
Abstract
Background:
For both patients and clinicians, differences between older and new anticoagulants have major implications for treatment selection, day-to-day management of therapy and adherence.
Aims:
To explore patients’ preferences for warfarin versus direct oral anticoagulant (DOAC) therapy.
Methods:
Mixed-method study involving anticoagulated older patients admitted to hospital. Part A comprised a vignette-based questionnaire; patients were asked whether they preferred Medicine A (warfarin) or Medicine B (DOAC). Part B interviews explored patients’ satisfaction with their current anticoagulant. Responses were thematically analysed.
Results:
Forty patients participated: 23 warfarin-treated, 17 DOAC-treated. Collectively, Parts A and B identified that most patients were satisfied with their current therapy (warfarin or DOAC), expressing reluctance to change to alternatives. Among patients who were able to numerically rate their satisfaction with therapy, most were ‘satisfied’ with their current anticoagulant, although warfarin-treated patients were slightly less ‘satisfied’ (median score 3.5) than those on DOACs (median score 5.0). Despite this, warfarin-treated patients still preferred their current therapy (over DOACs) due to familiarity and the security of regular international normalised ratio (INR) monitoring; those who preferred DOACs cited previous warfarin-related bleeding and unstable INRs as key reasons. DOAC-treated patients who preferred warfarin perceived regular monitoring as a major advantage; only those having had negative experiences with warfarin clearly preferred DOACs.
Conclusion:
Most patients accepted their currently prescribed anticoagulant, be it warfarin or DOACs. Features of specific anticoagulants, such as regular monitoring with warfarin, were perceived variably – some patients cited them as advantages and others as disadvantages. The clearest preference identified was for the agent already being taken.
Keywords
Introduction
To overcome the inherent challenges of traditional oral anticoagulant therapy (warfarin), new pharmacological entities have been developed. The direct oral anticoagulants (DOACs), also known as non-vitamin K antagonist oral anticoagulants, 1 have become available for use: dabigatran etexilate, rivaroxaban and apixaban. These newer agents are non-inferior to warfarin for stroke and systemic embolism prevention and are at least as safe as warfarin in terms of bleeding risk.2–4 However, compared with warfarin, they maintain key differences in their practical use, including dosing regimens, potential for drug and food interactions, and monitoring requirements. 5 For both the patient and the clinician, these differences have major implications for the initial selection of treatment as well as in the day-to-day management of therapy.6,7 This is particularly important for patients who have atrial fibrillation (AF), where long-term (life-long) anticoagulation is indicated for the prevention of stroke. 8 The European ‘Future of Anticoagulation Initiative’ (FAI) reports that the total cost-burden of AF in the European Union is approximately €26–30 billion, and that the prevalence of AF among adults over the age of 55 years is expected to double from 8.8 to 17.9 million between 2010 and 2060. 9
In its recommendations for care, the FAI report also emphasises a need for continued improvement in patient stratification and personalisation of care, 10 which must necessarily extend to the selection of treatment. The European Society of Cardiology (ESC) guidelines state that within the available treatments, DOACs may be preferable to warfarin for most AF patients, although no individual DOAC can be recommended over another. 11 For this reason, there is much variability in guideline recommendations internationally, including across European countries. 9 In choosing among the available anticoagulants, some clinicians may perceive that patients would prefer DOAC therapy. However, international studies have shown that warfarin may not be as burdensome to patients as often presumed, with minimal effect on quality of life.12,13 To date, there is a relative paucity of data regarding patient perspectives on the new anticoagulants, such that decision-making is often informed largely from the clinician’s perspective. To engage patients in therapeutic decision-making, optimise treatment satisfaction and improve adherence,14–17 further exploration of their views on these therapies is warranted. Therefore, the aim of this study was to explore patients’ preferences around anticoagulant therapy in the local setting, i.e., in a real-world, clinical practice setting in Sydney, Australia. The specific objectives were to: (1) identify patient’s preferences for warfarin versus DOAC therapy; and (2) explore the aspects of anticoagulant therapy that affect patient preferences for ‘older’ versus ‘newer’ therapies.
Methods
Study Design
A mixed method study was conducted over a 3-month period (August–October 2015), comprising two parts: Part A (brief vignette-based questionnaire) and Part B (patient interview). The study was conducted in a large (>900 bed) metropolitan teaching hospital in western Sydney (New South Wales, Australia), representing a demographically diverse patient population and where admissions for cardiovascular indications are common. Ethics approval was received from the Local Health District Human Research and Ethics Committee (HREC reference number LNR/14/WMEAD/248; SSA reference LNRSSA/14/WMEAD/274).
Participants
Patients were recruited via purposive sampling using the hospital as the sampling frame. Admissions to the target wards (e.g. cardiology, aged care, stroke unit) were screened by the lead researcher to identify patients meeting the inclusion criteria: patients aged ≥ 65 years with a diagnosis of AF (per medical records); currently taking an oral anticoagulant (irrespective of agent used or duration of therapy); fluent in English; cognitively intact (verified by nursing and medical staff and/or Mini-mental State Examination scores); without severe communication barriers (e.g. profound hearing or visual impairment); and able to provide informed written consent to participate. The criteria focused on recruiting those who were most likely to need, and be offered, long-term anticoagulation, rather than all patients prescribed oral anticoagulants for other indications, such as systemic embolism. This decision to focus on AF was based on targeting the largest (and increasing) group of patients using anticoagulation specifically for prophylaxis of a high-risk event; medication adherence is reportedly lower when medications are used for asymptomatic indications (e.g. prevention) rather than for symptomatic conditions (e.g. active treatment). 18
Data collection
De-identified background information about each patient (i.e. age, gender, comorbidities, current medication) was extracted from clinical notes and medical records. A purpose-designed questionnaire and interview guide were used to collect data. The interviews were audio (digitally) recorded, de-identified and then transcribed verbatim by an independent transcription service.
