
Abstract
Objective:
To provide a critical review and analysis of heart failure (HF)-specific symptom measures
Methods:
A systematic search using the PubMed and Cumulative Index of Nursing and Allied Health Literature (CINAHL) databases and reference lists of relevant papers was undertaken to identify symptom measures that were primarily designed for patients with HF.
Results:
The systematic search yielded seven instruments that included three or more symptoms. Of the seven instruments, only five had psychometric properties available and these were reviewed. Levels of comprehensiveness of symptom measures varied including the number of symptoms assessed (13–32 symptoms/signs) and symptom dimensions (e.g. frequency and severity). Information about reading levels, time to completion, and completion rates was limited. Psychometric properties of the five measures have not been extensively investigated or reported.
Conclusion:
The development and use of the HF symptoms instruments is at a relatively early stage. Thus, further investigation of the psychometric characteristics of existing HF-specific symptom instruments is necessary before one can be recommended for research and clinical use.
Introduction
Heart failure (HF) is a progressive, irreversible clinical syndrome, characterized by substantial symptom burden. 1 Patients with HF report an average of nine physical symptoms even when they are not experiencing an exacerbation. 2 Dyspnea and fatigue, the most prevalent HF symptoms, are experienced by more than half and up to 94% of all patients with HF.2–5 The presence of multiple symptoms negatively affects functional status, health-related quality of life (HRQOL), and survival.4–7 Thus, it is essential to provide effective symptom assessment and management in HF patients.
One of the primary goals of HF management is reducing patient symptom burden. To achieve this goal, it is important for clinicians to systematically assess symptom burden. Comprehensive evaluation of symptoms allows healthcare providers to (1) reduce symptom burden, a focus important to patients and (2) assess the effectiveness of interventions to improve symptoms.
