020, φC = 0.292).
Discussion
This article is the first to highlight various management strategies recommended Patches Paediatrics for the management of FASD for youth on remand in the communities or in detention in WA and the NT. Our study identified that only 40.6 per cent and 20.3 per cent of this cohort had a recommendation for GP and paediatric review respectively, although, 35.9 per cent had comorbid ADHD as a diagnosis. The recommendations would be expected to be higher. However, it may be because 43.8 per cent of this group were in ‘remote’ or ‘very remote areas’. In remote parts of Australia, access to an ADHD diagnostic service is limited (Arefadib and Moore, 2017). It could also mean that they already have been linked with a GP or paediatrician. Current services already received by the participants were not assessed in this study. The Office of the Inspector of Custodial Services (2013) reported that Australian Aboriginal often described themselves as being ‘disengaged and disheartened’. Given the disproportionately high number of Aboriginal participants in our cohort, this may suggest that they have similar emotions, hence, engaging this cohort in traditional health care settings can also be a challenge (Barnert et al., 2016). Therefore, it may be useful to provide greater access to paediatricians or assess ways to change traditional health care settings for young people involved in the justice system.
Our study also showed that those with adaptive functioning impairments were significantly more likely to be referred to a paediatrician. Those with underlying developmental concerns may manifest as impairments in adaptive functioning, hence this recommendation is ideal for further assessment. Children with impaired adaptive functioning are likely having significant functional impairments in their daily life so will need regular review/medical management by a paediatrician. However, this is often accompanied by referrals to occupational therapists to support activities of daily living. Having ADHD had no significant association with any recommendation apart from ‘family arrangements’. It would be expected that multiple allied health and medical management recommendations would be made for those with comorbid ADHD or suspected ADHD during the assessment process.
Interestingly there was a significant and strong correlation between ‘medication’ recommendations (18.8%) and impairments in attention, even though, the medications recommended were not to manage ADHD. These medications were suggested to treat skin, ear infections, lice and nutritional supports. Patel et al. (2020) identified that 50 per cent of those with FASD in the social welfare system (n = 14) were recommended medication changes and all participants (n = 18) were recommended psychotherapeutic interventions. However, they also noted that majority had medications prior to referral that were usually managed by their paediatrician (Patel et al., 2020). In our study, however, no ADHD or psychotherapeutic medication recommendations were made. However, exploring current services accessed by the participants is important to assess whether there is a potential gap in recommended services for this cohort. It could also suggest that participants were already on stimulants and managed by a medical specialist. As suggested by Borschmann et al. (2020) lower SES groups may be more likely to be engaged in substance misuse, as such, prescription for stimulants for ADHD with infrequent follow up, is not ideal. Given that just over half of our cohort were from ISRD 1–3 (low SES) groups, this may have been the case.
Another apparent gap was that none of the FASD diagnostic reports had recommendations for genetic assessment to rule out other genetic conditions as the 12.5 per cent of blood tests recommended were for iron deficiency or HIV screening. This highlights the importance of medical specialists to always rule out any history of genetic abnormalities, or family history of facial dysmorphology, suggesting other genetic conditions (e.g. differential diagnoses of chromosomal abnormalities) when considering a FASD diagnosis. This may be due to the proportion of our participants being from remote/ very remote parts of WA and the NT where access to services is limited. A recent systematic review of global literature concluded that in general, adolescents in detention experience poorer health outcomes in both physical and mental health domains, including neurodevelopmental disabilities, sexually transmitted infections (STIs), blood-borne viruses (BBVs), reproductive and sexual health (Barnert et al., 2016; Borschmann et al., 2020; Golzari et al., 2006). Hence, blood tests which screen for STIs and BBVs need to be considered to optimise general health in the detention cohort with FASD.
Our study showed that the mean age was 14.7, 13 years or over (90.6%), and male (81.2%). Evidence shows that in this age group, reproductive and sexual health needs to be discussed (Barnert et al., 2016; Borschmann et al., 2020). In addition, there is limited consideration regarding the needs such as for young females with FASD in contact with the justice system within the research literature. We incorporated education around reproductive health under recommendation of ‘life skills training’ which 35.9 per cent received. In our study, there were no specific recommendations for reproductive or sexual health. Most of our ‘life skills training’ included managing finances and day-to-day activities.
