
Abstract
Background:
Discharge planning is important to bridge the gap between hospital and home. Many patients with chronic heart failure are often fragile elderly with co-morbidities and functional decline due to increased symptom burden. A structured Gothenburg person-centred care (gPCC) approach may promote better discharge-planning.
Aims:
To evaluate whether proactive care-planning based on the gPCC model leads to improved efficiency in discharge procedures compared with usual care in patients hospitalized for worsening chronic heart failure.
Methods:
In a controlled before-and-after design, patients hospitalized for worsening chronic heart failure were assigned to either a usual care group or a gPCC intervention group. The patients’ social situation, their discharge destination and the number of days until the discharge were recorded. The time interval (in days) between notification and start of coordination of care was recorded.
Results:
In total, 248 patients were included, 123 in the usual care group and 125 in the gPCC intervention. During hospitalization, notifications to the community home help service and/or round-the-clock home nursing care services were more frequent in the gPCC-group (33.8%) compared with patients in the usual care group (12.1%). A confirmed discharge planning conference started within the first five days in the gPCC group whereas the usual care group ranged from one to 28 days. Compared with the usual care group, the gPCC group had fewer days in hospital (11 versus 35) ready for discharge.
Conclusion:
gPCC improves discharge processes because patients are viewed as competent to be involved in planning their subsequent care.
Introduction
After hospitalization, many patients need a period of recuperation, but some patients are fragile and not able to recover on their own. For that reason, coordination of continued care and support at home is a growing area of focus in both research and policy making. Hence, discharge coordination and planning is an increasingly important task in order to make the transition from hospital to home more effective. Where the discharge planning process fails to identify and/or address a patient’s care needs, the risk of hospital readmission is elevated and hospital length of stay is often longer.1,2 The discharge process requires multidisciplinary collaboration, and the patients themselves should have the option of being active in the process. 3
In a quasi-experimental study encouraging patients and caregivers to participate in the transition from hospital to home, Coleman et al. 4 reported a 50% decrease in re-hospitalization rates at 30-, 90- and 180-day intervals. They also reported that patients felt more confidence in self-management and were more knowledgeable about warning signs that indicated a worsening health condition. 4 Bragstad et al. 5 found that not managing well in the long term after returning home from hospital was associated with patients coming home to an empty house and not having adequate home-care service. In other words, plans or preparations for daily life after discharge were not made during hospitalization but instead left completely dependent on sources of help outside the hospital. In a review of the effects of discharge planning, Shepperd et al. 6 concluded that a structured discharge plan tailored to the individual patient brings about reduction in hospital length of stay and readmission rates for older people admitted to hospital with medical conditions. Parker et al. 7 found in their review support for the concept that hospital discharge planning and coordination can have beneficial effects on subsequent readmission rates in elderly patients. They concluded that interventions provided across the hospital–municipal interface, both in hospital and in the patient’s home, showed the largest effect.
Routine collaboration between the hospitals and the municipalities was first introduced in Sweden in 1992 3 and comprised a three step procedure when patients needed formal help from the municipality in order to make the discharge as efficient as possible. The first step is a notification to the patient’s municipal home help service and/or round-the-clock home nursing care service during the initial admission process at the hospital. During the hospital stay, an assessment of the patient’s needs for support after discharge is performed. The second step consists of sending a notice describing the patient’s expected status at the day of discharge. This note can be sent at the earliest when the patient is to be discharged within five days or less. If the patient needs support, a discharge care conference will be performed in hospital. The participants in these meetings include: the patient, the responsible nurse in the hospital, the municipal home help service and/or the round-the-clock home nursing care service. The third step is when the patient is ready for discharge. The best way to conduct this collaboration systematically, without causing a delay of discharge, has not yet been demonstrated.
