
Abstract
Background:
Heart valve replacement surgery is undertaken to improve cardiac function and health-related quality of life (HRQoL). Mechanical valves are typically used for younger people (aged <65 years). Implantation of these valves comes with life-long health self-management requirements which potentially impact on HRQoL.
Aims:
The purpose of this study was to identify the short and long-term impact on HRQoL after mechanical valve replacement surgery.
Methods:
Multiple electronic databases were searched for peer-reviewed studies published between 2000–2013, which focused on patients who had mechanical valve replacement, aged <65 years, and used a valid measure of HRQoL.
Results:
Eight papers were included, all of which used the Short-Form 36 Health Survey (SF-36). Preoperatively, HRQoL was impaired, particularly in the SF-36 health domains of role-physical, physical-functioning, vitality and role-emotional. Postoperatively, most people had positive and sustained HRQoL improvement. In the early postoperative period all data showed significant improvement in at least four of eight health domains (physical function, role-physical, vitality, social function). Two-thirds of people also had significant improvement in an additional two health domains (general and mental-health). Whilst most people sustained HRQoL over time, one-third of younger adults (age <24 years) showed impairment in three domains (physical-function, mental-health and general-health).
Conclusions:
Mechanical valve replacement surgery results in important and sustained improvements in HRQoL. Future research should include investigation of HRQoL outcomes after mechanical valve replacement for specific groups such as younger adults and people in developing countries, and include evaluations of the potential impact of valve-specific factors and health self-management requirements.
Keywords
Background
The global incidence of valvular heart disease (VHD) is conservatively estimated to exceed 42 million people.1–4 VHD arises from congenital conditions, or more commonly originates as an ‘acquired heart disease’.1,5,6 Causes of acquired VHD include rheumatic heart disease (RHD), age-related calcification and degeneration, coronary artery disease, and connective tissue disorders.2,5,6 In developed countries, the primary causes of VHD are degenerative calcific changes and congenital conditions, whereas in developing counties, RHD dominates.1,7,8
A major difference related to VHD causation is the age of presentation: RHD generally becomes symptomatic in early adulthood, whereas degenerative/congenital changes commonly have a lengthy latent period worsening towards middle and later-life. 1 Regardless of cause, as VHD heart failure progresses, symptomology such as fatigue and chest pain, increasing medical surveillance and hospitalisations result in illness-related lifestyle limitations.1,7,9 Treatments may slow the rate of functional deterioration, however physiological and haemodynamic changes and/or heart failure progression eventually necessitate surgical repair or replacement of the damaged valve/s.1,10 Valve replacement surgery is indicated when the cardiac function associated with valvular deterioration results in symptoms and/or when there is angiographic or echocardiographic evidence of serious valvular impairment (e.g. increased mean valve gradient with set valve-specific criteria).1,10
Treatment interventions are dependent on the VHD pathophysiology but may range from minimally-invasive therapies such as balloon valvuloplasty, to traditional heart valve replacement surgery. Recommendations on the mode and type of intervention are based on evaluation of the type and level of valvular disease, the existing heart structure, age, life-stage and lifestyle.1,2,10 The patient choice of valve prosthesis includes weighing up the benefits and risks of both types. Mechanical valves have the advantage of durability but the drawback of lifelong anticoagulation therapy and associated frequent medical follow-up. Conversely, biological valves have few medical follow-up needs but have reduced durability, requiring re-intervention and/or replacement at a future time.1,10
Valve replacement guidelines have historically recommended mechanical valves for people aged less than 65 years. In recent times there has been a move to emphasise that prosthesis selection be guided by informed patient choice rather than determined by age and surgical opinion.10,11 Such decisions not only require careful consideration of the existing health state, and the advantages and disadvantages of each valve type, but also the patient’s personal preference based on lifestyle and expectations after surgery. Information on all aspects of living with a mechanical valve prosthesis, the effect on HRQoL, and HRQoL evolution over time, would optimally be provided as this is as an important factor in patient decision-making preoperatively, as is the more common risk data (mortality and morbidity).11–13 Furthermore, age has an effect on expectations of HRQoL and there is a need to provide information relevant to the individual’s age group which may be less than 65 years, or 65 years and older. 14
