
Abstract
Objective:
The objective of this study was to assess the cost-effectiveness of a long-term, nurse-led, multidisciplinary programme of home/clinic visits in preventing progressive cardiac dysfunction in patients at risk of developing de novo chronic heart failure (CHF).
Methods:
A trial-based analysis was conducted alongside a pragmatic, single-centre, open-label, randomized controlled trial of 611 patients (mean age: 66 years) with subclinical cardiovascular diseases (without CHF) discharged to home from an Australian tertiary referral hospital. A nurse-led home and clinic-based programme (NIL-CHF intervention, n = 301) was compared with standard care (n=310) in terms of life-years, quality-adjusted life-years (QALYs) and healthcare costs. The uncertainty around the incremental cost and QALYs was quantified by bootstrap simulations and displayed on a cost-effectiveness plane.
Results:
During a median follow-up of 4.2 years, there were no significant between-group differences in life-years (−0.056, p=0.488) and QALYs (−0.072, p=0.399), which were lower in the NIL-CHF group. The NIL-CHF group had slightly lower all-cause hospitalization costs (AUD$2943 per person; p=0.219), cardiovascular-related hospitalization costs (AUD$1142; p=0.592) and a more pronounced reduction in emergency/unplanned hospitalization costs (AUD$4194 per person; p=0.024). When the cost of intervention was added to all-cause, cardiovascular and emergency-related readmissions, the reductions in the NIL-CHF group were AUD$2742 (p=0.313), AUD$941 (p=0.719) and AUD$3993 (p=0.046), respectively. At a willingness-to-pay threshold of AUD$50,000/QALY, the probability of the NIL-CHF intervention being better-valued was 19%.
Conclusions:
Compared with standard care, the NIL-CHF intervention was not a cost-effective strategy as life-years and QALYs were slightly lower in the NIL-CHF group. However, it was associated with modest reductions in emergency/unplanned readmission costs.
Keywords
Introduction
Chronic heart failure (CHF) is a costly and complex syndrome to treat. It remains the most frequent cause for hospital admission among elderly patients 1 and the proportion of CHF hospitalizations of patients below the age of 65 years has increased in the last decade. 2 This suggests a need for identifying high-risk younger patients directed to a systematic approach to preventing or delaying the onset of CHF. Given that many patients with subclinical cardiovascular disease (CVD) are known to have latent cardiac dysfunction that predisposes them to developing the full syndrome, 3 preventing cardiac dysfunction might be more cost-effective than managing the full syndrome in the long run. The Nurse-led Intervention for Less Chronic Heart Failure trial (NIL-CHF) was conducted to determine the effectiveness of a long-term, nurse-led, multidisciplinary programme of home/clinic visits in preventing progressive cardiac dysfunction in patients at risk of developing de novo CHF.4,5 As previously reported, the NIL-CHF intervention did not meet the primary endpoints for reducing all-cause mortality and readmissions from CHF or CVD; however, the intervention was associated with reduced emergency and CVD-related hospital stay and improved cardiac function over the long term. 4 The aim of this study was to conduct an economic evaluation of the NIL-CHF intervention versus standard post-discharge care as per the study protocol 5 and statistical analysis plan 6 where a cost-utility analysis was pre-specified.
Methods
A trial-based analysis was conducted to assess the cost-effectiveness of NIL-CHF intervention versus standard post-discharge care. The NIL-CHF trial was conducted between 2008 and 2013, the details of which have been previously published. 4 Briefly, prior to hospital discharge from a 390-bed tertiary-referral hospital in Australia, inpatients aged ≥45 years with overt cardiovascular disease (without CHF) or those actively treated for either of the two most common antecedents of CHF other than coronary heart disease (diabetes/metabolic syndrome or hypertension) were randomized into NIL-CHF (n=301) or standard care (n=310), respectively. 4 The NIL-CHF group received nurse-led multidisciplinary care with coordinated home-based care and close liaison with community-based healthcare professionals (a hybrid model of care). In the standard care group, no restrictions were placed on discharge planning and post-discharge follow-up was predominantly delivered via a specialist cardiac outpatient clinic of the administering hospital. The primary composite endpoint was the reduction of incident CHF hospitalization or all-cause mortality. 4
Cost data
The analyses were conducted from a perspective of the Australian healthcare system, and only direct healthcare costs during the follow-up period were included. Costs were grouped into three types: hospital-based, intervention and out-of-hospital (community-based) costs. Hospital costs were based on the Australian Refined Diagnosis Related Groups version 6.0 7 adjusted for the duration of hospital stay and the type of admission (i.e. emergency or elective). Intervention costs 8 were based on specialist cardiac nurse activities involving telephone consultation, home-visit travels and the labour costs of delivering personalized care based on standardized protocols. The personnel costs for cardiac specialist nurses were based on two nurses with 0.8 full-time equivalent of the average salary of AUD$70,000 per annum. The same personnel rates were applied to the number of hours worked for both study arms.