Approximately 20.3 per cent had recommendations for a hearing review and 7.8 per cent vision assessment. It would be the scope of a subsequent project to address any pre-existing deficits with hearing or vision impairments. A recent meta-analysis showed that the pooled prevalence of hearing impairments was the most common comorbidity and approximately 129 times higher in individuals with FASD than in the general population of the United States (Popova et al., 2016). This is of importance, given current evidence, which shows hearing or vision impairment as part of FASD can affect court proceedings (Kippin et al., 2018; Mutch, 2013).
As expected, just over half of our cohort had a referral to OT (56.3%). With 82.8 per cent of our participants having impairments in executive functioning, including impulse control and hyperactivity, 54.7 per cent in adaptive function, 53.3 per cent in attention, 3.1 per cent with motor impairment and the number of recommendations in this category would be expected to be higher. There was a strong correlation with impairments in affect regulation and recommendation to an OT. Most reports reviewed in our study recommended the ALERT programme as part of an OT assessment (Wagner et al., 2020). It is important to acknowledge that, the ALERT programme may be specific to certain clinics, and elsewhere general OT services are recommended.
A large proportion of justice-involved youth struggle with language and communication disorders, which contribute to behaviour, learning and mental health outcomes (Kippin et al., 2018). This is very relevant given English may not be their first language for those who come from rural and remote backgrounds. In a study done by Kippin et al. (2018), one in two young people had language impairment associated with FASD in the justice cohort in WA. In our study, 39.1 per cent had recommendations to a speech/language therapist for further diagnostic assessment and in a few cases for therapy. Our findings also suggest that those with language impairments were significantly more likely to be referred to NDIS as well as a key caseworker. However, those who received a speech/ language recommendation were also significantly more likely to have memory impairments. This is surprising, given one would expect those with language impairments (75% in our study) to have recommendations for speech/language therapy, education or occupational/ career recommendations (Hamilton et al., 2020a; Kippin et al., 2018), and/or possibly involving the Aboriginal health team or mentor (Doak et al., 2019). It could also indicate that since these services are not available in remote areas, making recommendations that are not possible is not beneficial. Management can involve a speech pathologist early as well as working with local cultural and language advisors and accredited interpreters to provide this group with a better outcome (Kippin et al., 2018). Youth justice staff also were able to identify that engaging youth early in speech and language services is essential to help with the complexity of communication difficulties this population faces, as highlighted in our study (Snow et al., 2018). Another important point, as discussed by Hamilton et al. (2020b), is that this impairment may also be largely contributed by how the participants are assessed and the language used. Both Australian Aboriginal and non-Aboriginal participants communicated that using culturally specific language is very important. For example, rather than saying ‘confusion’, using phrases such as ‘when your head is feeling all mixed up’ helped participants be involved better in the assessment and management process (Hamilton et al., 2020c).
There is large impact of mental health on youth in detention (Anoshiravani, 2020; Barnert et al., 2016; Borschmann et al., 2020; Hughes et al., 2020b; Jirikowic et al., 2010; Office of the Inspector of Custodial Services, 2018). Although not all participants were in detention at time of the assessment or may not have been found guilty down the track, recent reports show that those in detention do not have access to a formalised mental health programme (Office of the Inspector of Custodial Services, 2018). This is of importance, given a high number of our cohort having had child protection involvement in the past, suggesting they had a background of trauma and disrupted parental attachment. In our cohort comorbid psychiatric diagnoses were common, with 26.6 per cent having anxiety, 25 per cent depression and 21.9 per cent conduct disorder. Approximately 42.2 per cent had recommendations to a psychologist, 28.1 per cent to psychiatry/CAMHS and 25 per cent to a counsellor. Given the prevalence of mental health problems, these recommendations would be expected to be higher. Of note, 45.3 per cent of this cohort were recommended to Drug and alcohol services due to concerns regarding ongoing substance use. Our results indicated that a psychiatric diagnosis was strongly correlated with mental health recommendations as well as occupation and educational support. Drug and alcohol services were strongly correlated with those with affect regulation difficulties. This is keeping with the literature, which indicates that those with FASD had concomitant health, developmental and psycho- pathological concerns (Jirikowic et al., 2010). In addition, it is known that mental health impairments are a youth criminogenic risk factor that is dynamic and potentially amenable to change through intervention (Hughes et al., 2020b). Childhood trauma and adversity is one such aspect that determines mental health and targeting this early on through screening and assessment has lasting effects on development and participation in society (Hughes et al., 2020b). Given 64.1 per cent of youth in our cohort had child protection involvement, this suggests they are a vulnerable group that is at higher risk of being involved in the justice system.
