
Abstract
Background:
Chronic heart failure (CHF) and atrial fibrillation (AF) are complex cardiogeriatric syndromes mediated by physical, psychological and social factors. Thromboprophylaxis is an important part of avoiding adverse events in these syndromes, particularly stroke.
Purpose:
This study sought to describe the clinical characteristics of a cohort of patients admitted to hospital with CHF and concomitant AF and to document the rate and type of thromboprophylaxis. We examined the practice patterns of the prescription of treatment and determined the predictors of adverse events.
Methods:
Prospective consecutive participants with CHF and concomitant AF were enrolled during the period April to October 2013. Outcomes were assessed at 12 months, including all-cause readmission to hospital and mortality, stroke or transient ischaemic attack, and bleeding.
Results:
All-cause readmission to hospital was frequent (68%) and the 12-month all-cause mortality was high (29%). The prescription of anticoagulant drugs at discharge was statistically significantly associated with a lower mortality at 12 months (23 vs. 40%; p=0.037; hazards ratio 0.506; 95% confidence interval 0.267–0.956), but was not associated with lower rates of readmission to hospital among patients with CHF and AF. Sixty-six per cent of participants were prescribed anticoagulant drugs on discharge from hospital. Self-reported self-care behaviour and ‘not for cardiopulmonary resuscitation’ were associated with not receiving anticoagulant drugs at discharge. Although statistical significance was not achieved, those patients who were assessed as frail or having greater comorbidity were less likely to receive anticoagulant drugs at discharge.
Conclusion:
This study highlights multi-morbidity, frailty and self-care to be important considerations in thromboprophylaxis. Shared decision-making with patients and caregivers offers the potential to improve treatment knowledge, adherence and outcomes in this group of patients with complex care needs.
Keywords
Introduction
Chronic heart failure (CHF) is a common and multifaceted syndrome with complex self-care needs. 1 Previous studies 2 have highlighted that atrial fibrillation (AF) is a concomitant condition in up to 50% of patients with CHF and, as a consequence, these patients have a high risk of stroke. The use of thromboprophylaxis, including anticoagulant drugs, significantly reduces the risk of stroke. 3 In spite of evidence-based recommendations, the rates of thromboprophylaxis remain poor. 4 There are many factors underpinning the clinical decisions about why individual patients may not receive evidence-based treatment when indicated – these factors may be related to the healthcare system, treatment, socioeconomic status, the individual patient, or the condition. Specifically, these barriers can include poor self-care behaviour, non-adherence to medication, frailty, cognitive and functional impairment, or a lack of caregiver assistance. The research team have summarized these factors in previously published work. 5 There is still a need to better understand the factors that influence decision-making in thromboprophylaxis within the context of existing stroke and bleeding risk prediction models and complex comorbidities. Nurses have a key part to play in anticoagulation decision-making for stroke prevention. The key aspects of our role include education, counselling, advocacy and supporting patients and caregivers to make sense of complex risk–benefit information to elicit treatment preferences. 6 There is a need for an improvement in nurses’ knowledge and practice of care of patients with AF, as a lack of treatment knowledge may lead to inappropriate counselling and education. 7 Therefore it is important that nurses understand the key factors that influence the choice of anticoagulant and the decision-making process, and also the strengths and limitations of current risk prediction models.
Purpose
The aim of this study was to: (a) describe the clinical characteristics of a cohort of patients admitted to hospital with CHF and concomitant AF; (b) to describe the frequency and type of thromboprophylaxis used; (c) to examine practice patterns of the prescription of treatment; (d) to compare the overall quality of AF and CHF care in this cohort of patients when benchmarked against the recommendations of international guidelines; and (e) to determine the predictors of adverse events (including all-cause readmission to hospital and all-cause mortality, stroke/transient ischaemic attack (TIA) and bleeding events).
Methods
Design and setting
The AFASTER (
Baseline demographics and clinical characteristics of participants.
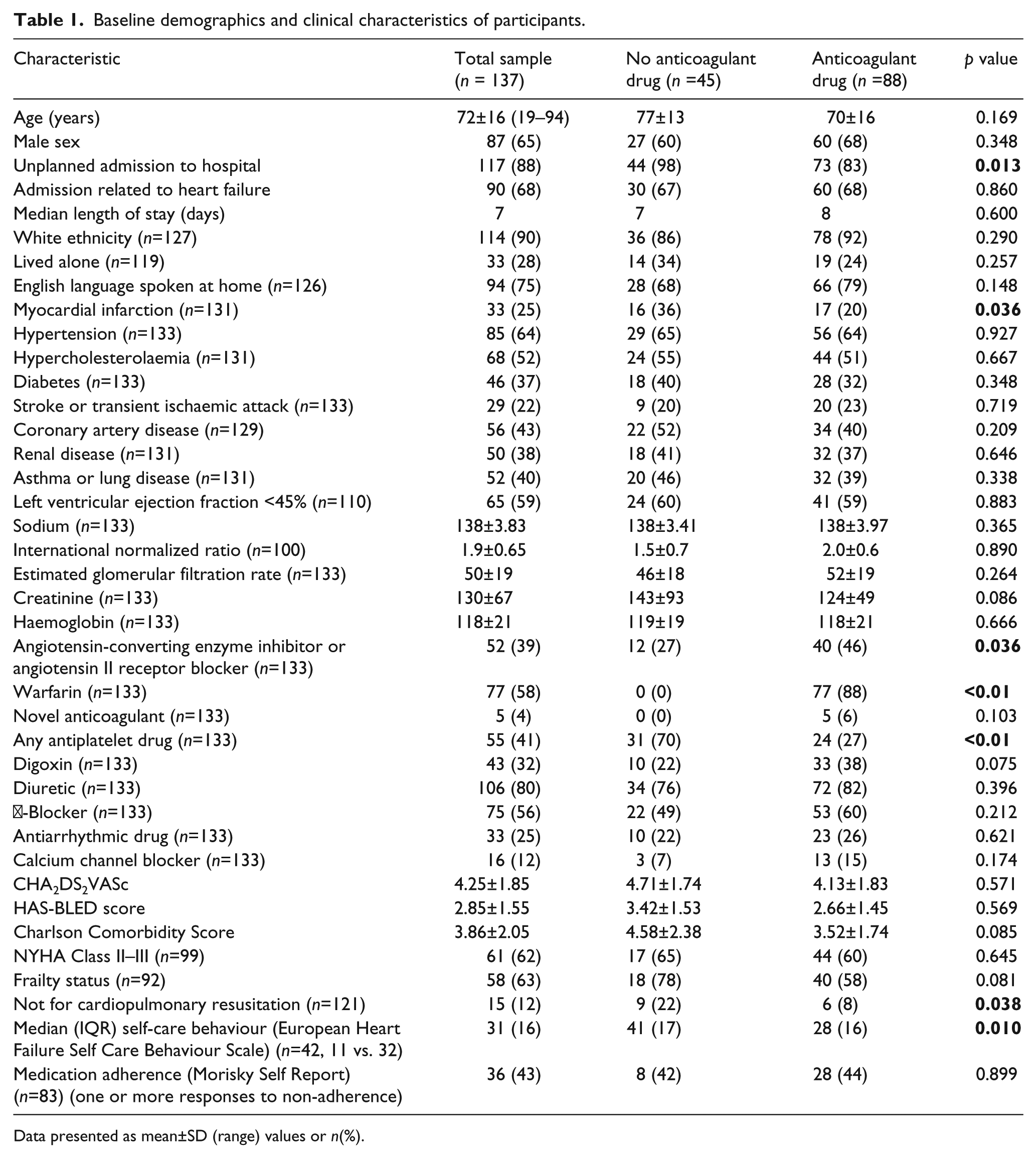
Data presented as mean±SD (range) values or n(%).
