
Abstract
Intimate partner violence (IPV) is closely associated with adverse sexual and reproductive health (SRH) outcomes; yet most IPV service agencies offer limited SRH-related support. This study used a constructivist grounded theory approach to explore the perspectives of survivors and service providers on how SRH can be identified and addressed within agency settings. Data was collected through semi-structured focus groups and interviews with 29 participants, including survivors and direct service providers at IPV agencies in the Southwestern United States. Using coding and constant comparative analysis, conceptual categories were identified that describe the experiences of participants in IPV agencies and in accessing SRH care. These categories were used to construct a phased SRH assessment framework that integrates screening and assessment at multiple stages of service engagement. Grounded in survivor and provider perspectives, this framework offers a trauma-informed, practice-based resource to guide IPV agencies in strengthening SRH services and expanding cross-sector collaboration.
Keywords
There is a well-established connection between women experiencing intimate partner violence (IPV) and negative sexual health outcomes (Campbell, 2002; Gielen et al., 2007; McGirr et al., 2020). Agencies serving IPV survivors have a unique opportunity to support women experiencing IPV by providing access to sexual and reproductive health (SRH) information and resources. Current data suggest that most IPV agencies offer few, if any, services to address SRH (Cavanaugh and Ward, 2021; McGirr et al., 2020). This study builds upon the findings from a previous qualitative study conducted by the authors that included interviewing IPV agency staff about their experiences discussing SRH topics with their clients. The results indicated that SRH conversations with clients were rare, but that staff were willing to engage in these conversations if provided with the training, support, and resources needed (Grace and Elias-Lambert, 2023).
Two major recommendations emerged from that data: (1) the need for an SRH assessment tool during intake and (2) enhanced sexual health education training for IPV service providers. This study utilized grounded theory methodology to explore experiences of IPV survivors and service providers. Through focus groups and interviews with IPV survivors and service providers, the authors explored how experiences with IPV impact women’s SRH decisions and how that can guide service providers in assessing SRH needs. The findings of this study propose a framework for screening and assessing the SRH needs of survivors within IPV agency settings. This framework was developed in collaboration with survivors and providers, thus incorporating the perspectives of those impacted directly in the research process.
Sexual and reproductive health and reproductive coercion in the context of IPV
Intimate partner violence (IPV) is defined as “any behavior within an intimate relationship that causes physical, sexual, or psychological harm” (World Health Organization, 2024) and is closely linked with reproductive coercion (RC), a form of abuse involving interference in reproductive decision-making (Bagwell-Gray et al., 2015; Grace and Anderson, 2018). RC includes behaviors such as pregnancy coercion, birth control sabotage, and controlling pregnancy outcomes (Miller et al., 2010, 2011; Moore et al., 2010).
RC has profound implications for IPV survivor SRH, contributing to increased risk for unintended pregnancies; sexually transmitted infections, including HIV; and other adverse outcomes (Anderson et al., 2017; Campbell, 2002; Coker, 2007; Gielen et al., 2007). Research suggests that 10% to 35% of IPV survivors experience some form of RC (Miller et al., 2010, 2011), underlining the urgency of identifying and responding to SRH-related harms within IPV relationships.
Gaps in SRH screening and provider readiness
Efforts to screen for RC and address the SRH needs of IPV survivors have primarily emerged from healthcare settings such as family planning clinics or women’s health centers (Decker et al., 2017; Miller et al., 2011; Moya et al., 2016; Ramachandran et al., 2013). Studies in these settings have piloted screening tools and trauma-informed scripts while also testing educational interventions to support providers (Decker et al., 2017; Miller et al., 2011). However, routine screening for RC and IPV remains uncommon (Burton and Caryle, 2015), and provider-related barriers, such as lack of time, training, and confidence, are well-documented. (Burton and Carlye, 2015; Ramachandaran et al., 2013; Stumbar et al., 2019).
These barriers are compounded by structural challenges such as survivors’ limited access to healthcare, especially in uninsured or underserved communities (O-Conner-Terry et al., 2022; Moya et al., 2016). To address these gaps, scholars have called for cross-sector collaboration, particularly between healthcare providers, social workers, and IPV advocates, to support effective, trauma-informed SRH responses (Park et al., 2016).
Survivor-centered and community-based approaches
Despite growing recognition of the link between IPV and SRH, limited research has explored how IPV service providers address SRH or how survivors experience SRH screening in non-clinical settings. Studies indicate that SRH conversations are rare in IPV service agencies, and few offer SRH-related support (Cavanaugh and Ward, 2021; McGirr et al., 2020; Rountree et al., 2008). Nonetheless, emerging evidence suggests that survivors prefer integrated services that address both IPV and SRH needs (Dichter et al., 2021).
Survivors’ narratives also point to a strong awareness of the health risks associated with abuse and highlight the need for trauma-informed care that validates their SRH concerns (Boyce et al., 2020; Grace et al., 2020; Wood et al., 2021). Survivors advocate for harm-reduction strategies, sexual safety planning, and provider sensitivity to the impacts of coercion and SRH decision-making (Bagwell-Gray et al., 2020; Park et al., 2016; Stockman et al., 2013). These findings underscore the value of survivor-informed tools and approaches that align with the lived experiences of IPV survivors.
Rationale for the current study
While there is growing recognition of the intersection between IPV and SRH, there remains a critical gap in practice: a survivor-informed, trauma-responsive process for assessing SRH needs within IPV contexts. This manuscript addresses that gap by proposing an SRH assessment framework designed for IPV survivors. Grounded in empirical research and survivor and service provider perspectives, this framework aims to strengthen provider capacity, enhance service delivery, and advance holistic, rights-based care for those impacted by IPV and RC.
Methods
This study utilized constructivist, grounded theory (GT) methodology to guide data collection and analysis. Although GT has traditionally been used to generate explanatory theories of underexplored phenomena, Charmaz (2006) emphasizes its broader utility in constructing conceptual frameworks and guiding intervention development through inductive analysis (Chun Tie et al., 2019; Sawyer and Brady, 2022). Aligned with this approach, the research team explored the SRH assessment experiences of survivors and service providers within IPV agency settings to develop a framework for addressing SRH needs.
