
Abstract
Cardiac diseases have direct and indirect effects on sexuality. Health care providers, especially nurses, have a major responsibility in addressing and discussing sexual concerns and providing sexual counseling needs for patients with cardiac diseases. Discussing sexual issues in Arabic Muslim countries is considered a taboo. Lack of information about sexual life can affect the quality of life for patients with cardiac diseases. In this study, concerns regarding counseling needs and sexual information pertaining to Jordanian patients with cardiac diseases are addressed. Non-experimental, cross-sectional, descriptive designs were employed, accompanied by a self-report questionnaire, as well as a structured interview using the Steinke Sexual Concerns and Sexual Activity questionnaires for cardiac patients. A convenient sample of Jordanian male and female patients with cardiac problems was recruited. Results revealed that only 11% of the participants with cardiac diseases reported receiving information regarding sexual life following cardiac-related events. Most patients (71%, F=81) preferred cardiologists to provide them with sexual information, and almost two-thirds of them (62%, F=75) considered nurses’ gender to be a barrier, preventing them from inquiring about their sexual life. Patients with cardiac diseases had sexual concerns, but none of incredible importance. However, most patients (76%, F=94) reported changes in sexual activities following cardiac-related events. Cardiac patients had sexual concerns and sexual counseling needs that they would not discuss. Health care professionals should arrange sexual counseling plans with the patient; as every patient has individual, specific, and unique sexual counseling needs, dependent upon their lifestyle, health conditions, and their type of cardiac disease.
Introduction
In Muslim countries, it is believed that God or “Allah” created human beings with inherent physical, psychological, sexual, social, and spiritual needs. Satisfying these needs is vital, in order to maintain a healthy state of equilibrium. Sexuality for example, is one of the human body’s most essential physiological needs; although, it is at the bottom of Maslow’s hierarchy of human needs. 1
Many diseases, such as cardiovascular disease (CVD), affect a human being’s sexuality and can yield negative consequences in a patient’s sexual life. Sexual dysfunction, sexual problems, and/or a decrease in sexual activity following any cardiac event, is evidenced in several studies.2–7 Fear is cited as a major cause of decreasing sexual activity in relation to patients with cardiac-related diseases and/or illnesses.5,8–13
Patients with cardiac diseases require information about different aspects of their new life.11,13 Although information concerning sexual needs is not considered to be a priority of cardiac patients,3,4 following recovery and a return to a normal sexual life, it could become one of the patient’s priorities. 6
Most cardiac patients complain of changes in their sexual life following their cardiac event. 14 These changes might lead to physiological disorders, as well as serious psychological problems, which could potentially affect the patients’ quality of life.8,9,14–18 In Jordan, there may be limitations that could prevent many patients from discussing their sexual concerns. Discussing sexual concerns and/or issues in certain societies is considered to be taboo,19–22 but in the Arab-Muslim Jordanian society the fear of being impotent may predominate over other fears, even fear of death. 23
Patients with cardiac diseases and/or illnesses reported many barriers in inquiring about sexual concerns and/or issues. The major barrier is embarrassment and shyness,23 –25 especially when the health care provider and the patient are of different genders.25,26 The health care provider must initiate the discussion regarding sexuality, in order to diminish cardiac patients’ embarrassment. 27
Health care providers, both physicians and nurses, are responsible for providing sexual information for patients, and they are the patients’ preferred source of information. Physicians, however, do not routinely discuss sexual issues with patients and, if they do, this is dependent upon the patient’s gender.23,25,26,28 Also, nurses do not perceive sexual needs as an essential part of their assessment of cardiac patients. 29 As far as the researcher is aware, there is no published study investigating the sexual information needs of Arab-Muslim cardiac patients.
The purpose of this study was to explore sexual-related concerns and counseling needs as they pertain to Jordanian cardiac patients. Specifically, the research questions were:
What are the sexual concerns and sexual counseling needs of Arab-Muslim cardiac patients?
