
Abstract
Background:
Although individual symptoms and symptom trajectories for various cardiovascular conditions have been reported, there is limited research identifying the symptom clusters that may provide a better understanding of patients’ experiences with heart disease.
Aims:
To summarize the state of the science in symptom cluster research for patients with acute coronary syndrome, myocardial infarction, coronary artery bypass surgery, and heart failure through systematic review and to provide direction for the translation of symptom cluster research into the clinical setting.
Methods:
Databases were searched for articles from January 2000 through to May 2015 using MESH terms “symptoms, symptom clusters, acute coronary syndrome (ACS), myocardial infarction (MI), coronary heart disease (CHD), ischemic heart disease (IHD), heart failure (HF), coronary artery bypass surgery (CABS), cluster analyses, and latent classes.” The search was limited to human studies, English language articles, and original articles investigating symptom clusters in individuals with heart disease. Fifteen studies meeting the criteria were included.
Results:
For patients with ACS and MI, younger persons were more likely to experience clusters with the most symptoms. Older adults were more likely to experience clusters with the lowest number of symptoms and more diffuse and milder symptom clusters that are less reflective of classic ACS presentations. For HF patients, symptom clusters frequently included physical and emotional/cognitive components; edema clustered in only three studies. Symptom expression was congruent across geographical regions and cultures.
Conclusions:
The findings demonstrated similarities in symptom clusters during ACS, MI, and HF, despite multiple methods and analyses. These results may help clinicians to prepare at-risk patients for proper treatment-seeking and symptom self-management behaviors.
Keywords
Introduction
Traditionally, clinicians have evaluated symptoms individually and in the context of the patient’s presentation in order to assess, triage, or diagnose.1–3 However, patients often experience multiple symptoms concurrently. Recently, researchers have examined symptoms incorporating the concept of clustering, defined as two or more symptoms that occur simultaneously and are related.4–6 Examining symptom clusters may provide clinicians with a broader perspective in order to better understand how patients experience symptoms, which may guide clinical management.
Kirkova and colleagues suggested that the outcome or impact of a symptom cluster may be different or greater than the sum of individual symptoms. 7 Although individual symptoms and symptom trajectories for various cardiovascular conditions have been reported, there has been little translation of symptom cluster research in order to inform clinical practice.2,3,8 For instance, knowledge of heart failure (HF) symptom clusters may help patients quickly recognize if their condition is deteriorating, thus decreasing the delay in seeking care, expediting treatment, and preventing hospitalization. 9
Given the limited number of studies and varying approaches to symptom cluster research in cardiovascular populations, further examination of the concept of symptom clusters is timely and warranted. Presently, it is unknown whether individual symptoms are common or form a pattern across cardiac populations. There is speculation that symptom clusters may share a common mechanism, such as ischemia, or that symptoms within a cluster may respond to a single treatment. 9 Further research can make a positive impact on clinical outcomes, but only after symptom clusters have been identified, examined, and understood within the context of ischemic cardiac disease. Therefore, the purpose of this systematic literature review was to summarize the state of the science in symptom cluster research for patients with acute coronary syndrome (ACS), myocardial infarction (MI), coronary artery bypass surgery (CABS), and HF, and to provide direction for future research and potential translation of symptom cluster research into the clinical setting.
Early symptom cluster research
Researchers have hypothesized that clusters of symptoms could share common mechanisms, be related, or have similar influences on outcomes.10–12 For example, there are common biological mechanisms of psychoneurological symptom clusters (depressive symptoms, cognitive disturbance, fatigue, sleep disturbance, and pain) in patients with cancer. 13 Yet few studies have examined the underlying mechanisms of individual symptoms or symptom clusters.
Researchers have examined the impact of symptom clusters on patient outcomes, including quality of life (QOL), health status, functional limitations, symptom burden, and mortality.14–20 Poor QOL was associated with the presence of symptom clusters in patients with cancer,17,20 systemic symptom clusters in patients with leg ulcers, 15 nausea and vomiting symptom clusters in cancer patients, 18 and emotional/cognitive and physical symptom clusters in multiple sclerosis (MS) patients. 19 Functional limitations were associated with a motor symptom cluster in patients with MS 19 and among HF patients experiencing both sickness behavior and discomforts of illness symptom clusters. 16 A uremic symptom cluster predicted mortality for dialysis patients. 14
Symptom clusters have also been used to reduce the barriers to chronic obstructive pulmonary disease (COPD) self-management.21,22 Investigators have used symptom clusters to predict treatment choices for COPD 23 and demonstrated how symptom clusters could influence interventions. 24 No outcome data are available to determine whether any of these symptom clusters were more robust than individual symptoms alone.