The Gothenburg person-centred care (gPCC) model provides a structured approach to person-centred care, where patients are partners in planning care both during the hospital stay and in primary-care service and municipal care.8,9 gPCC means a shift away from a model in which the patient is the passive target of a medical intervention to a model where a contractual arrangement is made involving the patient and often relatives as active partners in the care process. gPCC asserts that patients are persons and should not be reduced to their disease alone. Instead, their context, experiences, goals and wishes should be taken into account. 10 Results from studies using the gPCC model have, so far, shown positive effects such as reduced length of hospital stay, improved Activities of Daily Living (ADL) resources, and less uncertainty about the disease, treatment and care in the patients themselves.8,9,11 There have been attempts to understand the discharge process, to define what constitutes a ‘good discharge’, and to identify the most appropriate means of improving health, social and economic outcomes resulting from the process. gPCC is an attempt to contribute to this knowledge. The aim of the study was to describe and compare discharge processes in two care models, usual care and gPCC.
Methods
Participants
The sample for this study comprised 248 hospitalized Swedish patients with chronic heart failure (CHF) during the period of February 2008 to April 2010 and has been described by Ekman et al. 8 The study had a controlled before-and-after design, and the patients were consecutively enrolled. Participants allocated to the control group were enrolled in the study during February 2008 to April 2009 and received usual care, whereas the intervention group, who received gPCC, were enrolled in the study during May 2009 to April 2010. The usual care group served as a comparison group and also for mapping usual care at the hospital. Both groups were screened and included by the same predefined inclusion and exclusion criteria.
Recruitment of participants was achieved from five designated wards at the Department of Medicine at Sahlgrenska University Hospital/Östra in Gothenburg, Sweden. Patients seeking hospitalization with worsening CHF (mainly dyspnoea and/or fatigue) and with a prior diagnosis of CHF were screened. The patients were assessed by a specialized cardiologist before final inclusion, guided by the ESC guidelines 12 for diagnosing CHF. Patients were excluded from the study if one or more of the below mentioned exclusion criteria was present: acute myocardial infarction, chest pain and age <50 years, primary valvular disorder, severe concomitant illness (e.g. cancer) with survival expectancy <3 months, planned surgical intervention, cognitive impairment or unwillingness to participate. All eligible patients who fulfilled the inclusion criteria and received a final diagnosis of CHF (I 500–I 509) or cardiomyopathy (I 420) with no exclusion criteria were invited to participate in the study by trained research nurses (Figure 1).