Part A: vignette-based questionnaire
A vignette-based questionnaire comprises a set of vignettes (i.e. scenarios describing various situations, treatments, or outcomes), accompanied by a questionnaire to explore participants responses (e.g. perspectives, preferences, behaviours, actions) to each. In Part A, the lead researcher presented to patients two vignettes, each depicting a different anticoagulant: a traditional agent (i.e. warfarin) and a relatively newer agent (i.e. dabigatran). Dabigatran was chosen as the alternative therapy, given that it was the first DOAC used in practice and because it had a greater number of differences to warfarin amongst the available DOACs (e.g. frequency of dosing, non-bleeding side-effects). The vignettes were purpose-designed by the research team using an iterative feedback process. Each separate vignette was provided in hardcopy (A4 size sheet), in large type (size 16 font) text for ease of readability by patients. Each vignette briefly described how that specific medicine was normally taken (i.e. number of doses per day, with or without food), including its practical management (i.e. monitoring requirements, follow-up visits, dosage adjustments, any interactions) and common side-effects (including whether specific antidotes were available for reversal of anticoagulation in the event of major bleeding). Neither vignette stated the actual name of the medicine, but was labelled ‘Information about Medicine A’ and ‘Information about Medicine B’ for warfarin and dabigatran, respectively. After reviewing both vignettes, the patient was given time to compare the two treatment options. A brief questionnaire was used to elicit the patient’s responses to each vignette: specifically, whether they were familiar with either therapy; their preference for either of the two options; their willingness to take each option if it were offered or prescribed to them; main perceived advantage and disadvantage of either option; and a rating of their satisfaction with their current therapy relative to the alternative therapy presented in the vignette. Satisfaction was rated on a standard Likert scale (1 = very dissatisfied, 2 – somewhat dissatisfied, 3 – neither dissatisfied nor satisfied, 4 = satisfied, 5= very satisfied), in response to the following custom-designed question: ‘In thinking about the
Part B: patient interview
After completing Part A, the same patients completed Part B, which explored in-depth patients’ treatment satisfaction, and perspectives regarding the advantages and disadvantages of their
What are your overall thoughts about your current therapy?
Prompts: What are the good parts and bad parts about it? Do you have any concerns about this therapy? What are you concerned about?
What have been some of the biggest challenges in using this medication?
Prompts: monitoring, diet, adherence, dose adjustment and frequency of administration, drug–drug interactions, side-effects: risk of bleeding
If the doctor recommended an alternative therapy, like the one in this scenario, would you be willing to change to it?
Data analysis
Quantitative data were analysed using descriptive statistics in Microsoft Excel™ and IBM SPSS 23.0™. Inferential statistics were used to explore potential differences in patient subgroups; T-tests and Mann-Whitney U test were used to test for mean and median differences in continuous variables (for parametric and non-parametric distributions, respectively), whilst the Chi-square test examined differences in independent proportions. Thematic analysis of the interviews involved manual inductive coding. For reliability, two researchers independently analysed the transcripts before coming together to derive consensus on the findings (theme verification). Respondent validation was attained by forwarding a summary report of the findings to selected participants for their verification and feedback.
Sample Size
For the quantitative component (in Part A), the sample size calculation was based on attribute sampling; to detect an 80% willingness of patients to stay with their current treatment (with 10% precision, 95% confidence), 40 patients were required. For the qualitative component (Part B interviews), the target sample size was based on the number of patients required to achieve theme saturation; typically, this involves initially starting with a minimum of 6–8 persons for each main topic group, and continuing recruitment until no new themes emerge during the data collection (13). To account for incomplete interviews and potential variability in responses between patients using warfarin versus a DOAC, the sample size was doubled (and an overage added), such that approximately 20 patients were needed for Part B. Based on 3–4 interviews being conducted per day, a maximum of 40 patients could be feasibly recruited over the 3-month study period.
Results
Participant characteristics
Forty patients participated in the study, having completed both Parts A and B; the participant characteristics and response to the Part A vignettes are presented in Table 1. All were using anticoagulants for AF, and one patient additionally had prosthetic heart valves. Just over half (57.5%) were taking warfarin at the time of interview, and the remainder used DOACS (mostly apixaban, n = 7). Five patients used combination antithrombotic therapy: three were using warfarin ± an antiplatelet agent, two were using apixaban ± an antiplatelet agent. Among the four patients with new onset AF, three were initiated on apixaban during this hospital admission, one commenced warfarin. Three patients had a prior history of adverse drug reactions to warfarin and all three were currently anticoagulated: one on apixaban (previous bleeding on warfarin), one on rivaroxaban (reported hair loss with previous warfarin use), and one on warfarin (history of subdural haematoma).
Participant characteristics and responses to Part A vignettes.