Measurements
Baseline demographic and clinical data were obtained using a standardized case report form. Biochemical, haematological, echocardiographic and medication data were obtained at discharge from hospital. The Charlson Comorbidity Index was used to quantify comorbidity. This index is a simple and valid method to classify comorbid disease. 8 The patients’ social and living situation and social support information were collected.
Stroke and bleeding risk
The CHA2DS2VASc 9 and HAS-BLED10,11 stroke and bleeding risk stratification tools were used to stratify stroke and bleeding risk. Both schemata are well validated and simple to use in clinical practice and they are both recommended for use throughout international guidelines for the management of AF.12–14
In a retrospective study of patients with a history of AF and an implanted pacemaker, the CHA2DS2-VASc score had a high sensitivity to predict stroke with good sensitivity and predictive ability; however, it has a low specificty (7–24%). 15 The CHADS2 tool is more widely used in clinical practice; CHADS2 data can be derived from a CHA2DS2-VASc score and they assess for a greater number of well-established independent risk factors for stroke. In a recent post hoc analysis of the AMADEUS study population comparing the performance of the HEMORR2HAGES, ATRIA and HAS-BLED bleeding risk prediction scores in patients with AF undergoing treatment with anticoagulant drugs, the HAS-BLED score was identified as having a superior predictive performance for overall bleeding and intracranial haemorrhage (c-index 0.75). 16 A CHA2DS2VASc risk score of 0 identifies patients at low risk of stroke, a score of 1–2 identifies patients at moderate risk of stroke and a score >2 identifies patients at high risk of stroke. A HAS-BLED score ⩾3 identifies patients at a high risk of bleeding. 17
Current international guidelines advocate stroke risk stratification using the CHA2DS2VASc score and the prescription of a vitamin K antagonist or novel oral anticoagulant drug if CHA2DS2VASc score >1. Further assessment of bleeding risk is made using the HAS-BLED score and considerations should be made towards the patient’s individual values and preferences. Antiplatelet treatment should only be considered for thromboprophylaxis in AF for low-risk patients (CHA2DS2VASc <1) or those deemed unsuitable for treatment with a vitamin K antagonist or novel oral anticoagulant. 12 Given the validity, reliability and widespread recommendation for use of the CHA2DS2VASc and HAS-BLED scores within international guidelines, we selected these as suitable instruments for the stratification of stroke and bleeding risk in this study.
Adherence to medication
Patient self-reporting is a useful method of assessing adherence to medication. Self-reporting offers reliable predictors of a variety of cardiovascular health outcomes, such as blood pressure control and admission to hospital for CHF. 18 There are a number of tools available to measure self-reported adherence; the four-point Morisky Scale (MMAS) provides good predictive ability and can be easily integrated into a patient assessment. 19 The MMAS has a reported sensitivity and specificity of 81 and 44%, respectively; the Cronbach’s α for reliability is 0.61, which is below the accepted value of 0.7. This tool has been implemented in a large number of studies in clinical research and has the advantage of being easily integrated into a quick clinical assessment. 20
Self-care behaviour
The European Heart Failure Self Care Behaviour Scale 21 was used to measure self-care behaviour. This questionnaire is widely used in heart failure research and has been validated using pooled data from six European countries. Cronbach’s α was 0.81. This is a five-point scale ranging from 1 (I completely agree) to 5 (I completely disagree), with a global score ranging from 12 (better self-care behaviour) to 60 (worse self-care behaviour). This scale is specifically designed for evaluating the outcome of the management of CHF with a focus on self-care behaviour in patients with heart failure. A lower score indicates better self-care behaviour and a higher score indicates poorer self-care behaviour. 22
Frailty
The Survey of Health, Ageing and Retirement in Europe (SHARE) Frailty Index (FI) is a simple frailty screening instrument. 23 This instrument has been validated for use in primary care settings with a community-dwelling population and has demonstrated good predictive validity. This instrument is available with free and easy-to-access web-based calculators. There are five key variables in the SHARE-FI, including: fatigue, loss of appetite, handgrip strength, functional difficulties and physical activity. The SHARE-FI was selected for use in the study as a result of its brevity and simplicity to use during an assessment by a research nurse. Many other frailty instruments include a variable for weight; this is replaced with a variable for ‘loss of appetite’ in the SHARE-FI. This is an important consideration in the management of heart failure, where weight fluctuations may influence measurement. This instrument was delivered using a standardized method, which was important in the measurement of handgrip strength using the dynamometer. Frailty was assessed as close to discharge from hospital as clinically possible to maintain consistency in measurement. Two research nurses were trained to deliver the frailty screen to achieve consistent measurements.