Of the health care providers, from whom do patients desire to receive information regarding sexual counseling?
Do patients consider gender differences a barrier to seeking sexual counseling?
Method
Design
Non-experimental, cross-sectional, correlational, descriptive designs were used in the current study, utilizing self-report questionnaires and structured interviews. A descriptive design was utilized because very little is known about Jordanian cardiac patients’ sexual information-related concerns and counseling needs. With the lack of precedential studies, we needed descriptive studies to build up baseline data in order to develop a culturally suitable intervention.
Setting
The study was conducted in five governmental and two educational hospitals. Patients with cardiac diseases were approached in cardiac care units, medical floors, and cardiac outpatient clinics in these hospitals.
Sample
Non probability (convenient) sampling technique was used. We approached Jordanian male and female patients with any cardiac problems who met the inclusion criteria: being married before having cardiac problems, conscious, could understand Arabic, were willing and able to participate. Those who were illiterate and willing to participate were interviewed by the investigators and/or their assistants.
Data collection
Cardiac patients’ sexual concerns and counseling needs were measured using a questionnaire developed primarily for patients with heart failure which was modified to include patients with cardiac diseases in general.31,32 The questionnaire includes two major parts: the Steinke Sexual Concerns Inventory-General Cardiac Version and the Steinke Sexual Activity and Heart Disease Questionnaire. 32 The internal consistency of Steinke Sexual Concerns Scale-Heart Failure was 0.79, and test-retest reliability was 0.71. 31 Content validity was assessed by two nurse researchers experienced in heart failure and a cardiologist. 31 However, Cronbach’s alpha for Steinke Sexual Concerns Inventory-General Cardiac Version was 0.86. 32
The study tool originally was developed in the English language. It was translated into Arabic, the national language of Jordan, by a nurse with a PhD degree. Then the Arabic version was translated back to English by a bilingual person (PhD nurse and a Master’s degree nurse) following the back translation process. 33 A few modifications on the questionnaire were made according to the purpose of the study and Islamic and Arabic culture.
The questionnaire consists of five sections.
Chart information: including current diagnosis, length of diagnosis with cardiac problems, medications, and comorbidities;
Demographic data: age, gender, religion, educational level, employment level, the highest job title for the longest held job, total family income, and length of time having cardiac problems;
Sexual counseling: includes seven questions about features of sexual counseling provided for the patients with cardiac disease, one of these question is about the preferable person (cardiologist, physician, or nurse) to provide the sexual information, and another one is to explore if gender is a barrier that prevents patients from asking about sexual life; and question number seven is related to the patient’s perception of the sexual counseling needs; (d) The Steinke Sexual Concerns Inventory-General Cardiac Version section included 11 items related to patients’ sexual concerns using a four-point Likert scale. Of these questions; three assessed the patient and partners’ fear, three assessed the symptoms experienced by the patient during or after sexual activity, two assessed the presence of sexual dysfunction, and three assessed different sexual concerns;
The Steinke Sexual Activity and Heart Disease Questionnaire section included six questions about sexual activity, and one question about additional sexual concerns.
A pilot study was conducted in order to assess the reliability, readability easiness, and time required to complete the questionnaires and included 18 patients. The reliability for the modified Arabic version of the Steinke Sexual Concerns Inventory-General Cardiac Version, revealed Cronbach’s alpha of 0.90.
Approval was obtained from the Institutional Review Board (IRB) of Jordan University of Science and Technology’s (JUST) committee, Ministry of Health, and hospital administrators. Written informed consent was obtained from the patients. The investigator and assistants interviewed patients in a private place. Patients were assured that participation was voluntary, and that they could withdraw at any time, without any penalty. Furthermore, patients were informed that all their information would be both anonymous and confidential, and results would be reported in aggregate form.
Cardiac patients’ medical records were reviewed by the investigator and assistants, in order to look for eligible participants, and to collect chart information. Cardiac patients were approached by the investigator and assistants. Upon agreement, cardiac patients signed consent forms. Due to the sensitivity of the subject, male assistants approached men and the female investigator approached women. The assistants’ nurses were trained to use instruments before the data collection so as to assure consistency.