Analytic techniques in symptom cluster research
Researchers aiming to identify symptom clusters have used different instruments in order to query patients with cardiovascular disease about their symptoms, including instruments that have been previously discussed in the literature, 25 general symptom inventories, 9 disease-specific instruments,9,26,27 and instruments that have been validated for the assessment of individual symptoms. 28 Investigators have also used several statistical methods in order to classify symptom clusters, including latent class analysis,29,30 the hierarchical cluster agglomerative approach,25,31 factor analysis, 16 and model-based clustering methods. 32 It remains unknown as to whether the use of different analytical techniques results in different symptom clusters.
Methods
The investigation conforms with the principles outlined in the Declaration of Helsinki. 33
Data sources
PubMed, CINAHL, MEDLINE, and Web of Science databases were searched for articles from January 2000 through to May 2015 using a combination of the MESH terms “symptoms, symptom clusters, ACS, MI, ischemic heart disease (IHD), coronary heart disease (CHD), HF, CABS, cluster analyses, and latent classes.” The search was limited to human studies, those published in English, and original articles investigating symptom clusters in adults with heart disease.
Study selection
Descriptive or observational studies lack interventions, outcomes, and other study designs to consider when evaluating quality; therefore, we were unable to utilize the Cochrane criteria for systematic reviews of intervention guidelines or the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) of controlled trial guidelines for this systematic review.34,35 Instead, we were guided in study selection and evaluation by criteria reported by Grimes and Schulz, 36 who noted that descriptive studies have several important roles in research, as the data are often the first venture into a line of investigation or a condition. This is the case with symptom clusters in cardiovascular diseases. According to Grimes and Schulz, 36 good descriptive research, similarly to reporting in the popular press, should include the five “W” questions – who, what, why, when, and where – with an implied sixth question – so what? For the purpose of this review, “who” represents the sample population; “what” represents the symptoms assessed; “why” represents the aims of the studies; “when” is the year of publication; and “where” represents the setting. Our “so what?” includes the interpretation of the findings and recommendations for future research.
A total of 706 articles were identified in the search process as potentially relevant. Abstracts were independently reviewed by the authors (blinded for review). Conflicts were resolved through discussions with all authors. An additional six articles