In contrast to the options available in developed countries, many developing countries where RHD is endemic have scant health resources and limited surgical access, consequently when surgery is available, and is a ‘one-shot-option’, mechanical valves are used.10,15–18 The concurrent lifelong anticoagulation required, along with additional needs such as RHD prophylaxis, may impact on HRQoL differently to those in developed countries. HRQoL may be further influenced in resource-poor environments where substantial efforts have to be made to obtain medical follow-up and access medications. 19
HRQoL
The impact of treatment/s on HRQoL is just as important as a component of effectiveness, as is improvement in symptomatology and functional status. 20 Recognising this, the American Heart Association (AHA) has recently included HRQoL evaluation as a strategic treatment- impact goal for cardiovascular health, 20 with HRQoL defined as the ‘discrepancy between actual and desired functional status and overall impact of health on well-being.’ (p. 2234) 11
The impact of treatments on HRQoL can vary on different aspects of a person’s life including physical, mental, and social health, therefore the World Health Organisation (WHO) recommends that multiple dimensions are measured. 21 Instrumentation with which to evaluate HRQoL exists in many formats but one of the most commonly used worldwide is the Short-Form 36 Health Survey (SF-36).11,14,20,22 This instrument incorporates 36 questions evaluating eight domains, which are both physically and emotionally based: physical functioning; role limitations due to physical health; role limitations due to emotional problems; energy/fatigue; emotional well-being; social functioning; pain; general health. 14 Raw scores on the SF-36 range from 0–100, with lower scores indicating worse HRQoL. Normative scores also exist for different populations where scores are scaled to a mean of 50, enabling easy visual interpretation of outcomes. 14 As many people have multiple health conditions there is often also a need to differentiate the specific impact which a condition, or treatment, may have. 23 To do this, a disease-specific instrument and/or disease-specific questions are recommended as adjuncts to the generic HRQoL instrument(s).22,24 In the context of mechanical valve replacement surgery, valve-specific items that may relate to life areas affected by implantation, such as audible valve click and life-long anticoagulation therapy, are necessary to augment a generic HRQoL in order to fully understand the HRQoL impact of treatment. 23 It is important also to measure HRQoL over time as not only do treatments and conditions vary but also HRQoL is an evolving and subjective state. 13 For instance, the effects of valve replacement on HRQoL are likely to vary within different health domains over time because of the patient’s variable health state preoperatively, the age and life-stage at time of surgery, the nature of the surgery and longer term self-management requirements. 25
Method
Aims
The aim of this review was to identify early and late HRQoL outcomes following mechanical valve replacement surgery. This information will help to inform patients regarding their likely HRQoL following surgery and identify areas and times in the operative course where additional support is needed. The specific focus is on those aged <65 years. A secondary aim was to determine if there were differences in HRQoL between patients in developed and developing countries.
Design
Initial searching of the literature identified evidence informing HRQoL for valve replacement surgery that arose from a range of study designs. Consequently, an integrative literature review method was selected. An integrative review methodology is an approach that facilitates synthesis and analyses of diverse methodologies as a mechanism for generating new perspectives on a topic. 26
Search methods
The databases OVID Medline, PsycINFO (OVID), PubMED, CINAHL (EBSCO), ProQuest Health and Medicine, and the Cochrane Library (Wiley) and Google Scholar were searched using MeSH terms from PubMED along with additional terms. All databases were searched using the terms: ‘cardiac valve replacement/surgery’, ‘mitral valve replacement/surgery’, ‘aortic valve replacement/surgery’, ‘health-related quality of life’, ‘heart valve prosthesis’ OR ‘heart valve prostheses implantation’. LJTM conducted the search and RDG later replicated the search and checked the number of papers included to validate the process. Following this, an ancestry search of the reference lists from papers sourced was also undertaken.
Inclusion and exclusion criteria
The criteria for inclusion of papers were: (a) original English-language papers; (b) peer-reviewed, and (c) published between January 2000–April 2013. Papers were excluded if: (a) HRQoL outcomes were not reported numerically; (b) HRQoL outcomes were undifferentiated by prosthesis type; (c) a validated HRQoL instrument was not used, and (d) exclusively focused on people aged over 65 years. Twenty-four articles were identified as potentially relevant based on applying the inclusion and exclusion criteria to the abstracts. Each article was then evaluated in full, for inclusion and methodological quality, by two independent reviewers (LJTM and RDG) and a third reviewer (DWS) made a final decision when differences occurred (Figure 1). Of the 24 papers, nine were excluded as HRQoL was not reported for mechanical valves separately, four were excluded because HRQoL results were only reported graphically and three papers focussed on a specific, complex surgical process related to the mechanical valve replacement. Eight papers met the inclusion criteria (Figure 1).