The data used to estimate community-based costs were available only for the NIL-CHF arm and comparative data were not available for standard care. As out-of-hospital costs typically account for a small portion of total healthcare cost (e.g. 11–15%), 9 community-based costs were not included in our analysis (i.e. hospital-based costs and intervention costs were included in our analyses). Given the skewed nature of healthcare cost data, generalized linear models with a gamma distribution (log link) were used to compare cost per patient between the study groups. Models were adjusted for age and sex at baseline.
All costs are reported in 2013 Australian dollars (AUD$) (the purchasing power parity for AUD$1 in 2013 was US$0.70 in 2016). 10 The costs and outcomes accrued after one year were discounted at an annual rate of 5% as per the guidelines of the leading health technology assessment body in Australia. 11
Effectiveness data
The total duration of follow-up from index hospital discharge until death or censoring events (loss to follow-up or patients alive censored on 30 December 2013) was used as a proxy of life-years. A utility value assigned to a specific state of health 12 was assessed within the trial using the EuroQol generic health index (EQ-5D-3L) questionnaire. 13 This was converted to utility weights using an Australia-specific algorithm. 14 Multiple imputations with a randomly-generated seed number were used to replace missing values in the EQ-5D-3L measurements at baseline (2.0%), 18 months (21.6%) and 36 months (22.7%). For each missing value, 10 possible values were created using multiple linear regression with the covariates of age, sex, status of living alone, education level and Charlson Comorbidity Index at baseline. The mean value from the 10 data sets was used as the final imputed value. The quality-adjusted life-year (QALY) value per patient was then estimated using the area-under-the-curve method from patient-reported utility scores.
Cost-effectiveness analyses
Cost-effectiveness was assessed by the incremental cost per benefit gained from the NIL-CHF intervention versus standard care. QALY was the primary measure of effect, but life-year was also assessed. The incremental cost and QALY were computed (NIL-CHF minus standard care) and the uncertainty surrounding it was quantified by bootstrap simulations. 15
This was accompanied by a cost-effectiveness acceptability curve (CEAC) to report a probability of NIL-CHF intervention being cost-effective versus standard care for a range of willingness-to-pay thresholds per additional QALY gained. 16 We graphically presented the ellipse on cost-effectiveness plane and CEAC to demonstrate the extent of uncertainty. We used AUD$50,000 per QALY cost-effectiveness threshold, as it is a commonly cited threshold in Australian cost-effectiveness analyses.17–19 This value was then varied from AUD$10,000 to AUD$150,000 to assess its impact on the probability of the NIL-CHF intervention being cost-effective versus standard post-discharge care.
Cardiac function/structure
Further to our previous findings on the NIL-CHF trial suggesting an improved cardiac function over three years, 4 we conducted a post-hoc analysis to explore its impact on life-year, QALY and associated healthcare costs. Global cardiac function/structure was assessed at baseline and reassessed at three years. The change was grouped into four levels in the order of severity: 1) normal cardiac function (best), 2) other cardiac abnormality, 3) diastolic dysfunction, and 4) systolic dysfunction with/without diastolic dysfunction (worst). The three-year change in cardiac function was grouped as improved, stable (no change) or worsened compared with baseline. We compared survival and cost outcomes in those who had non-missing values at both baseline and three years irrespective of the study arm (pooled, n=451).
Analyses were performed using Stata version 14 (Stata Corp), and bootstrapping and the CEAC were conducted in Microsoft Excel.