Data management, statistical analyses and missing data
Data were managed and analysed using IBM SPSS Statistics version 21 (IBM Corp., Armonk, NY, USA). The baseline characteristics of the study cohort were described using frequencies and percentages for categorical variables and values for the mean±SD, median and interquartile range for continuous variables. Event-free survival time was calculated using Kaplan–Meier survival analysis for a composite endpoint of all-cause admission to hospital and mortality. Cox regression analysis was used to calculate hazards ratios.
Ethical considerations
This study was approved by the hospital and university Human Research Ethics Committee, approvals LNR/12/SVH/62 and 2013000181. Consent was waived for baseline data collection and a routine 12-month follow-up phone call. Participants were provided with written information on the study and were free to withdraw at any stage.
Results
Sample baseline demographic information and clinical characteristics
A total of 1860 patients was screened between April and October 2013 at a single site. Of these, 365 patients had a diagnosis of CHF, consistent with international guidelines. From this sample, 156/365 (43%) patients were eligible for inclusion as they had concomitant AF of any type. Six patients died during hospital admission, 11 patients were not included for other reasons (declined or enrolled in another clinical trial) and two withdrew patients from the study. Of the final cohort of 137 participants, four were not included in the comparative analysis as a result of missing medication data at discharge (Figure 1).
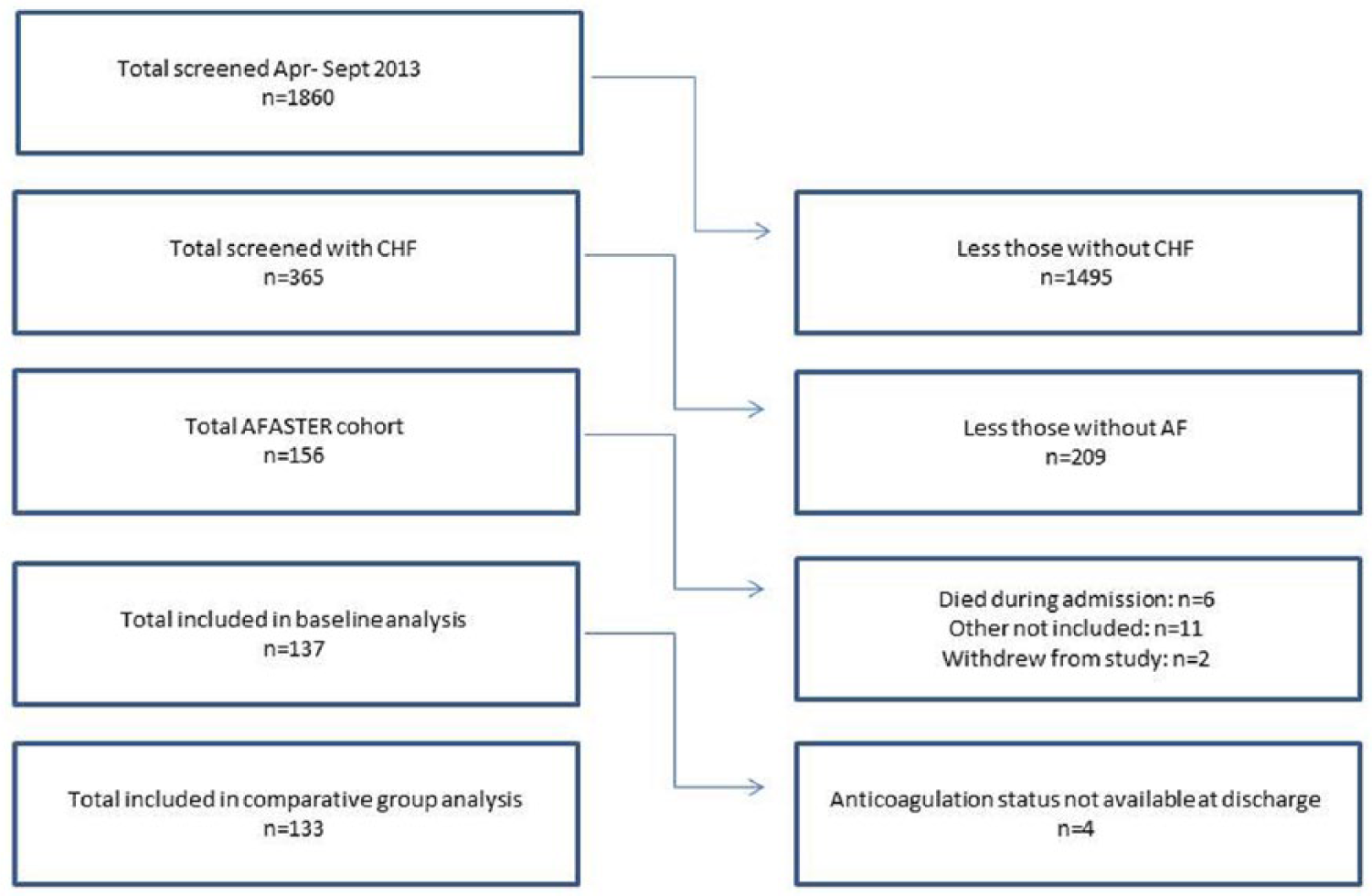
Screening and recruitment of participants. AF: atrial fibrillation; CHF: chronic heart failure.
The baseline analysis included 137 hospitalized patients who were consecutively enrolled into the study on discharge between April and October 2013. The mean±SD age was 72±16 years, 65% were men, 62% were NYHA class II–III and 59% had a left ventricular ejection fraction <45%. The mean±SD CHA2DS2VASc score was 4.25±1.85, the mean±SD HAS-BLED score was 2.85±1.55), the mean±SD Charlson Comorbidity Score was 3.86±2.05 and the mean±SD number of drugs on discharge was 11±4. Twenty-eight per cent of participants lived alone.