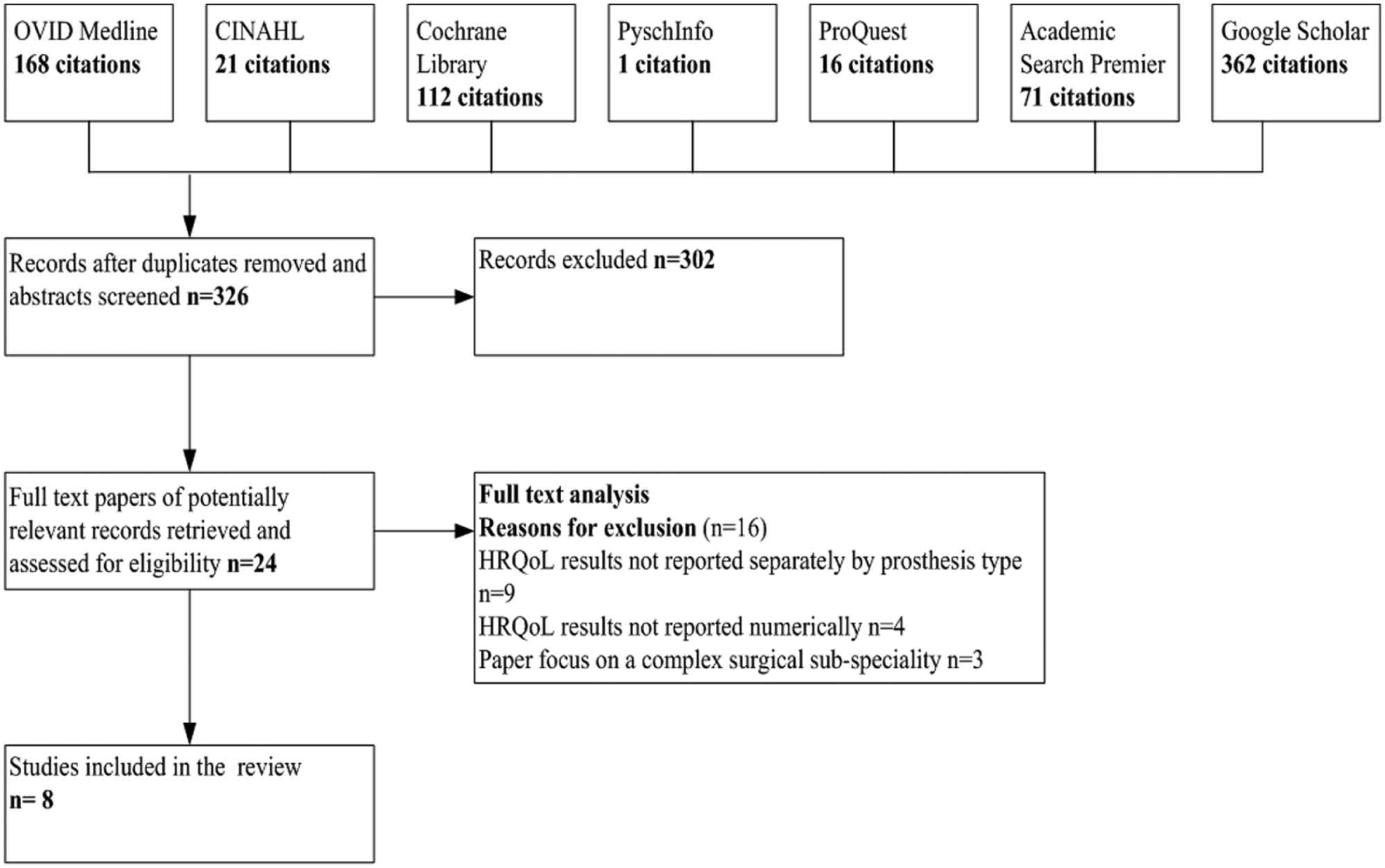
Results of systematic review process.
Quality assessment
The relevant sections from the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) study 27 and the Critical Appraisal Skills Programme (CASP) tools 28 were applied for quality evaluation. The STROBE and CASP tools incorporate instructions and a checklist of questions that facilitate systematic evaluation of the methodological quality of a study’s design and reporting. Based on STROBE/CASP criteria, all included studies were considered to meet methodological rigour (Table 1).
Quality evaluation of included studies (amended from Critical Appraisal Skills Programme (CASP) and Strengthening the Reporting of Observational Studies in Epidemiology (STROBE)).