Results
The median duration of follow-up for the NIL-CHF Trial was 4.2 years (mean 4.1 and maximum 5.5 years). Patients’ mean age was 66 years, 71% were male, 39% were living alone and the mean left ventricular ejection fraction was 60%. 4
Healthcare cost
The healthcare costs collected within trial are presented in Table 1. Compared with standard care, the costs of all-cause readmissions were slightly lower in the NIL-CHF group: AUD$2943 per patient (p=0.219) and AUD$70 (p=0.325) per patient per month alive. A greater reduction in the costs of emergency-related readmissions was observed in the NIL-CHF group: AUD$4194 (p=0.024), and to a lesser extent for cardiovascular-related readmission costs: AUD$1142 (p=0.592). On the other hand, the cost of intervention per patient was higher in the NIL-CHF group although the amounts were very small: AUD$676 ± 236 in NIL-CHF versus AUD$476 ± 98 in standard care (p<0.001). The total healthcare costs were lower in the NIL-CHF group: AUD$2742 per patient (p=0.313) and AUD$25 (p=0.239) per patient per month alive compared with standard care.
Costs measured during a median follow-up of 4.2 years.
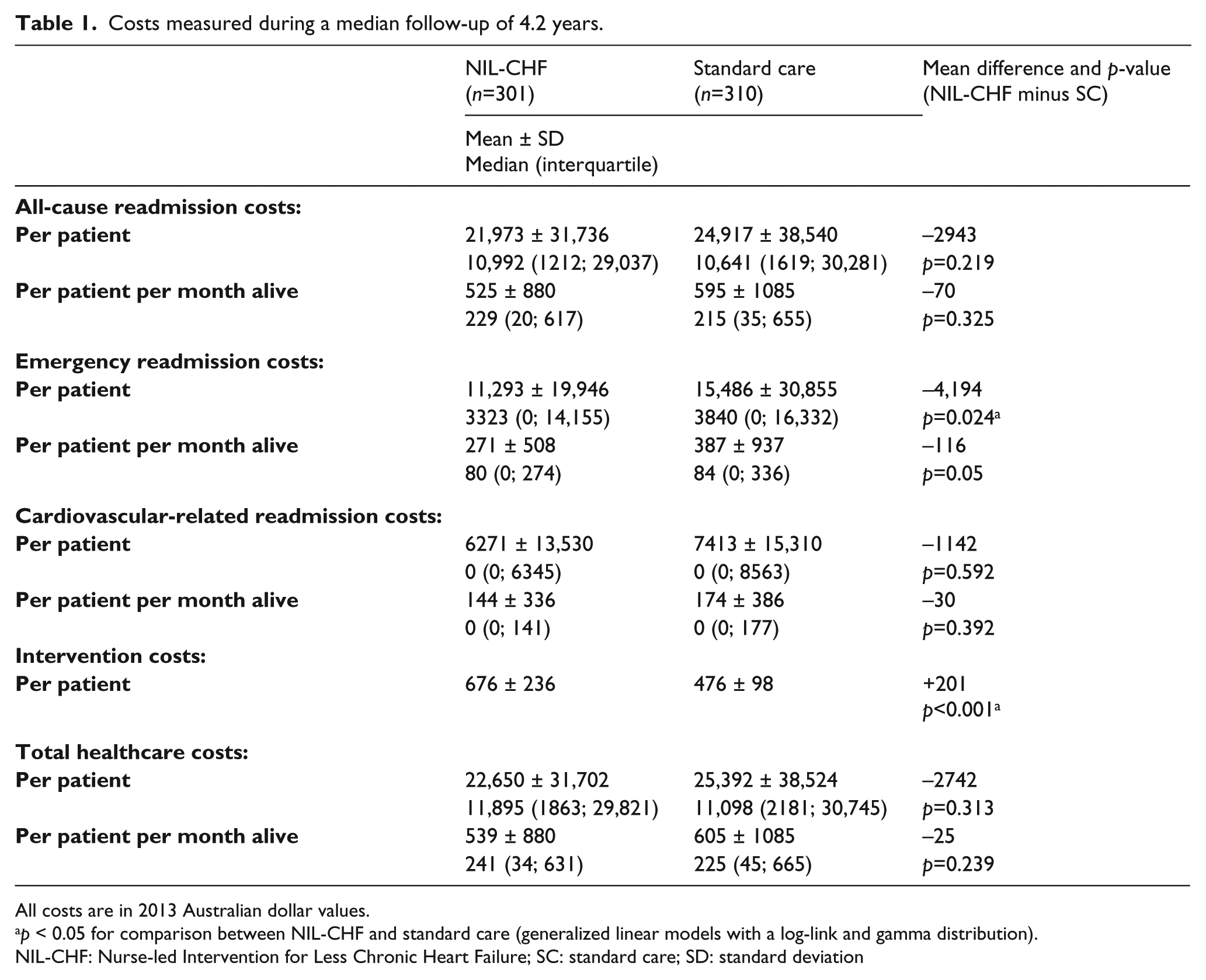
All costs are in 2013 Australian dollar values.