Through focus groups and interviews with survivors, the researchers explored their experiences navigating SRH decisions and receiving services at IPV agencies. In separate focus groups with service providers, the researchers explored their experiences discussing SRH needs with clients and implementing assessment measures. Utilizing inductive analysis of the data, key concepts that emerged were used to interpret the findings and construct a proposed framework grounded in participant data. The resulting framework has the potential to inform practice-based interventions and services, representing an innovative application of GT not yet reflected in the literature.
Researcher reflexivity
Constructivist grounded theory emphasizes the interactive role of researchers with participants, highlighting the importance of reflexivity in shaping data collection and interpretation (Birks and Mill, 2015; Charmaz, 2006; Creswell and Poth, 2016). In alignment with this perspective, the research team engaged in reflexive practice and memoing to consider how their identities and positionalities may have influenced the research process. The first author is a PhD-level, licensed master social worker, who is a white, cisgender, heterosexual woman with nearly two decades of professional experience working with trauma survivors. While she has not personally experienced intimate partner violence (IPV), her perspective is shaped by her personal and professional experiences with survivors. The second author is a Middle Eastern, cisgender, heterosexual woman with over 20 years of professional experience in the gender-based violence prevention field. As a PhD-level licensed master social worker, she develops, implements, and evaluates programs to prevent gender-based violence. While she has not personally experienced IPV, her perspective is shaped by her professional experiences collaborating with survivors, service providers, and other community members working to prevent gender-based violence.
Sample
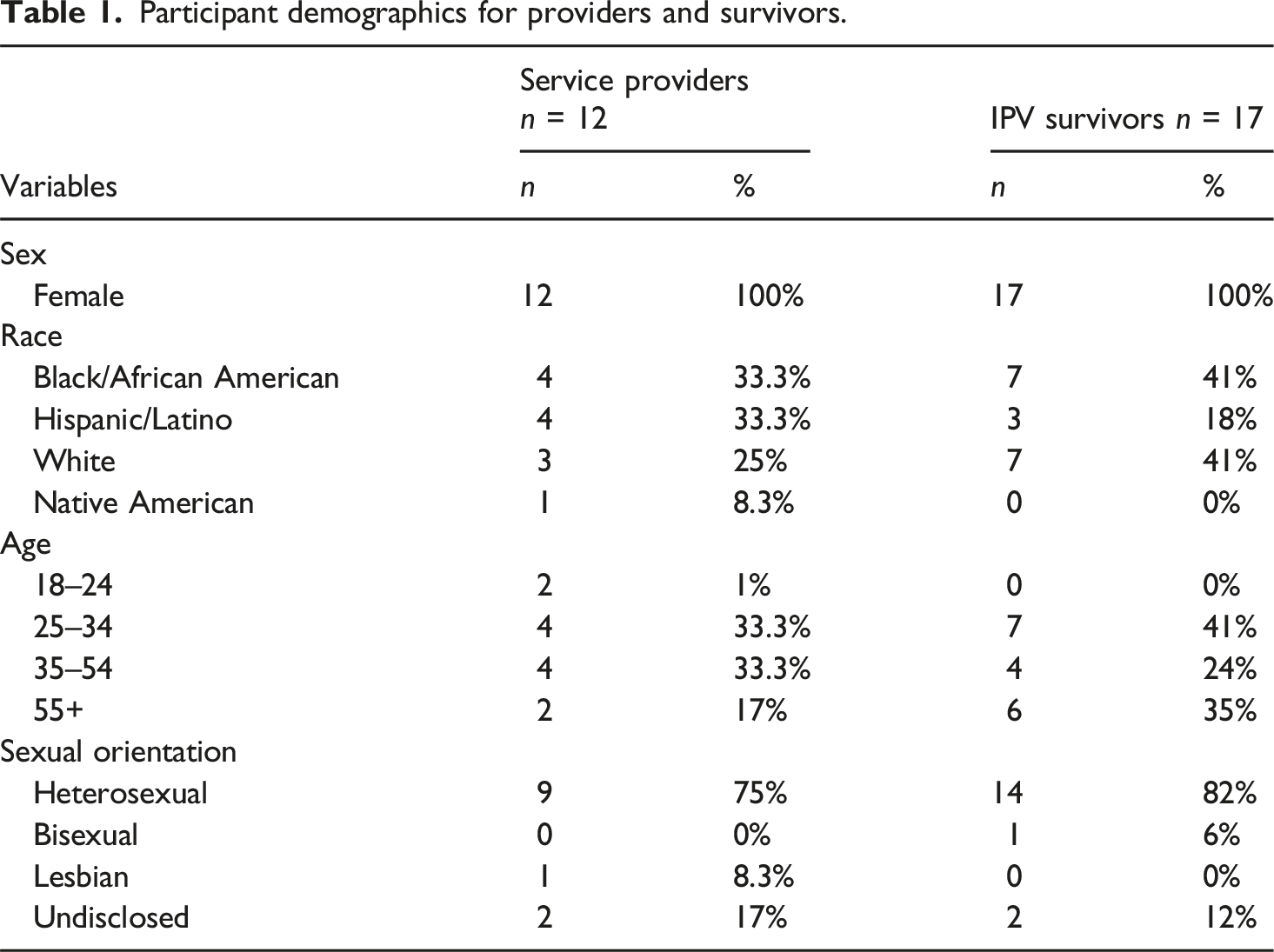
The target population for this study was twofold: (1) female survivors of IPV and (2) direct care providers employed at IPV agencies. Inclusion criteria for IPV survivors were individuals 18 years of age or older, English-speaking, and a current or former client of an agency serving survivors of IPV in this metropolitan area. Inclusion criteria for service provider participants were individuals 18 years of age or older, English-speaking, and employed as direct service providers at an IPV agency located in the same metropolitan area. Agency provider participants included case managers, counselors, intake coordinators, and social workers in residential and non-residential IPV settings. Survivor participants included current clients of IPV agencies that provide services including emergency shelter, counseling, outreach, and housing programs. Consistent with a transformative or feminist research lens, the individuals most directly impacted were included in the development process (McPhail et al., 2007; Plummer and Young, 2010).
Participant demographics for providers and survivors.
