
Abstract
Objectives:
To determine whether weight loss interventions, which combine dietary, exercise and behaviour change strategies, result in reduced weight, body mass index (BMI) and waist circumference in people with coronary heart disease (CHD), hypertension (HTN) and/or type 2 diabetes mellitus (T2DM).
Design:
A systematic review of studies published 1997 to 2010.
Data Sources:
The electronic databases MEDLINE, PsycINFO, COCHRANE, CINAHL and EMBASE.
Review Methods:
Studies were included if samples were: ≥ 18 years old, overweight or obese (BMI 26–39.99 kg/m2), and diagnosed with CHD, T2DM and/or HTN. Only randomised controlled trials (RCTs) or systematic reviews of RCTs reporting group-based interventions that combined dietary, exercise and behavioural change strategies and outcomes for weight, BMI and/or waist circumference up to 12 months were included. Two researchers extracted data and appraised quality, with a third making final decisions.
Results:
Eight RCTs were included (total n = 1428). Participants’ mean age was 60.4 years and 61% were female. Interventions varied by contact time, content and delivery. Mean weight loss ranged from −2 kg to −4 kg (SD 4 kg) at 3–4 months, −1.3 kg to −8.2 kg (SD 4 kg) at 5–6 months and −0.87 (SD 0.57 kg) to −6.9 kg (SD 4 kg) at 12 months. Of the few studies that measured waist circumference the mean reduction was −3.1 cm at three and 12 months.
Conclusions:
Weight loss interventions that combine exercise, diet and behaviour change strategies result in minor weight loss at 3–12 months in people with CHD, T2DM or HTN. Further research is required to determine the most effective and efficient methods.
Introduction
The rising prevalence of overweight and obesity presents multiple health challenges to clinicians and health service providers as these conditions contribute to the development and progression of disease. 1 In people at risk of cardiovascular disease (CVD) events due to a diagnosis of coronary heart disease (CHD), hypertension (HTN) and/or type 2 diabetes mellitus (T2DM), obesity and overweight is particularly problematic, as it is both an independent risk factor and more prevalent in this population.2,3
The association between obesity and the acceleration or exacerbation of existing CVD is well established. Increases in cholesterol levels, insulin resistance, triglycerides and blood pressure are widely acknowledged mechanisms. In particular, weight gained around the abdomen, as central adiposity, is strongly associated with increased risk.4–6 Obesity is also associated with CVD through the development and progression of other conditions, especially T2DM and HTN. Moreover, these diseases are often concurrently present, furthering cardiovascular risk. Estimates from the National Diabetes Information Clearinghouse 7 suggest that adults with T2DM have CVD mortality rates two to four times higher than the general population. 7
Purposeful, sustained moderate weight loss of 5–10% in conjunction with regular physical activity has been shown to produce clinically significant reductions in CVD risk factors and future CVD events.2,8,9 Given these benefits, weight loss interventions have been developed and include medications, bariatric surgery and lifestyle modification programmes. While a combination of these approaches is reported to be effective for weight loss, 10 the use of medications and surgery can be accompanied by risk for people with CHD, T2DM and HTN. In contrast, lifestyle interventions including diet, exercise and behaviour change strategies have been demonstrated as effective for weight loss, 11 and for reductions in mortality. 12
The relative benefit of weight loss interventions for people who may have CVD as well as T2DM and/or HTN, has not been clearly distinguished. In fact, individuals with these conditions may be intentionally excluded from weight loss interventions because the presence of these diseases may present barriers to weight loss.11,13 Few weight loss interventions targeted at the high CVD risk population account for the complex nature of CVD, and often fail to provide an emphasis on modifying and managing commonly associated conditions such as T2DM and HTN. Furthermore, secondary prevention programmes such as Cardiac Rehabilitation (CR) are less successful at supporting weight loss. Most overweight CR patients do not lose weight, regardless of any gain they may make in other areas such as exercise capacity.4,14
Dombrowski et al. 15 reviewed the effect of weight loss interventions in people with comorbid conditions including T2DM, impaired glucose tolerance, HTN and CVD amongst others. This review reported that behavioural interventions that address diet and physical activity were most effective in producing weight loss. 15 The effects of these interventions on people diagnosed with CHD, T2DM or HTN were not distinguished from other comorbid conditions. Similarly, a systematic review conducted by Norris et al. 16 focusing on people with pre-diabetes reported that interventions that combine diet, exercise and behaviour change strategies, delivered by frequent contact with health professionals over several months were most effective, resulting in two to three kilograms of weight loss at 12 months. However, no systematic review was found which reported weight loss interventions that combined all three strategies and was designed specifically for overweight or obese people diagnosed with CHD, HTN and/or T2DM. Furthermore, few reviews identify whether delivery method includes group methods, a strategy recommended to reduce costs and promote peer support and commitment in this population. 17 In the absence of such a review, it is difficult for health professionals to determine the most effective and suitable interventions for their clients in this population; arguably a group with a particularly high need for intervention. Therefore, this systematic review aims to address this gap by a comprehensive search and appraisal of the availability and effectiveness of weight loss interventions that combine diet, exercise and behaviour change strategies delivered by group for overweight and obese individuals with CHD, T2DM and/or HTN.