There are few symptom instruments developed for HF patients that measure the full range of symptoms experienced by patients. For example, some instruments only include physical symptoms, although emotional symptoms are prevalently experienced by patients with HF. 2 Symptom experience is multidimensional, meaning that it includes not only presence or absence of symptoms, but also frequency, severity, and distress related to symptoms, some instruments are designed to evaluate only one aspect of the symptom experience. Thus, to accurately assess the symptom experience in patients with HF, it is critical to evaluate commonly used instruments.
The purpose of this paper is to provide a critical review and analysis of self-reported symptom measures designed for and used in patients with HF. The specific aim of this paper is to evaluate their quality with five criteria (i.e. content, measuring scale, psychometric properties, completion process, and information).
Methods
A systematic search using the PubMed and Cumulative Index of Nursing and Allied Health Literature (CINAHL) databases (August 1978 to June 2012) was undertaken. Search terms were selected by scanning search strategies of a systematic review on a similar topic 8 and examining index terms. Combinations of keywords and subject headings were used for the electronic database search (Figure 1). Reference lists of all pertinent articles identified by online database searches were searched.
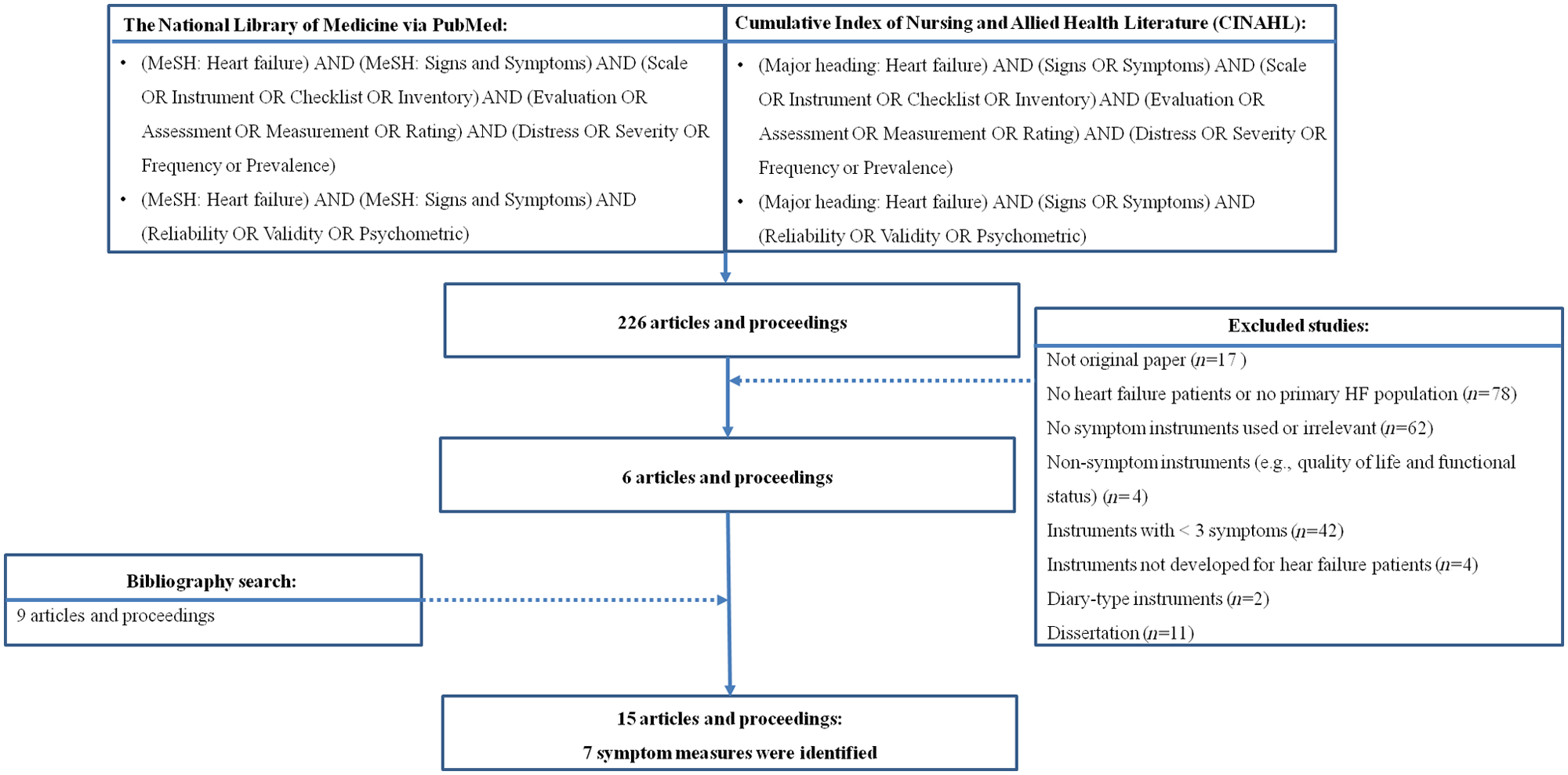
Flowchart of literature search.
The search was limited to journal articles and proceedings published in English. Instruments were included in the review if they were primarily designed or modified for patients with HF to measure multiple symptoms (≥ three symptoms). Exclusion criteria included HRQOL instruments or their modified versions; single-symptom item instruments; instruments measuring symptom perception (awareness) or functional status rather than symptoms; or diary-type instruments.
Instrument evaluation
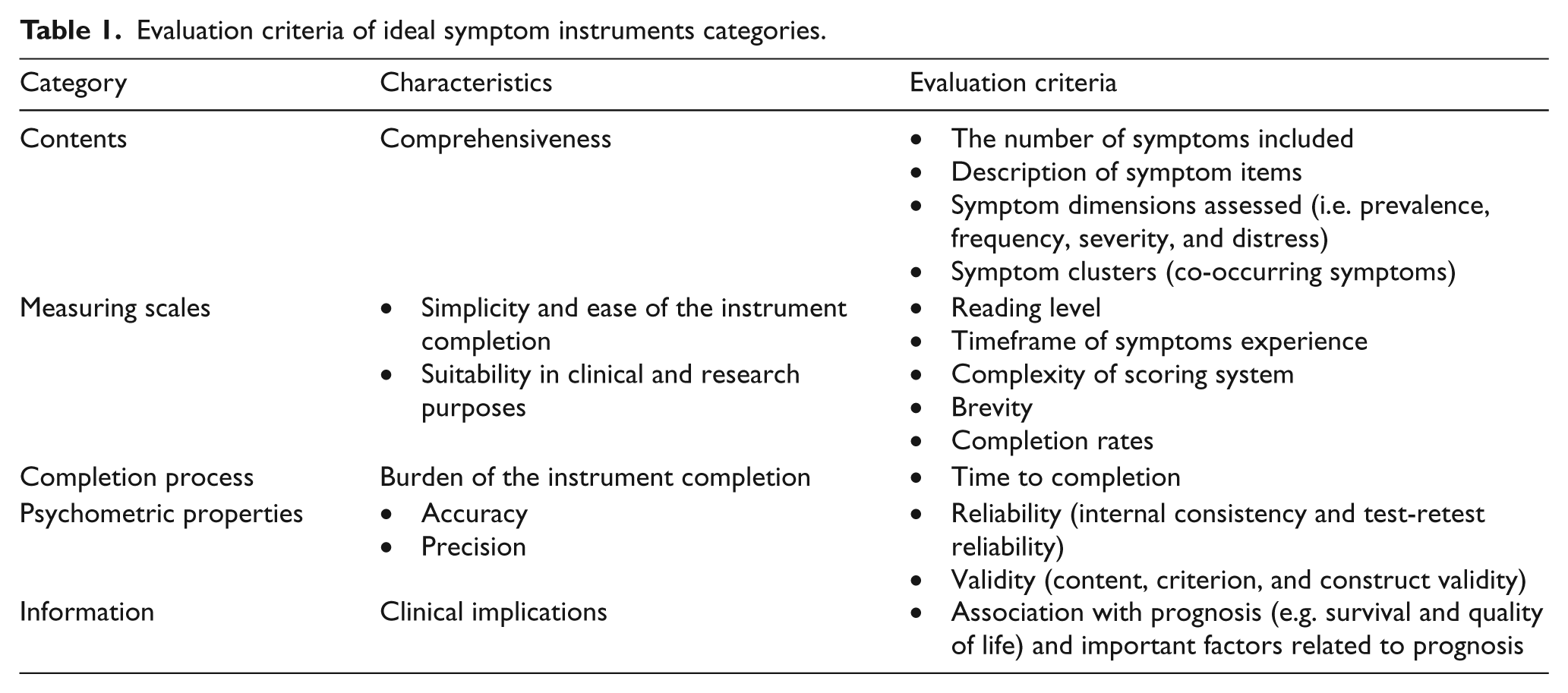