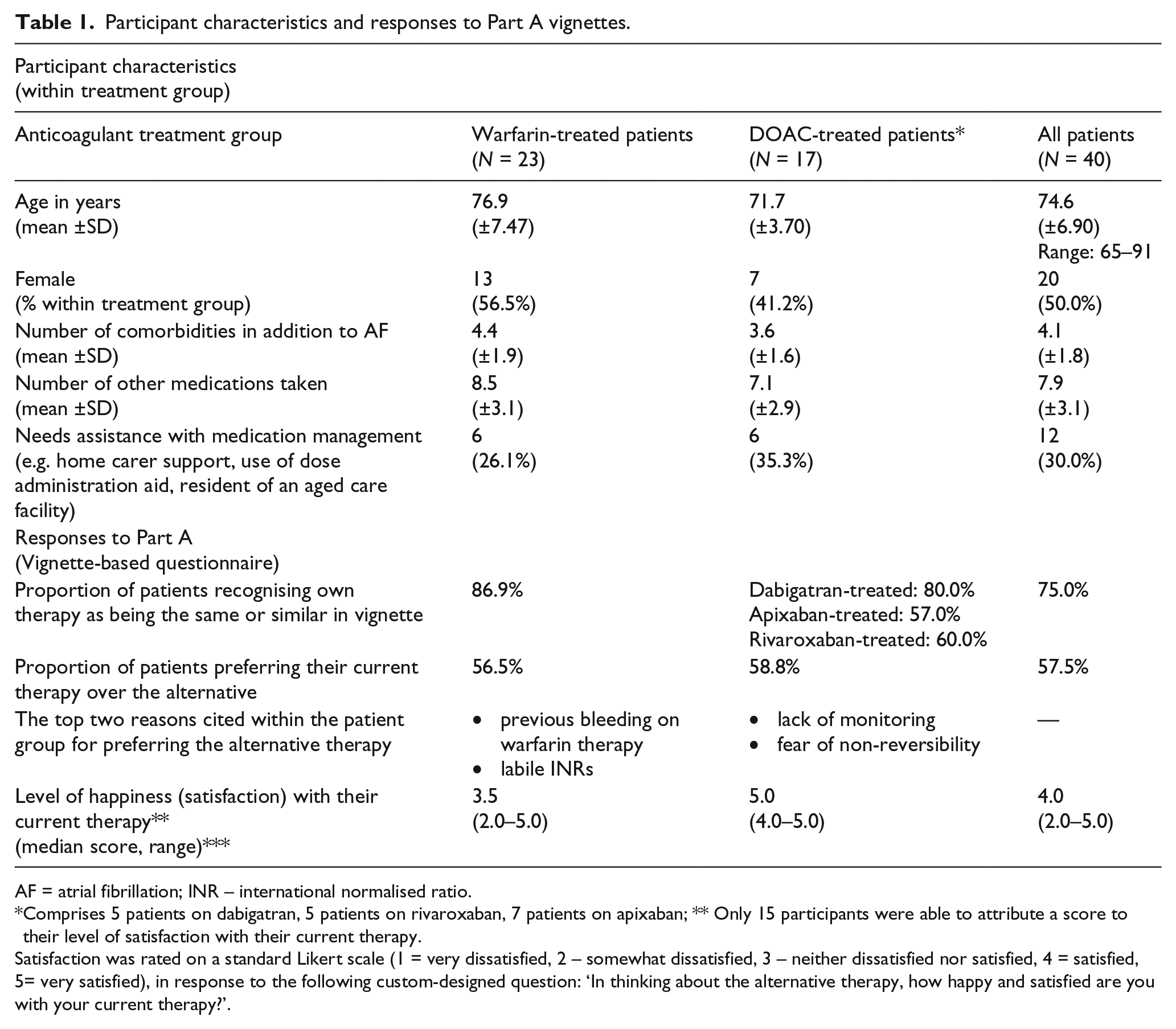
AF = atrial fibrillation; INR – international normalised ratio.
Comprises 5 patients on dabigatran, 5 patients on rivaroxaban, 7 patients on apixaban; ** Only 15 participants were able to attribute a score to their level of satisfaction with their current therapy.
Satisfaction was rated on a standard Likert scale (1 = very dissatisfied, 2 – somewhat dissatisfied, 3 – neither dissatisfied nor satisfied, 4 = satisfied, 5= very satisfied), in response to the following custom-designed question: ‘In thinking about the alternative therapy, how happy and satisfied are you with your current therapy?’.
There were no significant differences between warfarin- and DOAC-treated patients in terms of number of additional comorbidities (p = 0.23), number of medications taken (p = 0.15) or need for assistance with medication management (p = 0.53). However, the nature of medication assistance used differed across the two groups: among warfarin-treated patients, only one used a dose administration aid with the remainder relying on family members; among the DOAC-treated patients, all but one used dose administration aids and/or received medication management assistance through their residential care facility. Warfarin-treated patients were older than those using DOACs (p < 0.01).
Part A: responses to vignettes
Most participants recognised that their current therapy was the same or very similar to that presented in one of the vignettes; expectedly, a higher proportion of patients currently using warfarin and dabigatran were able to do so (Table 1). Only 15 patients were able to numerically rate their satisfaction with their current therapy in terms of assigning a score, leaving this question blank and preferring instead to describe their satisfaction in words to the researcher; among those that did assign a number, most were satisfied with their current therapy (score 4.0). Warfarin-treated patients were less satisfied with their current therapy than those on DOACs (Table 1). Despite lower satisfaction scores, a higher proportion of warfarin-treated patients preferred to stay on their current therapy than the alternative DOAC therapy presented in the vignette; those who preferred the DOAC vignette cited previous bleeding on warfarin and problems with being stabilised on warfarin (achieving stable international normalised ratios (INRs)) as key reasons for their preference. DOAC-treated patients who preferred the warfarin vignette cited regular monitoring as the key advantage.