Recruitment
The study was a purposive sample recruited in partnership with three IPV service agencies in a metropolitan area in the Southwestern United States. Each agency provides multiple services to individuals experiencing IPV. These programs include, but are not limited to, emergency shelter, short-term housing support, a 24/7 crisis hotline, counseling, legal assistance, and advocacy. The primary researcher had prior experience working with these community partners and contacted agency leadership to distribute recruitment flyers. When requested, this researcher attended staff and client meetings to share study information and elicit participation. Anyone who met the inclusion criteria was invited to participate. Initial challenges in participant engagement prompted the research team to shift data collection to onsite residential programs and coordinate with agency directors to provide childcare, increasing accessibility for survivors. All participants received a gift card for their participation. Data collection took 3 months to reach a sufficient sample size for this study.
Information power
Determining sample size in qualitative research poses challenges due to the absence of calculations commonly found in quantitative studies. Qualitative studies often follow Sandelowski’s (1995) guidance, which states that “qualitative samples should be large enough to allow the unfolding of a new and richly textured understanding for the phenomenon under study, but small enough so that the deep, case-oriented analysis of qualitative data is not precluded.” However, the interpretation of this guidance varies across studies. In grounded theory, saturation involves ongoing analysis and is achieved when no new themes or concepts emerge from the data (Glaser and Strauss, 1967).
To ensure a representative sample from both groups of participants, the research team applied the concept of information power to evaluate the adequacy of the sample size. Information power emerged from qualitative research and is used to determine the extent to which a sample adequately represents the target population. Unlike data saturation, information power assesses the study sample across five dimensions: study aim, sample specificity, use of established theory, quality of dialogue, and analysis strategy (Malterud et al., 2016). Information power is enhanced by the breadth and depth of the data rather than the sheer number of participants.
Throughout data collection, the research team continuously revisited the data to track emerging concepts and their alignment with the dimensions of information power. The researchers sought a diverse sample of participants from different agency settings, programs, demographics, and experiences with IPV. The diversity of the sample strengthened specificity, as participants ranged from women recently leaving abusive partners to those distanced from IPV situations for years. The sample included women across the reproductive life cycle, from childbearing age to post-menopausal. Participant dialogue was robust in quality, as determined by the primary researcher, who utilized prompts to explore participant perspectives in greater depth. Given the study’s focus on conceptualizing an SRH assessment framework, the sample of 29 total participants was deemed sufficient.
Instrumentation and data description
The primary researcher served as the moderator for focus groups and utilized an IRB-approved interview guide to lead the discussion. The interview guide included open-ended questions organized around SRH needs, experiences with SRH services, and components of an assessment process, including preferred content, delivery, duration, and required resources for implementation within IPV agencies. Examples of questions included: What do you consider the most urgent SRH needs of survivors of IPV?, What is the preferred way to ask questions about SRH needs?, and What resources are needed to support the implementation of an SRH assessment within IPV agencies? Survivors and providers were asked parallel questions to capture their perspectives on shared processes and to identify points of divergence.
Consistent with grounded theory methodology, the primary researcher reviewed transcripts shortly after data collection to compare with previous groups and to assess information power. All focus groups and interviews were audio-recorded and transcribed for data analysis. The study received approval from the university’s Institutional Review Board (IRB).
Data collection
Data was collected through semi-structured focus groups and individual interviews with survivors and providers onsite at participating IPV agencies. Interviews were utilized for participants who could not attend a focus group or when only one individual showed up for a group. The study included five focus groups and three individual interviews. Focus groups were facilitated separately for providers and survivors. Focus groups and interviews were recorded with an audio device for data analysis. The primary researcher served as the moderator and took notes throughout each session. Focus groups ranged from 2 to 11 participants and lasted between 40 and 75 min. Interviews lasted between 20 and 60 min.
Before each group or interview, participants were informed of the purpose of the study, signed an informed consent, and were assured that participation was voluntary. Focus group guidelines outlined the expected procedures, and participants were asked to verbally agree to adhere to those guidelines. Since data collection took place at IPV agencies, the researcher ensured that any information collected would not be shared with agency leadership or other staff members. After each session was transcribed, all identifying information was removed to ensure the confidentiality of participants throughout the data analysis process and in the final dissemination of findings.
Data analysis
Consistent with a grounded theory approach, data analysis followed an iterative process in which data collection, coding, and analysis occurred concurrently through constant comparative analysis (Glaser and Strauss, 1967). After each audio recording was transcribed, the primary researcher conducted an initial review and began open coding. The goal of this stage was to generate as many codes as possible from the early data (Bryant and Charmaz, 2007; Charmaz, 2006). In the constructivist approach, Charmaz (2006) emphasizes keeping codes as close to the data as possible. Important words or groups of words were labeled and identified using the qualitative software program, Dedoose.
Although a standard guide of open-ended questions was used across focus groups and interviews, when new concepts were identified during analysis, they were incorporated into question probes to explore further with the next participants. Both researchers coded independently and then compared codes to reduce potential bias and ensure accurate representation of the data. Data collection concluded when no new concepts emerged, and the research team determined that information power was sufficient. Analysis then moved to focused coding, where initial codes were refined and organized into broader categories that reflected the experiences of survivors and providers within IPV agencies (Chun Tie et al., 2019). Memoing was used throughout all phases of analysis as an audit trail to document researcher perceptions, thought processes, and justification for methodological choices.