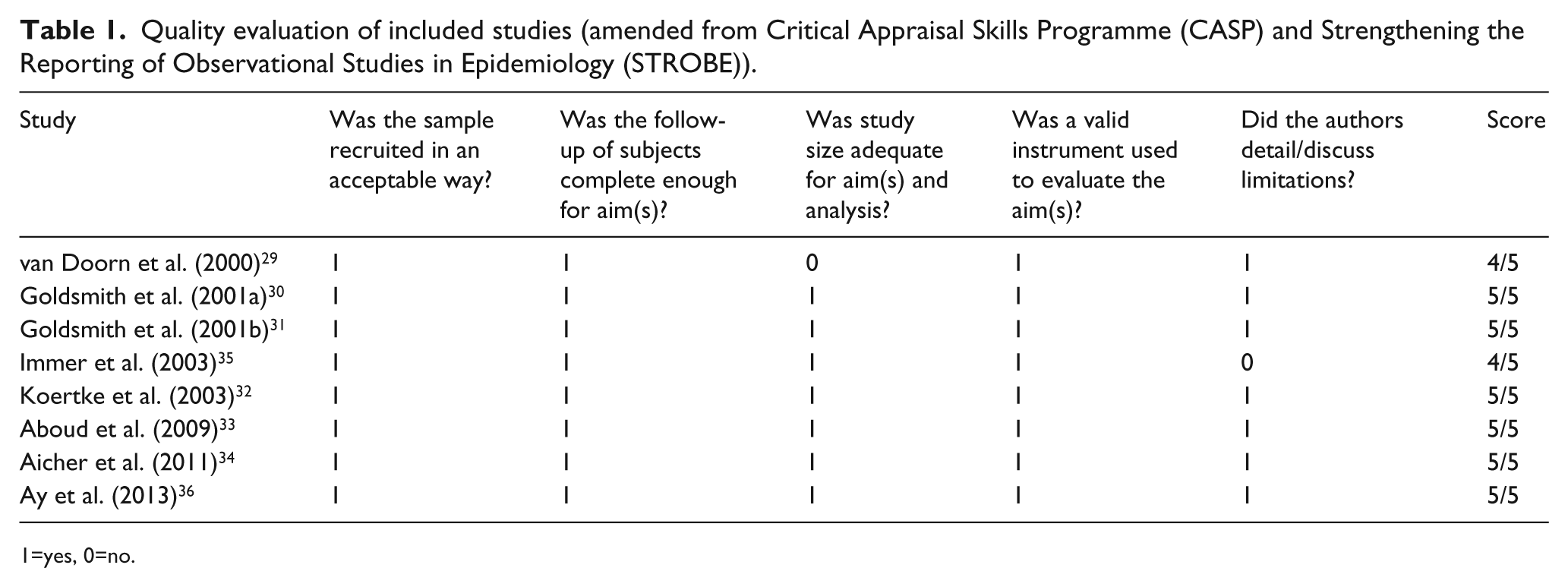
1=yes, 0=no.
Results
Sample sites and designs
All eight studies were conducted in developed countries with three set in the United Kingdom (UK),29–31 three in Germany,32–34 and one each in Switzerland 35 and Turkey 36 (Table 2). No study was found that was conducted in a developing country. Data for one 33 of the eight studies were collected from three sites; the remainder were single-site studies. The research designs varied and included prospective observational,30–32,36 cross-sectional,33–35 descriptive 29 and longitudinal 32 studies. Study timing was categorised as ‘preoperative’, ‘early postoperative’ (up to six months postoperatively) and ‘late postoperative’ (greater than six months postoperatively).
Key characteristics of included studies.
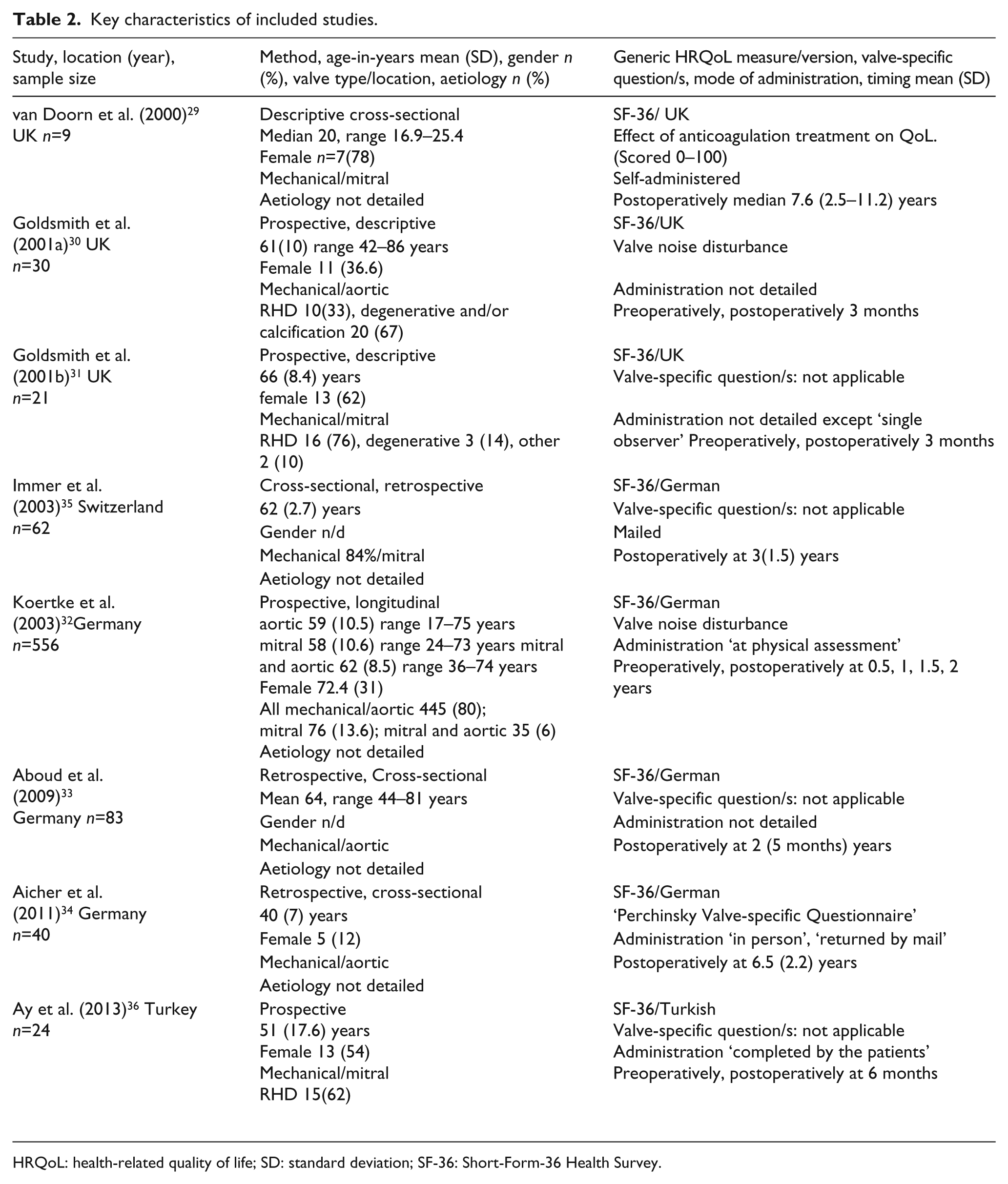
HRQoL: health-related quality of life; SD: standard deviation; SF-36: Short-Form-36 Health Survey.