NDIS referrals were the highest recommendations from our study (75%). We found 25 per cent had impairments in four domains with a majority having impairments between three and six domains. As such, it is expected that a large number of participants would need allied health input, necessitating the need for NDIS funding. NDIS was also typically recommended for those with language and adaptive functioning impairment. It would be expected that NDIS services would also need to be recommended for those with other comorbid diagnoses and impaired neurocognitive domains, providing these impairments have a functional impact on the individual’s ability to navigate their life. It is important to note that regardless of which domains are impaired it is inevitable that clinicians would recommend NDIS support as a primary financial support system for those with FASD in WA and the NT.
All research suggests that the justice cohort is a highly vulnerable group, and a ‘gold-standard’ therapeutic approach would be multidisciplinary to address individual needs (Anoshiravani, 2020). It would also be interesting to see if more recommendations along with NDIS, were made for those with a greater number of impaired domains. Research indicates that lower SES groups were more likely to need help with available therapies (Hughes et al., 2020b), which can be looked into further in our cohort which had approximately 51.5 per cent from ISRD 1–3. It may also be that those from mid- to high SES families are already receiving interventions, which was not explored in our study. Australian Aboriginal children and youth were 45 times more likely to be in detention compared with non-Aboriginal counterparts (Commissioner for Children and Young People WA, 2020). Approximately 9.4 per cent of the cohort had recommendations for an Aboriginal health care worker to assist with community integration and provide cultural support. Given a large rural/remote representation (nearly 74%), it would be expected for this number to be higher or it is possible that participants were already receiving appropriate cultural support. It could also be possible that the GP in such communities or the Aboriginal health care team were serving this role. In addition, our study found that 46.7 per cent had a recommendation for a mentor. Perhaps in rural/remote communities, the mentor, Youth Justice Officer (YJO), community elder or member of the Aboriginal health care team may act as an access point to engage participants in culturally appropriate activities as well as liaise with an NDIS caseworker. Given the rural representation, it is important to enable families to access disability services. Digital platforms such as social media or mobile devices in remote communities can provide access to knowledge and health care (Doak et al., 2019). Further research looking into a formal needs analysis of services that these families may be lacking is required.
Our study found that sleep recommendations such as testing for sleep apnoea or sleep mediation were made in only 4.7 per cent, but 35.9 per cent had comorbid sleep impairment. There was a significant relationship between sleep disturbance and recommendations for referral to a paediatrician, psychiatrist, diversionary activities and sleep management. While there is no direct research into sleep and youth with FASD who are involved in the justice system, research that has shown that youth who report sleeping 5 hours or less per night reported more violent behaviour than those who reported sleeping the recommended 8–10 hours per night (Clinkinbeard et al., 2011). It has also been noted that PAE can affect children with sleep problems (Inkelis and Thomas, 2018; Wengel et al., 2011). Children with FASD demonstrated lower than normal sleep efficiency, increased sleep arousal index (i.e. fragmented sleep) and they can meet criteria for sleep disorders as well as sleep apnoea (Chen et al., 2012; Goril et al., 2016; Inkelis and Thomas, 2018; Wengel et al., 2011).