As analysis progressed, conceptual categories emerged that captured not only recommendations for SRH assessment processes within IPV agencies, but also the underlying thought processes and experiences of survivors and service providers. These were captured into conceptual categories identified as Survivor Outlook, Existing SRH Processes, and Tool Recommendations. Together, these categories describe an interconnected process that emphasizes the impact of trauma and prior agency experiences in shaping how participants perceive SRH needs and their assessment in IPV agencies. These interconnected categories informed the construction of the SRH assessment framework developed in this study. Figure 1 provides a visual representation of this iterative, constructivist-grounded theory process. Model of constructivist grounded theory process.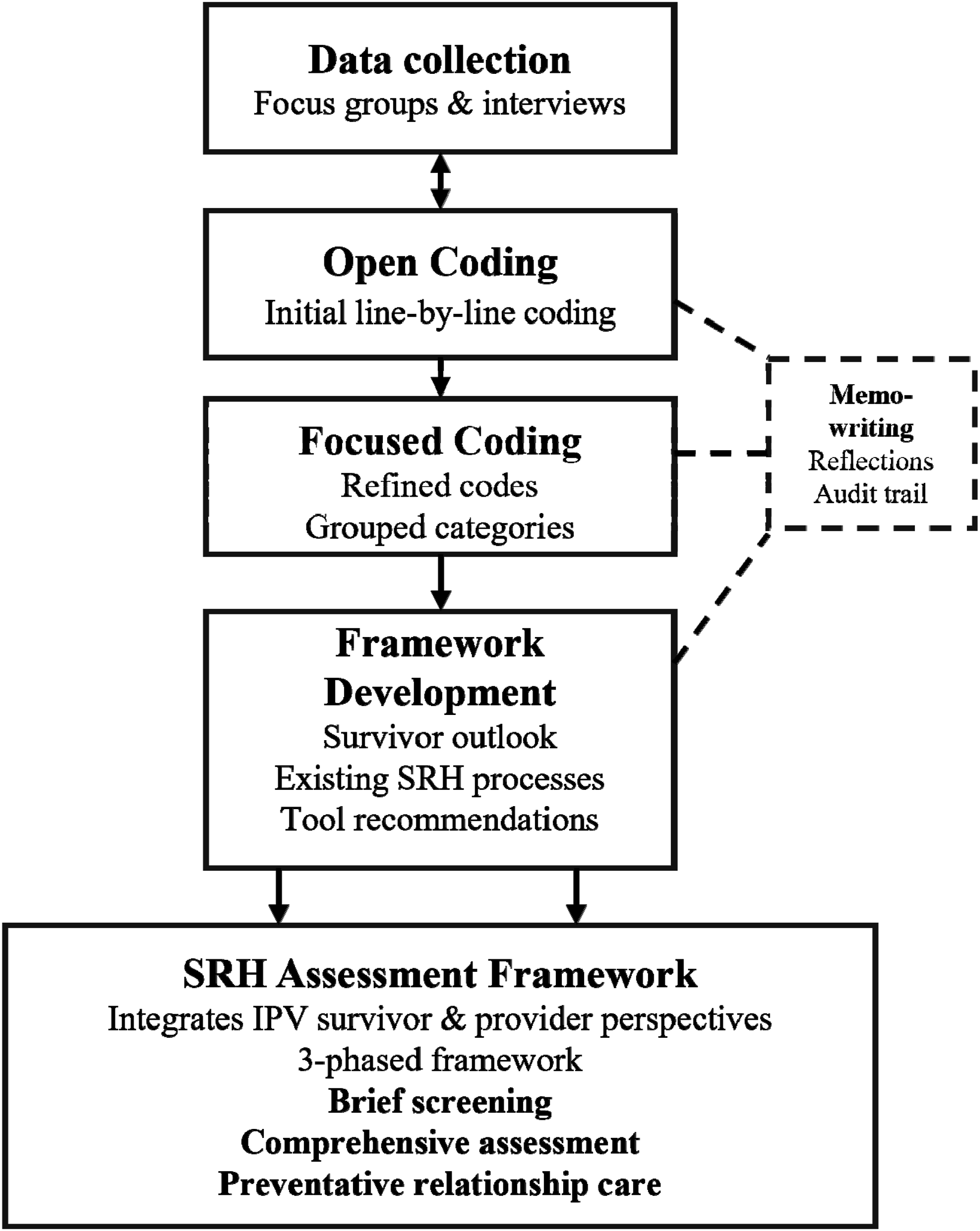
Enhancing trustworthiness
This study used several techniques to enhance the trustworthiness of the research process. The research team incorporated three forms of triangulation: investigator, method, and data source. Memoing was also used to enhance rigor. Due to the challenges of accessing the target population after groups were over and potential safety concerns, member checking was not feasible.
Results
In grounded theory methodology, data analysis traditionally culminates in the generation of a formal theory grounded in the participant data (Birks and Mills, 2015; Chun Tie et al., 2019). In contrast, this study utilized participant quotes, memos, and emerging conceptual categories to construct a framework for SRH assessment within IPV agency settings. The research team explored relationships between categories to identify the core storyline of the study; how survivor and provider experiences shape their perspectives, preferences, and recommendations for SRH assessment in IPV agencies. Although the initial aim focused on identifying preferred processes or strategies for SRH assessment, further analysis revealed the deeper role that trauma played in shaping participant perspectives. The data also highlighted how prior interactions with service providers affect survivors’ trust, thus emphasizing the importance of trauma-informed implementation strategies.
The categories also capture the experiences of service providers working within IPV agencies as they navigate SRH topics with their clients. Provider dialogue revealed a sense of ambivalence between balancing the perceived importance of initiating SRH conversations with their desire to avoid re-traumatization.
The constructed SRH framework that emerged from this study comprises the conceptual categories generated from participant data. These were defined as Survivor Outlook, Existing SRH procedures, and Tool Recommendations. Together, these categories represent an integrative framework that reflects the interaction between trauma, prior agency experiences, and SRH needs. The following section expands each of these conceptual categories. The discussion underscores how the constructed framework not only reflects participants’ lived experiences but also expands current understanding of how SRH needs can be addressed in IPV agencies. Grounding the framework in participant voices ensures that any implementation stays responsive to survivors’ needs. Barriers to implementation are addressed in the discussion of the study findings.
Category 1: Survivor outlook
The conceptual category of Survivor Outlook provides insight into the mindset and needs of IPV survivors when interacting with IPV agencies. Although participants represented different programs and agencies, most described their entry point as an emergency shelter. This category includes two interrelated subcategories: the impact of trauma on service engagement and the specific SRH needs identified by survivors and service providers.