Instruments were evaluated based on five criteria, which we modified according to the criteria developed by Kirkova and colleagues 8 to rate the quality of the instrument (Table 1). The five evaluation categories were: contents, measuring scale, psychometric properties, completion process, and information.
Evaluation criteria of ideal symptom instruments categories.
Results
The search strategies yielded 226 articles and proceedings. Of those, 15 articles5,9–19 and proceedings20–22 met the inclusion and exclusion criteria for this review. Of the 15 articles and proceedings found, seven symptom measures developed for HF patients and including three or more symptoms were identified. However, the EuroHeart Failure Survey-Symptom 17 and the modified version of the Cardiac Symptom Survey 18 were excluded because information on these instruments (e.g. psychometric properties or how it was developed) was unavailable in the literature or from the corresponding authors. Two articles,10,19 in which the modified Memorial Symptom Assessment Scale-HF (MSAS-HF) was used, were also excluded from this review. Because these studies were conducted in Korea, it was impossible to evaluate the quality of this symptom measure. Therefore, we reviewed five symptom measures (Table 2).
Symptom measures reviewed.

Targeting HF patients with cancer.
NA: not available; HF: heart failure; NYHA: New York Heart Association.
Of the five symptom instruments, three were modified based on symptom measures developed for patients with cancer or cardiac surgery (i.e. the HF Symptom Survey 20 from the Cardiac Symptom Scale, the M.D. Anderson Symptom Inventory-HF (MDASI-HF) 15 from the M.D. Anderson Symptom Inventory, and MSAS-HF 21 from the MSAS).
Symptom measures reviewed in this paper included signs (e.g. weight gain and diarrhea) along with symptoms, despite the fact that definitions of signs, defined as ‘objective evidence or indication of disease’ 23 and symptoms, defined as ‘bodily or mental phenomenon, circumstance, or change of condition arising from and accompanying a disease or affliction, and constituting an indication or evidence of it,’ 24 are different and clearly describe distinct phenomena. However, symptom measures did include signs as well as symptoms; we evaluated each measure as originally developed by the authors.