were identified after hand-searching reference lists. A literature search flowchart conforming to PRISMA guidelines appears in Figure 1. Of these 712 articles, 15 met the following inclusion criteria: (1) included samples of patients with ACS, MI, CABS, and HF; (2) assessed symptom clusters using any measure; and (3) analyzed symptom clusters using cluster statistical methods (factor analysis, latent class analysis, or hierarchical cluster agglomerative analysis). Studies were excluded if: (1) single symptoms only were analyzed; or (2) aggregate data were reported without providing details of the symptoms in each cluster. ACS and MI studies were examined separately because the diagnosis of ACS includes patients with unstable angina.
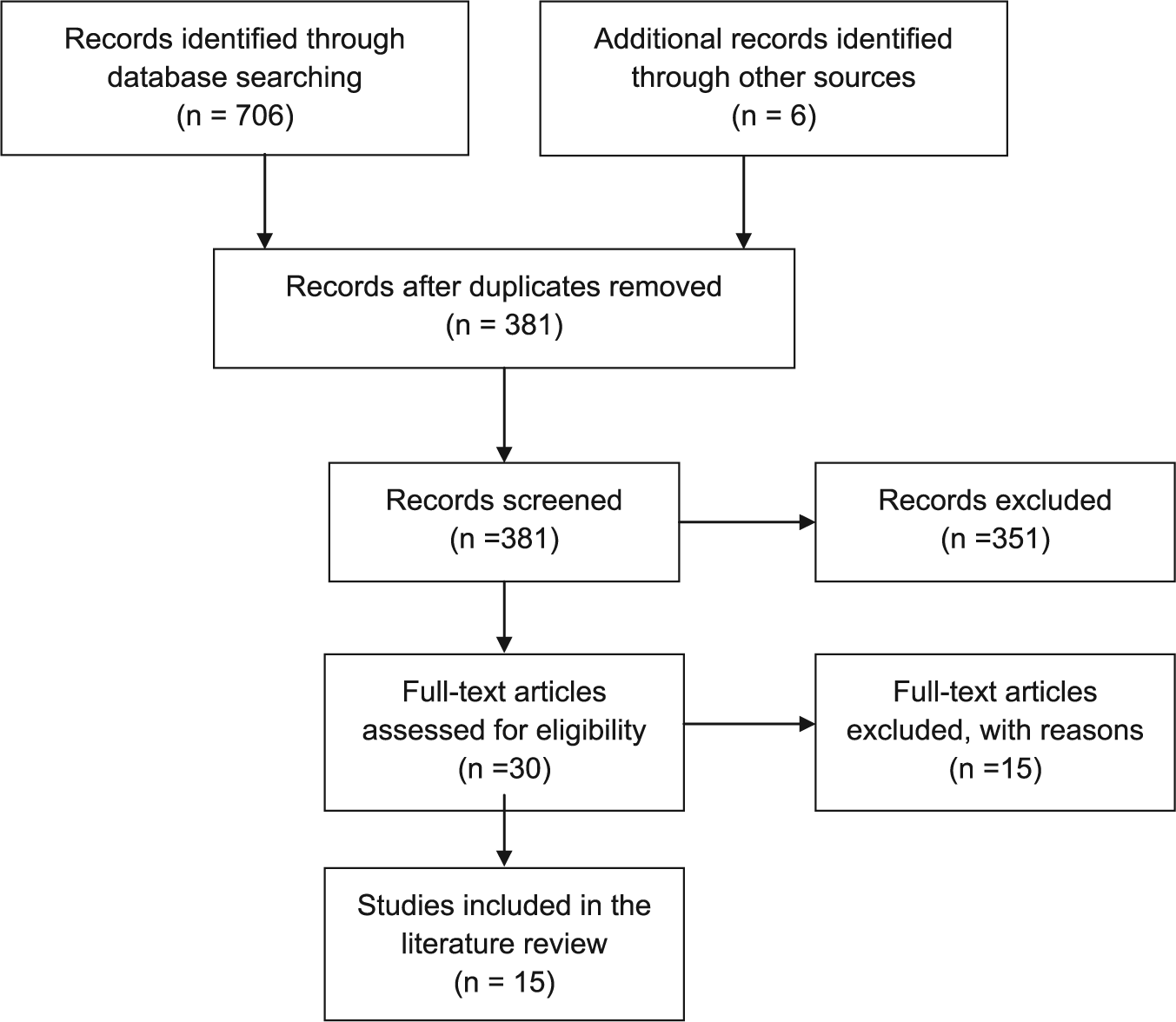
Preferred Reporting Items for Systematic Reviews and Meta-Analyses literature search flowchart.
Results
Data extraction
Fifteen studies met the inclusion criteria. Nine studies met the criteria for the examination of symptom clusters in ACS, MI, or CABS (Table 1). The aims of the studies were to classify groups of individuals with common symptom clusters. A variety of analytical methods were used, including cluster analysis, latent class analysis, and agglomerative hierarchical cluster analysis. The mean age of participants across studies was 64 years. Younger patients were more likely to be in clusters with the most symptoms.37,38