Impact of trauma
Across interviews and focus groups, survivors emphasized the deep influence of trauma on their thought processes during intake and early service engagement. It became clear that the intake process itself often reactivates trauma responses and shapes how survivors perceive and trust providers. Survivors described feeling overwhelmed and, in some cases, retraumatized by having to repeatedly tell their story to different staff members, as this survivor described, When I came, the intake over the phone had you tell your story. The first day that I got here, I had to tell my story. The next day that I got here,I had to tell the story again. These were three different intake people… Just overwhelmed.- Survivor
Other survivors mentioned needing to “take a breath” and difficulty processing intake information. Shame and guilt were used by several survivors to describe how they felt asking for help. A few women expressed anger at their partner for putting them in this situation and forcing them to rely on others. As this survivor described, We’re asking for so much because it's wrecked our lives. And so, I'm constantly apologizing, and I hate apologizing. I hate it when other people apologize. And I'm always like, Don't apologize for needs. But I internally have to fight that battle of like, I should be able to do this for myself, and I can't…this man took everything from us. - Survivor
Service providers recognized similar dynamics and were aware that experiencing IPV could influence a survivor’s willingness to discuss SRH topics. They described how they integrate trauma-informed care principles in their approach. This provider shared the importance of responding in ways that promote safety and trust. Being very mindful about trauma in the brain and how a survivor may present when they're having to potentially talk about something that is very triggering or traumatic for them. I think the person who's asking the question really has to be mindful about what that is like for a client. – Provider
This interaction between survivor and provider perspectives illustrates a shared awareness of the influence of trauma on help-seeking and communication, informing a key concept within the overall SRH framework.
Specific SRH needs
When participants were asked about urgent SRH concerns for survivors, both survivors and providers identified needs that included sexually transmitted infection (STI)/HIV testing, well-women exams, pregnancy tests, emergency contraception, and access to birth control. Responses were consistent across both participant populations, with one exception. Service providers added that education around consent and sexual coercion, especially within marriage, was an essential yet often overlooked need. As this provider stated, “Clients don’t understand that they don’t have to have sex. They have sex because he’s my husband and he forces me. And they think it’s okay.”
Providers indicated that education on consent would be beneficial in identifying potential SRH needs and recognizing sexual coercion as a form of IPV. Although survivors didn’t address this specifically, the research team noted that several participants described experiencing acts of sexual violence or coercion by their partners but struggled with defining that as a form of abuse. As this survivor described, He would wait till I took my night medication that puts me to sleep because I have night terrors and things, and then he would have sex with me without my knowledge. And I think that happens more often than not. And because it's your partner, you make it somehow be okay in your own head.-Survivor
Although abortion was mentioned a few times by both participant populations, when probed for more detail, survivors did not indicate this was a common need, and providers could not provide any examples of helping a client obtain or seek abortion care. In cases where providers mentioned clients considering abortion, those individuals decided to continue with their pregnancies or secured assistance elsewhere. However, it is important to interpret these findings within the broader policy environment, as the study was conducted in a region of the United States with a current ban on abortion care, which may have influenced how participants discussed this topic. When providers were asked about the impact of those restrictions, they reported limited awareness of both state-level restrictions and organizational policies concerning abortion referrals.
Category 2: Existing SRH processes
The conceptual category, Existing SRH Processes, captures how both survivors and providers experience and enact SRH assessment within IPV agencies. Survivors reflected on how SRH was addressed during the intake process, highlighted the benefits of onsite healthcare collaboration, and described how they prioritized SRH needs relative to other urgent needs of survivors. Providers shared their approaches to screening for SRH needs and their perceptions on the importance of offering SRH services. This category describes the participants’ view of current assessment practices, perceived priorities, and barriers to implementation. Two interrelated subcategories, assessment experiences and SRH priority, are used to illustrate the differences in participant perspectives.
Assessment experiences
Both survivors and providers described SRH screening or assessment for SRH needs as rare within IPV agencies. None of the survivors in this study had been asked about needing pregnancy tests, STI/HIV testing, birth control, or assistance obtaining a well-woman’s exam. The only exception to this was an IPV agency with an on-site health clinic. Participants in that setting stated that when receiving medical services at this facility, the on-site nurse did ask about SRH needs.
Although most participants stated that SRH assessments were rare, a few providers mentioned having SRH conversations with clients. These conversations were almost always triggered by a disclosure of sexual abuse. When probed about the content of these conversations, providers described discussions that were centered on sexual coercion in IPV and how that relates to other forms of abuse. As this provider shared, “If we are talking about sexual or reproductive health, it’s more focused on the abuse”. None of these providers connected clients to SRH resources as part of these conversations. However, this indicates that some IPV service providers are navigating SRH conversations.
Several providers stated they were aware of the SRH risk factors present for survivors of IPV and were open to screening for SRH needs. However, providers were hesitant to bring up SRH needs for fear of retraumatizing a client. As this provider stated, We want to be cautious as far as how much we're wanting them to open up because they are traumatized. It's an emotional roller coaster, …a new environment. So, it's like, I don't want to overwhelm you even further than you already are. -Provider
One consideration that may influence this hesitancy is that several providers in this study identified as counselors. This type of provider may be more equipped to navigate therapeutic dialogue around abuse and relationships, but less prepared to assess specific SRH needs. As a result of this hesitancy, providers were more likely to wait until a client mentioned an SRH need before responding. Survivor participants resisted this hesitancy, stating that being asked directly about SRH needs was a sign of care rather than intrusion. Survivors universally agreed that if the expectation relies on them to initiate SRH conversations, they are unlikely to bring them up on their own. As this survivor stated, I definitely need a woman's exam. It's been eight years, so probably that would be good. But it's already an uncomfortable thing. I'm never going to ask for that. But if I get asked “Hey, why don't you reach out to the advocate? I won't” -Survivor
This divergence between service providers waiting for survivors to ask about SRH needs versus survivors waiting for providers to initiate those conversations emerged as a recurring pattern in the data.
SRH priority
Despite their complex needs, survivors viewed SRH needs as important and should be universal at IPV agencies. There was some disagreement about the timing of when these assessments should take place, but overall, survivors agreed that screening for emergency SRH needs should be done at intake. Emergency needs were described as access to emergency contraception and pregnancy tests. When asked about the importance of SRH when compared to other needs, survivors resisted prioritizing one as more important than another. As this survivor described the importance of emergency contraception following a sexual assault, I think that's still a very important question. Women coming out of the hospitals or off the streets, being raped or whatever, I would feel like Plan B is an important thing. So I think it varies depending on what that person's needs are. For somebody, it might not be. But for someone who had something happen to them, it's going to be an important need for them.-Survivor
Providers overall expressed that SRH needs were secondary to other basic needs when entering services.