Seventy per cent of participants (96/137) had a CHA2DS2VASc score ⩾4 points with a mean±SD of 4.25±1.85 (Figure 2). Sixty-eight per cent of participants (56/137) had a HAS-BLED score ⩾3. This equates to >3.74 bleeds/100 patient-years (mean±SD 2.85±1.55) (Figure 3). Although the differences were not significant, participants who were not prescribed anticoagulant drugs at discharge were generally at greater risk of stroke (4.71 vs. 4.13; p=0.571) and bleeding (3.42 vs. 2.66; p=0.569), as indicated by the CHA2DS2VASc and HAS-BLED schemata, and tended to have greater comorbidity (p=0.085) than those prescribed anticoagulant drugs. Only 66% of participants were prescribed an anticoagulant drug (58% warfarin, 4% novel oral anticoagulant and 2% subcutaneous anticoagulation).
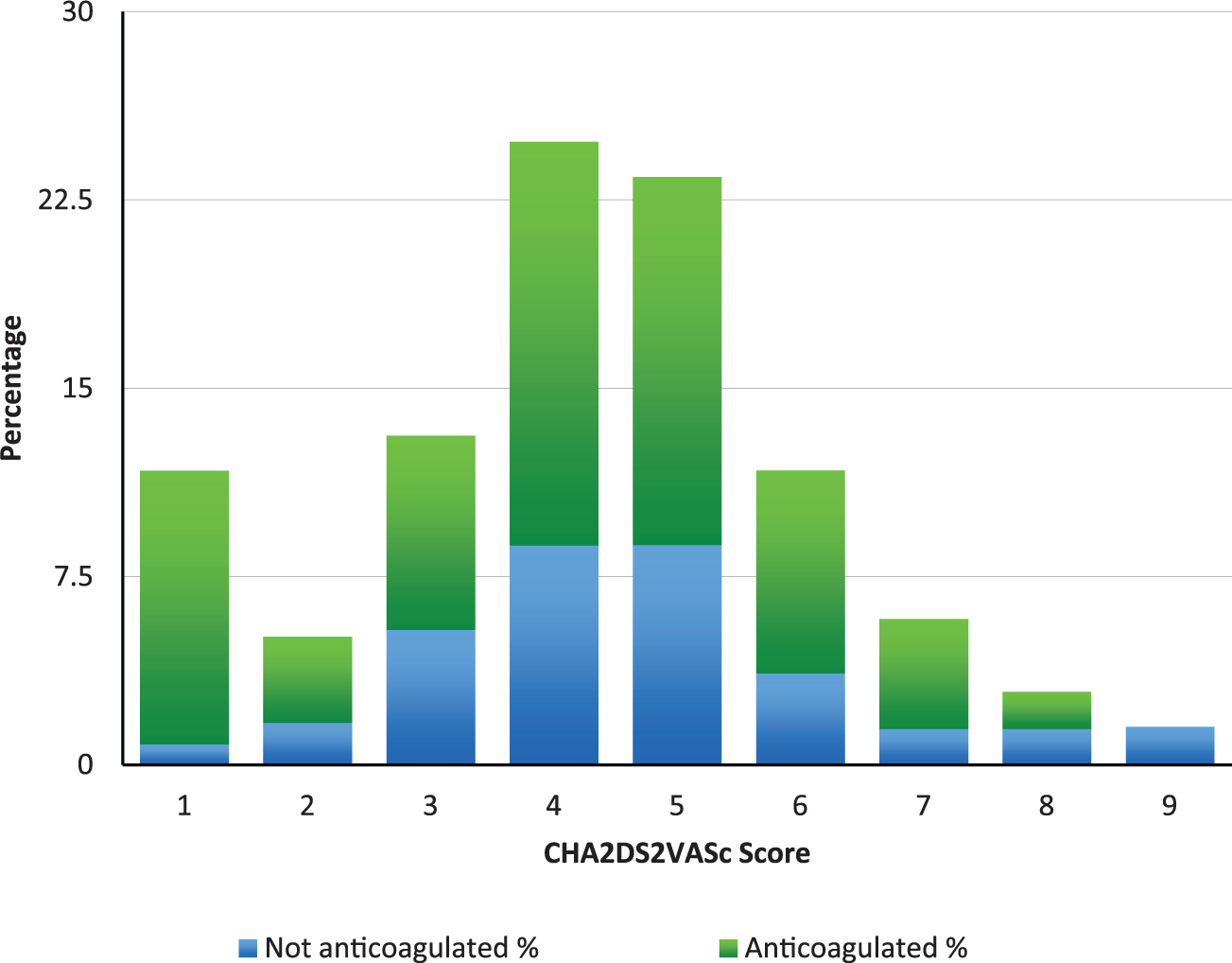
Stroke risk distribution at discharge based on treatment with or without anticoagulant drugs.