Methods
The search strategy is summarised in Figure 1 and began by searching five bibliographic databases: MEDLINE (through PubMed), PsycINFO, COCHRANE, CINAHL and EMBASE from 1997 to 2010. We used the following search terms and their Boolean combinations: weight, loss, diet, exercise, physical activity, management, intervention, treatment, overweight, obesity, cardiovascular, risk, coronary, HTN and diabetes. Only articles written in English were selected. We also searched the reference lists of the selected studies to identify further studies which had not been retrieved through the initial search.
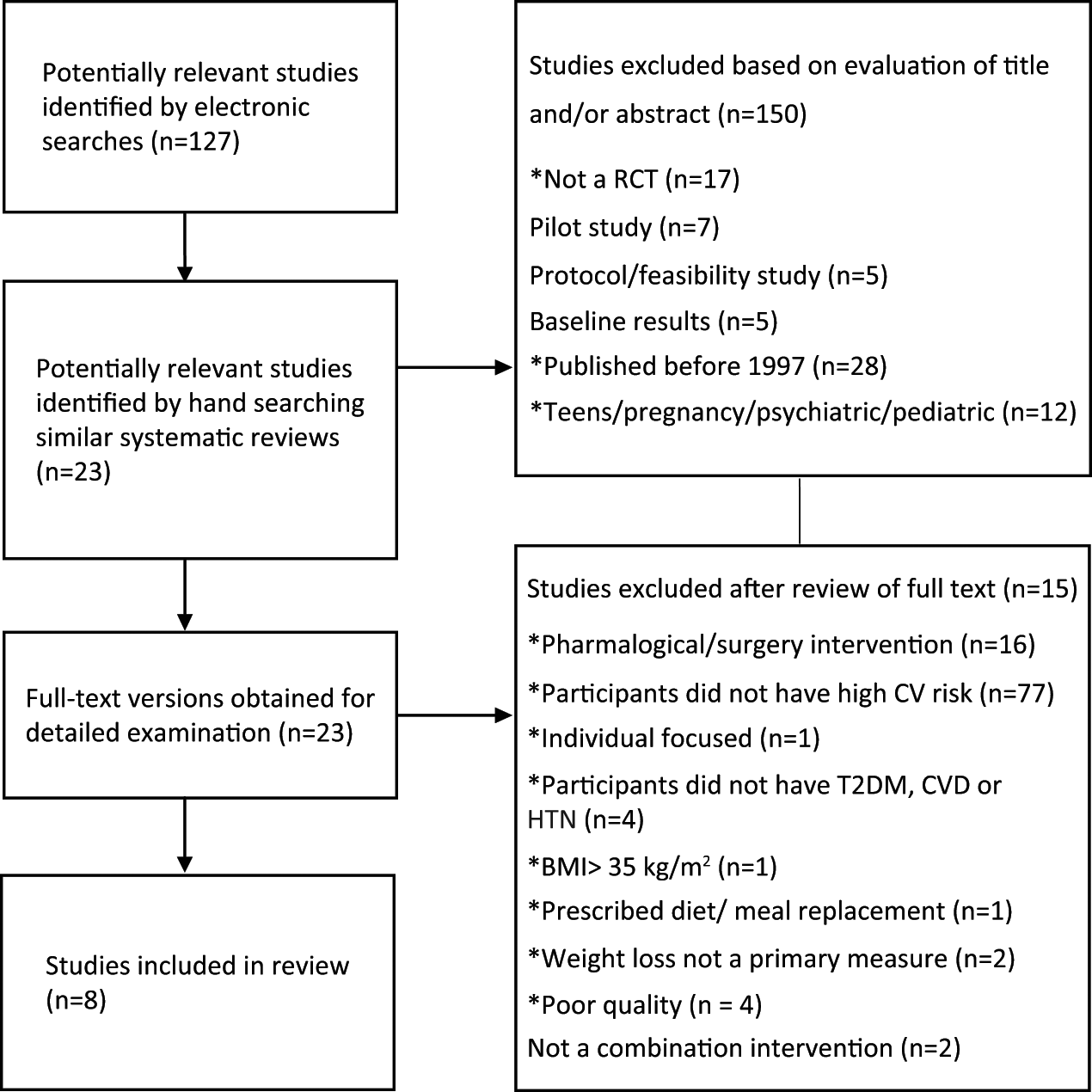
Search strategy.