Survivors in this study did not perceive asking about SRH needs as triggering if they were provided the option to respond. They emphasized that while one woman may not want to discuss SRH needs, it could enable others to have a conversation they may not have initiated on their own. One survivor stated that having SRH conversations could reduce the shame and guilt associated with experiencing sexual violence. As she described here, I think if we talk about sexual health, I think it could also, break cycles. Like I need these other resources for sexual health, and I don't even know where to go or talk about it. Now I'm over traumatized… some cycles could be broken if you just have one sit-down, one little thing. -Survivor
These findings demonstrate that talking about SRH needs can be healing for survivors and does not necessarily re-traumatize them. In every focus group and interview, survivor participants continued to emphasize their desire for service providers to initiate these questions.
Category 3: Tool recommendations
The final conceptual category, Tool Recommendations, reflects participants’ co-constructed suggestions for designing and implementing SRH assessment processes within IPV agencies. Participants in both groups were asked for their thoughts on specific SRH content, implementation strategies, potential questions, ideal length, and suggestions for linking survivors to external resources. Three subcategories, content/structure, delivery, and resource linkage, are described in further detail below.
Content & structure
Participants envisioned an assessment process grounded in survivor choice and phased timing. Survivors prioritized immediate needs at intake, such as emergency contraception and pregnancy tests, and suggested addressing broader health concerns once they felt more stable. This survivor recalled that her first concern was the possibility of pregnancy, “I know I got pregnant with my last child in the middle of intimate partner violence. And I remember thinking, “I hope I’m not pregnant now,” right after.” Additionally, survivors in the study emphasized the timing of questions rather than the nature of the questions themselves.
Survivors and providers described an approach to SRH screening and assessment guided by choice and facilitated by providers. As this survivor explained, “I think that you should give the client a choice. I think a lot of women want to be asked [about SRH]. We just don’t know that we have that option.” (Survivor). Survivors recommended that providers start with a brief screening at intake that includes a drop-down checklist of potential SRH needs. They felt this would assist clients in identifying available resources and eliminate any confusion around the terms “sexual and reproductive health”. Survivors and providers suggested that a more comprehensive assessment could occur later when survivors are better equipped to process information. In a more in-depth assessment, questions about experiences of reproductive coercion and women’s broader health needs, such as gynecological services and mammograms, could be explored.
Several survivors emphasized a need for education around sexual autonomy and how previous experiences with coercive sex may impact future intimate relationships. This was suggested for survivors farther along in their healing journey and removed from crisis. One woman referred to this as ‘preventative relationship care” and could include discussions of family planning goals and navigating sexual boundaries. As she described the psychological impact of IPV on her view of sex, There's also the psychological realm that sex was used as another tool of control and coercion and was not normal. You come here and you don't necessarily know what normal is. And so that is, I think, another whole area of education that needs to be restored in someone who's been through a situation. It's like they teach you how to look for relationship green flags and avoid cycling that way. But you also don't know what normal sexual relations look like. Your self-esteem has been shredded and your stability has been shredded. And so that doesn't just grow back normally in a sexual relationship either. -Survivor
This perspective expands the definition of SRH care to include healing from sexual violence and is not solely focused on SRH screening and assessment.
There were mixed responses within both groups on how to consider the cultural or religious beliefs of survivors in any assessment strategy. Most providers believed it would be helpful to know whether a client has religious or cultural beliefs that prohibit certain forms of SRH care. Survivors thought that asking a simple question about beliefs would be appropriate, although a few women disagreed, stating that someone’s religious views aren’t relevant to the conversation.
Service providers noted the importance of including questions that were inclusive of survivors in same-sex and polyamorous relationships. When asked for sample questions, providers didn’t offer specific suggestions, but felt it was important to include diverse perspectives, noting that most tools are centered on heterosexual relationships. Survivors in this study also mentioned including questions for individuals in same-sex relationships; however, most survivors identified as straight. Future research is needed to gain the perspectives of survivors who identify as LGBTQ.
Delivery
Participants emphasized that how questions are asked matters as much as what is asked. Participants in both groups recommended that the initial screening be brief, take less than 5 min, and include only a few questions. Survivor responses varied when it came to whether questions should be administered verbally or through a paper questionnaire. Some survivors expressed support for the use of an app for SRH screening, while others opposed a digital method. The overall recommendation was that providers should provide choices to survivors in how they answer these questions.
Survivors were aware that many service providers feel uncomfortable discussing certain topics and emphasized the importance of training staff to navigate SRH conversations effectively. If staff are not knowledgeable in SRH topics, survivors recommend involving a nurse or other healthcare provider, as this survivor stated, It should be done by the nurse or somebody that is in that field, because I know a lot of the intake people, a lot of the case manager people, they are not experienced in that level. So I don't feel comfortable with sharing that information because I feel like it's just going down the drain. -Survivor
Participants in both groups stressed that any questions be administered sensitively, keeping in mind the mental state of the survivor before proceeding. Providers felt it was important to be mindful of the language used in conversations and seek ways to normalize the discussion. These comments reinforce that the delivery of an assessment process is deeply tied to trust, competence, and safety, all key components in trauma-informed practice.
Resource linkage
Both participant groups offered internal and external suggestions for linking survivors to SRH resources. Internal suggestions focused on IPV agencies providing more SRH services onsite. Both providers and survivors recommended providing SRH kits directly to clients at intake. As this survivor described, “I feel like when somebody comes in there at intake, they should be given a goody bag full of condoms, pads, and tampons.” Other survivors added that pregnancy tests, birth control information, and emergency contraception should also be included. Providers recommended adding SRH resources to their referral cards, organizing on-site events focused on SRH needs, and developing psychoeducational groups on reproductive health topics.
External resource suggestions were focused on enhancing healthcare access, particularly since some agencies did not offer any healthcare services, and many survivors lack health insurance. Participants in both groups strongly recommend enhanced collaboration between IPV agencies and women’s health providers. Survivors expressed the need for better inter-agency collaboration between providers, including intake staff, case managers, housing specialists, and therapists. The agreement of these strategies across participant groups suggests mutual support for integrated SRH services that extend beyond screening and assessment.