Summary of symptom cluster studies for patients with acute coronary syndrome/myocardial infarction/coronary artery bypass surgery.
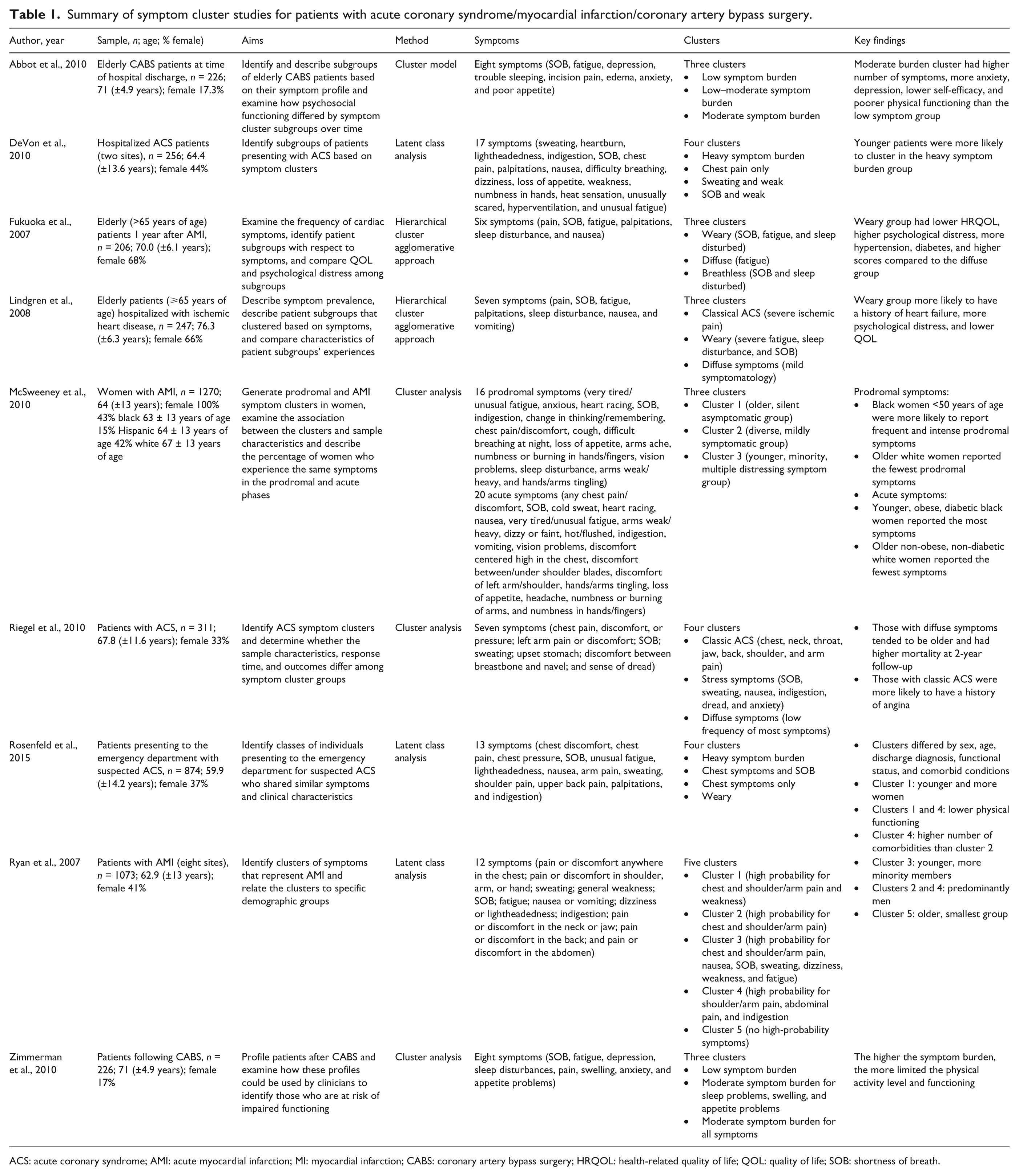
ACS: acute coronary syndrome; AMI: acute myocardial infarction; MI: myocardial infarction; CABS: coronary artery bypass surgery; HRQOL: health-related quality of life; QOL: quality of life; SOB: shortness of breath.
Six studies were identified that examined symptom clusters in patients with HF. Four prospective studies used hierarchical cluster analysis in order to examine symptom clusters,26,27,39,40 while two studies used factor analysis.9,16 With one exception, 27 all of the HF studies examined the relationships of symptom clusters with outcomes.
A synthesis of the data is presented thematically. Summaries of the findings from ACS, MI, and CABS populations appear in Table 1. Summaries of the findings from HF populations appear in Table 2. The individual symptoms used for cluster analyses in each study are presented in Table 3.
Summary of symptom cluster studies for patients with heart failure.
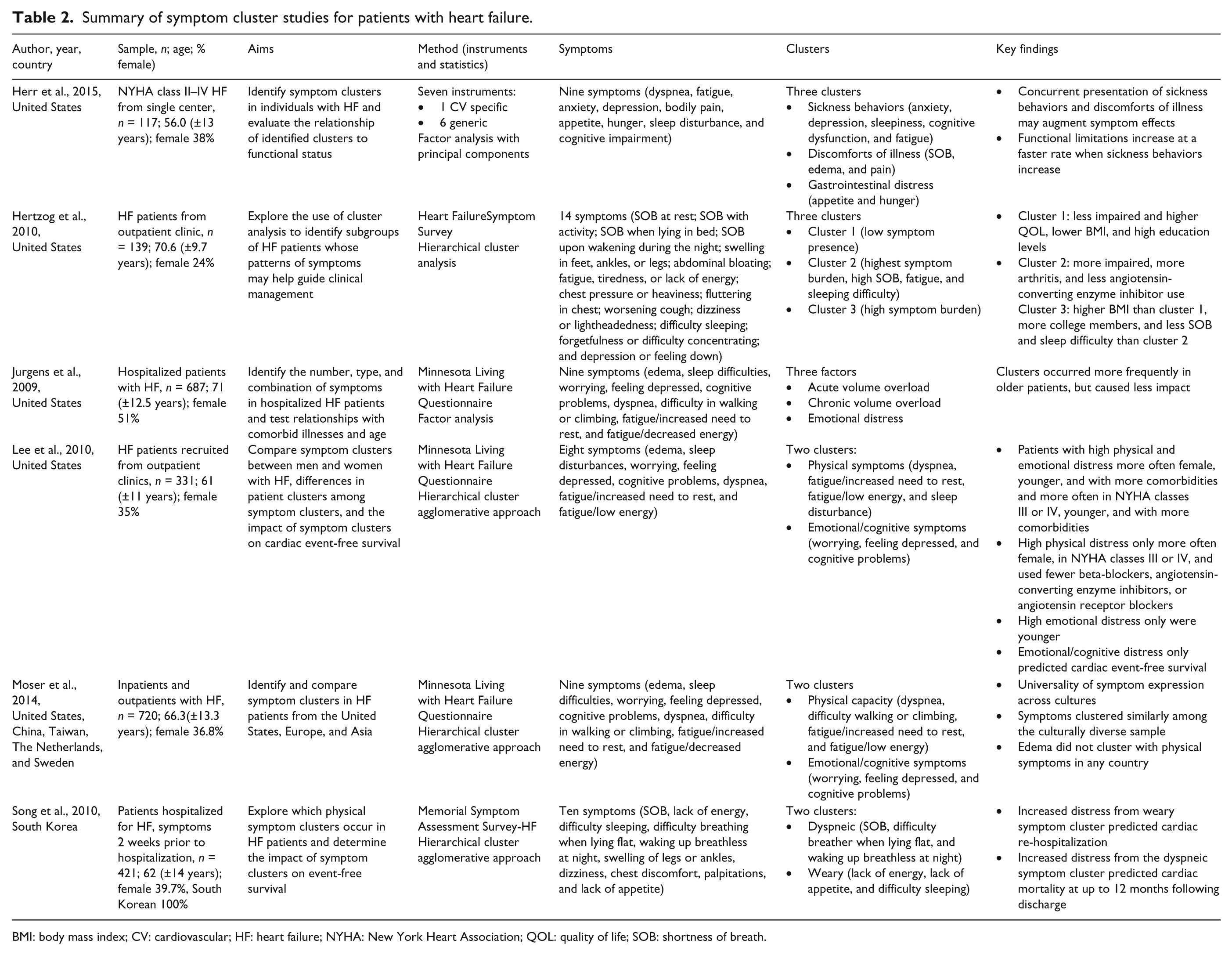
BMI: body mass index; CV: cardiovascular; HF: heart failure; NYHA: New York Heart Association; QOL: quality of life; SOB: shortness of breath.
Individual symptoms used in the cluster analyses.
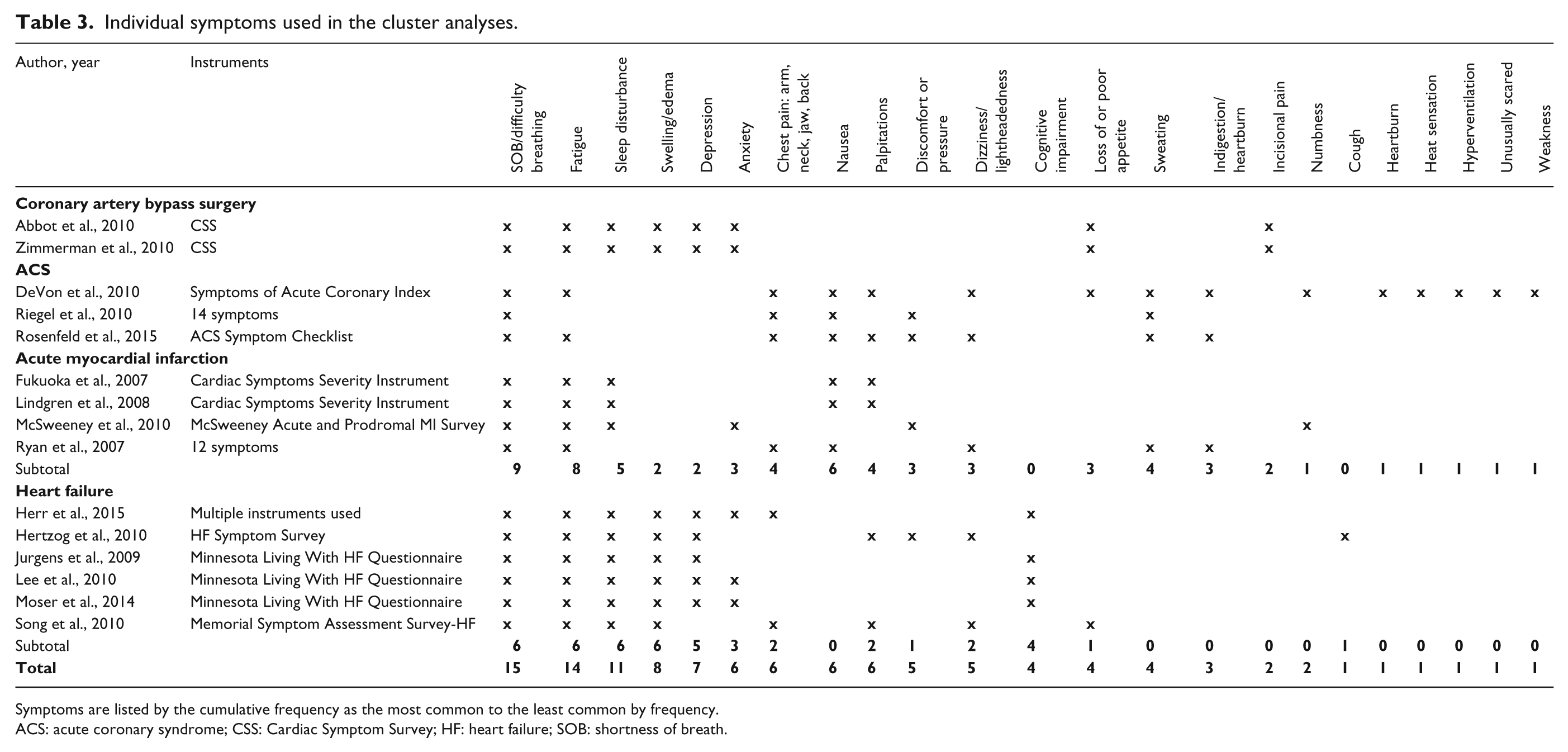
Symptoms are listed by the cumulative frequency as the most common to the least common by frequency.