Data analysis
The Statistical Package for Social Science (SPSS) for Windows Version 17.0 was used for data analysis. Descriptive statistics and the chi-squared test were used to analyze the data. 34
Results
A total of 167 patients were approached. Of those, 29 patients refused; they were worried or anxious about hospitalization and the disease process. Only 138 patients agreed to participate, which represents a response rate of 83%. Fourteen questionnaires were excluded (13 questionnaires were incomplete, and one because the patient had the disease prior to marriage). Thus, the total number of patients was 124.
Demographics
All patients were Muslims and mostly males (72%, n=89), between 27–78 years old (M=55, SD=10). Most patients (63%, n=78) have been admitted to public hospitals, 75% (n=93) with a cardiac problem as their main complaint from as long as one to five years ago (40%, n=50). Additionally, 122 (98%) patients reported that they had one or more comorbidity and 57% (n=71) reported taking one or more medications. Table 1 shows patients’ demographic characteristics.
Patients’ demographic characteristics (n=124).
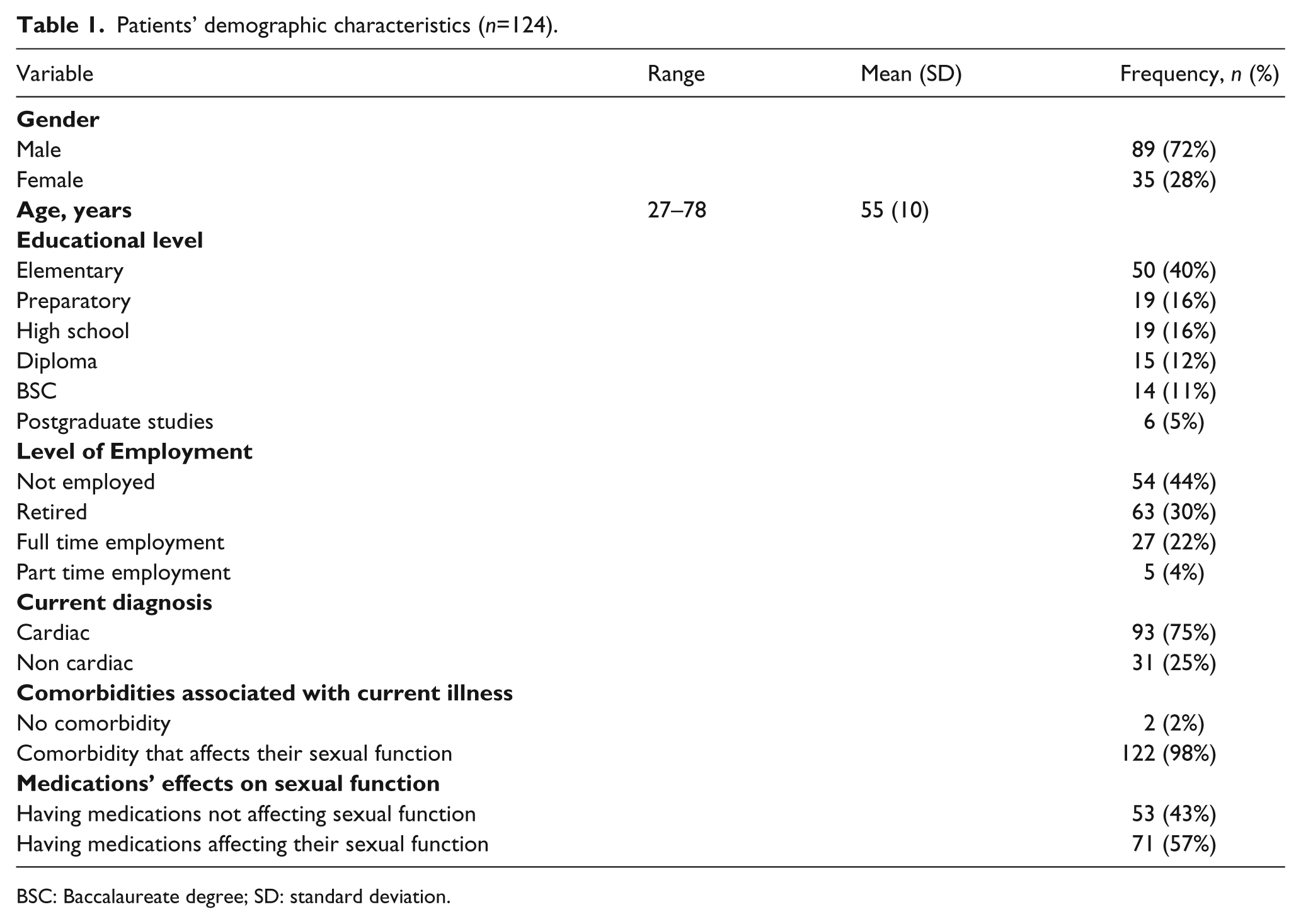
BSC: Baccalaureate degree; SD: standard deviation.