Sample sizes and participant characteristics
Four studies30–32,36 included preoperative data collection, three studies30,31,36 evaluated during the early postoperative period and five studies32–35,37 evaluated HRQoL in the longer-term with the longest follow-up time being six years (Table 2). A total of 826 participants were included in the eight studies. Sample sizes varied from n=9 29 to n=556. 32 Seven30–36 of the eight studies had comparable data (i.e. all reporting mean values) and the mean age of these participants ranged from 40 34 to 66 years. 31 In the eighth study, 29 age was provided as a median of 20 years (range 16.9–25. 4 years). Six studies29–32,34,36 (total n=685) detailed gender proportions, with individual study proportions of females ranging from 12% (n=5) 34 to 78% (n=7). 29
Most participants had their aortic valve replaced (n=598, 72%), with over a quarter (n=197, 29%) having their mitral valve replaced and a small number (4%, n=35), having simultaneous aortic and mitral valve replacement. Whilst the aetiological reasons for valve replacement were detailed in three studies30,31,36 this only accounted for 9% (n=75) of the total population and consequently not reported here.
HRQoL measures
All studies used the SF-36. Goldsmith et al.30,31 also used the ‘Change in Health’ question supplied as a component of the SF-36. Normally, this question asks participants to compare current health to perceived health 12-months previously: Goldsmith et al.30,31 used this within the context of health perceived at three months postoperatively compared to preoperatively.
Mechanical valve issue questions aimed at determining the specific impact of having a mechanical valve on HRQoL were used in four studies29,30,32,35 and aspects assessed included anti-coagulation therapy, regular venepuncture, valve-noise and residual scarring from operative approach. Two of these studies29,32 also examined the relationship between the valve replacement surgery-disease-specific responses and HRQoL domains.
Preoperative HRQoL
Preoperative HRQoL was measured in four studies30,31,32,36 (Table 2). These data showed that many patients perceive their HRQoL as impaired. The lowest scoring domains were role-physical (mean=24), physical function (mean=43), vitality (mean=41) and role-emotional (mean=39). The highest scoring domains were bodily-pain (mean=62) and mental-health (mean=63). Whilst there was consistency between studies, across all domains, three of the lowest-scoring domains had a wide ranges: role-physical (range: 15–32), physical-function (range: 28–54) and role-emotional scores (range: 25–49).
Early (three–six months) post-operative HRQoL
Three studies, all on isolated valve procedures, measured and compared preoperative HRQoL to early postoperative HRQoL.30,31,36 Whilst all HRQoL domain mean-scores demonstrated positive change (Table 3), this reached statistical significance (p< 0.05) consistently across all studies in four of the eight domains (physical-functioning, role-physical, vitality and social-functioning). Goldsmith et al. 31 and Ay et al. 36 also identified significant improvement in the domains of general-health and mental-health with the Goldsmith et al.30,31 studies additionally finding significant improvement in the role-emotional domain. HRQoL domains showing no significant change were bodily pain for Goldsmith et al.30,31 whereas for Ay et al. 36 this was role-emotional. The SF-36 ‘change-in-health’ question was a component of the Goldsmith et al studies30,31 with responses indicating that the majority of patients have a significant improvement in their overall health postoperatively (p<0.004).
Mean health-related quality of life (HRQoL). Short-Form 36 Health Survey (SF-36) scores by domain and time-period.