Contents
The five instruments varied in the number of symptoms/ signs assessed (13–32 symptoms/ signs) (Table 3). The HF Signs and Symptoms Checklist, 14 the MDASI-HF, 15 and MSAS-HF 21 included not only typical HF symptoms related to fluid overload (e.g. edema) but also atypical symptoms (e.g. dry mouth). Three of the five instruments contained both physical and psychological symptoms, but the HF Symptom Checklist 9 and the HF Signs and Symptoms Checklist 14 did not. Orthopnea, paroxysmal nocturnal dyspnea, edema, and coughing were addressed in all five instruments. Psychological symptoms were excluded in the HF Signs and Symptoms Checklist 14 and the HF Symptom Checklist, 9 and fewer psychological than physical symptoms were included (2–5 psychological symptoms vs. 12–27 physical symptoms). Symptoms were described with different descriptors. Coughing was further specified as ‘worsening cough,’ 20 ‘nighttime cough,’ 15 ‘dry and hacking cough,’ 9 and ‘severe cough – keeping awake at night or chest hurts when coughing.’ 14 Symptoms items in the HF Signs and Symptoms Checklist were more descriptive than other instruments. For example, weight gain was also further specified as ‘greater than 2 pounds in a day or 5 pounds in a week’ in the HF Signs and Symptoms Checklist, 14 whereas general terms were used in other measures such as ‘weight gain’ in the MSAS-HF. 21
Symptoms included in the symptom measures.

Patients are asked to check the box to indicate the swelling sites (ankles or legs; abdomen; or all over).
Fatigue, tiredness or lack of energy were assessed with one item.
Profound fatigue with exertion or generalized weakness were assessed with one item.
Nausea, vomiting, diarrhea and/or loss of appetite were assessed with one item.
Difficulty concentrating or forgetfulness was assessed with one item.
HF: Heart failure.
Multiple symptom dimensions (e.g. frequency and severity) were addressed in three measures (i.e. the HF Symptom Survey, MDASI-HF, and MSAS-HF), whereas only presence or absence of symptoms was assessed in the HF Symptom Checklist 9 and the HF Signs and Symptoms Checklist. 14 Symptom frequency was the least frequently reported, whereas severity and distress (or interference) were the most frequently included. There were no symptom measures that inquired about co-occurring symptoms to examine the presence of symptom clusters.
Measuring scale
Reading levels of the instruments were not explicitly addressed. However, authors who developed the HF Signs and Symptoms Checklist and the MDASI-HF mentioned their efforts to simplify wording of items to increase patients’ understanding.14,15
Depending on the purpose of symptom instruments (e.g. daily or intermittent symptom assessment), patients were asked to recall their symptom experience within a certain time period. Timeframes varied from ‘during last 24 hours’ 15 to ‘during previous 2 weeks,’ 9 although most instruments measured symptoms that had been experienced over 7 days.
With the exception of the two instruments (i.e. the HF Signs and Symptoms Checklist and HF Symptom Checklist) measuring the presence or absence of the symptoms (yes or no),9,14 numeric ratings were used in three instruments (i.e. the HF Symptom Survey, MDASI-HF, and MSAS-HF).15,20,21 In the HF Symptom Survey, patients were asked to write down the appropriate numeric values to indicate their symptom scores from 0 to 10, whereas response options in the MSAS-HF and the MDASI-HF were laid out and patients circled their rating. Each numeric point in the scale was labeled with adjectives (e.g. mild and severe) in the MSAS-HF, whereas adjectives were given at the anchors in the MDASI-HF.
Scores on each dimension (e.g. severity and frequency) were commonly derived by summing and/or averaging scores of each symptom. However, to compute total distress scores in the MSAS-HF its original distress scores, which ranged from 0 to 4, were rescaled with a 0.8 increase. 5 Composite scores of all the dimensions scored were formed in the MSAS-HF and the MDASI-HF. The total burden score in the MSAS-HF was determined by averaging scores in each dimension of symptoms (frequency, severity, and distress). 5 An overall symptom distress score in the MDASI-HF was computed based on the mean scores of six symptom interference items (i.e. how have your symptoms interfered with your life). 15 There were subscales for HF-specific symptoms in the MSAS-HF and the MDASI-HF that were scored by averaging scores of HF relevant symptoms, such as edema, coughing, and palpitations.