ACS: acute coronary syndrome; CSS: Cardiac Symptom Survey; HF: heart failure; SOB: shortness of breath.
Cluster concepts
Clustering can be conceptualized as groups of symptoms or groups of individuals clustered by personal characteristics and symptoms. 41 The studies were nearly evenly divided between these two concepts. Important covariates, such as sex, age, and race, which influenced symptom cluster membership were included in the statistical analysis in most of the studies reported here.9,26,27,30,37–40 Age was significantly associated with cluster membership, with the youngest patients being more likely to be in the heavy symptom burden cluster in a study of 256 patients with ACS. 35 Similarly to studies in ACS patients, sex and race were statistically significantly associated with cluster membership in a study by Ryan et al. 30 Age, race, body mass index (BMI), history of heart disease, diabetes, and smoking were associated with the clusters of symptoms in a cluster analysis study by McSweeney et al. 38 Following MI, younger, obese, diabetic black women reported the most acute symptoms, while older, non-obese, non-diabetic White women reported the fewest. In a study of HF patients, age was the only predictor of membership in each of three clusters (odds ratio (OR) = 0.965–0.969, 95% confidence interval (CI) = 0.94–0.99, p ⩽ 0.001), while diabetes was a significant predictor of the emotional cluster (OR = 0.644, 95% CI = 0.42-0.99, p = 0.046). 9
Study designs
Most studies had cross-sectional, descriptive designs. Five were secondary data analyses,9,30,32,38,42 and one examined repeated measures at 6 weeks, 3 months, and 6 months following hospital discharge for CABS. 42 In a large multi-site study, Rosenfeld et al. 29 examined symptom clusters in 874 patients evaluated in the emergency department for possible ACS; this was the only study in which symptoms were measured as they were occurring.
Objectives of symptom cluster analyses
There were many differences in the aims of the analyses, with most ACS/MI studies focusing on classifying groups of individuals who shared clinical characteristics or common clusters of symptoms. Variations in symptom clusters were evaluated by patients’ general physical and mental health, mood states, and QOL in a study of elders hospitalized for MI or CABS. 31 The authors concluded that older adults experienced more diffuse and milder symptoms that were less reflective of classic ACS presentations. One year later, the same cohort was sampled in order to determine the frequency of cardiac symptoms and to determine whether the subgroups varied based on QOL and psychological distress. 25 Patients in the weary group had the poorest recovery outcomes, lower health-related QOL, and more psychological distress.
Abbott et al. 32 described cluster subgroups, determined if cluster subgroups varied by demographic and clinical characteristics, and examined the impact of symptom clusters on psychological functioning over time in 226 patients who had undergone CABS. There was a significant difference between patients in the low symptom burden cluster group and those in the moderate symptom burden group: those is the low symptom burden group had higher physiological functioning and lower anxiety or depression. The investigators also found that, regardless of recovery time, cluster group membership was significantly associated with mental scale scores.
Zimmerman et al. 42 examined the impact of the three patient clusters on physical functioning and physical activity at 6 weeks, 3 months, and 6 months after surgery using data from the Abbott et al. study. 32 All three groups improved in both physical functioning and physical activity over time. Riegel and colleagues 43 examined symptom clusters, delay times, and outcomes in 331 individuals who had confirmed ACS. Riegel et al. also measured mortality rates within two years of follow-up in an ACS cohort. 43 Subjects in the diffuse symptom group (no highly represented symptoms) had higher mortality rates; however, this group was significantly older than the other groups, which may explain these differences.
The ACS/MI studies mostly focused on identifying and describing symptom clusters in order to improve symptom assessment and reduce delays in seeking treatment, while the HF studies attempted to tie clusters to the outcome variables of functional status, event-free survival, mortality, and hospital readmissions.
Patient populations
Symptom cluster studies were identified in cardiovascular populations with four different diagnoses (ACS, MI, CABS, and HF), although most of the studies sampled patients with ACS/MI and HF. Most of the studies were conducted with hospitalized patients (n = 9), and five studies (33%) enrolled patients in outpatient settings or by telephone. A total of 7104 patients were included in the 15 studies: 4321 inpatients, 2063 outpatients, and one study with a combination of inpatients and outpatients. 27 Sample sizes were generally large and varied from 117 16 to 1270. 38 Three studies examined symptom clusters in international populations.27,31,40 Moser et al. 27 described and compared symptoms in 720 patients with HF from inpatient and outpatient settings in three global regions – Asia (China and Taiwan), Europe (The Netherlands and Sweden), and the United States – in a cross-sectional, observation study. Congruence of symptom expression was found across cultures. Song et al. 40 sampled 421 patients with HF exclusively in South Korea, and Ryan et al. 30 included a study conducted in England (n = 88).
