
Abstract
Background:
Atrial fibrillation represents a substantial clinical and public health issue. The definitive impact of body mass index on prognosis of patients with chronic (persistent or permanent) atrial fibrillation remains undetermined.
Aim:
The purpose of this study was to investigate the association of body mass index with health outcomes (mortality and re-hospitalisation) of patients with chronic atrial fibrillation.
Methods:
Using data from the Standard versus Atrial Fibrillation spEcific managemenT strategY (SAFETY) trial (a randomised controlled trial of home-based, atrial fibrillation-specific disease management), we performed post-hoc analyses of mortality and re-hospitalisation outcomes during minimum 24-month follow-up according to baseline body mass index profile.
Results:
Of 297 participants (mean age 71±11 years, 47% female, mean body mass index 29.6±6.7 kg/m2), 35.0% of participants were overweight (body mass index 25.0–29.9 kg/m2) and 43.1% were obese (body mass index≥30 kg/m2). During follow-up, n=42 died including 16/65 (24.6%) classified as normal body mass index, 16/104 (15.4%) classified as overweight and 10/128 (7.8%) classified as obese. Increasing body mass index was not associated with increased mortality but was associated with re-hospitalisation due to cardiovascular disease with greater length-of-stay (odds ratio 1.05; 95% confidence interval 1.00–1.09, p=0.032). Obese individuals experienced increased unplanned admissions compared to overweight individuals (incidence rate ratio 0.71; 95% confidence interval 0.53–0.96, p=0.028), and increased cardiovascular-related (incidence rate ratio 0.58; 95% confidence interval 0.39–0.86, p=0.007) and all-cause admissions (incidence rate ratio 0.63; 95% confidence interval 0.45–0.89, p=0.008) compared to those classified as normal body mass index.
Conclusion:
Overweight and obesity were not associated with survival in patients with chronic atrial fibrillation but were associated with more frequent hospital care and prolonged stay.
Introduction
Atrial fibrillation (AF) is the most common cardiac rhythm disturbance and represents a substantial clinical and public health issue. Prevalence of AF is expected to reach epidemic proportions globally in the coming decades as the world’s population ages. 1 AF, particularly if inappropriately treated, is associated with poor patient outcomes such as heart failure, stroke and death. 2 Efforts to address the complex causes of AF are required to attenuate future AF-related morbidity, mortality and overall economic costs. In addition to increasing age, hypertension, diabetes and prevalent cardiac disease, AF is commonly associated with the emergent epidemics of overweight and obesity. 3 Weight reduction strategies are suggested as important management tools in order to improve the prognosis for AF patients. 4 Studies thus far have revealed inconsistent results on the relationship between body weight and morbidity and mortality outcomes in AF patients. Both reduced and excess body weight have been associated with adverse outcomes in AF,5,6 although some have shown better outcomes in obese patients 7 or no impact of body weight at all. 8 Furthermore, there is minimal delineation between the different but critically important sub-types of AF (i.e. paroxysmal, persistent or permanent).5–8 Recent studies performed in patients with paroxysmal and persistent AF found that weight loss decreased disease burden in obese AF patients and the effect was related to amount of weight lost.9,10 It must be noted that although combining paroxysmal and persistent AF is common, up to 50% of AF patients have permanent AF. 4
To our knowledge, the relationship between body weight and survival among patients with persistent or permanent AF has not been previously addressed; although the possibility of an interaction with age and body mass index (BMI) has previously been highlighted. 5 Using data from the Standard versus Atrial Fibrillation spEcific managemenT strategY (SAFETY) trial, 11 we aimed (in a post-hoc analysis) to determine if, independent of confounding factors including age and sex, BMI was associated with all-cause mortality and hospital admissions in patients with persistent or permanent AF.
Methods
Study setting
Details of the SAFETY Trial design (a multicentre, randomised trial of AF-specific disease management) and primary outcomes have been reported previously. 11 Briefly, 335 inpatients (52% male) from three tertiary referral hospitals in Australia with a diagnosis of persistent or permanent AF (defined here as chronic AF) were randomly assigned into the study and subject to comprehensive baseline profiling between June 2010–March 2012 with follow-up completed by March 2014. Participants were randomised to either standard post-discharge management or an AF-specific nurse-led, home-based management strategy aimed to reduce morbidity and mortality. Those in the standard management group underwent usual post-discharge care, had no restrictions on their health care imposed and attended annual study follow-up visits. The intervention involved comprehensive health assessment, risk delineation, individualised care based on risk profile, Holter monitoring to understand if therapeutic targets (rate/rhythm control) were being met and annual follow-up visits. All participants were followed-up for a minimum of 24 months with comprehensive details of all deaths and re-hospitalisations collected from electronic health records. The co-primary outcomes were all-cause death or unplanned re-hospitalisation due to any reason. Endpoint events (including the type and nature of admissions) were adjudicated by a blinded endpoint committee who were unaware of group allocations. Hospitalisations were coded as being all-cause (due to any cause), cardiovascular disease (CVD)-related (due to CVD) and unplanned (an emergency admission) or elective. 11
The SAFETY Trial was prospectively registered with the Australian New Zealand Clinical Trials Registry (ANZCTRN: 12610000221055) and was CONSORT compliant with outcomes reported appropriately for a pragmatic trial comparing the efficacy of two non-pharmacological health interventions (https://www.anzctr.org.au/Trial/Registration/TrialReview.aspx?id=335204&isReview=true). Written informed consent was obtained from each study participant prior to any study procedure being conducted. The investigation conforms with the principles outlined in the Declaration of Helsinki and was approved by the relevant human research committees of all participating institutions.