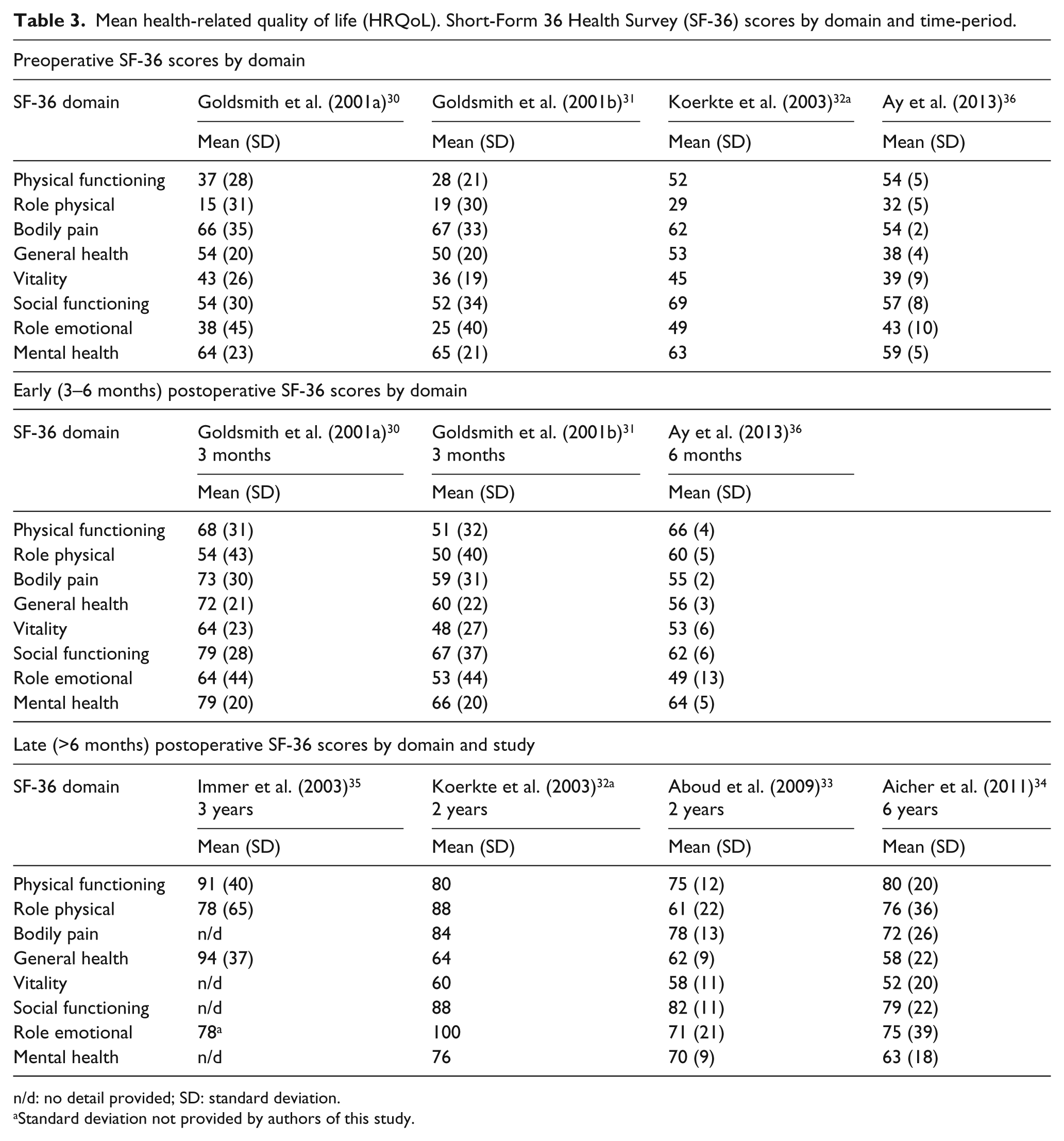
n/d: no detail provided; SD: standard deviation.
Standard deviation not provided by authors of this study.
Comparing early HRQoL by study location and valve position, recipients of aortic valves in the UK 30 had significant improvement in seven of eight health domains (p<0.05). In contrast, the mitral-valve recipients in the (UK 30 and Turkey 36 had significant improvement in only five of eight domains. The mitral-valve sample in the UK had no significant improvement in general or mental-health, whereas for the Turkish mitral-valve sample, the opposite was true. The Turkish mitral-valve sample then fared poorly in role-emotional but the UK mitral-valve sample significantly improved in role-emotional. All of the studies at this time point had similar gender composition (11–13% female) however, the Turkish sample had a much younger mean age (51 years) than either the UK aortic (61 years) or UK mitral (66 years).