p < 0.05 for comparison between NIL-CHF and standard care (generalized linear models with a log-link and gamma distribution).
NIL-CHF: Nurse-led Intervention for Less Chronic Heart Failure; SC: standard care; SD: standard deviation
Effect
Table 2 shows the key measures of effectiveness, total healthcare costs (all-cause readmissions plus intervention costs) and its subsets (emergency-related readmissions plus intervention costs, cardiovascular-related readmissions plus intervention costs). The mean life-year per patient was 4.10 years (NIL-CHF) versus 4.15 years (standard care). The mean QALY per patient was 3.05 years (NIL-CHF) and 3.12 years (standard care). Utility weights in the NIL-CHF group and standard care were 0.74 versus 0.76 (baseline), 0.76 versus 0.77 (month 18) and 0.76 versus 0.76 (month 36). Utility weights were similar across groups or time points and the between-group difference in QALY was mainly driven by life-year.
Incremental cost-effectiveness results (median follow-up of 4.2 years).
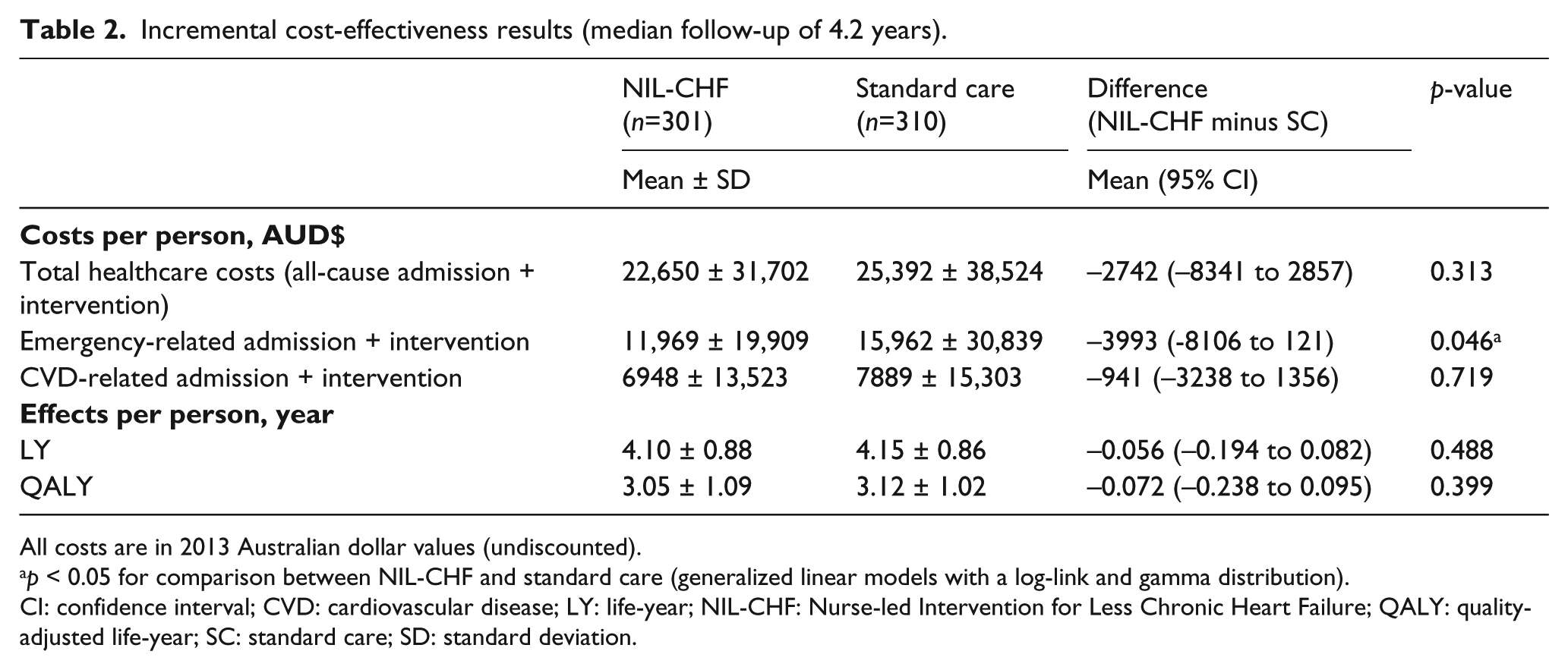
All costs are in 2013 Australian dollar values (undiscounted).