Approximately 67.2 per cent had recommendations for education involvement and individualised assistance within the classroom. It would be interesting to identify if there was any existing school involvement such a school aide or individual education plan. While recommendations were made, there is a gap is the apparent lack of educational support provided to those with FASD in schools in WA. For example, unless they have an intellectual disability, they are for the most part ineligible for an aide or individualised assistance (Statewide Support Services, 2020). However, given our cohort is of a median age of 14.7, with a large portion from remote locations and lower SES backgrounds, it can also be argued that a community-based programme, therapeutic rehabilitation programme or occupation advice may be of more relevance given they have likely left school. Hamilton et al. (2020a) explored the hopes, relationships and educational experiences of 38 detained youth. Participants expressed a strong connection to ‘country and community’. This is in keeping with previous research from the same group which identified this as a ‘Recovery Capital’ incorporating – social capitals (family, social connections, trust), physical capitals (housing, employment, food), human capitals (aspirations, hope, access to resources) as well as cultural capitals (values and beliefs) to be important in improving well-being (Hamilton, 2019; Hamilton et al., 2020b). Stability was identified a major concern, especially those under care of the state or child protection. This affected their hopes and outlook into the future. It was proposed that in terms of FASD, it is necessary to introduce a concept of a ‘Justice Capital’ specific to those with neurodevelopmental deficits such as FASD. This focusses on ways to fairly engage with this cohort in detention facilities (Hamilton, 2019; Hamilton et al., 2020b).
In our study, recommendations for family arrangements (32.8%) included recommending a change in family circumstances, future family planning, family carer support programme and care placement on release. It has been found that barriers to making and acting on recommendations include other disabilities, parental age, employment status of caregivers, housing, financial costs of supports, availability of allied health and overloading families with recommendations (Doak et al., 2019). This needs to be kept in mind when creating therapeutic recommendations for FASD. There was a significant and strong relationship between recommending family arrangements (as described above) for those with a comorbid ADHD diagnosis and impairments in executive functioning. In this highly vulnerable cohort, it has been argued that providing for a structured and supportive environment to support a person’s cognitive functioning was the best chance to stay out of the justice environment (Freckelton, 2016). Freckelton (2016) argued that not making changes to the current family and community environments, which predisposed to antisocial behaviours, is detrimental.
Our study indicates that 29.7 per cent were provided with recommendations for occupational advice, with 9.4 per cent recommending a disability employment programme. Interestingly, there was a strong correlation between impairments in academic functioning and recommending a participant to a disability employment programme. It is of note that only 7.8 per cent were given recommendations for career support and 6.3 per cent provided recommendations for a therapeutic rehabilitation programme and community work programme, respectively. This suggests a potential gap in clinical recommendations provided, as past studies have found that Australian Aboriginal caregivers were able to identify that ongoing management needs to be focussed on family networks and community; whereas, non-Aboriginal caregivers, were interested in seeing how their children’s interactions with health systems and schools would vary (Hamilton et al., 2020c). Our study showed that diversionary activities were recommended in 35.9 per cent cases. With Australian Aboriginal communities, it has been recommended that it is best to involve all members and seek advice to ensure adequate follow up and funding for such a process, and involve methods to employ research staff who can look into ways to best involve the community (Symons et al., 2018). This can be achieved by a reliable mentor, substance abuse counselling, workplace programmes and providing a more supportive environment (Doak et al., 2019; Symons et al., 2018).
Another avenue to further explore from this study would be the preparedness of custodial officers and clinicians in managing FASD. Evidence shows that many officers who work with youth in the custodial workforce lacked specific knowledge of FASD (Passmore et al., 2018b). Equipping staff to deal with and support those with FASD while incarcerated or on remand in the community is required (Passmore et al., 2018a). Passmore et al. (2020), devised a ‘Reframe the Behaviour intervention’ for custodial officers as a method to increase knowledge and enable a better information sharing process. In addition to this, in 2006, only about 34 per cent of paediatricians (in a study of 1600) felt prepared to case manage individuals with FASD (Gahagan et al., 2006). Less than 20 per cent of paediatricians knew all the features in diagnosing FASD and a large proportion agreed that prevention is the way forward in particular, asking women about alcohol intake during pregnancy (Payne et al., 2011). Educating the medical and allied health community is hence vital, as well as providing tools to aid case management and also recommendations to this complex condition.
