
Abstract

Purpose: Sexual problems in cardiac patients are receiving increasing attention, because sexual functioning may be impaired due to heart failure, cardiac medication, or psychological barriers. It is anecdotally reported that patients with congenital heart disease may have problems with sexual functioning, because some of them are afraid for physical overexertion. Since this has not been investigated so far, we assessed whether adults with congenital heart disease perceive problems with sexual functioning, and explored potential differences with that of healthy persons.
Methods: Secondary data analysis was performed on data from a quality-of-life study in which 404 patients were matched to 404 healthy counterparts, according to age, gender, educational level, and employment status. The sample consisted of 54.7% males. Median age was 23 years. 57.4% of the patients was unmarried and living with their parents; 33.9% was married or cohabiting; and 8.7% was living alone, divorced or widowed. The CHD-TAAQOL was used to assess determinants of quality of life. This questionnaire includes 5 items on sexual functioning. For each item, both the perceived frequency and associated distress was scored. Group differences were expressed as mean standardized differences between patients and healthy counterparts. One sample t-test was used to evaluate whether mean standardized differences significantly differed from zero (p<0.05).
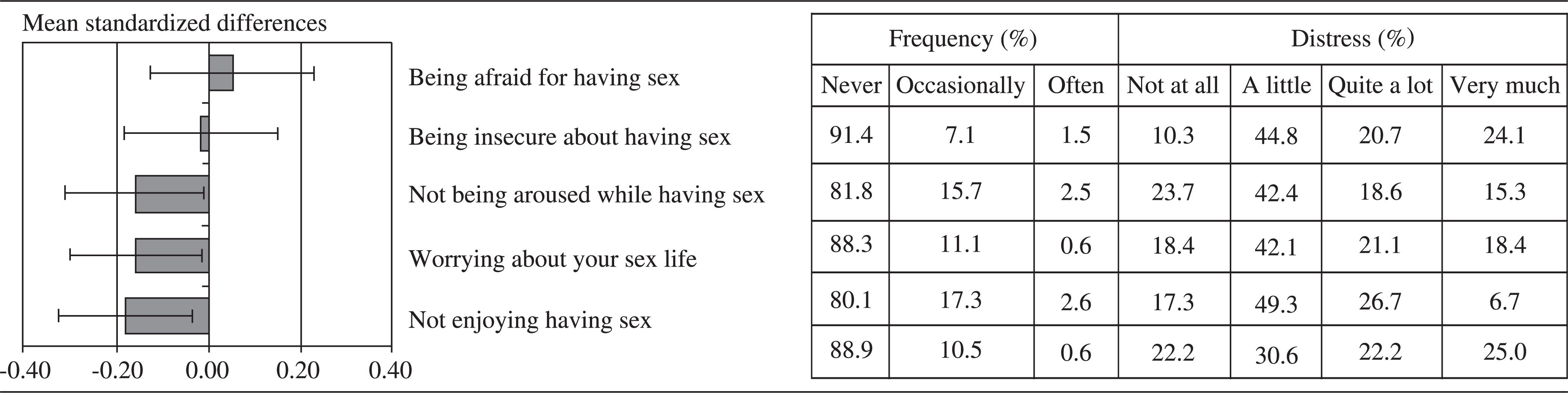
Results: Sexual problems were perceived by 10% to 20% of the patients. If these problems occurred, they were distressing for most patients, though in varying degrees. Patients reported significantly less distress for ‘not being aroused while having sex’, ‘worrying about your sex life’, and ‘not enjoying having sex’ than healthy counterparts.
Conclusion: The majority of the patients do not report sexual problems. Although some aspects of sexual functioning are perceived as very distressing for up to a quarter of the patients, they are equally or even less distressing in patients than in healthy controls. However, these results have to be interpreted with caution because this study was based on secondary data analysis; no data on sexual activity or stable relationship were available; and it is possible that patients are more likely to provide social desirable answers than controls. Hence, further research to scrutinize sexual functioning in these patients is needed.