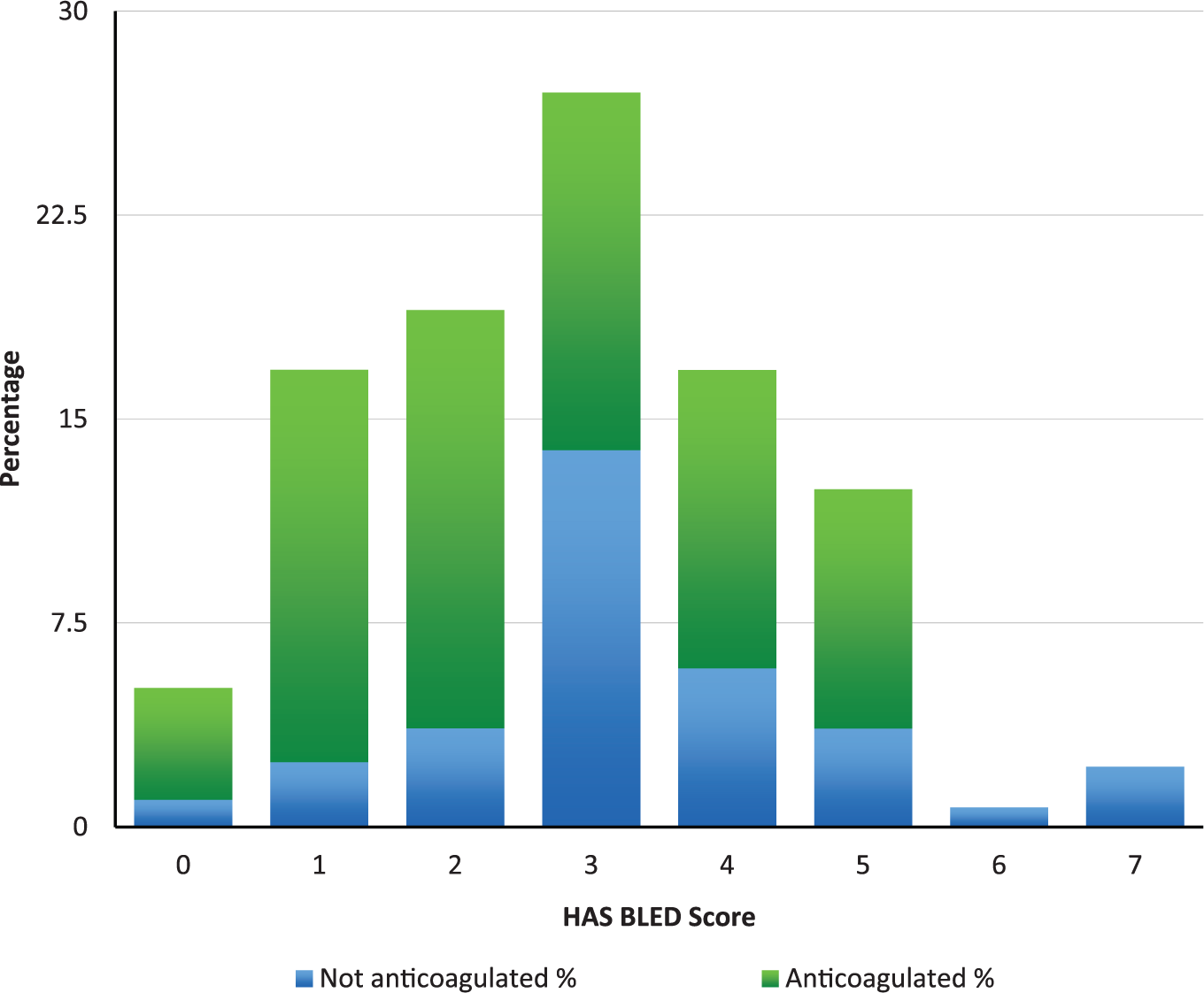
Bleeding risk distribution at discharge based on treatment with or without anticoagulant drugs.
Poorer self-reported heart failure self-care behaviour (p=0.010) and having a resuscitation status as ‘not for cardiopulmonary resuscitation’ (p=0.038) were associated with not receiving anticoagulant drugs at discharge. Sixty-three per cent of 58 patients were classified as frail. Although statistical significance was not achieved, being frail and having a higher comorbidity were associated with not receiving anticoagulant drugs at discharge. When the categories of non-frail and pre-frail were combined, frailty was associated with a suboptimum prescription of anticoagulant in patients with CHF and concomitant AF (78 vs. 58%; p= 0.081).
12-month outcomes
All-cause readmission to hospital was frequent (68%) and the 12-month all-cause mortality was high (29%) (Figure 4; Table 2). The prescription of anticoagulant drugs at discharge was significantly associated with a lower mortality at 12 months, but was not associated with lower rates of readmission to hospital among patients with CHF and concomitant AF. Patients prescribed anticoagulant drugs at discharge had lower unadjusted rates of all-cause mortality (23 vs. 40%; p=0.037) at 12 months (Figure 5). All-cause mortality at 12 months in patients receiving anticoagulant drugs was almost half that of patients not receiving anticoagulant drugs at baseline (p=0.037; hazards ratio (HR) 0.506; 95% confidence interval (CI) 0.267–0.956).