Cardiac patients’ sexual concerns
In the questionnaire, the responses were divided into three categories; however, to prevent the fragmentation of the results, a combination of the positive responses (responses of moderate and high concerns) were combined. Thus, the final two responses we have are whether the patients have concerns or have never had concerns. The results revealed that three-quarters of patients reported a lack of interest in sex (77%, n=96) and half of the participants had concerns related to the change in their relationship with their spouse (52%, n=64) since developing cardiac diseases. In addition, patients were concerned about their spouses’ fear of having sex (52%, n=65) and their spouses’ over-protectiveness (72%, n=89). Patients had a fear of having sex (61%, n=75) and a fear of a recurrent heart attacks if patients decided to have sex (60%, n=74). Physical symptoms with, or after, having sex were reported in terms of fatigue (80%, n=99), chest pain (69%, n=85), and shortness of breath (76%, n=94). Sexual problems were also reported as concerns, including difficulties in having orgasms (69%, n=82); and/or having erectile problems (64%, n=80) (Table 2).
Sexual concerns of cardiac patients (n=124).
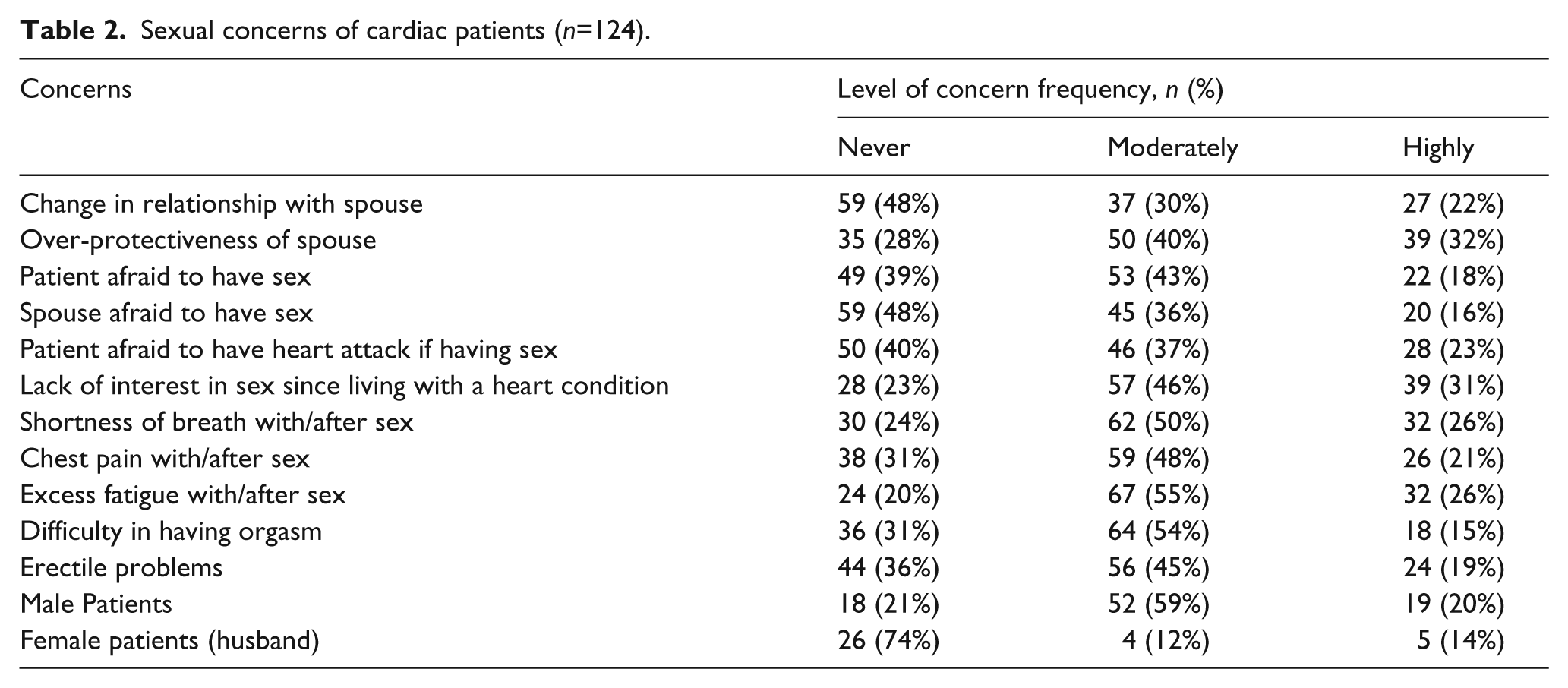
Additionally, there was a significant statistical decline change (χ2=6.7, df=1, p=0.009) in sexual activities regarding cardiac events. A majority of patients (76%, n=94) reported changes in sexual activities before and after having a cardiac problem. Physically associated heart problems (48%, n=30) were the most reported causes behind this change.
Patients’ sexual counseling needs
Cardiac patients ranked medications’ effect on sexual activity as the chief concern (68%, n=84) and sexual activity preparation the least important (10%, n=12) sexual counseling needs (Table 3).
Features of sexual counseling provided for the patients.
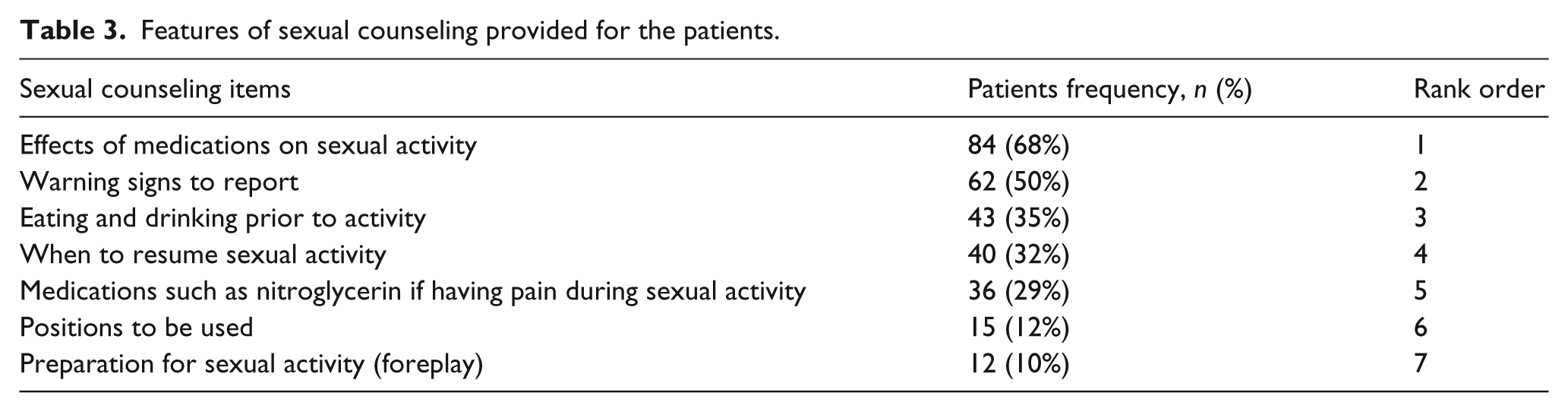
Features of sexual counseling provided to cardiac patients