The five symptom measures covered 13–32 symptoms/signs, but the number of items that patients answered was often larger than the number of symptoms included in the measure. This occurs because multiple symptom dimensions were assessed with each symptom item. For example, in the HF Symptom Survey, in which 14 symptoms were included and four dimensions were assessed in each symptom, patients answered a total of 56 items.
Information about completion rates was unavailable except for the HF Symptom Survey. In a study using the HF Symptom Survey, 5% of patients did not fill out all symptom dimensions of each symptom or responded in a contradictory manner (e.g. despite indicating not having a symptom, non-zero ratings of other symptom dimensions for the same symptom were given). 11
Completion process
Completion time was unavailable except for the HF Symptom Checklist. It took approximately 10 minutes for patients to complete the 13-item HF Symptom Checklist. 13 All instruments were designed to be a paper–pencil format as opposed to a computerized format.
Psychometric properties
Reliability
Internal consistency was reported in all instruments except for the HF Signs and Symptoms Checklist. Stability was not reported in any of the five symptom instruments reviewed.
The HF Symptom Survey
Good internal consistency across the four symptom dimensions (i.e. frequency, severity, interference with physical activity, and interference with enjoyment of life) was observed with Cronbach’s α of 0.80–0.88. 20
The HF Symptom Checklist
The Cronbach’s α was 0.68,9,12,13 which is lower than the desirable values of the internal consistency (Cronbach’s α ≥ 0.8). 25
The MD. Anderson Symptom Inventory-HF
Good reliability was observed for the 13 MDASI-HF core symptoms, eight HF symptoms, and six interference items with Cronbach’s α of 0.89, 0.83, and 0.92, respectively. 15
The Memorial Symptom Assessment Scale-HF
Internal consistency reliability of burden scores in each subscale was examined using Cronbach’s α, which were 0.80–0.87 for the physical symptom subscale; 0.83–0.91 for the psychological symptom subscale; and 0.73–0.85 for the HF symptom subscale.5,21
Validity
The HF Symptom Survey
The 14 symptoms were identified by literature review. A HF expert panel consisting of four nurses examined its content validity. 11 Criterion validity was not reported. Construct validity was examined with convergent validations. Moderate to strong correlations were found between the subscale scores of the HF Symptom Survey and the Kansas City Cardiomyopathy Questionnaire, which measures HRQOL in patients with HF (r = −0.62 to −0.78). 20 Symptom frequency and severity scores in the HF Symptom Survey increased significantly as New York Heart Association (NYHA) functional class increased from I to IV. 20
The HF Signs and Symptoms Checklist
Content validity was evaluated by a panel of four HF experts. 14 Lynn’s method, 26 which consists of a two-stage content validity process (instrument development and quantification of content validity using Index of Content Validity), was used to ascertain content validity.
Criterion validity was not explored. Construct validity was supported by demonstrating the association between symptom scores (the number of symptoms reported by patients) and their functional status measured by NYHA functional class. 14 Patients in a hospital care setting experienced more symptoms than patients in an ambulatory care setting. 14
The HF Symptom Checklist
The items in the HF Symptom Checklist were identified from HF symptoms listed in the Agency for Health Care Policy Research 1994 publication on HF practice guidelines.9,12,13 Two cardiac clinical nursing specialists validated the items.9,12,13 High correlations were reported between the items in the HF Symptom Checklist and a symptom checklist which was developed for medical record reviews.9,12,13 No information about construct validity was available.