Age
Mean age ranged from 56 years 16 to 76.3 years. 31 The definition of older and younger patients varied between studies. Fukuoka and colleagues 25 defined elderly as ⩾65 years of age. McSweeney et al. defined younger as <50 years of age. 38 DeVon et al. did not define younger and older, but the mean ages among four clusters ranged from 57 to 67.5 years, with younger women more likely to be in the heavy symptom burden group. 37 Similarly, the mean age ranges for four clusters in Rosenfeld et al.’s study were 54.8–65.4 years, and younger patients were more likely to be in the heavy symptom burden cluster. 29
Number and type of symptoms entered into the cluster analysis
The number of symptoms differed widely and ranged from 6 to 33. Most studies (n = 13) evaluated 6–14 symptoms; the mean number of symptoms evaluated was 11.3. Collectively, the most common symptoms measured were shortness of breath (n = 14), fatigue (n = 13), sleep disturbances (n = 10), swelling (n = 8), and depression (n = 7). Notably, all of the HF studies measured swelling, SOB, fatigue, and sleep disturbances; some type of pain was measured in all of the non-HF studies. Cognitive impairment was measured only in the HF studies, while incisional pain was measured solely in the CABS studies. Individual symptoms appear in Table 3.
Measures
The use of a variety of multidimensional, multi-symptom instruments in order to measure symptom clusters is evident in this review of the literature. These included a secondary analysis 30 ; intensity of seven cardiac symptoms 31 ; six of those seven symptoms in a follow-up 25 ; the ACS Symptom Checklist 29 ; responses to eight early recovery (6 weeks and 3 months following surgery) symptoms from the Cardiac Symptom Survey 32 ; and 14 symptoms generated from the REACT trial (seven symptoms) 44 and from patients (seven symptoms). 43 The volume and variation of instruments used in the studies make comparisons across studies challenging.
In the nine ACS/MI/CABS studies evaluated, six different instruments were used. Two studies used the same instrument,32,42 and two29,37 used iterations of previous instruments. Herr and colleagues 16 identified symptom clusters in HF patients, evaluating nine symptoms using seven different instruments. Jurgens et al. 9 analyzed the data of 687 patients from the Heart Failure Quality of Life Trial Collaborators registry in order to identify symptom clusters in patients who were hospitalized with a confirmed diagnosis of acute HF. Nine symptoms from the Minnesota Living with Heart Failure Questionnaire (MLHFQ) were analyzed using factor analysis.
Hertzog et al. 39 used cluster analysis in order to identify patient subgroups with HF whose symptom patterns might help guide clinical management. Symptoms were measured with the Heart Failure Symptom Survey, which is a modified version of the Cardiac Symptom Survey. The instrument most commonly used in the HF studies was the MLHFQ. This instrument was used in acute to chronic HF patients and in an international study, allowing some comparisons of clusters. In the Song et al. study, 40 the presence and level of perceived distress of ten physical symptoms that are specific to HF reported for the previous 2 weeks were assessed using the Memorial Symptom Assessment – Heart Failure questionnaire. Patients in the weary cluster who experienced more distress had a 50% higher risk of re-hospitalization within 1 year of discharge. 40
Analytic techniques
Some investigators analyzed clusters of symptoms using factor analysis32,38,42,43 and some grouped individuals according to personal characteristics and common clusters.25,29–31,37 Most studies (n = 6) used hierarchical cluster agglomerative techniques; four used cluster analysis techniques; three used latent class; and two used factor analysis. Investigators used several statistical software programs, including SPSS, SAS, MPlus, and Latent Gold.
Number of clusters
The number of clusters across studies ranged from two to five. Only one study identified five clusters. 30 The three studies that identified two clusters sampled patients with HF.26,27,40 The three studies that identified four clusters included ACS patients with classic-type clusters (chest symptoms) and less classic clusters. Most studies (n = 8) found three clusters.
Cluster labels
Researchers labeled symptoms by: (1) intensity or “burden” (n = 3)32,39,42; (2) type, such as physiological or psychosocial (n = 5)9,16,26,27,43; (3) a cross between intensity and specific symptoms (n = 7)25,29,30,37,38,40,43; and (4) as “typical,” “atypical,” or “classic” (n = 2).31,43 A number of investigators used the same labels in order to identify clusters such as “weary,”25,29,31,40 “diffuse,”25,43 “physical,”26,27 and “emotional/cognitive.”9,26,27 The terms “low,” “moderate,” and “heavy symptom burden” were commonly used across patient populations.29,32,37,39,42
Internal validity
Some studies were well-powered and had large sample sizes, supporting the internal validity of their findings. For example, Ryan et al. 30 completed a secondary data analysis of MI symptoms from nine different research studies (n = 1073) in order to identify the cluster of symptoms for AMI and to determine whether clusters were related to demographic groups.