Of the participants; 81 (71%) out of 114 patients (10 patients did not provide any information) preferred the cardiologist to provide education about sexuality. In addition, 75 (61.5%) of 122 patients (two patients did not provide any information) believed that nurses’ gender was a barrier that prevented them from asking about their sexual life following cardiac-related events. Moreover, 10.7% (n=13) reported receiving information about sexual activity and how it could affect their daily activities. Twelve of 13 patients reported receiving sexual counseling from the cardiologist (and one from a nurse); eight (67%) of 13 patients received information verbally and three (25%) patients received both verbal and written information (one patient did not state how he received the information, and one patient received a CD). The information was provided either for patients at hospitals (54%, n=7 of 13) or outpatient clinics (46%, n=6 of 13). The information provided was about a decreased frequency of intercourse, medication effects on sexual activity, warning signs of cardiac health problems, and whether to take medications, such as glyceryl trinitrate, if pain is experienced during sexual activity.
Discussion
Few cardiac patients reported receiving information about sexual activity and how it could contribute to complications following heart disease. Our results were congruent with previous studies as cardiac patients were either not informed at all, or inadequately informed, about sexual issues.12,14,23,31,35
Holistic care means providing sufficient information based on patients’ needs. 29 In our culture, it is embarrassing to discuss sexual activity. Some patients might not even be interested in receiving information about sexual activity. 36 Our current study results revealed that patients with cardiac diseases and/or illnesses who received sexual information received it either verbally or in writing. This is consistent with a previous study for patients with heart failure, 31 and a Swedish national survey conducted among cardiac health care providers in order to obtain knowledge on the sexual information type. 10 Verbal and written information are easy to provide and are always available. In our culture, however, discussing sexual information needs verbally is difficult and would not be acceptable for some patients; therefore, written materials would be both more comfortable and more effective. Understanding patients’ needs, giving patients the opportunity to express their needs, 29 and providing patients with written materials (booklet, pamphlet), videotape, CD, or even referring them to other health care professionals (patient’s cardiologist, fellow nurse specialists or sexologists) will solve many problems for the patients.10,37