The M.D. Anderson Symptom Inventory-HF
HF symptom items were generated by literature review, patient interviews, and HF experts and refined by a panel of HF experts. 15 Index of content validity was used to rate the relevance of items by the expert panel. 15 Initially, 30 items were included in the MDASI-HF, and three items were removed (i.e. depression, anxiety, and limitation of physical activity) due to item redundancy. 15
Criterion validity using concurrent validation was supported by moderate correlations of two commonly used symptom measures with the MDASI-HF (r = 0.59–0.62 for NYHA functional class and r= 0.55–0.65 for the Eastern Cooperative Oncology Group, respectively). 15 Construct validity was evaluated by comparing differences in average severity and interference scores by B-type natriuretic peptide (BNP) categories formed using the cutoff point of 100 pg/ml. Significant group differences were observed in symptom severity scores but not interference scores. 15 Factor analysis was performed using eight HF symptom items. Two underlying factors emerged: (1) overt HF symptoms (nighttime cough, paroxysmal nocturnal dyspnea, fatigue, orthopnea, and palpitations); and (2) covert HF symptoms (sudden weight gain, abdominal bloating, and edema). 15
The Memorial Symptom Assessment Scale-HF
Information on the validity of the MSAS-HF was limited. Zambroski and colleagues modified the MSAS by adding five HF-specific symptoms and eliminating five cancer-specific symptoms from the MSAS. No information was available about the content validation of the modified items in HF patients. Information supporting criterion validity was not reported. The construct validity was supported by demonstrating that patients with HF had higher scores in symptoms prevalence than healthy adults without HF. 21 Symptom burden and prevalence scores were associated with scores of the Minnesota Living with HF Questionnaire, which measures HRQOL. 5
Information
There were a limited number of studies in which a longitudinal approach was used to examine the relationship between symptom scores and prognosis. Friedman and colleagues found a small correlation (r = 0.34) between scores of the HF Symptom Checklist administered during hospitalization and scores 4–6 weeks after the index hospitalization. 9
The associations between scores in the symptom measures and outcomes (e.g. HRQOL) and important factors associated with outcomes (e.g. depressive symptoms) were investigated in three studies.5,9,15 In a study in which the MSAS-HF was used, the scores of total symptom prevalence and total symptom burden scores predicted HRQOL. 5 In another study in which the HF Symptom Checklist was used, symptom scores at baseline (during hospitalization) explained 13% of the variance in scores of depressive symptoms 4–6 weeks after the index hospitalization. 9 Symptom severity scores measured with the MDASI-HF were significantly different between patients who had high and low BNP levels. 15
Discussion
We reviewed five symptom measures that have been designed for and used in HF patients. This critical review suggests that, taking into account evaluation criteria, at present the MDASI-HF is the most appropriate multidimensional symptom measure, although its target population is HF patients with cancer. The challenge in this review was the dearth of information about the development process and psychometric properties of symptom measures. Only one article 15 and three proceedings20–22 were aimed at exploring psychometric properties of symptom measures. None of the symptom measures reviewed in this paper provided sufficient information on all five criteria used to evaluate instrument quality.
Levels of comprehensiveness of symptom measures varied among the five measures reviewed. The variability in content among symptom measures may be associated with instrument developers’ views of the separateness of symptoms. In the HF Signs and Symptoms Checklist, ‘nausea, vomiting, diarrhea and/or loss of appetite,’ which are gastrointestinal-related problems, were assessed with one item. In the MSAS-HF feeling nervous and feeling irritable, which are the characteristics of anxiety, 27 were counted as separate symptoms. A possible problem with combining symptoms together is that healthcare providers are unable to capture exactly which symptoms are experienced by patients without further probing. On the other hand, too fine a separation of symptoms may be unwarranted as patients may be unable to distinguish subtle differences between similar symptoms.
Another factor related to the content variability may be what kinds of symptoms (typical and/or atypical HF symptoms) instrument developers intended to measure. The HF Symptom Checklist consisted of typical HF physical symptoms, whereas the other four included typical as well as atypical HF symptoms. In an initial clinical assessment, instruments containing a variety of symptoms may be beneficial to gain a fuller picture of patients’ symptom experiences. Given that multiple comorbid conditions and polypharmacy are common in patients with HF, patients often experience cardiac and non-cardiac symptoms.2,28 A comprehensive symptom instrument can serve as a prompt for patients to ensure that they provide information about all symptoms they are experiencing. 14 After the initial assessment with a comprehensive symptom measure, healthcare providers may determine which symptom measures, either HF symptom-focused or full version, can be used for the follow-up visits depending on patients’ symptom experiences.