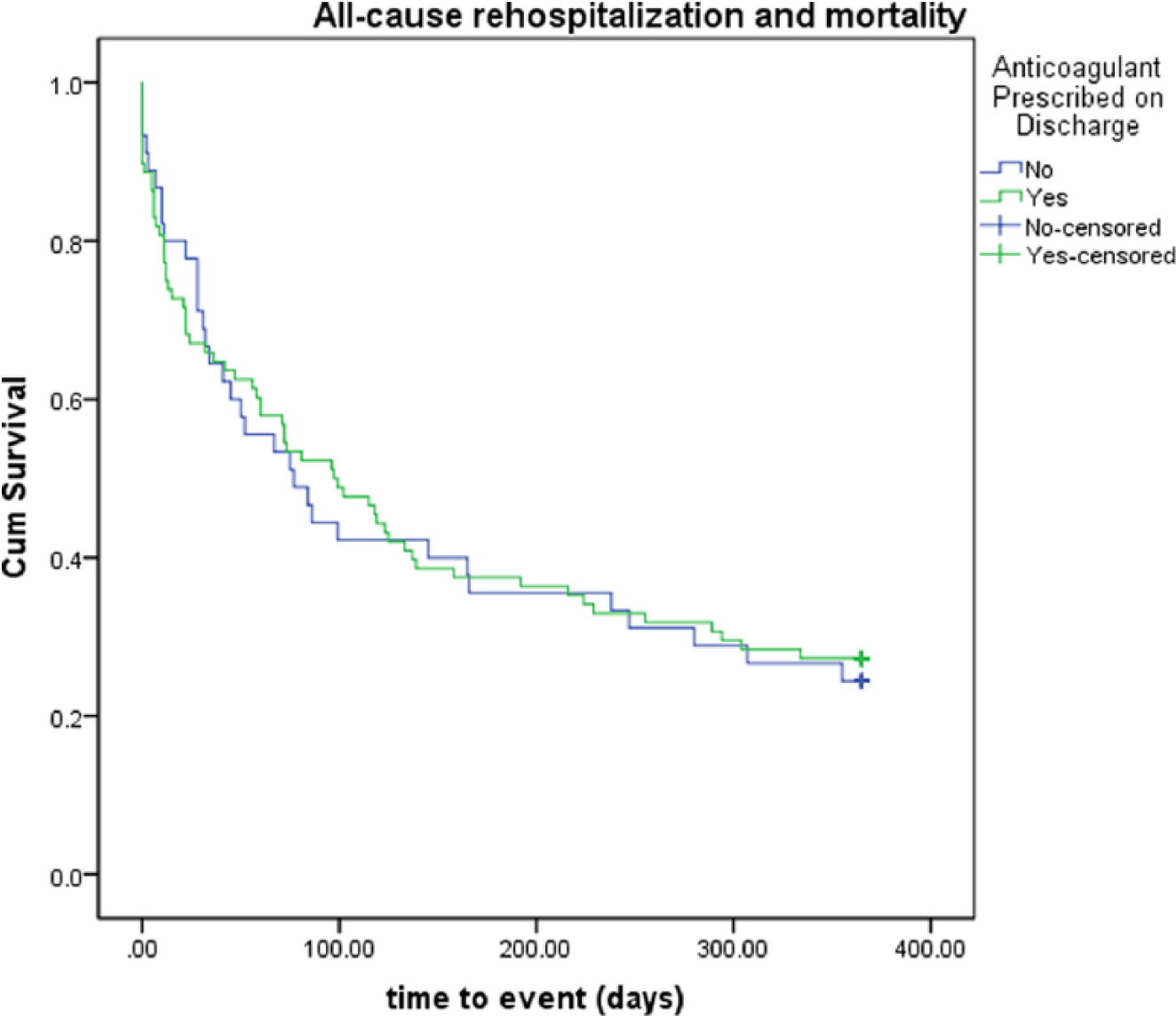
Kaplan–Meier survival analysis for composite endpoint of all-cause admission to hospital and mortality.
Unadjusted events at 12 months after admission to hospital.

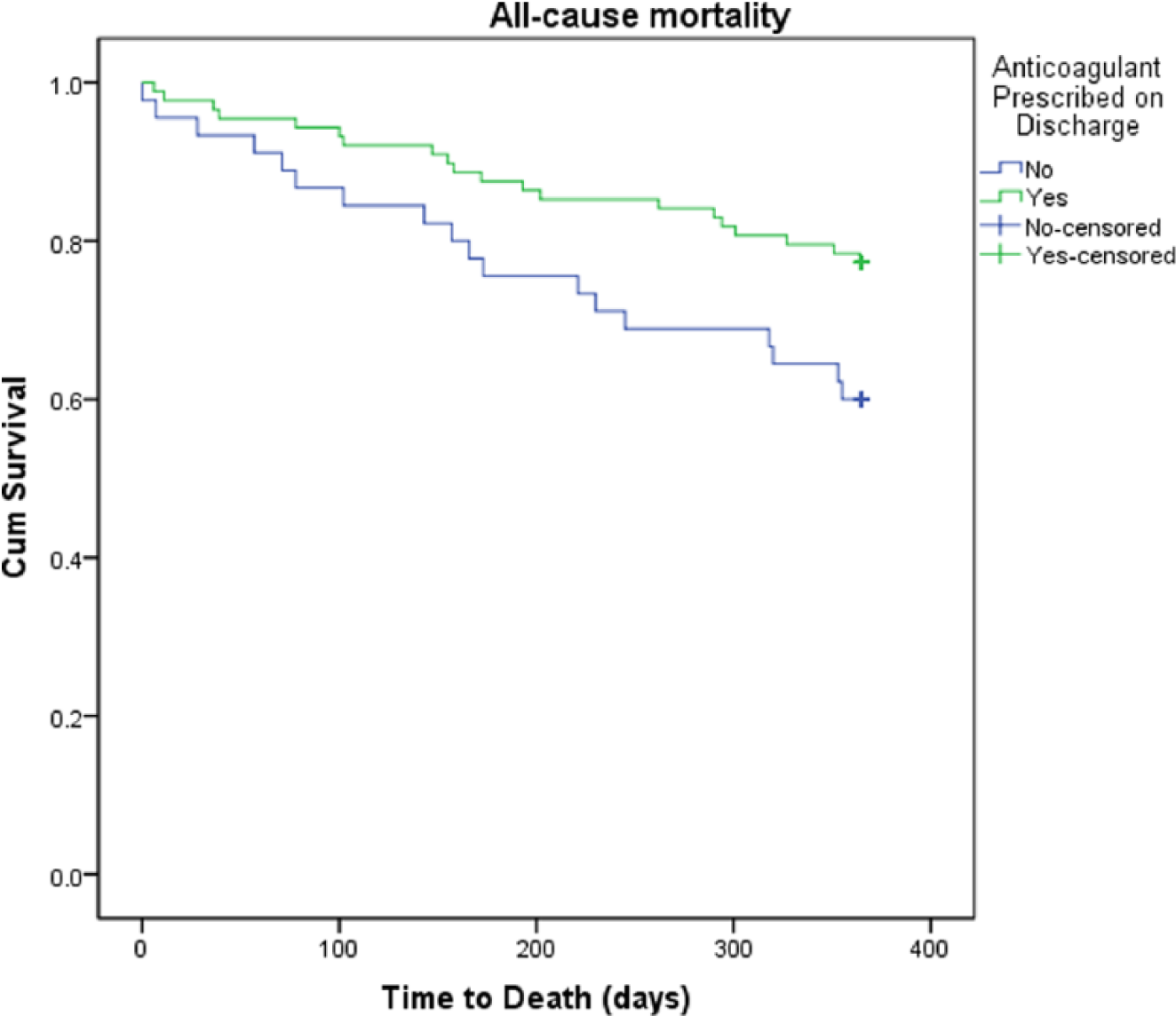
Kaplan–Meier survival analysis for all-cause mortality.