p < 0.05 for comparison between NIL-CHF and standard care (generalized linear models with a log-link and gamma distribution).
CI: confidence interval; CVD: cardiovascular disease; LY: life-year; NIL-CHF: Nurse-led Intervention for Less Chronic Heart Failure; QALY: quality-adjusted life-year; SC: standard care; SD: standard deviation.
Cost-effectiveness
Compared with standard care, the NIL-CHF intervention had a small health loss in terms of life-year and QALY and a modest reduction in total healthcare costs (Table 2). The bootstrapped cost-effect pairs sampled from the trial data are presented on the cost-effectiveness plane (Figure 1). The data-points in the south-west quadrant indicate that NIL-CHF was associated with lower QALYs and lower direct healthcare costs (i.e. an inferior but less-costly intervention). The CEAC showed the probability of NIL-CHF being cost-effective over a range of willingness-to-pay threshold (AUD$10,000–150,000) per QALY gained. There was a 19% probability of NIL-CHF being cost-effective at the threshold of AUD$50,000 and the probability did not exceed 19.4% even if the willingness-to-pay was AUD$150,000 per QALY. Cost-effectiveness was defined as providing health gain at a cost less than $50,000 per QALY; the south-west quadrant was not deemed ‘cost effective’ as this space represents health loss.