Late (greater than six months) postoperative HRQoL
Five studies29,32–35 reported late HRQoL, with outcomes appearing to show that postoperative HRQoL improvements are sustained over time for most people (Table 3). The highest scoring domains differed across studies. Immer et al. 35 reported the highest scores in the domains of physical-function (mean=91) and general-health (mean=94) and Koerkte et al. 32 reported the highest scores in role-physical (mean=88) and role-emotional (mean=100) domains. In one study 29 there was some evidence to suggest that late HRQoL for younger adults (16–24 years) 29 was impaired up to seven years postoperatively with the domains of physical-function, mental-health and general-health, for one-third, being below the norm of the age and gender-matched reference population.
Preoperative and late HRQoL outcomes were measured in one study but the differences between the two time points were not tested for statistical significance. 32 Nonetheless, Koerkte et al. 32 results showed considerable mean domain improvement across all domains at two years compared to preoperatively (Table 3). The greatest observable postoperative improvement was in role-physical (29 vs 88) and role-emotional (49 vs 100).
Valve-specific issues
Two papers investigated the effects of mechanical valve-specific aspects post mechanical valve replacement and these were related to anticoagulation 29 and valve-related noise. 32 Anticoagulation requirements were investigated by van Doorn et al., (2000) using an author-created questionnaire in similar formatting and question style to the SF-36. The authors concluded that the impact on overall HRQoL from anticoagulation-related tasks such as daily tablet taking, blood-tests, and medical visits, was minimal for younger adults 29 . Koerkte et al. 32 looked at the association between valve noise disturbance and HRQoL up to two-years post-operatively. At six months, a small number (10%, n=54) of patients were sufficiently disturbed by valve noise for this to negatively impact HRQoL, however, this had halved (5.4%, n=30) by two years postoperatively. Importantly, the patients who remained disturbed by valve noise at two years also had significantly (p<0.05) impaired HRQoL scores across all SF-36 domains, compared to those who were less disturbed by valve noise. 32 Analysis in this study indicated that people aged 60 years or less, had an 8.2% additional risk of heightened noise perception; being female had an independent 11% risk but being female and younger than 60 years resulted in a risk factor of 17.1%.
Discussion
The intent of this integrated literature review was to identify the overall HRQoL outcomes after mechanical valve replacement surgery, in the short and longer-term. The results of this review highlight that, whilst preoperative VHD can have a pronounced negative impact on HRQoL, undergoing mechanical valve replacement surgery will, for the most part, improve HRQoL with this improvement being sustained over time. However, the results from this review also indicate that greater understanding is required for specific aspects of HRQoL, including the effect of age, and in particular for patients undergoing mechanical valve replacements in developing countries. An intention in the original aim of this review was a focus on research in developing countries, however, no studies conducted in developing countries was found. This highlights an important knowledge-gap and future research should endeavour to address this.
Despite the limited studies available comparing HRQoL for age, results from two studies suggest that younger age is associated with less improved HRQoL.29,32 Younger age has long been identified as a predictor of a poorer perception of HRQoL including in cardiac populations.23,37,38 Consequently, the association between younger age and less improved, or even impaired, HRQoL outcomes is not an unexpected finding from this review. Younger age (<60 years) was associated with heightened noise perception which had a negative impact on all domains of HRQoL. 32 In a separate study, 29 a third of younger adults sustained impaired HRQoL in three of eight domains, although these results are from a very small sample and require further exploration. In a recent study 37 exploring why HRQoL is better in older rather than younger patients with heart failure, it was noted that older people contextualise how they are currently feeling with an attitude of ‘it could be worse’. This is despite the older people generally being in worse physical states and with poorer prognosis. 37 The study authors concluded that older people have the ability to reconceptualise their expectations of HRQoL and living with heart failure better than younger people because of their more adaptable psychosocial status, and lesser levels of anxiety and depressive traits. 37
Further conclusions relating to age, were limited by the decision to exclude studies specifically focused on older people from our review. Comparisons were made even more difficult because three31–33 of the eight studies included patients aged over 65 years.
There is scant literature on differences in postoperative HRQoL by valve position. Grady et al., in 2011, investigated HRQoL of isolated cardiac procedures using the SF-36 and conducted analysis by valve (aortic or mitral) position. 38 However, these authors included repairs and replacements in each of the valve position groups and used the SF-36 composite scores rather than domains. This may explain the opposite findings to the studies included in our review, with mitral valve patients faring significantly (p<0.003) better in physical component scores at each of five time-points out to three years than aortic patients, but with no differences between valve position groups on the mental composite scores. 38
Longer-term HRQoL outcomes demonstrate that improvement after mechanical valve replacement surgery is sustained over time with many people showing continued HRQoL improvement rather than plateauing or declining. The stability of improved HRQoL over time does not appear to be unique to mechanical valve replacement patients. A study of 2524 isolated cardiac surgical procedures (including coronary artery bypass grafting and mitral or aortic repairs or replacements) by Elliott, Lazarus & Leeder (2006) found that whilst significant improvement occurs in HRQoL during the first six months, HRQoL then stabilises over the subsequent two years. 39
Although mechanical valve replacement surgery improves overall HRQoL, there is an associated need to evaluate the effect of mechanical prostheses-specific aspects. Interestingly, there seems to be little discourse surrounding the exchange in health status that occurs with implantation of a mechanical prosthesis, which limits the opportunities for patients to make an informed choice about treatment. Whilst a deteriorating chronic condition (valvular impairment) has been corrected with surgery, the mechanical valve-prosthesis implantation means that the postoperative health status remains that of a chronic health condition, albeit with different management needs. Two-thirds of studies included valve-specific questions indicating that clinicians recognise that aspects associated with valve implantation may be of concern to patients. Many of the valve-specific questions diversified from health self-management requirements (impact of regular blood testing, medical visits, and daily medication) to include topics such as patient satisfaction with the surgery and the effect of sternal scarring, to the perception of valve noise. Exploration of these elements provide descriptive information that may be important to patients but the absence of correlations to HRQoL scores, make it difficult to evaluate if there is a measurable related effect on HRQoL.