The majority of participants stated that they received, as well as preferred to receive, sexual information from the cardiologist, believing that cardiologists are more knowledgeable. This is compatible with previous studies.31,38 On the other hand, it could be due to the fact, that nurses do not initiate a discussion about sexual concerns with the patients, since they lack the knowledge in counseling patients regarding the impact of illnesses on sexual activity,20,22,37,39 although they agreed that it is part of their assessment role.20,22,29
Sexual information that was provided by cardiologists for patients in the current study, which is from cardiologists’ perspective, as reported by patients, regarded the frequency of intercourse, medication effects on sexual activity, warning signs of cardiac health problems, and whether or not to take medications if experiencing pain during sexual activity. These items are vital. They concern a patient’s life and are easily discussed, as they are considered to be topics of general sexual information. It is not as nerve-racking or uncomfortable as discussing sexual positions and/or foreplay, topics that are considered to be extremely intimate and private.
A significant number of cardiac patients in the current study argued that gender was indeed a barrier, deterring patients from inquiring about any information regarding their sexual life. The number of patients who would accept discussing sexual issues with a stranger of a different gender, is expected to be very low.14,25,27,40 In the current study, contrary to what was expected, almost two-thirds of the participants perceived gender as a barrier, whereas we expected the number of participants to perceive gender as a barrier to be greater. This could be attributed to the average age of patients (M=55 years); many patients stated that there were no problems in discussing sexual concerns with a nurse of the opposite gender because they considered the nurse to be like their son or daughter.