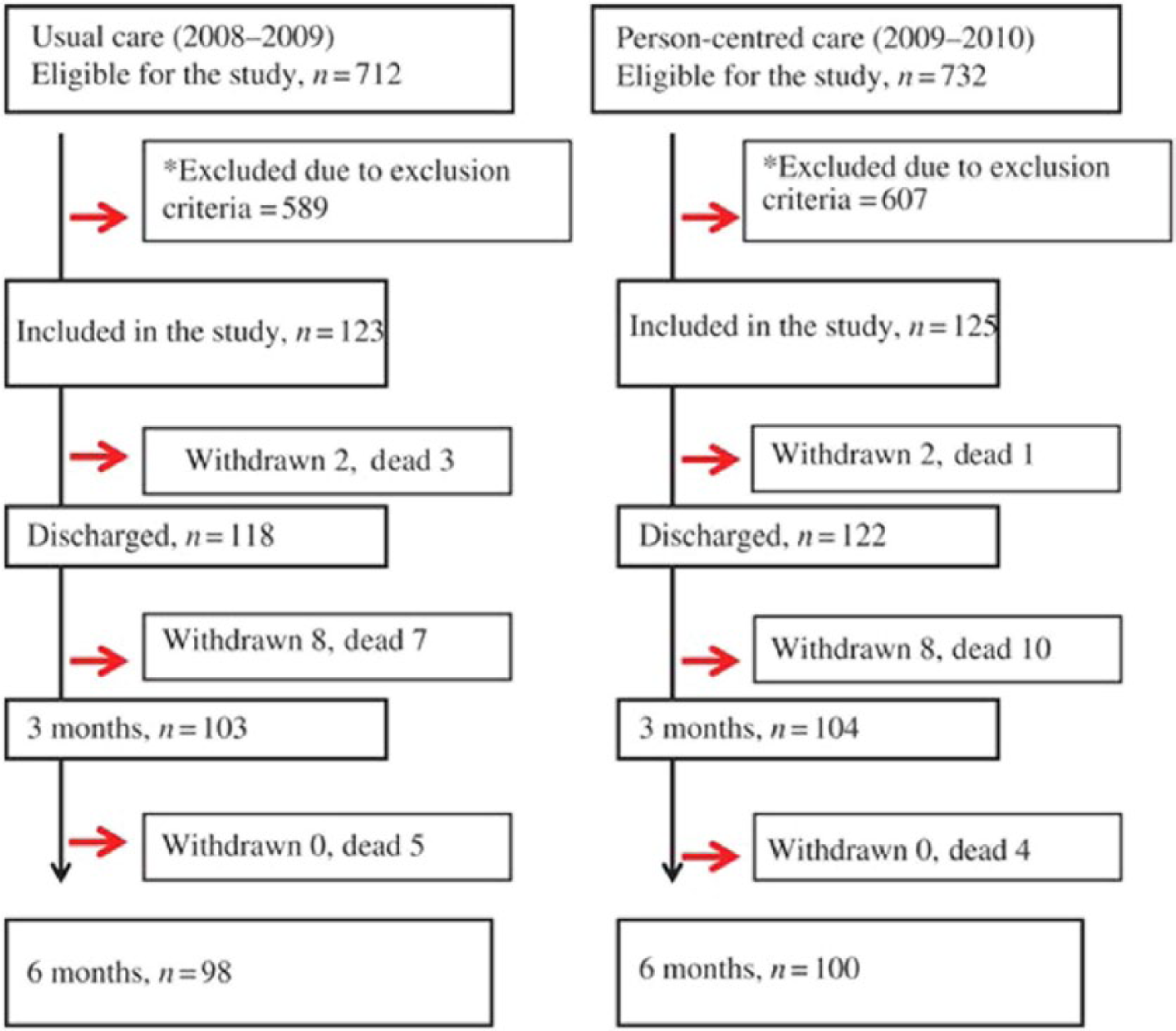
Study profile, participant flow.
Discharge routine in usual care
As described in the Introduction, a three step procedure was performed when patients needed formal help from the municipality. The discharge procedure for patients receiving usual care was not done in a systematic or timely manner. The discharge planning was decided by the individual nurse who cared for the patient and not based on predetermined measures.
Person-centred care intervention
The gPCC health plan8,10 starts with the patient narrative, which includes information regarding everyday life and symptoms prior to and during the worsening of the condition. In addition, the patient’s resources are identified, including motivations and goals. The social situation and the possible need for additional support at home after discharge from hospital are also of importance. Finally, within 24–48 hours, all information and facts are summarized and written in the gPCC health plan, which also includes planned investigations, treatment goals and length of stay at hospital.
Thereafter, the first notification can be sent to the patient’s municipal home care service and to the primary healthcare service, which is Step 1. The patient and healthcare professionals discuss the gPCC health plan and reach an agreement. The gPCC health plan is regularly evaluated (and if necessary, revised) in all aspects of care (such as symptoms, resources, management and treatment) by the patient and the healthcare professionals during the hospitalization. The gPCC health plan forms the basis for the second notice to the municipal home care service and to the primary healthcare service with an accurate and detailed description of the patient’s anticipated status (including for example symptoms and resources) at discharge, as well as any anticipated discharge planning conference in the hospital, which is Step 2. The third notice is recorded when the patient is ready for discharge, also in concordance with the gPCC health plan projected number of days of hospitalization, which is Step 3.
Measures
The first endpoint was the number of days from admission to Step 1, the first notice to the municipality, including the municipal home care service and the primary healthcare service. The second endpoint was the number of days from admission to the second notice to the municipal home care service and to the primary healthcare service confirming the discharge planning conference, or Step 2. The third endpoint, Step 3, was the number of days from admission to the notice to the municipality that the patient was ready for discharge from hospital.