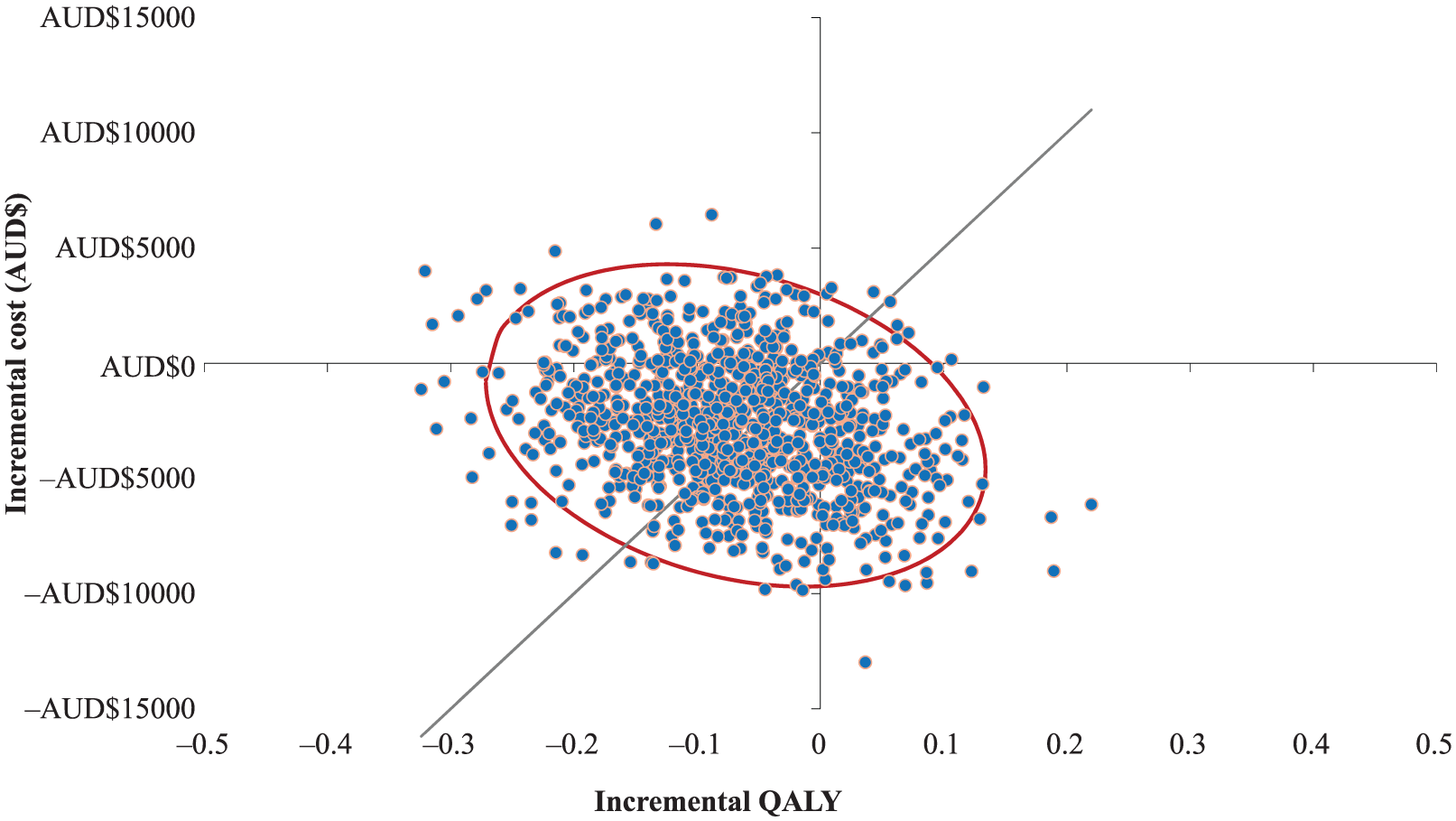
Cost-effectiveness plane: incremental cost and QALYs (NIL-CHF minus standard care).
Cardiac function/structure
Figure 2 shows a similar proportion of patients with worsened cardiac function at three years: 14.60% NIL-CHF versus 14.67% standard care. Conversely, more patients in the NIL-CHF group (29.65% vs. 21.33%) had improved cardiac function at three years. Table 3 shows whether survival and cost outcomes differed by the extent of three-year change in cardiac function. Although QALY and life-year were similar across the level of improvement, there was a modest downward trend in the total costs (hospital readmissions plus intervention) as the severity of cardiac function improved. Those who worsened at three years had the highest total healthcare costs for all groups compared, except the median value for cardiovascular-related costs (AUD$833, Table 3).
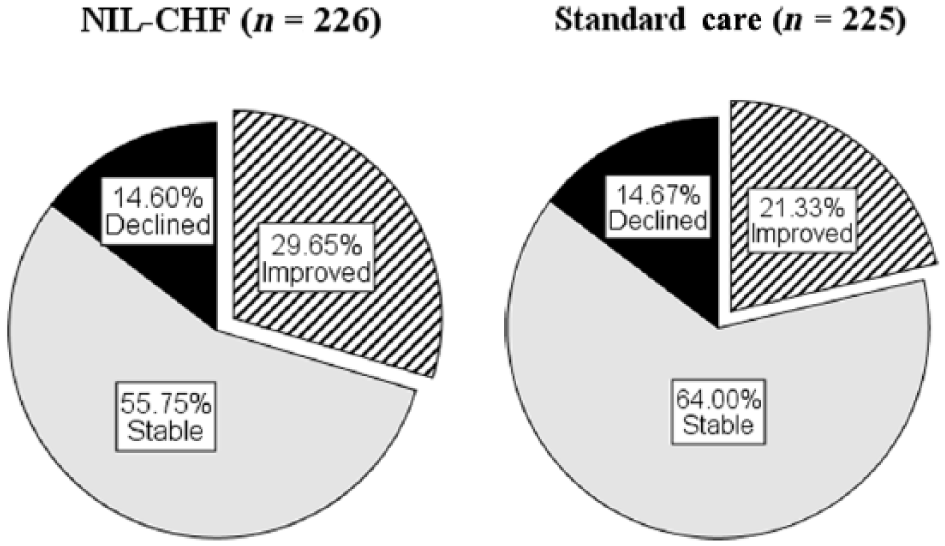
The three-year change in cardiac function/structure: NIL-CHF (n=226) versus standard care (n=225).