Participants had concerns about all items included in the sexual concerns inventory. They perceived that all items were important. Over-protectiveness of the spouse was considered to be one of cardiac patients’ concerns, related to the spouse’s fear of having sex. Fear of having sex may be related to incorrect information provided for patients; whereby many patients rely on friends or relatives, with similar heart problems, to ask about sexual issues. Cardiac patients could also be afraid of dealing with decreased sexual performance. Sexual performance for men in the Arab culture is considered a vital point. Fear of impotency may predominate over the fear of death. 23 Furthermore, a lack of information about sexual life can cause a fear of having sex for the patient and/or their spouse. Surprisingly, the level of concern of our patients’ or spouses’ fear about having sex in the current study is considered quite high compared to an American study and an Iranian study. The American study revealed that the majority of heart failure patients were never or rarely concerned about the fear of having sex, while more than half of them were never or rarely concerned about their spouse’s fear of having sex 31 and an Iranian study showed that one-third of Coronary Artery Disease (CAD) patients experienced fear of sexual intercourse. 42 The percentage of patients with cardiac diseases in the current study, who were concerned about having a heart attack was congruent to a Turkish study, which showed that about two-thirds of Myocardial Infarction (MI) patients experienced a fear of a heart attack. 23 Additionally, most of Turkish MI patients considered fear of re-infarction to be the major reason for decreased sexual activity. 7
Our results also revealed that about half of cardiac patients’ relationships with spouses have changed. Couples should be assured by health care providers that they should discuss all sexual problems and concerns that could affect their relationship. The results of studies among American heart failure patients revealed that their relationships with their spouses were not or slightly changed,31,43 while in a study among Dutch heart failure patients; only a few patients reported changes in their relationships with their spouse as a result of the disease. 44
The study demonstrated that cardiac patients were concerned about physical symptoms associated with sexual activity such as fatigue, shortness of breath, and chest pain. Fatigue was ranked as the highest concern, while shortness of breath was ranked as the 3rd highest concern. Health care providers must address cardiac patients’ concerns about physical symptoms because patients could erroneously perceive these symptoms as a heart attack. These symptoms also depend on the cardiac disease, and the progress of the disease. For example, heart failure patients complain of fatigue and shortness of breath with minimal exertion.43,44 Conversely to the current study results, one study revealed that most heart failure patients were never, or rarely, concerned about physical symptoms of chest pain and/or fatigue, while half of them were never, or rarely, concerned about shortness of breath. 31 Also, few Turkish patients with MI complained of chest pain and dyspnea, while half of them complained of early fatigue in sexual activity. 23
Other concerns of cardiac patients were sexual dysfunctions. Two-thirds of cardiac patients had concerns about erectile dysfunction and difficulties in experiencing an orgasm. Reporting such a problem is rare, especially the erectile dysfunction, as it is difficult to admit the presence of such a problem among Arab men, as impotency affects his masculinity and manliness. Discussing such topics is culturally sensitive and could be a barrier. 21 Many studies reported that 37–50% of cardiac patients had experienced erectile dysfunction.3,6,7,45
Lack of interest in sex was ranked as the 2nd highest concern. It could be related to the fact that men and women of age are considered in the Arab-Muslim culture as being sexually inactive. They have no right in expressing such feelings, and if doing so, they will be strongly criticized. From society’s point of view they have to focus on their real task of devoting themselves to their families. Our result was congruent with other studies among patients with different cardiac problems, whereby participants declared a lack of interest in sex.23,27,31,43
The results of the current study revealed that many patients reported changes in their sexual activities before and after experiencing cardiac problems. Physically associated heart problems were the most reported causes behind this change, followed by physical and psychological causes. Many studies showed varied percentages of cardiac patients who reported marked changes in sexual activities caused by their illnesses, these ranged between 41–76%,4,7,12,43,44,46 and many of them reported complete cessation of sexual activities.43,44 This change can be attributed to many factors like fear of a heart attack or coital death, aging, worsening of the health condition, associated symptoms with or after sex, pain, exhaustion, lack of interest, sexual dysfunction, anxiety, spouse’s anxiety and concerns, feeling of guilt, depression, and social changes.4,12,13 All of these factors could be attributed to cardiac patients’ lack of information about their conditions and sexual life.