Two studies, Koerkte et al. and van Doorn et al., did analyse valve-related issue question-responses against HRQoL scores.29,32 Interestingly, the health self-management needs relating to ‘anticoagulation-taking, monitoring and medical surveillance’ did not correlate to impairment in HRQoL in young adults. 29 This is the opposite of findings from a critical literature review of 28 HRQoL studies investigating postoperative HRQoL outcomes for elderly people. 23 Those authors compared HRQoL by valve type (biological versus mechanical) and identified that the greatest influence on HRQoL was not age or valve type but instead was ongoing anticoagulation treatment and noise disturbance from the clicking valve. 23 Further investigation in a larger sample of younger people on anticoagulation is warranted. Conversely, for Koerkte et al., the perception of valve noise disturbance was associated with a negative effect on HRQoL across all domains for 10% of people, with younger age and female gender being identified as risk factors – both for experiencing valve noise disturbance and having it negatively affect HRQoL. 32 The findings related to valve noise are at odds with the results of the aforementioned critical literature review which highlights the need for identification of independent predictors of impaired HRQoL for mechanical valve replacement patients.
There was a noticeable lack of information which identified the people at risk of impaired HRQoL after mechanical valve prosthesis implantation. To some extent, this was due to small samples sizes and individual study focus. Most studies had alternate aims that happened to include a sample of people with mechanical prosthesis – rather than these people being the primary focus. Three studies sought to identify independent predictors of HRQoL but either combined mechanical and biological prostheses for this type of analyses,30,31 sought predictors for other reasons such as valve-noise perception, 32 or analysed mechanical prostheses against valve repair. 30 Exploration of the impact on HRQoL of core sample characteristics such as age or gender is scant, with only one study 32 evaluating and identifying age and gender as risk factors for valve noise disturbance, as noted earlier.
Importantly, very few studies have reported on HRQoL outcomes for mechanical valve prosthesis, in younger to middle-aged adults who have different needs and lifestyle activities than the older age groups. The paucity of such information is of concern because it is important to know HRQoL outcomes by different age and lifestyles along with predictors of lesser improvement, in order to both facilitate individual preoperative prostheses choices as well as provide tailored support to those identified at risk of poor outcomes postoperatively.14,39
Several limitations were present. An important limitation was the quality of the methods of the individual studies which, overall, was not optimal. For instance, no study reported a sample size calculation so we were not able to determine if sample size was adequate for the analyses conducted. We note particularly the van Doorn et al. (2000) study SF-36 component, only had a sample size of nine 29 . A further limitation of this review is that in comparing SF-36 scores between different samples, these samples were not divided into age and gender subgroups, therefore caution should be used when interpreting these findings.
Conclusion
Valve replacement surgery, using mechanical prostheses, improves patients’ perceived HRQoL in both the short and longer-term. However, there are gaps in our understanding. Currently there is a scarcity of HRQoL evaluation of outcomes after mechanical valve replacement surgery for people in developing countries, younger adults and adults at different life-stages. Concurrently, there is limited investigation regarding the possible influences of gender, valve position, and ethnicity along with the valve-specific factors such as anti-coagulation, and RHD prophylaxis on HRQoL.
Footnotes
Conflicts of interest
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Standard cardiac-education information given to valve-replacement patients includes information that they will be ‘back to normal’ by three months postoperatively, including resumption of work and leisure activities. Results from HRQoL studies provide tangible evidence which is important for patient education and discharge support. Detailed information on the impact of potentially negative aspects of living with a mechanical heart valve (e.g. valve clicking) is required to better prepare patients pre and postoperatively. Researchers need to augment generic HRQoL instruments (such as the SF-36) with valve-specific questions in order to identify if factors, such as wound scarring, valve noise and health-self management needs, have an effect on HRQoL. Younger mechanical valve replacement patients and patients in developing countries may have different needs and concerns. Further research is warranted to provide evidence-based detail important for patient preparation and preoperative decision-making.