Survival and cost outcomes stratified by the three-year change in cardiac function (N=451) a .
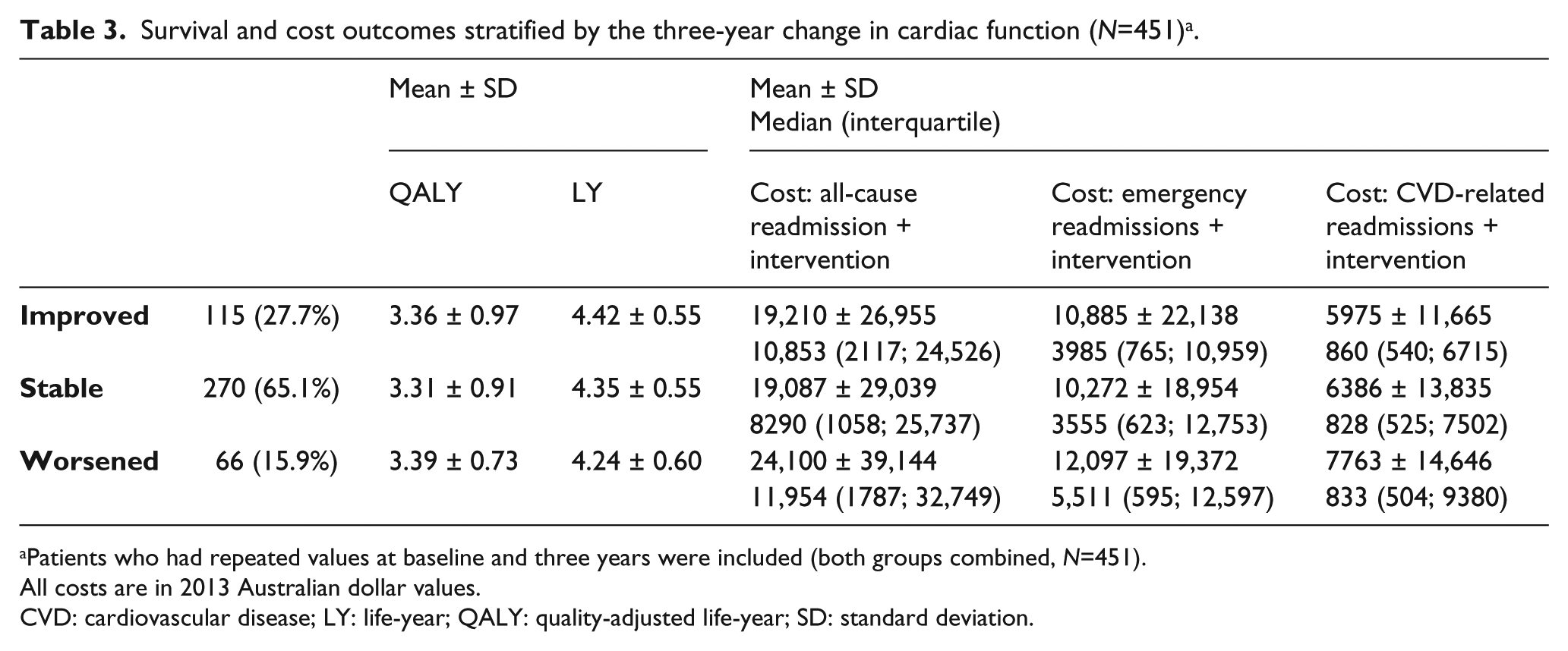
Patients who had repeated values at baseline and three years were included (both groups combined, N=451). All costs are in 2013 Australian dollar values.
CVD: cardiovascular disease; LY: life-year; QALY: quality-adjusted life-year; SD: standard deviation.