Part B: themes (qualitative interviews)
From these interviews, five broad themes emerged: acceptance of current therapy; perceived necessity for monitoring; frequency of dosing; adverse effects associated with DOAC therapy; and, a lack of knowledge about therapy.
Theme: acceptance of current therapy
The most common theme identified was the patient’s acceptance of their current anticoagulant therapy (Table 2). For most patients, this translated to a preference for their current therapy, whether it was warfarin or a DOAC. In the case of warfarin, many patients stated they were ‘used to it’. Familiarity with therapy and established routines around its management seemed to be a key factor influencing their preference. Even among the few patients who expressed a dislike for certain aspects of their current therapy (e.g. INR monitoring or dietary restrictions associated with warfarin), which may have been obviated by the use of the alternative therapy presented in the vignette, they still preferred their current therapy.
Theme: acceptance of current therapy.
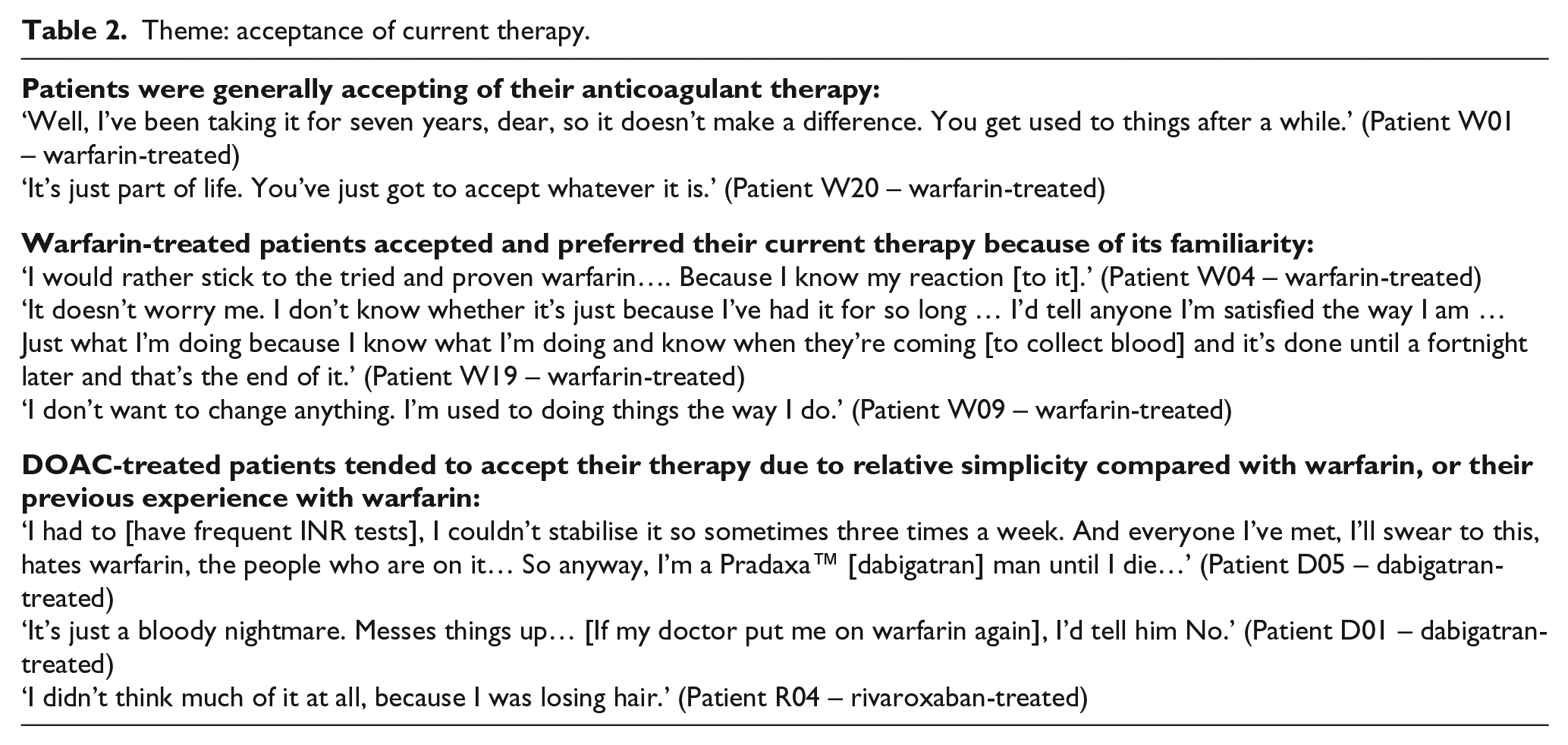
DOAC-treated patients tended to prefer this therapy largely due to previous negative experiences with warfarin, including serious bleeding events and labile INRs. Similarly, many of the warfarin-treated patients who stated that they preferred the DOAC vignette reported having experienced adverse effects, such as bleeding events or labile INRs, with their current therapy. However, some patients preferred the DOAC vignette for more practical reasons such as less frequent blood tests or the absence of significant food-drug interactions:
‘It would be nice [to have blood tests less often] because sometimes I’m so sick. He sends me up every second day or every day, you know.’ (Patient W07 – warfarin-treated)
Conversely, DOAC-treated patients who preferred warfarin largely perceived the more stringent therapeutic monitoring associated with warfarin as a key benefit:
‘I think it’s better because they monitor it and they know how it’s working, how it’s affecting me and all this, you know.’ (Patient A01 – apixaban-treated)
In a number of interviews, it was also clear that patients’ acceptance (or rejection) of therapy was heavily influenced by the experiences and reports from family or friends, rather than by their healthcare team:
‘[I don’t like warfarin] only because of the results of my friends’ (Patient A05 – apixaban-treated) ‘I was a bit worried because it [dabigatran] was only new on the market and I didn’t know, you know much, but my daughter from Queensland, she rang me and she says, mum, I’ve got a friend here who’s just started it… He said that it was very good but he didn’t have any side effects or anything.’ (Patient D04 – dabigatran-treated)
Even when contemplating alternative therapy, most participants defaulted to the opinions of their family or friends, prior to consulting their doctor:
‘No probably not but I could talk to my daughter about it, what they think and see what they’ve got to say. See whether it will work easier for me … or I can talk to my doctor.’ (Patient W08 – warfarin-treated)
However, when probed, most participants felt that they could discuss their treatment preferences with their doctor, even if there were differences of opinion:
‘Oh, yes, I mean, gosh yes, my dear, I can talk to them about medicines, my word, yes’ (Patient W06 – warfarin-treated) ‘There is no way I’d go back ever … well, I’d like [the doctor’s] advice … but, I’d give them the reasons why I don’t like warfarin’ (Patient D05 – dabigatran-treated)
Theme: perceived necessity for monitoring
Patients expressed a spectrum of attitudes toward the monitoring requirements associated with warfarin, ranging from nonchalance through to strong dislike (Table 3). However, there was a firm understanding that this was a necessary aspect of warfarin therapy, particularly amongst warfarin-treated patients who expressed a sense of security from this:
‘[I like that] it’s monitored more frequently. My system seems too up and down for no apparent reason.’ (Patient W20 – warfarin-treated)