The three conceptual categories of Survivor Outlook, Existing SRH Processes, and Tool Recommendations reflect components of the broader SRH assessment framework. Together, these categories describe a relational process where trauma, autonomy, and agency culture interact and shape how SRH needs are identified, discussed, and addressed in IPV settings. The research team examined this process to construct a trauma-informed SRH framework grounded in the experiences of survivors and providers. The phased approach of this new SRH assessment framework illustrates how each category was incorporated to guide a practical application of these findings in agency settings. This framework begins by prioritizing trust and safety (Survivor Outlook), moving gradually to promote shared understanding and dialogue (Existing SRH Processes), and concludes with structured, collaborative practices for implementation (Tool Recommendations).
Discussion
This study addresses a critical gap in IPV research and practice by proposing a survivor-informed SRH framework that integrates both screening and assessment, while centering survivors’ lived experiences. Consistent with prior findings that survivors prefer integrated, trauma-informed care (Boyce et al., 2020; Grace et al., 2020; Wood et al., 2021), participants in this study highlighted the diverse needs of individuals at different stages of service engagement. These insights informed the development of a framework comprised of three conceptual categories: Survivor Outlook, Existing SRH Processes, and Tool Recommendations. Each of these categories reflect the perspectives of both survivors and service providers and offers practical guidance for agencies to deliver responsive, survivor-centered care and strengthen SRH support in IPV contexts.
The framework is broken into three phases to respond to the SRH needs of survivors (See Figure 2). The initial phase is SRH screening at intake or shortly after. This screening should be brief, consisting of one to two questions, focusing on immediate SRH needs, and include a drop-down list of options. Identifying specific needs should be included to eliminate any confusion around the terms “sexual” or “reproductive health”. As with all phases of this framework, responses should be optional. Immediate or time-sensitive needs, such as emergency contraception, abortion care, and pregnancy tests, would be prioritized during this phase, and connection to those resources should be immediate. SRH assessment framework for IPV agency settings.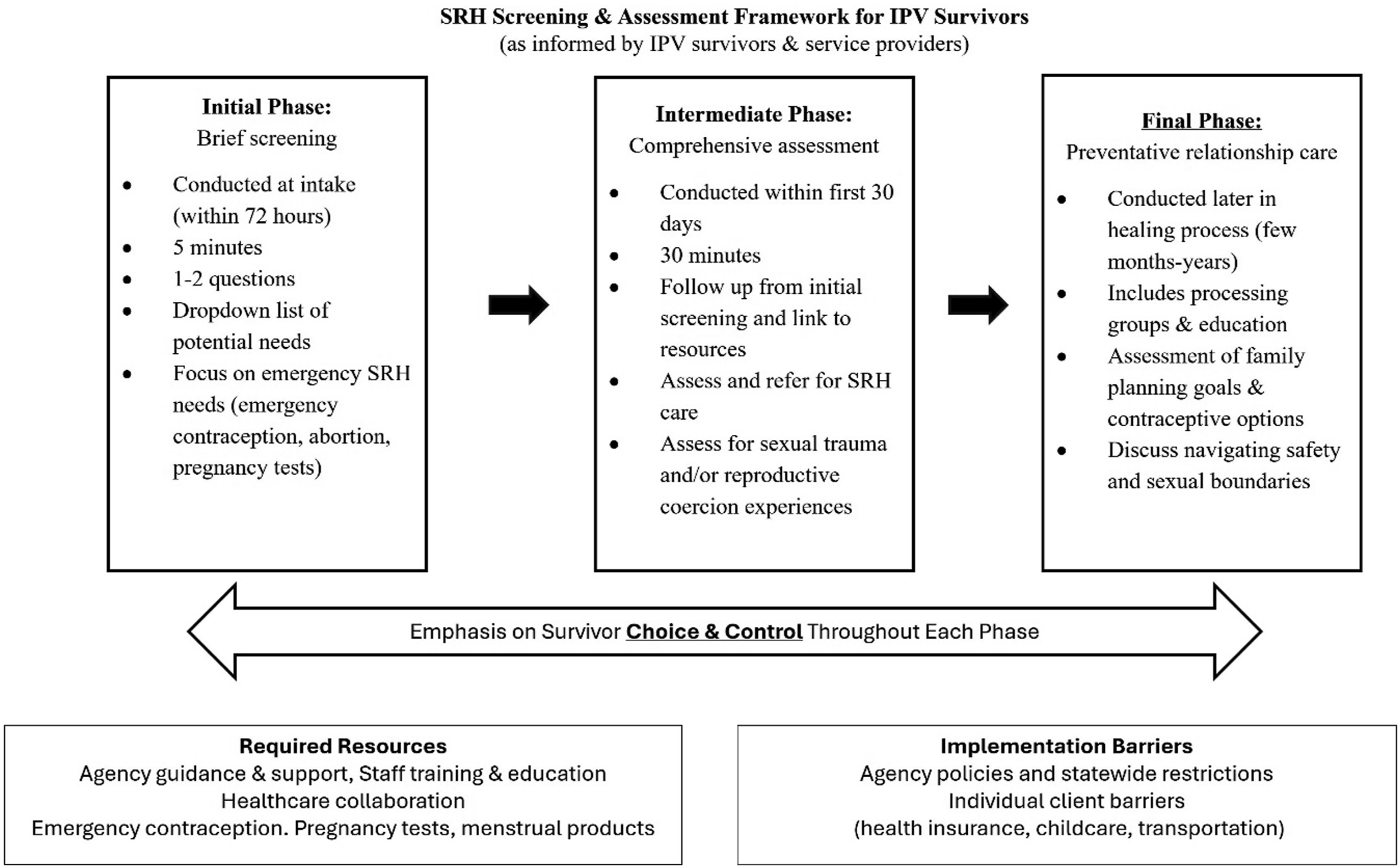
The next phase in the framework would occur later in the service delivery process, but within the first 30 days. In this phase, providers would conduct a more detailed assessment of survivors’ SRH experiences and link to healthcare resources such as women’s exams and mammograms. Providers would assess for RC and provide education on the relation to other forms of abuse. Service providers in this phase must be adequately trained to handle discussions and to refer survivors to external community resources.