Discussion
The 43% incidence of AF in patients with CHF within our overarching screening sample is consistent with other studies. 24 This study demonstrates that thromboprophylaxis is underused in this frail, elderly, high-risk cohort. Our findings are similar to those reported in existing studies and systematic review data. 4 There is scope for improvement in thromboprophylaxis for stroke prevention in these patients.
Most patients in the group who did not receive anticoagulant drugs were prescribed antiplatelet drugs at discharge (70% compared with 27% in the group who received anticoagulant drugs; p=<0.01). This could be explained by coexistent coronary artery disease (52%) or separate carotid disease (20% previous stroke or TIA). This suggests that clinicians are prepared to prescribe an antiplatelet drug as thromboprophylaxis in some patients under circumstances in which they are not prepared to use oral anticoagulant drugs.
Within the AFASTER cohort, 56% of patients were prescribed β-blockers at the time of discharge from hospital. A recent study by Kotecha et al. 25 found that the use of β-blockers led to a significant reduction in all-cause mortality in patients with sinus rhythm (HR 0.73, CI 0.67–0.80; p<0.001), but not in patients with AF (HR 0.97, 95% CI 0.83–1.14; p=0.73), with a significant p value for interaction of the baseline rhythm (p=0.002). The study authors recommended that β-blockers should not be used preferentially over other rate-control drugs and should not be regarded as standard treatment to improve the prognosis in patients with concomitant heart failure and AF.
Importance of considering multi-morbidity
CHF and AF occur with a complex interplay. They seldom exist independently of other comorbidities and cardiovascular risk factors.26,27 Multi-morbidity, including AF, adds to the complexity of care management for patients with CHF. Clinical practice guidelines have a vital role in the translation of evidence into practice and the improvement in quality of care for patients with chronic conditions. However, in patients with multi-morbidities, the application of key care recommendations may lead to polypharmacy and an overwhelming treatment burden. 28 This may negatively affect their adherence to treatment regimens, including thromboprophylaxis.
There is robust evidence that the use of thromboprophylaxis (including warfarin, dabigatran, rivaroxaban and apixaban) significantly reduces the risk of stroke in patients with CHF and AF. In contrast, there is insufficient evidence to support the use of anticoagulant drugs in CHF alone. 29 Systematic review evidence reveals that thromboprophylaxis in patients with AF continues to be underused in clinical practice. 4 International data from the Global Anticoagulant Registry in the FIELD registry draws attention to the concern that thromboprophylaxis is not being best used in accordance with stroke risk scores and guidelines. These data, which include 10,641 participants, also highlight the overuse of thromboprophylaxis in low-risk patients and underuse in those at high risk of stroke. 27 The decision to treat high-risk patients with thromboprophylaxis is a complex choice for patients, caregivers and healthcare providers. 30 Previous research has highlighted the frequent mismatch between patient and clinician values in the context of decision-making. 31 For example, physicians are likely to advocate against thromboprophylaxis when patients would choose it and, in contrast, patients are likely to be prescribed treatment they would not choose. 31 Treatment decisions around thromboprophylaxis ought to be patient-centred. They must be considered in the context of the best evidence to date, within the scope of the clinician’s expertise, and be a treatment that is central to the individual patient’s situation, knowledge, attitudes, values and beliefs. 30
Luong et al. 32 emphasized the importance of recognizing that, although stroke continues to be the most worrisome consequence of AF, it is not the primary cause of death in patients with AF. The increased utilization of anticoagulant drugs in the last three decades has seen a decrease in the incidence of stroke in patients with AF. 33 However, there has been no reduction in mortality, regardless of effective thromboprophylaxis. This highlights that stroke is not the best predictor of mortality in patients with AF. These patients are more likely to die as a result of heart failure than from a stroke.32,34
Guideline-based treatment in the context of multi-morbidity
There is a need to address comorbidity in the provision of patient-centred care. Guidance incongruence and recommendation divergence may exist for complex patients, when recommendations are based on a singular comorbidity. Guideline blending is needed for similar chronic conditions. 28 There is scope for the amalgamation of CHF and AF practice guidance and future models of the delivery of a long-term care service. There is also a need to tailor clinical practice guidelines to account for clinical judgement, acknowledging the role of the patient throughout person-centred models of care. 35
High risk of readmission to hospital and death
The prevalence of CHF and AF are predicted to increase, with the incidence of AF expected to double in the next 20 years. 36 The prevalence of AF increases with the severity of CHF, as defined by the NYHA functional class. 37 Readmission to hospital is common and costly for both chronic conditions. Over 50% of patients with CHF are readmitted to hospital within six months and approximately 40% of patients with AF are readmitted within 12 months.38,39 Pre-existing AF has been previously established as an independent predictor of 30-day readmission for patients with CHF in an analysis using data from 3758 patients enrolled in the AFA Get-with-the-Guidelines registry from 2007 to 2010. 40 These data suggest that patients with CHF and AF had 1.39 times increased odds of readmission than those with CHF without AF. From this cohort, 21% (780/3758) patients were admitted to hospital within 30 days. 40 Patients who experience a CHF-related admission to hospital have more than double the likelihood of not being alive within two years. 41 CHF-related admission to hospital is a recognized indicator of syndrome progression and is associated with poor outcomes. 41
Despite recent advances in healthcare technology and pharmacotherapy, CHF continues to place a large burden on the healthcare budget. 42 The annual cost of heart failure was recently estimated at 2% of the total US healthcare budget, amounting to US$39.2 billion in 2010. Almost 60% of these costs are related to hospital care. 42 There has been renewed attention and debate on innovative methods to prevent potentially avoidable HF-related admissions to hospital.