Theme: perceived necessity for monitoring.
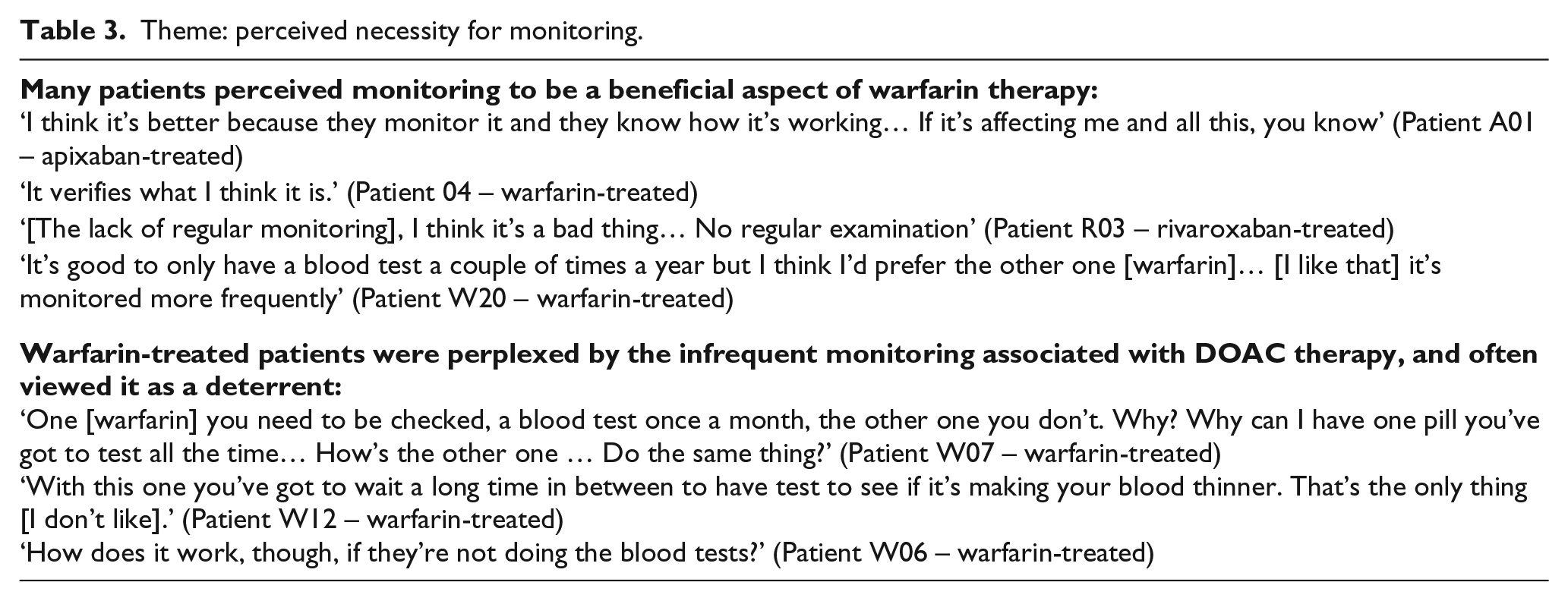
Concern and a lack of understanding around the low level of monitoring with DOAC therapy were often expressed by these patients. Many warfarin-treated patients found it difficult to comprehend why such differences would exist and were often reluctant to relinquish INR monitoring even if they disliked having it done:
‘I wouldn’t feel that safe with it [less frequent monitoring with a DOAC], would I?’ (Patient W17 – warfarin-treated)
Although more prevalent amongst warfarin-treated patients, some DOAC-treated patients also felt the lack of monitoring associated with newer therapies as a concern:
‘You’re probably getting too much and what, too late before you know it. Monitoring is a safety factor. I’ve been taking too much Pradaxa™ (dabigatran), they’re going to lower it.’ (Patient D03 – dabigatran-treated)
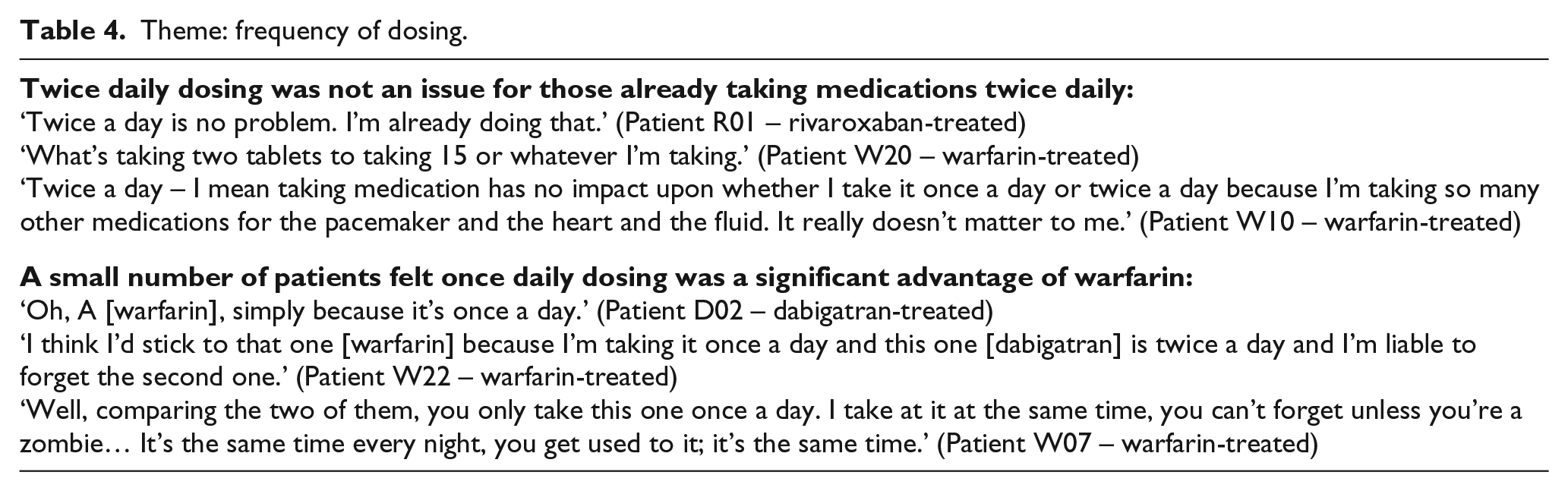
Theme: frequency of dosing
When comparing the frequency of dosing between warfarin (once daily) and the DOAC (dabigatran – twice daily), patients who were already taking medications twice daily in general did not perceive the twice daily regimen in the DOAC vignette as a barrier (Table 4):
‘Well, it’s not going to make any difference taking it night and morning because I take tablets morning and night.’ (Patient W23 – warfarin-treated)
Theme: frequency of dosing.
In some cases, patients also felt it would not be problematic as they had assistance managing their medications:
‘Doesn’t matter, because it’s all in a Webster™ (blister) pack anyway’ (Patient A03 – apixaban-treated)
While the majority of patients did not feel twice daily dosing would be an issue, a small number of patients did, expressing that it would be difficult to remember the second dose. These patients felt that twice daily dosing was a more significant barrier to using the therapy than INR monitoring (and associated dose changes) and therefore expressed a preference for warfarin.