Cardiac patients ranked the effect of medications on sexual activity as the highest important sexual counseling need, and preparation for sexual activity as the least important sexual counseling need. Sexual counseling needs depend on the impact of specific information, or the long term effect of illness on sexual life, such as warning signs, when to resume sex, and medication effects on sexual activity. This information is needed for patients, especially before discharge. However, additional specific information is needed later on (e.g. positions to be used, using foreplay, and appropriate settings) as they readjust to normal life.31,39,47
Cardiac patients in our study ranked eating and drinking before sexual activity as the 3rd highest important sexual counseling need, while it was considered as the lowest important sexual counseling need in a previous study for MI patients. 47 This is related to patients’ feelings of tiredness after eating and drinking, so they would avoid sexual activity.48,49 For Jordanian families, especially those who work, the main meal is dinner, which is taken before they go to sleep. Regardless of the ranking of sexual counseling needs, all must be addressed and discussed with health care professionals.
Strength and limitations
This study dealt with a very sensitive topic, so sensitive in fact that we did not expect patients’ participation; however, we obtained a high response rate. The first limitation of this study was the use of a self-report questionnaire that imposes response set bias and feelings or behaviors that society judges to be controversial, especially those issues related to sex in the Arab-Muslim world. However, with sensitive topics such as sexual information needs, self-report would be more appropriate. Additionally, patients’ responses during structured interviews can be influenced by the age, gender, or even culture, since discussing sexual issues is considered a sensitive topic. Lastly, the number of male patients was greater than female patients, so caution is required when interpreting the study findings as related to gender.
Conclusion
In this study, we investigated cardiac patients’ sexual concerns and needs, as well as sexual counseling provided for the patients. Patients with cardiac problems experience many sexual concerns and needs; however, little attention is directed towards such concerns given the Arab-Muslim culture. Barriers, such as culture and gender differences are obstacles in discussing sexual concerns, and should be taken into consideration. In the Arab-Muslim culture, sexual concerns are rarely perceived as part of standard care.
Administrators should have an active role in developing policies regarding health education, and these policies should be provided for cardiac patients prior to discharge. Health care providers should arrange sexual counseling plans with the patient, as every patient has individual, specific, and unique sexual counseling needs, dependent upon their lifestyle, health conditions, and their type of cardiac disease. All of these implications should be taken into consideration, and should be recognized as essential elements to be assessed in the patient care process.
Footnotes
Acknowledgements
The authors would like to thank the Faculty of Scientific Research/Jordan University of Science and Technology for providing the grant (grant number 20100255) to conduct the study. In addition, the authors would like to acknowledge the patients who took part in this study. The authors also gratefully acknowledge the invaluable contribution of Manar Y Saleh, University of Houston, Department of Liberal Arts and Social Sciences, in editing the paper.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This research was granted by the Faculty of Scientific Research/Jordan University of Science and Technology (grant number 20100255).
To the researcher’s knowledge, there are no published studies investigating the sexual information needs of Arab-Muslim cardiac patients. Few cardiac patients reported receiving information about sexual activity and how it could contribute to complications after heart disease. There were no sexual concerns of high importance from the participants’ perspective. A significant number of cardiac patients believe that gender is a barrier, causing them to refrain from asking about sexual life. In Arab-Muslim culture, sexual concerns are rarely perceived as part of standard care. Policy makers (administrators and educators) should have an active role in developing policies regarding sexual health education.