Statistical methods
Continuous variables were described using means, SDs and medians, and comparisons between groups were performed using the Mann–Whitney U-test. Ordered categorical variables were analysed with the Mantel–Haenszel chi square exact test and described with frequencies and percentages. Relevant baseline variables that differed significantly between the two groups were adjusted (dyspnoea and New York Heart Association (NYHA) class level) for the analysis. All statistical tests were two-sided with a significance level of p ≤ 0.05. Adjustments for baseline covariates were performed by using logistic regression specifying the treatment group as dependent variable. The data were analysed using SAS version 9.2 (SAS Institute Inc., Cary, NC, USA), and IBM SPSS statistics version 20.
Intention-to-treat analysis included all patients who fulfilled all inclusion criteria above and no exclusion criteria. The per-protocol analysis excluded patients from the analysis if the gPCC health plan was not conducted by the healthcare professionals either within the first 72 hours or within each of the subsequent 48 hour periods designated for re-evaluations of the gPCC health plans until discharge.
Ethical approval
Ethical approval was given by the Regional Ethical Review Board in Gothenburg, Sweden (DNo. 046-08). All patients received oral information about the study and gave their signed informed consent. The study was approved by Regional Ethical Review Board and conformed to the principles outlined in the Declaration of Helsinki. 13
Results
In total, 123 patients in the usual care group and 125 patients in the gPCC intervention group were enrolled in the study as Intention-to-treat; however, only 74 patients received per-protocol treatment. Table 1 presents the patients’ demographics at admission to hospital. The mean age was 77 years in the gPCC group and 80 years in the usual care group. Patients in the gPCC group were more symptomatic compared with the usual care group, regarding functional status (NYHA class level, p=<0.01) as well as the level of breathlessness (p= 0.03). There were no differences in the numbers of co-morbidities between the gPCC group and the control group. With respect to ADL, the gPCC group showed a non-significantly higher level of dependency.
Baseline characteristics.
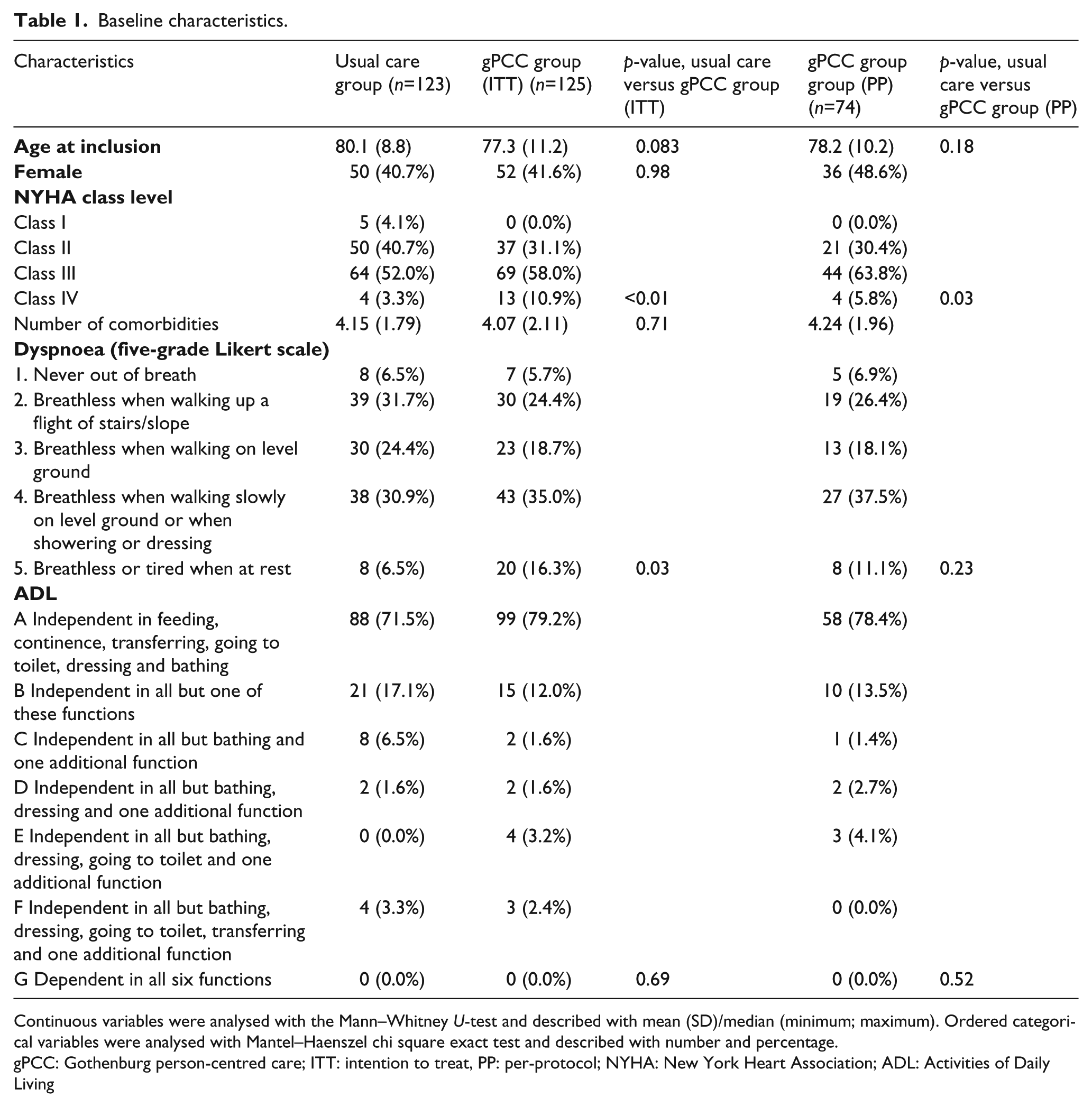
Continuous variables were analysed with the Mann–Whitney U-test and described with mean (SD)/median (minimum; maximum). Ordered categorical variables were analysed with Mantel–Haenszel chi square exact test and described with number and percentage.