Theme: adverse effects associated with DOAC therapy
Warfarin-treated patients were relatively less concerned about side-effects than DOAC-treated patients. The potential side-effects associated with DOACs were an issue for many patients, including the risk of bleeding in the absence of an antidote:
‘… You always think if anything happens, you know, like they can’t stop it [the bleeding], they can’t reverse it. This is the worst thing.’ (Patient A02 – apixaban-treated)
Stomach upsets were most commonly highlighted as a concern by patients, more so than bruising or bleeding:
‘Stomach upsets. Bwah! Would not suit me.’ (Patient A04 – apixaban-treated) ‘I don’t like stomach upsets. I’ve always said I’d rather get a tooth out than vomit.’ (Patient W19 – warfarin-treated)
A small number of patients reported already experiencing side-effects as a result of their DOAC therapy:
‘I’ve been very well on it but there are side effects where you get excruciating pain from the top of your shoulder right down to your feet…. That chap, who was on Xarelto™ (rivaroxaban), they took him off it. He had diarrhoea as well as the pains.’ (Patient R02 – rivaroxaban-treated)
Theme: lack of knowledge about therapy
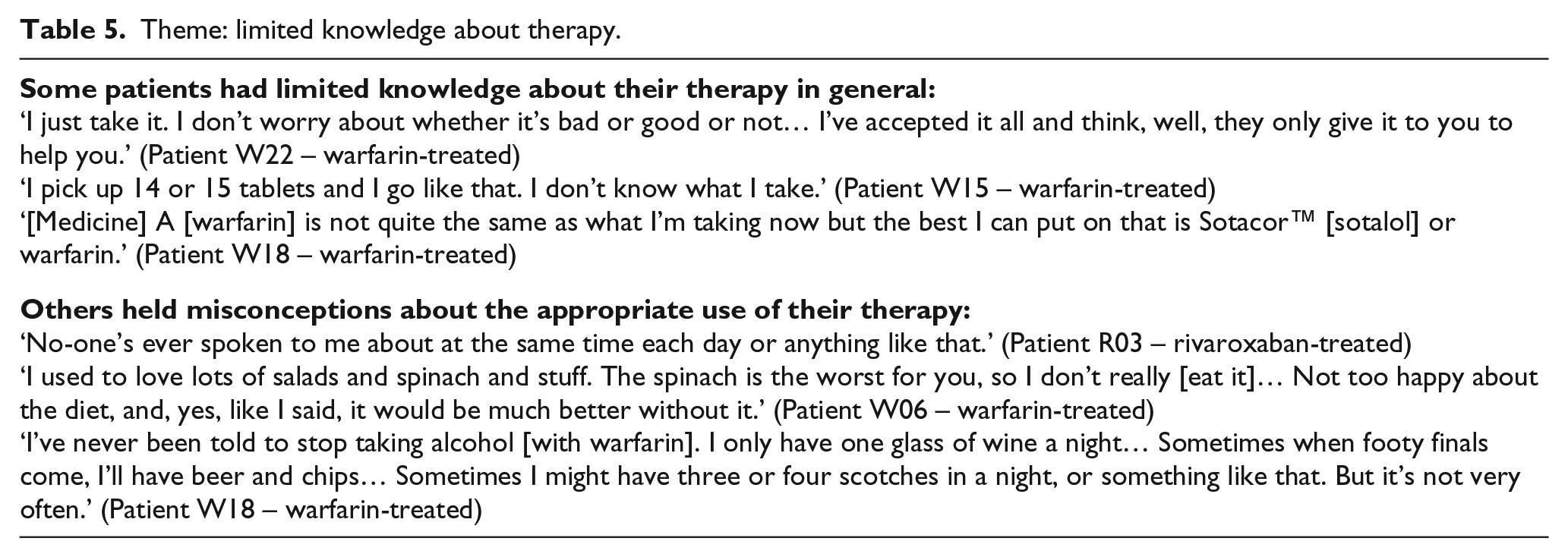
In exploring the treatment options, some patients’ responses highlighted significant deficits in their knowledge about their therapy (Table 5) including an inability to name their anticoagulant, inability to recognise their medication when presented in the vignettes, and uncertainty as to its role in the management of their health. Furthermore, patients often held misconceptions about their therapy, particularly in regard to interactions with food and alcohol in the case of warfarin. In a few patients, this lack of knowledge underpinned their disengagement from decision-making around therapy:
‘As I say, I do what I’m told to do, I don’t ask why, I just take it.’ (Patient R04 – rivaroxaban-treated)
Theme: limited knowledge about therapy.
Discussion
This study provides insight into the contemporary perspectives of patients regarding available anticoagulant therapies in the local setting. Overall, our study patients were satisfied with their current therapy, be it a DOAC or warfarin, and this finding is concordant with previous studies in warfarin-treated patients.13,19,20 The general acceptance of and tendency to prefer current therapy suggests that patients’ perspectives are intrinsically tied with their past treatment experiences. Furthermore, the opinions of family and friends influence their treatment preferences, despite good relationships and lines of communication with doctors. Previous studies have highlighted the importance of the patient-doctor relationship in influencing patient’s acceptance of anticoagulation, 21 , despite initial fears, anxieties and a lack of knowledge. 22 Although this study has focused on a local practice setting with a select group of participants, these findings may signal a potential evolution in the patient–doctor relationship, whereby patients feel more empowered to seek external advice and present their viewpoints to their doctor, in-line with the concept of the activated patient. 23 Indeed, patient engagement and empowerment are at the core of patient-centred care, 24 enabling shared decision-making, 25 and positively influencing treatment outcomes, 26 including medication adherence.27,28 Likewise, improvements in medication adherence have been shown to improve patient-centred outcomes. 29
Although often considered burdensome, INR monitoring may not have a significant impact on patient satisfaction.13,30,31 Patients, especially those who were warfarin-treated, often perceived the lack of monitoring with DOAC therapy as a deterrent to their use, a notion supported elsewhere.19,31 Gebler-Hughes et al. attribute this to patients perceiving less frequent monitoring (of INR) as an indicator of reduced contact time with their clinician. 19 However, our study suggests that patients also derive a sense of security from regular INR monitoring - most warfarin-treated patients expressed concerns about the lack of monitoring associated with DOAC therapy, and were unsure how an anticoagulant could be safely used without this close surveillance. Other studies have also highlighted that even among those patients who were not satisfied with their warfarin therapy there was hesitation about transitioning to alternative agents due to the lack of monitoring.31,32 Overall, patient complaints do not necessarily translate to a desire to change therapy. This may also explain why some patients were unable to assign a numerical value to their level of satisfaction with their current therapy; although some patients raised issues about their current therapy, they were overall happy to remain on it. From the clinician’s perspective, it should be seen as an opportunity to discuss patient concerns further, rather than a cue to alter treatment. The need to support and educate patients was highlighted by their perplexity about different monitoring requirements for warfarin compared to DOACs.