Discussion
Although the NIL-CHF intervention did not meet the primary endpoints in reducing all-cause mortality and CHF-related readmissions, we conducted an economic evaluation as per the study protocol 5 and statistical analysis plan 6 where a cost-utility analysis was pre-specified. We found that the NIL-CHF intervention did not improve life-year or QALY and was not a cost-effective strategy. However, it was associated with a modest reduction in hospital-based costs related to emergency/unplanned readmissions and to a lesser extent in cardiovascular readmissions. In addition, given an increased proportion of patients whose cardiac function improved in the NIL-CHF arm (previously published), 4 we also explored whether such improvement influenced survival or cost outcomes and found that there was a modest downward trend in total costs as the severity of cardiac function improved, although QALY and life-year were similar regardless of the severity. Whilst acknowledging the post-hoc nature of such analyses, if the patients in the NIL-CHF arm were less-acutely ill on admission due to a proactive access to hospital care, this may explain the lower costs with shorter hospital stays in the NIL-CHF group. 4
Although the NIL-CHF group had shorter hospital stays for emergency and cardiovascular-related readmissions, 4 the shortening effect on hospital-based cost was smaller in cardiovascular-related readmissions than in emergency readmissions. This difference may be explained as follows: first, hospital stays in the NIL-CHF group were shorter on average by 3.3 days for emergency readmissions and by 1.4 days for cardiovascular-related readmissions, respectively. Such differences would have affected the proportion of ‘long-stay’ admissions (i.e. above the upper limit of a Diagnosis Related Groups-specific ‘inlier’ range or a fixed cost for the average duration of hospital stay within boundaries expected for the type of admission based on diagnosis, age and complications or comorbidities) and not those within an ‘inlier’ range unless patients were discharged <5 days (‘short-stay’) before an ‘inlier’ cost starts to apply (i.e. ‘short-stay’ cost is substantially less than the ‘inlier’ cost). Among emergency long-stay hospitalizations (n=110), the last-day variable mean cost per admission was AUD$1056, accounting for 10.3% of its total hospitalization cost (per admission). Since the NIL-CHF group had shorter hospital stay (mean –3.3 days) than standard care, the expected reduction of the last three-day-variable mean cost was estimated as AUD$3420 (33.3% of its total hospitalization cost). On the other hand, among cardiovascular long-stay hospitalizations (n=51), the last-day variable mean cost per admission was AUD$1091, accounting for 8.8% of its total hospitalization cost (per admission). As the NIL-CHF group had approximately 1.4 days shorter hospital stay, the expected reduction of the last 1.4-day-variable mean cost was estimated as AUD$1550 (12.5% of its total hospitalization cost). Second, the shortening effect (per day) on cost was larger in an emergency admission than in a cardiovascular-related admission. That is, the impact of the (variable) costs attributable to the last day of a hospital stay on total hospital costs (versus the impact of ‘inlier’ fixed costs to total costs) was one-fifth (8.8% vs. 45.4%) for a cardiovascular-related readmission versus one-fourth (10.3% vs. 41.1%) for an emergency readmission.
The limitations of this study are as follows. First, comparative information on the use of community-care was not available, thus, out-of-hospital costs were not included in our analyses. However, as the majority of healthcare costs is predominantly represented by hospital-based costs (85–89%), 9 the lack of out-of-hospital costs would have been minimal. Second, this economic evaluation focused on clinical outcomes that were previously reported: reduced hospital stay in emergency and cardiovascular-related readmissions and the potential to improve cardiac function. Analyses for these endpoints were not pre-specified and its post-hoc nature may have led to spurious findings. We thus restricted our analysis to descriptive statistics and carefully reviewed how reducing the last day of a hospital stay might have influenced the costs of emergency-related and cardiovascular-related readmissions.
Conclusion
Compared with the standard care, NIL-CHF intervention was not a cost-effective strategy as life-years and QALYs were slightly lower in the NIL-CHF group. However, it was associated with modest reductions in emergency/unplanned readmission costs.
Footnotes
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This work was supported by the National Health and Medical Research Council of Australia (program grant number 519823) and the Victorian Government’s Operational Infrastructure Support Program. SS is supported by the National Health and Medical Research Council of Australia. MJC is supported by a Future Leader Fellowship (Award Reference 100802) from the National Heart Foundation of Australia.
Although timely efforts to prevent cardiac dysfunction in patients at risk of developing de novo chronic heart failure might be more cost-effective compared with managing the full chronic heart failure syndrome over the long term, the Nurse-led Intervention for Less Chronic Heart Failure was not shown to be a cost-effective strategy during 3–5 years of follow-up. The Nurse-led Intervention for Less Chronic Heart Failure showed the potential to reduce hospital stay, leading to modest reductions in hospital readmission-related costs. Further research is needed to confirm this.