Including different symptom dimensions also influences the variability in the content. The MSAS-HF and the HF Symptom Survey contained three dimensions whereas the HF Signs and Symptoms Checklist and the HF Symptom Checklist had one dimension (presence or absence of symptoms). A multidimensional approach to symptom assessment is important because simple presence or absence of symptoms does not fully describe symptom experiences. 29 However, there are issues with the length of multidimensional symptom measures and their potential use in a busy clinical setting, given that the completion time for the 13 item-HF Symptom Checklist was approximately 10 minutes. 13
Information about reading levels was unavailable for the five measures reviewed. Albert and colleagues addressed their efforts in selecting simple, easy wordings to describe symptom items in the HF Signs and Symptoms Checklist. 14 Also, the authors included operational definitions of symptom items. For example, sudden weight gain was defined as ‘greater than 2 pounds in a day or 5 pounds in a week’ in the HF Signs and Symptoms Checklist. Providing definitions helps patients understand the meaning of items by increasing the clarity of items. 14 It is also beneficial for healthcare providers to obtain accurate, reproducible results by conveying a consistent meaning of symptom items to patients. However, it would be difficult to compare results among symptom instruments if each instrument developer defines similar symptoms differently. It is necessary to conduct critical evaluations of which definitions most properly describe symptoms.
Completion rates are one of the important indicators to evaluate applicability of instruments. Age and disease severity are associated with completion rates of measures.8,11 Older adults and critically ill patients are less likely to answer all items of the measures. Similarly, older patients had higher levels of incomplete responses to items in the HF Symptom Survey than younger patients. 11 Therefore, population characteristic of interest should be considered when developing or selecting symptom measures to increase the acceptability.
Clear instructions to patients are important in order to obtain quality data. Inadequate instructions led to the problem of patients providing frequency or severity despite endorsing the absence of the same symptom. 11 Similar errors were also reported by Chang and colleagues 30 when they used the MSAS in the cancer population. Because the MSAS-HF used instructions similar to the MSAS, it is expected that this same problem may occur when the MSAS-HF is administered to HF patients.
Psychometric properties of the five measures have not been extensively investigated or reported. Of the four measures in which internal consistency was examined, good internal consistency was supported in all measures except for the HF Symptom Checklist. Stability has not been investigated in any symptom measure reviewed, which may be related to relatively rapid changes in symptom status.
Four measures9,14–16 showed evidence of content validity. Rigorous content validation processes were described by instrument developers by conducting literature review, using the Index of content validity, or consulting with a panel of HF experts. However, there is no report available regarding content validity of the MSAS-HF.
Criterion validity was not commonly performed, which may be related to the fact that there is no gold standard to measure symptoms in the HF population. Construct validity was demonstrated by convergent validations and factor analysis. However, as the validation process is ongoing, more validation studies about these measures are needed. Despite the dearth of information about psychometric properties, the MDASI-HF has been rigorously examined and showed sound psychometric properties.
Symptom measure scores should be helpful to make clinical decisions and facilitate symptom management. Only three studies5,9,15 demonstrated that symptom scores were associated with outcomes. The limited information regarding clinical implications may be related to the fact that the five symptom measures were recently introduced (2001–2010) and were not widely used in HF research.
Based on the review, we propose a couple of elements of ideal HF symptom measures. Because a comprehensive symptom assessment should guide clinicians to manage symptoms in patients with HF, HF symptom measures that include typical and atypical symptoms of HF are preferable. Creating subscales, such as acute symptoms of HF decompensation, may be practical to perform a focused, rapid assessment. As symptoms are multidimensional, the presence or absence of symptoms provides limited information, thus, the ideal instrument should include multiple dimensions of symptoms such as, severity of symptoms and the burden associated with them. It must be remembered, however, that measures without well-established psychometric properties are not useful in clinical or research settings. Therefore, ideal measures are ones that assist clinicians to conduct a comprehensive symptom assessment and that have been demonstrated to have adequate psychometric properties.
Conclusion
HF is a clinical syndrome which manifests a variety of symptoms. Symptom assessment and management are imperative to monitor the progress of illness and the impact of symptoms on outcomes. Symptom assessment is challenging as standardized symptom measures are lacking for HF patients. Because existing symptoms measures are at a relatively early stage, the information regarding the criteria that we modified to examine the quality of symptom measures is insufficient. More studies are needed to further validate existing HF symptom measures before one can be recommended for research and clinical use.
Footnotes
Declaration of conflicting interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.