In regard to other practicalities of use, many patients did not perceive twice daily dosing to be problematic, since most were already taking other medication at least this often. This contrasts with Böttger et al.’s findings which identified once daily dosing as the factor most important to patients when choosing an anticoagulant. 33 However, their study recruited patients prescribed a once daily regimen (either warfarin or rivaroxaban), and clinicians might have already aligned their patients’ therapy with their preferences. While twice daily dosing was not perceived as problematic, our patients expressed concerns about side-effects associated with DOAC therapy, particularly the potential to cause stomach upset. Previous qualitative studies have also found gastrointestinal symptoms to be of concern to dabigatran-treated patients, accounting for nearly half of all forum comments relating to adverse effects. 32
Knowledge about anticoagulant therapy was generally superficial and scattered, with many patients unaware of its role in managing their health, consistent with previous research.22,34 This lack of knowledge was also evident in DOAC-treated patients. Similar to previous studies, this seemed to be coupled with unilateral decision-making, with patients describing a paternalistic approach to the decision to start or continue anticoagulant therapy. 34 This suggests that the education that patients receive from healthcare providers is, at times, ineffective. Aside from potentially leading to inappropriate use, poor knowledge may indicate that patients are disengaged from decision-making about their therapy, and are ill-equipped to participate in this process. A review by Pandya and Bajorek has highlighted the need to explicitly incorporate patients’ perspectives in decision-making processes for anticoagulant selection, which must address patients’ lack of knowledge about the purpose of anticoagulation, and the risks and benefits of treatment. 35 A previous qualitative study found that current methods for warfarin education, such as one-off counselling or provision of educational booklets, are insufficient for patients and carers in this regard. 7 A review by Nasser et al. identified that education resources about anticoagulation are most effective when they include simple written information as a supplement to verbal counselling alongside the use of purpose-designed communication tools such as cue cards, audio-visual resources depicting real-life scenarios, and/or socio-culturally appropriate images/figures. 10 Furthermore, O’Connor et al. describe the value of decision aids as important resources here, as they can present balanced personalised information about available options, enabling patients to arrive at informed judgments about the personal value of those options. 36
Pandya et al. have highlighted that patients’ engagement in shared decision-making and adherence to medicines may be undermined by the suboptimal quality of information provided in some resources, reinforcing that health professionals have an important role to play. 37 Aside from general practitioners and specialist doctors, the European FAI has emphasised that others can contribute in this regard, including pharmacies, care homes and carers, and specialist nurses. 9 Hendriks and co-workers have reported the various ways that nurses within an integrated chronic care model of management for AF can facilitate patient-centred care and shared-decision-making through structured patient education and activating self-management.38,39 Boswell and Bungard have likewise demonstrated the significant way in which pharmacists can support patient-centred care, including patient education, through the lens of a specialty anticoagulation clinic. 40 Collectively, the contemporary literature identifies various opportunities to utilise the expertise of nursing, pharmacy, and allied health professionals to deliver tailored and structured patient education, whilst utilising techniques such as motivational interviewing and resources such as decision-aids, to better support patients in this context. 41
In considering these findings, some limitations need to be acknowledged. First, this study primarily focussed on the practical aspects of oral anticoagulant use. However, decision-making is more complex, such that patients and clinicians also need to consider treatment safety and efficacy. Second, recent studies have also identified the non-reversibility associated with some DOAC therapy as a key concern for patients – a factor not considered in the dabigatran-based scenario presented to patients in this study, given the focus on day-to-day practicalities of use.19,32 Since the conduct of this study, an antidote (idarucizumab) has become available to reverse the actions of dabigatran, which may affect patients’ acceptance of the therapy. Third, all participants were already anticoagulated. Given the clear connection between current treatment and preferences, it is unknown how anticoagulant-naïve patients would respond. Finally, a key study limitation is the size of this study. Given the high prevalence of AF (i.e. approximately 2%, in the general population and >10% in persons aged ≥ 65 years), this was a relatively small study; as such, a small sample of patients selected from the local, Australian practice setting may not represent the preferences and perspectives of the thousands of patients encountered in other practice settings, whether in Australia or more globally. The small sample size also precludes an exploration of whether any patient characteristics may have affected patient preferences.
Conclusion
Most patients are accepting of their currently prescribed oral anticoagulant therapy, whether being treated with older therapy (i.e. warfarin) or newer therapy (i.e. a DOAC). Even patients who are reportedly dissatisfied with aspects of their current therapy still prefer their existing therapy than any alternative agents. Features of specific anticoagulants, such as the regular monitoring required with older therapy (i.e. warfarin), may be seen by patients as both an advantage and a disadvantage. Overall, there is no clear preference among patients for older versus newer anticoagulants, given that patients have variability in perspectives around specific agents.
Footnotes
Acknowledgements
The authors sincerely thank the clinical staff of the hospital wards for providing access to the patients for the purpose of the study interviews.
Declaration of Conflicting Interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Given the variability in patients’ values and preferences, it is difficult to predict which anticoagulant an individual may actually prefer to use. Health professionals must not assume that their expert assessment of the pharmacological and practical advantages and disadvantages of any particular therapy actually aligns with their patient’s preferences. There is a need to actively engage patients in therapeutic decisions to ensure that their prescribed regimen is not only clinically appropriate but sympathetic to their preferences and values. More effective education of patients is needed to improve their treatment knowledge, thereby better engaging and empowering them in the process of care. Nurses, pharmacists and allied health professionals have a role to play in educating patients and supporting them in their decision-making around treatment selection.