Discussion
ACS, MI, and coronary bypass grafting
The finding that younger patients were more likely to be in clusters with the most symptoms37,38 and older adults more likely to be in clusters with the fewest number of symptoms may hinder treatment-seeking and self-care behaviors. Older adults also experienced more diffuse and milder symptom clusters that are less reflective of a classic ACS presentation.29,30,37 These symptoms have been linked to poorer recovery, lower health-related QOL, more psychological distress, 31 and higher mortality. 43
Classic29,43 and weary25,31 clusters were very common in ACS patients, and clinicians should be vigilant for more non-specific symptoms such as fatigue and sleep disturbances that may represent ACS, especially in older adults. Older adults tend to attribute symptoms as normal signs of aging, but should be counseled that most symptoms are not normal and should be evaluated. In addition, older adults who are at risk for CHD can be educated regarding non-specific symptoms and told about American Heart Association recommendations to call emergency services within 5 minutes of the onset of chest pain. Finally, because approximately 32% of patients with ACS do not experience chest pain, 45 individuals with a history of CHD should be reminded that the symptoms of ACS are often vague and may be difficult to distinguish from other health problems.
Heart failure
HF symptom clusters frequently have physical and emotional/cognitive components, 26 reflecting the functional decline and cognitive impairment associated with HF. 9 Different investigators use different labels, but the individual symptoms in the cluster are similar. For example, the label “sickness behaviors” 16 contains nearly the same symptoms as the label “emotional/cognitive.”26,27 The label may be informative for other researchers, but, regardless of labels, the information can be used to counsel patients regarding the importance of responding to multiple symptoms that co-occur and may signal deterioration in their condition. Of the six HF studies, three used the MLHFQ, and all used multidimensional measures of symptoms.
Clusters with the highest burden or severity of symptoms were related to higher New York Heart Association (NYHA) class (greater physical impairment) 39 and higher BMI. 40 Higher levels of distress were correlated with worse outcomes, such as cardiac arrest. 26 Higher levels of distress were also associated with increased re-hospitalization independent of NYHA class, BMI, age, or sex. 40 Notably, edema appeared in a symptom cluster (discomforts of illness) in only one study of outpatients, 16 which included stable patients optimized on guideline-directed therapy. In two other studies, edema appeared in a cluster when the sample included patients with acute HF 9 and in a sample in which 21% of patients were not prescribed diuretics. 39 It is possible that edema was treated as a sign rather than a symptom in some studies, or was not perceived as stressful 26 and consequently underreported by patients. This requires further research in order to determine whether this is clinically relevant.
Symptom clusters across international cohorts were reported in only one study, and no differences were found. 27 Whether symptoms, symptom burden, or expression of symptoms vary across cultures requires further research. Future research should examine potential mechanisms in order to determine whether symptom clusters are related from a biological perspective. In addition, whether symptom clusters change throughout the course of a disease (acute versus chronic phases) has not been investigated in cardiovascular populations. Finally, the impact of symptom clusters on patient outcomes should be evaluated for all populations in order to determine whether symptom clusters add value to patient assessment and, if so, how to optimize symptom-related interventions.
Conclusions
Differences in cluster concepts (clustering symptoms versus clustering groups of individuals with common symptom clusters), study design (retrospective versus prospective), sample characteristics (inclusion and exclusion criteria and adjustment of confounders), measures (no standardized instruments and unidimensional versus multidimensional measures), and statistical analyses make it challenging to compare results across studies and to generalize findings. None of the studies addressed the possible mechanisms of action explaining symptom clusters. Studies of all patient populations had long-term goals of developing interventions in order to improve patient outcomes.
Footnotes
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
There are no direct practice implications resulting from this review of the emerging field of symptom clusters in ischemic heart disease; however, we recommend:
Clinicians should be vigilant for more non-specific symptoms such as fatigue and sleep disturbances that may represent acute coronary syndrome, especially in older adults. Older adults who are at risk of coronary heart disease should be educated regarding non-specific symptoms and be counseled to call emergency medical services within 5 minutes of the onset of chest pain. Patients with heart failure should be informed of the importance of responding to multiple symptoms that co-occur and may signal deterioration of their condition. Research should include conceptual models and adjust for customary potential confounders such as sex, age, and race. There is a need for population-based studies that use standardized symptom measures. No studies of patients with acute coronary syndrome have addressed how symptoms within a cluster may be related.