Our results highlight the importance that ongoing management efforts are needed to address the health and social determinants of youth detention (Barnert et al., 2016; Borschmann et al., 2020; Golzari et al., 2006). It is vital to explore the applicability of recommendations to different areas of remoteness and SES groups, working alongside both families and the individual with FASD. In summary, our study was able to identify potential gaps in recommended services for this cohort. For example, additional recommendations for those with comorbid ADHD, a baseline genetic evaluation to rule out other suspected genetic conditions and adequate sleep management. It also highlighted gaps in recommending therapeutic rehabilitation programmes, community work programmes, speech/language therapies, life skills support and education support for those with FASD. In addition, exploring methods to make recommendations (including NDIS services) accessible, feasible and culturally appropriate to rural or Australian Aboriginal communities is necessary. Finally, educating staff in the justice system involved in care, assessment and ongoing community engagement for our cohort.
Limitations
Of note is the small sample size and short time frame of data collection, which limits definitive conclusions of our results. Over the last year, the NDIS scheme has changed considerably, with new community centres and organisations offering services to clients. Consequently, some of the earlier clinical reports from 2017 reviewed in this study were unable to capture these data. Pre-existing medication regimes as well as community, welfare or education resources already being accessed by the individuals were not known during this study. As such, it could be that recommendations were not made, as the patient already had access to these resources (particularly if linked to a paediatrician or psychiatrist with pre-existing ADHD). Hence, the number and types of recommendations reported in the current study could be an underestimate. Also, for those in rural or remote areas, they may already be accessing appropriate cultural support, which we did not look at. In addition, it is important to acknowledge that clinicians have their preferred recommendation suite and may vary with clinicians in other states of Australia or those working outside of Patches Paediatrics, for example, an ALERT programme may not be available elsewhere. Overall, it is also important to understand that the Patches Paediatrics team could only provide recommendations (rather than directly implementing them), as its main role in this setting was a FASD diagnostic service for justice system.
Conclusion
Our study has highlighted several important areas of recommendations for youth with FASD in the justice cohort. Overall, it shows that clinicians working in the field consider addressing comorbid diagnoses and recommending appropriate therapies relevant to these are important. Addressing academic, life skills training, therapeutic, diversionary activities and family arrangements is likely to be crucial to facilitate community reintegration. Supporting this population with NDIS (especially with psychology, OT or speech/language therapy) that is location specific and culturally relevant is also vital. Providing NDIS supports during diversionary processes pre-youth justice involvement can be considered a strategy as well, to hopefully prevent contact with the justice system in the first place. The ultimate goal would be the ability to have FASD recommendations, which can be built into established clinical guidelines and used along NDIS for funding for accessing therapy. This has the ability to reduce the involvement of youth in the justice system, by engaging them with appropriate supports. This could be incorporated into a private or public community developmental assessment centre, or as part of national/state guidelines focussing on state-specific resources. This article provides an initial outline, which identifies the need for such a larger study to occur.
Footnotes
Acknowledgements
The authors wish to acknowledge the Patches Paediatrics team and the UWA team involved in this research for their invaluable contributions to the work presented in this article.
Author contributions
Natasha K. Russell performed conceptualisation, data curation, formal analysis, methodology, software, resources, roles/writing – original draft and writing – review and editing; Kuen Yee Tan performed conceptualisation, data curation, formal analysis, methodology, resources and writing – review and editing; Carmela F. Pestell performed conceptualisation, methodology, resources, supervision and writing – review and editing; Sophia Connor performed data curation and writing – review and editing; James P. Fitzpatrick performed conceptualisation, methodology and supervision.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this article. They also declare the following financial interests/personal relationships, which may be considered as potential competing interests: Dr Fitzpatrick is Director of Patches Paediatrics, and Dr Fitzpatrick and Dr Pestell provide clinical services through Patches Paediatrics. Their input into analyses and objective interpretation of findings were not influenced by their employment.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.