Studies were included if they included adults who were moderately overweight or obese as determined by BMI of 26 kg/m2 to 39.99 kg/m2, 1 and having a diagnosis of CHD, HTN and T2DM; randomised controlled trial (RCT) or systematic reviews of RCTs; measured weight, BMI or waist circumference as outcomes up to 12 months; interventions which included exercise, diet and behaviour change strategies. Behaviour change strategies were considered to be those that influence an individual’s ability to adopt and sustain new lifestyle behaviours in the long term and may incorporate problem-solving skills, providing adaptive coping strategies and skills, self-monitoring, goal setting and stimulus control.17,18 Exercise strategies included were supervised, structured exercise sessions and/or specific advice for group-based exercise programmes. Any dietary strategies modified for the complex needs of patients with CHD, T2DM and/or HTN by a nutritionist or other health experts, were also included in this review. Studies were excluded if participants had other severe conditions such as heart failure, renal disease or psychiatric illness or were single-focus strategies, such as diet, exercise or behaviour change or included pharmacological or surgical therapy or diets that did not clearly involve self-direction, such as meal-replacement shakes, pre-prepared meals and highly specific prescribed diets.
Following this process, the remaining studies were then appraised by two researchers (RG and EA) using a modified JADAD quality scoring criteria. The criteria used and percentage of studies that incorporated the criteria is in parantheses as follows: 1, the technique for randomising participants to groups is stated and appropriate (63%); 2, the sample size is sufficient to answer the question (50%); 3, methods of standardising the intervention are described (100%); 4, all participants including withdrawals and dropouts are described (100%); 5, intention-to-treat analyses is used (13%); 6, blinding of data collectors and statisticians is described (0%). 19 Only studies meeting at least two of the six quality appraisal criteria listed were included in the review.
Results
The review yielded eight studies, all RCTS, which were summarised by two of the researchers (RG and HW) (Table 1). We report mean differences in weight change between the intervention group and the comparison group for each time period, and as a percentage of baseline weight to determine if weight loss reached a clinically significant difference using the National Institutes of Health (USA) guidelines of 5–10% weight loss. 19 Table 1 summarises the weight loss results of all studies over time.
Description of included papers, sample, intervention and results.

Mean difference in weight change between the intervention group and the comparison group for each time period, (as % of baseline weight).
BMI: Body Mass Index; CG: control group; CHD: coronary heart disease; T2DM: type 2 diabetes mellitus; Dx: diagnosis; HTN: hypertension; IG: intervention group; NS: not statistically significant; SD: standard deviation.
Characteristics of the participants
The total sample was 1428, the mean age was 60.4 years and overall proportion of females 61%, with one study comprised 100% female. 20 Participants were obese, with an average BMI of 33 kg/m2 (range 30 21 to 36.77 kg/m2 22). Four studies purposefully recruited participants with T2DM,20 –23 two studies recruited participants with HTN,24,25 one study recruited participants with CHD, 26 and one study recruited participants with CVD, 27 although participants often had multiple comorbidities. Three studies recruited a specific population subgroup including postmenopausal women, 20 older African-American people 23 and underserved rural communities. 22 Sample sizes ranged from 64 23 to 288. 27 Six studies took place in the USA20,22–24,26,27 and one each in Australia 25 and the Netherlands. 21
Weight loss interventions
The interventions were heterogeneous for the delivery methods and the amount of contact time with the intervention team. All interventions used face-to-face group delivery methods and these sessions took place in community or hospital outpatients clinics, although the interventions differed in contact time with each intervention team. Individual sessions were also included in six of the interventions,21–23,25–27 but were not always compulsory 25 and could be delivered either face-to-face21–23,25 or by telephone.23,27 Studies targeting specific groups included additional strategies to promote feelings of empowerment and social support.20,22,23 The interventions were delivered by dieticians and exercise physiologists20,23,24,28 or specifically trained registered nurses 21 although some studies did not provide this detail.22,25,27