gPCC: Gothenburg person-centred care; ITT: intention to treat, PP: per-protocol; NYHA: New York Heart Association; ADL: Activities of Daily Living
Prior to the hospital admission, most of the patients had a similar history of independent living, 93.2% in the gPCC group versus 93.5% in the usual care group (Table 2). Before admission to hospital, the gPCC group needed slightly less (32.4%) assistance in ADL and Instrumental ADL (IADL) than the usual care group (35.8). In comparison between the 74 gPCC patients and the 123 usual care patients, visits for round-the-clock home nursing care were more common in the gPCC group (18.9%) than in the usual care group (13.1%). During hospitalization, first notifications (Step 1) to the patients’ municipal home-care services and/or round-the-clock home nursing care services were more frequent in the per-protocol gPCC group (33.8%) compared with the usual care group (12.1%), but not significantly so. In addition, the notifications to municipal home-care services and/or round-the-clock home nursing care services were sent within two days in the gPCC group whereas the usual care group registrations to municipal home-care services and/or round-the-clock home nursing care services were delayed up to 14 days (Figure 2). During hospitalization, the number of days from admission to notices to the patients’ municipal home-care services and/or round-the-clock home nursing care services for confirmed discharge planning conferences (the second notification or Step 2) was significantly decreased (p=0.03) in the per-protocol gPCC group compared with the usual care group (Table 2). The discharge planning conferences in hospital were scheduled within five days for the gPCC group (range 1–5 days) whereas the timing of the coordinated care conferences in the usual care group was more dispersed, with a range of 1–28 days (Figure 2). The proportion of patients who were able to return to independent living was increased in the per-protocol gPCC group (95.9%) compared with the usual care group (90.6%) at discharge from hospital. The length of stay in hospital and the time to the third notification (Step 3) to the patients’ municipal home-care services and/or round-the-clock home nursing care services were significantly decreased: 6.77 days in the per-protocol gPCC group compared with 9.22 days in the usual care group (p<0.01), and 11 days in the per-protocol gPCC group compared with 35 days in the usual care group (p=0.01), respectively (Table 2).