The final phase in the framework is intended for survivors who are further along in their healing journey, months to even years after leaving their abusive partner. This phase was constructed in response to survivors’ desire to address the impact of abuse on their understanding of sex and navigating future sexual relationships. Although IPV education typically includes identifying red flags in relationships, survivors stated that more is needed to address how body shaming and forced sex from abusive partners distort their view of sexual encounters. This phase would help survivors identify sexual boundaries and promote personal safety.
Framework implementation barriers and opportunities
The findings also offer insight into the barriers and opportunities of implementing SRH assessment into standard IPV services. Screening or assessing SRH needs is ineffective without follow-up action. Agencies implementing SRH screening must ensure access to pregnancy tests and emergency contraception. While not a central focus of this study, statewide restrictions on abortion care and emergency contraception can significantly limit survivor options and must be considered in service delivery planning. For agencies in states with such restrictions, providers should be familiar with state laws and organizational policies for assisting survivors with reproductive health services. Additionally, individual barriers such as transportation and childcare can hinder survivors from accessing external resources, including access to healthcare.
On-site health care partnerships emerged as a significant strength in our study. This is consistent with a previous study indicating that IPV survivors favor programs integrating healthcare and IPV-related services (Dichter et al., 2021). The onsite clinic at one agency provided survivors with immediate access to healthcare services, regardless of their health insurance status. For service providers, this streamlined access to SRH through experienced medical staff, who were also well-versed in IPV. However, establishing and maintaining those partnerships requires considerable effort and resources. For settings where this is not feasible, IPV agencies should seek to collaborate with external community health clinics.
Implications for social work practice, policy & research
Findings from this study highlight the critical intersections between IPV and SRH, underscoring the need for trauma-informed, survivor-centered responses across research, practice, and policy. By amplifying survivor voices and examining provider perspectives, this work identifies both barriers and opportunities for advancing SRH assessment in IPV contexts. The following implications outline actionable directions to strengthen research agendas, enhance service delivery, and inform policy development.
Research implications
Engaging survivors and service providers in the research process ensures that SRH assessment frameworks reflect lived realities. Survivors in this study described how trauma can impair their ability to process information, articulate needs, or seek help, reinforcing the importance of trauma-informed approaches in screening and assessment (Hussain and Khan, 2008; O’Connor-Terry et al., 2022).
Future research should: • Prioritize participatory methods that center survivor voices. • Investigate provider training needs and organizational readiness to integrate SRH into IPV services. • Evaluate the effectiveness of SRH assessment frameworks across diverse settings and populations.
Research must move beyond documenting needs to co-develop and test survivor-informed frameworks that can be implemented in practice.
Practice implications
The proposed framework provides IPV service providers with a structured approach to assessing SRH needs. Consistent with prior research on reproductive coercion (Grace and Anderson, 2018; Logan et al., 2007; Miller et al., 2010), findings revealed a disconnect: providers tended to wait for survivors to initiate SRH discussions, while survivors expected providers to lead. Survivors also emphasized that proactive dialogue could reduce stigma and foster trust.
Practice recommendations include: • Training IPV service providers and healthcare professionals to initiate and normalize SRH conversations. • Embedding trauma- and violence-informed principles into assessment protocols. • Offering survivors choice and flexibility in how SRH topics are introduced to respect autonomy while ensuring access. • Incorporating ongoing supervision and reflective practice to address provider discomfort with sensitive topics.
Providers should be equipped and empowered to lead survivor-centered SRH conversations that normalize dialogue and reduce stigma.
Policy implications
Policy development is critical as restrictions on reproductive health care heighten risks for IPV survivors. Without clear guidance, providers may lack tools to navigate conflicting mandates.
Policy recommendations include: • Advocating for federal and state protections that safeguard access to comprehensive SRH services for IPV survivors. • Developing agency-level policies that provide clear guidance on SRH assessment within restrictive legal contexts. • Allocating resources for provider training, organizational infrastructure, and cross-sector collaboration. • Promoting survivor-centered, trauma-informed policy frameworks that integrate SRH into IPV service delivery.
Policies must ensure consistent access to SRH services for IPV survivors by embedding trauma-informed, survivor-centered standards across systems.
Limitations and future research
This study involved 29 participants (12 service providers and 17 survivors), all from a single metropolitan area in the Southwestern United States. While participants represented diverse programs and agencies, the findings may not reflect the experiences of survivors and providers in rural areas, those identifying as LGBTQ, or individuals who speak languages other than English. Most participants identified as heterosexual and English-speaking, further limiting generalizability. Additionally, focus group methodology may have introduced social desirability bias, and, as with all qualitative research, researcher bias is possible despite efforts to mitigate it through triangulation.
Future research should expand to include more diverse populations, particularly LGBTQ and Spanish-speaking survivors, and survivors in rural contexts. Studies are also needed to test the feasibility and effectiveness of implementing SRH assessment frameworks in both IPV agency and healthcare settings, as well as to evaluate survivor outcomes when these tools are applied.
Conclusion
This study contributes an IPV survivor- and provider-informed framework for assessing SRH needs, advancing knowledge at the intersection of IPV and reproductive health. Findings underscore the critical role of IPV service providers in proactively addressing SRH needs, especially for survivors with limited access to healthcare. By integrating trauma-informed, survivor-centered approaches, service providers and policymakers can help reduce stigma, increase access, and promote holistic well-being for survivors of IPV. Ultimately, integrating SRH assessment into IPV services represents not only a clinical or organizational shift but also a broader commitment to advancing equity and dignity for survivors. Continued collaboration among researchers, providers, and policymakers is essential to ensure that survivors’ voices remain central in shaping the future of practice and policy.
Footnotes
Ethical considerations
This study received ethical approval from the TCU Institutional Review Board (approval #2023-350) on October 31, 2023.
Consent to participate
This study was approved by the TCU IRB from the TCU Institutional Review Board (approval #2023-350) on October 31, 2023. All participants provided written informed consent before participating.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the study was funded by an internal Texas Christian University (TCU) Student Research Grant.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author, upon reasonable request. The data are not publicly available due to them containing information that could compromise research participant privacy/consent.