Exercise
Physical activity designed to promote a negative energy balance was promoted in all interventions, with one intervention promoting high-calorie-expenditure exercise and longer duration of activity to accelerate weight loss. 26 Supervised structured exercise sessions of 30–60 minutes were included in five studies,20,23,24,26,27 varying in frequency from a maximum of four sessions per week for six months 24 to one/week for three months,23,27 beginning with frequent sessions gradually decreasing for a further 5–6 months.26,27 One study included supervised yoga and relaxation sessions along with the structured exercise sessions for the first six months. 20 Exercise diaries were used to help participants monitor and advance their efforts.21–23,26,27
Diet
Dietary advice promoted caloric restriction, control of carbohydrate and fat intake and increased intake of grains, fruit and vegetables, alongside the use of diet diaries to promote self-monitoring of intake. Two studies identified a specific type of diet, either the Mediterranean diet, which promotes an alpha-linolenic acid-rich diet, 20 or the DASH diet, which limits sodium intake. 25 Similar to exercise, diet sessions were group-based and via one or two additional individual consultations in two studies.22,23
Behavioural change
Behaviour change strategies involved the promotion of goal-setting and self-monitoring of progress against goals, and the development of self-efficacy in all studies. Specific strategies included behaviour modification,23,26,27 promoting the development of self-efficacy21,27 and self-regulation, 23 and stress management. 20 Theoretical frameworks upon which their strategies were based included social cognitive theory,20,21,27 behaviour modification,22,23,25–27 social action theory, 23 group dynamics, 27 self-care and proactive coping, 21 and goal systems. 20
Contact time with intervention team
The amount of contact time participants had with the intervention team members varied greatly. The intervention with the most amount of contact included a two and a half day workshop in a retreat format at the commencement of the intervention, followed by four hours of contact/week for six months. 20 The intervention with the least amount of contact included five two-hour sessions over 12 months. 21 However, the majority of interventions had at least weekly sessions for a 3–6-month intervention phase, followed by reduced frequency of sessions for a further 3–6 months.20,22–24,26,27
Comparison groups
The multicomponent weight loss interventions that are the focus of the review were compared to usual care,20,24,25 and several other types of interventions including: minimal interventions such as a single information session21,22 or a mail-out of educational material, 23 a single-focus strategy such as exercise 24 or information, 22 and Phase II cardiac rehabilitation (6–8 weeks of structured exercise and information sessions). 26
Outcomes
Outcomes for weight loss, BMI and waist circumference are reported as differences from baseline and mean differences (calculated where possible) in the study summary (Table 1).
Weight loss
Interventions that combine diet, exercise and behaviour change strategies achieved more weight loss than single-focus or usual care comparison groups in all studies reviewed. In these groups, weight loss increased over time to 6 months and declined at 12 months, so that at 3–4 months mean differences were relatively small at −1.8 kg 23 and −2.8 kg, 25 but had increased at 5–6 months to −0.44 kg, 20 −1.6, 22 −3.2 kg, 23 −4.5 kg, 26 −6.1 kg, 24 −7.1 kg 27 and −8.6 kg 24 decreasing slightly by 12 months to −1.9 kg, 22 −2.3, 21 −2.5 kg 25 and −4.1 kg. 26 In the comparison groups, the most weight loss occurred in the standard Phase II CR comparison group at −3.7 kg at five months and −2.8 kg at 12 months. 26 Single-focus-only comparison groups achieved much less weight loss, for exercise only −1.8 kg 24 and −0.5 kg 27 and for information and support only −1 kg 22 and −0.8 27 at six months.