Baseline housing, round the clock home-nursing, municipal home-care service and differences in discharge planning in hospital.
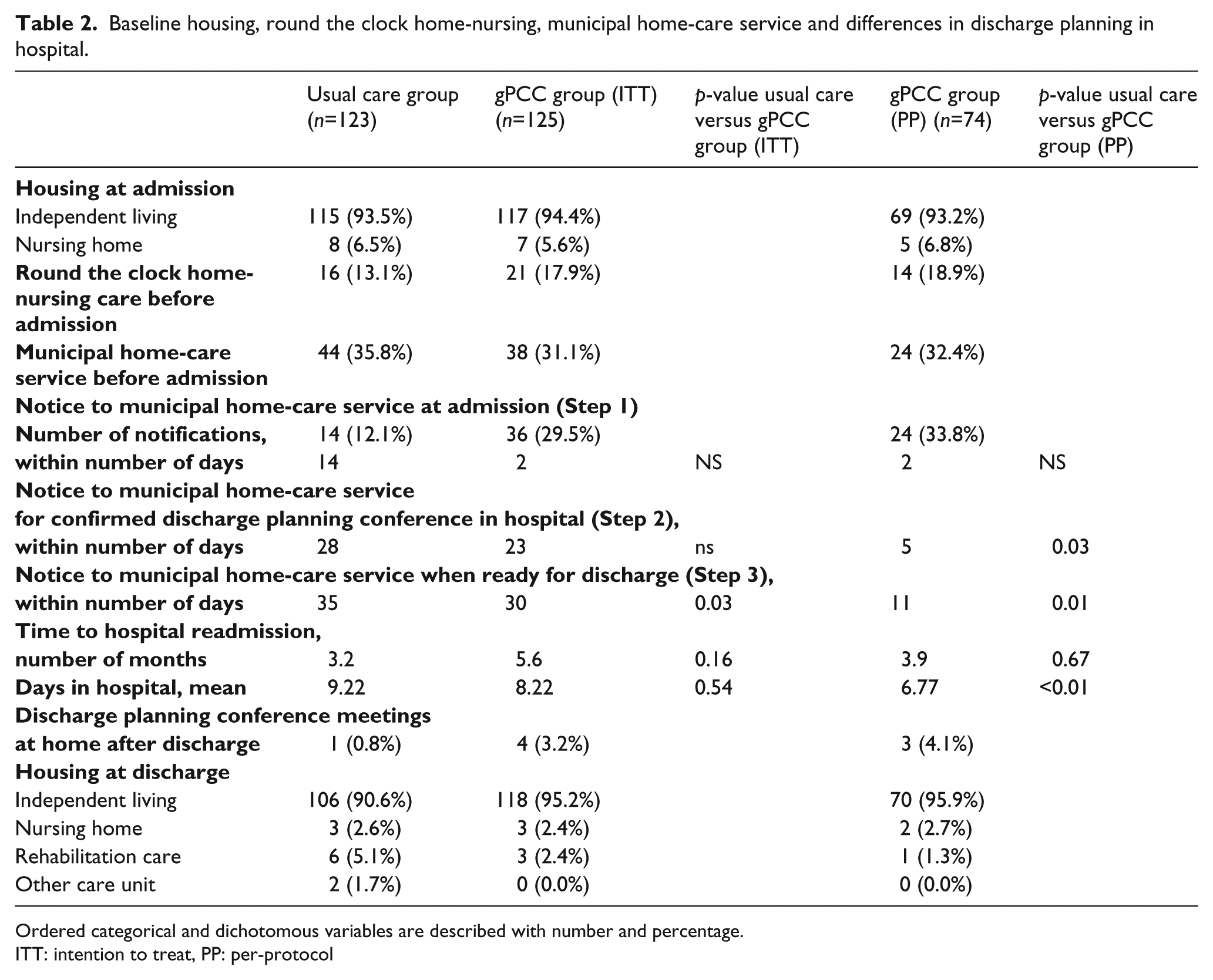
Ordered categorical and dichotomous variables are described with number and percentage.