Living alone and frailty as risk factors for increased admission to hospital and mortality
Previous studies have demonstrated that living alone and loneliness are predictors of increased mortality. Data from the Global Reduction of Atherothrombosis for Continued Health Registry, which followed up 44,573 participants aged ⩾45 years from 44 countries for four years, showed that 19% (8594/44,573) of this cohort lived alone. Living alone was associated with a higher four-year mortality. 43
Associations between frailty and adverse outcomes (including readmission to hospital and mortality) have previously been established. Poorer outcomes are evidenced with increasing severity of frailty. 44 Fried et al., 45 using data from the Cardiovascular Health Study, which included 5317 participants with a seven-year follow-up, identified poorer outcomes for severely frail patients when compared with patients with intermediate frailty, including admission to hospital (HR 1.27, 95% CI 1.11–1.46 vs. HR 1.11, 95% CI 1.03–1.19) and mortality (HR 1.63, 95% CI 1.27–2.08 vs. HR 1.32, 95% CI 1.13–1.55). Similarly, previous research by Perera et al. 46 has demonstrated that frail elderly inpatients with AF are less likely to receive warfarin than non-frail patients (p<0.001) and appear more susceptible to adverse outcomes, regardless of treatment with or without thromboprophylaxis.
Self-care behaviour
Our finding of poorer self-reported heart failure self-care behaviour associated with not receiving anticoagulant drugs at discharge should be interpreted with caution, given some missing data. It is widely recognized, however, that self-care behaviour is an important measurement in improving other important outcomes, such as reduced admission to hospital and mortality. 47 There remains a need for the development and validation of tools for the assessment of self-care behaviour in AF. To date, much research has focused on self-care behaviour in patients with heart failure and the quality of self-care behaviour in patients with AF remains to be clearly defined within the nursing literature.
Patient preferences
Although our study has revealed that only 66% of participants received anticoagulant drugs at discharge, the reasons for the non-prescription of these drugs warrants deeper exploration within future studies. Our study highlights that barriers remain for the prescription of stroke thromboprophylaxis for patients with CHF and AF. It is increasingly recognized that shared decision-making has the ability to improve treatment choices for patients and may favourably affect adherence to treatment regimens and patient outcomes. Recent research by Siouta et al. 48 draws attention to improvements in clinician–patient relationships to create the optimum climate for patient partnerships in clinical consultations. It is important that patients and caregivers are viewed as active partners in clinical decision-making for anticoagulant drugs and not as passive recipients of clinician-led decisions. Importantly, the conversation ought to be bidirectional, with supportive and clear conversation that builds confidence.48,49
Limitations
This study has some limitations. First, the SHARE-FI is not validated for use in the inpatient setting, 23 although it is quick and simple to conduct in an acute inpatient setting. Initially developed for the community setting, it has not been validated for the heart failure population in an inpatient setting. Second, participants with cognitive dysfunction and those speaking languages other than English were excluded from some measures, including the assessment of frailty, heart failure, self-care behaviour and self-reported adherence to medication. Third, the outcome assessment of stroke/TIA and bleeding events were often self-reported. Stroke was confirmed by via electronic methods where a computed tomography brain report was available. Fourth, the status of living alone was obtained via a review of the medical records. Although statistical significance was not achieved to compare differences in multi-morbidity and frailty, the values trended towards significance. Therefore a larger and more comprehensive snapshot that provides prospective observational data is recommended. The majority of our cohort were English-speaking with a white ethnic background, thus limiting the utility and generalizability of this research. In spite of these limitations, this study has several strengths. This study offered a detailed insight using multiple, routinely collectable clinical variables. Selection bias was reduced through the recruitment of prospective consecutive participants and the waiver of consent for enrolment at baseline.
Conclusion and implications
The results of our study demonstrate that thromboprophylaxis was underused in this frail, elderly and high-risk cohort. All-cause readmission to hospital was frequent and the 12-month all-cause mortality was high. The prescription of anticoagulant drugs at discharge was significantly associated with an improved mortality at 12 months, but was not associated with improved rates of readmission to hospital among patients with CHF and concomitant AF. This study highlights that frailty, multi-morbidity and self-care abilities are important considerations in thromboprophylaxis decision-making. Patients and caregivers must be central to treatment choices for thromboprophylaxis, although the CHA2DS2VASc and HAS-BLED schemata are useful in practice to risk-stratify stroke and bleeding. It is problematic to simply use these tools in isolation to guide treatment decisions. Although helpful, they lack the ability to provide a comprehensive assessment that includes key considerations including multi-morbidity, frailty and self-care ability.
Footnotes
Acknowledgements
The research team acknowledges Christine Hwang (heart failure research nurse), Kim Bardsley and Carol Whitfield (heart failure nurse practitioners) for their assistance with participant screening and recruitment. CF contributed to the study design, data collection, data analysis and interpretation, manuscript preparation. SI contributed to the study design, data interpretation, manuscript preparation. PJN contributed to the study design, data collection, data analysis and interpretation, manuscript preparation. SM contributed to preparation of the manuscript. PSM contributed to the study design, data interpretation, manuscript preparation. PMD contributed to the study design, data collection, data analysis and interpretation, and manuscript preparation.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article. This research received funding from the Australian College of Nursing through a grant of AUS $5000 awarded in 2013. Caleb Ferguson is currently supported by a UTS Doctoral Scholarship (2012–2015). Sally C. Inglis is currently supported by a Cardiovascular Research Network Life Science Research Fellowship supported by the Heart Foundation and the NSW Office for Medical Research (CR 11S 6226).
Although the CHA2DS2VASc and HAS-BLED models are useful tools in clinical practice to stratify stroke and bleeding risk, they do not consider other important factors in thromboprophylaxis decision-making and should not be used in isolation. Although preventing stroke is important in this high-risk cohort of patients, the rates of readmission to hospital and mortality are very high and are often related to the management of heart failure symptoms. Future research should explore clinicians’ fear and patient choice in thromboprophylaxis. Optimizing atrial fibrillation management needs to be considered in the context of multi-morbidity, frailty, self-care ability, cognitive functioning and caregiver support. There is need to target clinical interventions that improve self-care behaviour and self-management of atrial fibrillation in the setting of chronic heart failure.