Overall, weight loss varied between groups, but was generally more pronounced with greater contact time. Weight loss benefits were generally greatest in the interventions with the most contact time with the intervention team, at mean difference −8.6 kg 24 versus comparison groups with the least contact time at 5–6 months, at mean differences of −7.1 kg 27 and −4.5 kg. 26 An important exception to the trend of more weight loss with greater contact occurred for the study which had the most amount of contact time with the intervention team with only a relatively small (–0.44 kg) weight loss advantage. 20 Inclusion of weekly supervised exercise sessions achieved mean differences in weight loss that were ≥ 5% and thus clinically significant.24,27
BMI was measured in six studies21–26 and the patterns of BMI change were consistent with weight changes, with mean differences between the intervention and comparison groups of −0.8 kg/m2 23 at 3–4 months, −0.81 kg/m2 22 to −3 kg/m2 24 at 5–6 months and −1.4 kg/m2 21 at 12 months. While three studies measured waist circumference outcomes,23,25,26 only one study resulted in reduced waist circumference with −3.1 cm change, both at 3–4 months and 12 months. 25
Discussion
Weight loss interventions combining diet, exercise and behaviour change strategies, result in weight loss in people diagnosed with CHD, HTN and/or T2DM and in the moderately overweight or obese. Only three interventions achieved a clinically significant difference in weight loss of ≥ 5% at six months24,26,27 and only one sustained this weight loss to 12 months. 26
The most sustained weight loss was achieved in interventions that had high levels of contact time with the intervention team, particularly where this contact time included regular supervised exercise sessions and where this exercise was of sufficient time and intensity to promote a negative energy balance.24,26,27 These interventions clearly addressed cardiovascular risk factor reduction by focusing on combined physical activity and dietary lifestyle change interventions as recommended in a scientific statement recently released by the American Heart Association (AHA). 17 As a result, weight loss was greater than the 2.8 kg at 12 months reported in systematic reviews of more general lifestyle interventions. 16 Furthermore, interventions which focused on exercise alone did not achieve as much weight loss as interventions that incorporated supervised exercise with other disease management aspects such as Phase II CR.24,26,27
Another important component in successful weight loss interventions generally appears to be prolonged and frequent contact.16,17 Frequent contact supports the cognitive behavioural strategies which are integral to the interventions, such as goal-setting, feedback on progress, and promotion of self-efficacy. However, in the review addressed in this paper, the critical element is most likely the length of time over which contact occurs, rather than the total amount of contact alone, as the intervention with the most contact had poor weight loss outcomes. 20 A great deal of the contact in this intervention occurred in an initial 2.5-day retreat versus the consistent and prolonged contact of other high-contact interventions which had better weight loss outcomes.26,27 However, other potential explanations are likely as the Toobert et al. 20 study which included the early retreat exclusively recruited women, and women have been reported to have poorer weight loss outcomes than men. 28
It is important to note that contact time not only applies to the health professionals delivering the intervention but also to other group members, as all interventions were delivered by group. The role of the group in providing peer support for behaviour change should not be underestimated. Peer support not only provides role models and potential solutions to problems, but also the opportunity to share experiences that may not be found in everyday life.17,29 Peer-based support likely enhances the cognitive-behavioural strategies integrated into the interventions reviewed. The role of peers may be particularly important in people with CHD, HTN and T2DM because they face additional barriers to weight loss, such as comorbid conditions and disease management issues. 29 Commitment to the group and enjoyment may also contribute to retention in the interventions.
In the studies reviewed, attrition rates were moderate at 16–20%, but little detail was provided on the techniques used to promote continued attendance by participants. This lack of detail is important when considering how the interventions can be implemented into reality. Additionally, given that contemporary views hold that obesity itself is a chronic condition, 11 the means of effectively helping participants achieve sustainable weight management habits and strategies is crucial for independent and ongoing management of weight. No study included in the review reported on how participants achieved this independence or how transition to community and group-based endeavours was promoted, and it would be an important consideration for future research.
The implication for practice is that overweight and obese people with T2DM, HTN and CHD can lose weight with the support of multi-component weight loss interventions. A range of successful intervention models are available from this review which could be implemented in ambulatory settings. Given that most of the resources required are available when programmes such as CR and diabetes education are combined and the populations overlap substantially, a suitable, cost-effective model could be developed. As these services are generally recommended for patients, if such a model were successful it could be scalable to the public health level. The role of the peer group needs to be fully explored and the potential for trained peers to reduce the contact time and costs of health professionals needs to be considered as intensive and prolonged interventions are likely to be more expensive and difficult for health services to sustain. 10 Finally, the use of technology in supporting weight loss is currently under-investigated, yet offers opportunities for supporting weight loss that are effective and relatively inexpensive. 30
Limitations
Although the search for literature was extensive, some relevant studies may have been missed. The review is limited by the availability of relevant data from selected studies due to insufficient and specific detail of outcomes including weight, BMI and waist circumference reduction. The results of the review may not be generalisable to contexts beyond the USA where most of the studies were conducted. Furthermore, more detail is required than presented in the studies on the type of personnel required, the specific training that they may have received and their expertise in CHD, HTN or T2DM. Finally, the costs of programmes were not reported, making it difficult for health service providers to determine the relative costs of the resources required to run the interventions for the weight loss achieved.
Conclusions
This review demonstrates that group-based weight loss interventions which combine behaviour change, exercise, diet and follow-up strategies, are effective for reducing weight and BMI in people who are diagnosed with CHD, HTN and/or T2DM and moderately overweight or obese. Most benefit occurred when supervised exercise was included, there was frequent contact in the first 4–6 months and follow-up continued to 12 months. Further research is required to establish the relative contribution of the peer group and costs to determine the most effective model.
Footnotes
Acknowledgements
We acknowledge Patrick Gallagher for editorial assistance.
Conflict of interest
None declared.
Funding
We acknowledge the Australian Technology Network of Univer-sities Centre for Metabolic Fitness for funding this review.