ITT: intention to treat, PP: per-protocol
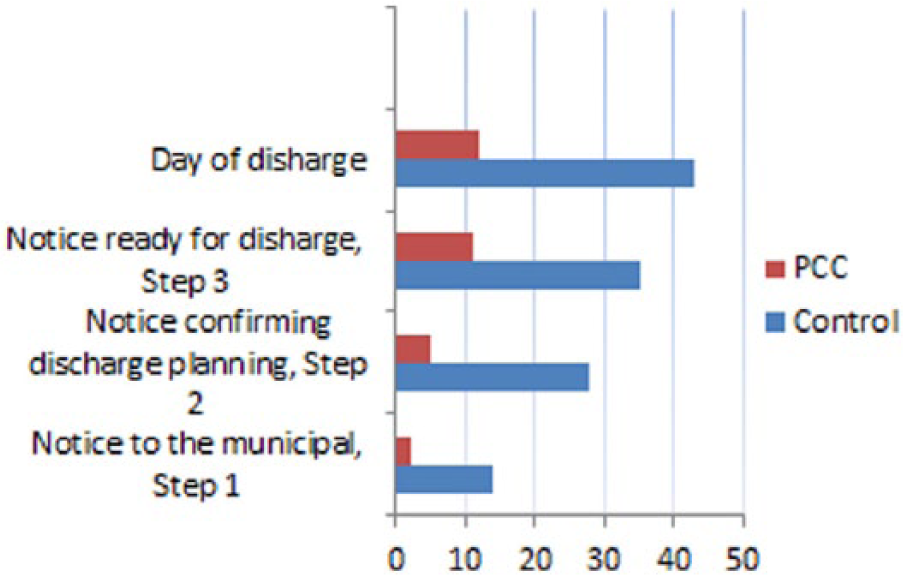
Main components in the discharge process. Maximum numbers of days in hospital.
Discussion
The main finding in the present study was the difference in timing of the important components of the discharge process between per-protocol gPCC and usual care. The gPCC model (including the admission process and the three steps in the collaboration process with the municipal home-care services and the round-the-clock home nursing care services) followed in a systematic and timely manner resulted in shorter lengths of hospital stay. In the gPCC model, the partnership was in focus from the start, meaning that not only medical information was gathered but also information about the patient’s perception of the situation at home and activities in daily life. The gPCC structure facilitated the identification of the patient’s need and resources after discharge during an early stage (within 24–48 hours) in the hospitalization, which created an increased timeframe for the patient/relatives to be included in the planning of care also after discharge. The advantage of such discharge planning was in line with the study by Bragstad et al. 5 and by Holland et al., 14 who reported significantly improved patient-reported success in a well-organized discharge process.
A structured and person-centred admission and discharge planning was a vital link in the continuity of care for both patients and care professionals in the present study. Discharge from hospital may mean anxiety for frail older people and their relatives and informal care-givers, since they may feel rushed or poorly prepared for the situation at home. Moreover, patients and healthcare professionals are often not collaborating in the discharge planning, something that is more evident in elderly and vulnerable patients. 15 The advantage of the gPCC model is that the healthcare professionals and the patient/relatives create a partnership from the first days in hospital. By mapping the patient’s resources and needs within 48 hours from admission, a gPCC health plan is developed that includes a prediction of length of stay, and after discussing the gPCC health plan in a partnership with the patient, an agreement may be achieved. 8 This gives more time for planning and preparing the discharge, and decreases the possibility for mistakes in the planned support.
In the structured gPCC health plan, the need for formal support at home was identified at the first patient narrative in hospital, so that the first notice (Step 1) to the municipality care was sent immediately. The prediction of length of stay made it possible to send the second notice (Step 2) for the discharge planning conference to the municipal home-care service and/or round-the-clock home nursing care service earlier in the gPCC group compared with the usual care group. The ability to predict length of hospital stay owing to accurate and detailed information about patient resources, needs and motivation was most likely the main reason for the difference in the discharge process between the two care models. A common cause for delay in the discharge process is when patients are dependent in ADL and IADL.16,17 In the control group, the length of hospital stay was sometimes prolonged because discharge was not discussed until the physician brought up the issue. This uncoordinated discharge process may put unnecessary stress on both the patients and their relatives, who may be unprepared for the discharge. Bowles et al. 18 describes similar problems as the majority of patients discharged from the hospital were without post-discharge referrals despite the presence of several characteristics associated with the need for home care and risk for poor post-discharge outcomes. Bragstad et al. 5 found that the discharge process does not have to be more complicated or perceived as less good by patients with high dependent care needs. They also found that patients that present high dependent care needs reported satisfaction with the discharge, which was probably because the good planning compensated for the dependency. 5 Moreover, having someone at home upon returning from hospital and having adequate formal home-care services were significantly associated with good patient-reported outcomes in the long term after returning home from hospital.5,19 Additionally, Parker et al. 7 found in their review of outcomes of discharge that older patients consistently mentioned poor communication and consultation by staff, inadequate notice of discharge and little assessment of home circumstances.
The above-mentioned areas highlight the need for a structured admission where these issues are included in a systematic way. In the gPCC group, healthcare professionals were able to identify each patient’s motivation and resources from the patient narrative already at admission. Together, the patient and the healthcare professionals created a personal health plan that covered the care as well as the gap between the hospital and home. This allowed sufficient time to collaborate with the municipal home-care services and/or round-the-clock home nursing care services and also for the patient, their relatives/informal care-givers, and healthcare professionals to prepare the return to home in a safe, calm and proper way.
The present study has some limitations. It was a single centre study with patients diagnosed with CHF, which may not generalize to all patients with different diagnoses at different hospitals. However, regardless of which hospital and what diagnosis, it is necessary to provide a discharge process where patients are actively involved. 3 Another limitation was that 41% of the patients did not receive per protocol treatment according to the gPCC health plan. The reason for this as far as we understand was that the healthcare professionals simply fell back into usual care. In the study there were two trained research nurses who also supported the healthcare professionals, but they could not supervise the care round-the-clock. This is not a new phenomenon: in a recent study different working groups’ resistance to change was described, and the authors concluded that it is difficult to change routines in healthcare organizations.20,21 Moreover, the gPCC group was three years younger as well as more symptomatic than the usual care group. Despite having more severe symptoms at admission, more patients in the gPCC group were discharged to independent living in housing than in the control group.
Conclusions
gPCC means creating a partnership between patients and health professionals in planning and performing care. In hospital, this significantly improves the transfer process for patients with worsening CHF in need of municipal home-care services and/or round-the-clock home nursing care services. gPCC improves discharge processes because patients are viewed as persons who are competent to be involved in the planning of their care. The present finding contributes to the growing evidence that the gPCC is more effective than usual care.
Footnotes
Acknowledgements
We gratefully acknowledge Kerstin Frid, patient research partner from the Heart and Lung Association in Gothenburg and the Swedish Disability Foundation, for invaluable advice and assistance in this study, and Nils-Gunnar Pehrsson (PhD) for the statistical analysis.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This work was supported by the Centre for Person-Centred Care at the University of Gothenburg (GPCC), Sweden. GPCC is funded by the Swedish Government’s grant for Strategic Research Areas, Care Sciences (Application to Swedish Research Council no. 2009-1088) and co-funded by the University of Gothenburg, Sweden.
The Gothenburg person-centred care model facilitates healthcare professionals to identify and utilize patients’ resources. The Gothenburg person-centred care model improves the transfer process for patients with worsening chronic heart failure in need of municipal care services. Viewing patients as competent persons improves the discharge process because they are subsequently involved in the planning of their own care.