Participants
As part of the overarching SAFETY trial and utilising a systematic screening program to identify eligible participants at each participating institution, inpatients were approached for recruitment if they were aged 45 years or older; had a documented diagnosis of chronic AF; were going to be living independently in the community or their own home post-discharge; and were able and willing to provide written informed consent to participate. We included individuals aged ≥45 years as they were most likely to demonstrate chronic AF. Those who had a primary diagnosis of valvular heart disease; had a transient form of AF; were scheduled for catheter ablation and/or had concurrent heart failure (confirmed on echocardiography (included screening of evidence of diastolic heart failure) and defined as displaying symptoms indicative of New York Heart Association class III–IV with a documented left ventricular ejection fraction of less than 45%) were excluded from participation.
Baseline profiling
Comprehensive baseline profiling (involving the collection of detailed information regarding current and previous health, disease and risk factors) was conducted in all participants during index hospitalisation. Data were collected on sociodemographic status; past medical history (including AF-specific details); index hospital management and planned post-discharge management; thromboembolic risk as calculated by the CHA2DS2-VASc score 12 (C=congestive heart failure/LV dysfunction (one point), H=hypertension (one point), A2=age ≥75 years (two points), D=diabetes mellitus (one point), S2=stroke/systemic embolism/transient ischemic attack (two points), V=vascular disease (one point), A=age 65–74 years (one point), Sc=sex category (female sex; one point)); and comorbid conditions. Clinical data collected included admission and discharge pathology results; prescribed therapeutics (i.e. all medications prescribed at the time of discharge); admission electrocardiogram (ECG); depressive symptoms (measured using the Arroll questionnaire 13 and, if positive, the Centre for Epidemiological Studies Depression Scale; 14 physical activity (measured using the International Physical Activity Questionnaire; 15 cognitive functional status (i.e. the presence or absence of mild cognitive impairment (MCI) which was determined by a score <26 on the Montreal Cognitive Assessment (MoCA) tool) 16 and anthropometric measurements. Last recorded weight measurement (taken during index admission) and height were collected from each patient’s medical record and BMI was subsequently calculated. If measurements were not available, data were collected via self-report. These data were available for n=297 of the total cohort of 335 patients. The well-known cut-offs for BMI were used to classify individuals into BMI categories; a BMI of 18.5–24.9 kg/m2 was considered ‘normal’ whilst participants with a BMI of 25.0–29.9 kg/m2 and BMI ≥30 kg/m2 were classified as overweight and obese, respectively. 17
Statistical analyses
Descriptive data are presented as mean (with standard deviation (SD)) or median (with inter-quartile range (IQR)) for continuous variables or as a proportion (%) for categorical variables. Between-group comparisons were conducted with the χ2 test, one-way analysis of variance (ANOVA) with post-hoc Bonferroni correction and the Kruskal-Wallis test where appropriate. We performed Kaplan-Meier survival analysis to assess event-free survival from all-cause mortality in participants classified as being of normal BMI versus those considered overweight and obese. Group comparisons were performed with a log-rank test and univariate Cox regression analyses was conducted to compare survival between normal BMI and overweight individuals and normal BMI and obese individuals. Mean follow-up time (with 95% confidence intervals (CIs)) was calculated for each respective group. A Cox proportional hazards model was constructed using baseline profile data (and BMI as a continuous variable) to derive adjusted hazard ratios (HRs) for independent correlates of all-cause mortality using a backwards, step-wise approach (due to the total number of covariates and modest sample size). Multiple logistic regression models (with BMI as a continuous variable) were also undertaken using a backwards, step-wise approach (again due to the total number of covariates and modest sample size) to identify independent predictors of inclusion in the lower quartile of days alive and out-of-hospital (≤765.5 days), upper quartile of all-cause hospital stay (≥26.5 days) and upper quartile of CVD-related stay (≥7 days) and adjusted odds ratios (ORs) were derived. All models were adjusted for the socio-demographic (age, sex, living alone, education level), lifestyle (smoking, high risk alcohol consumption, exercise level), medical history/status (type of AF, CHA2DS2-VASc score, asymptomatic or not, rate or rhythm control, heart rate, blood pressure, total cholesterol, BMI, hypertension, coronary artery disease, diabetes, prior cerebrovascular event, chronic obstructive pulmonary disease, vascular disease, depressive symptoms, renal impairment, MCI, Charlson Comorbidity Index) and treatment factors (beta blocker, digoxin, anti-arrhythmic, diuretic, warfarin, aspirin randomisation group) listed in Table 1. We compared the pattern of recurrent hospital admissions between dichotomised BMI categories (normal versus obese and overweight versus obese). The number of admissions and length of hospital stay (days) were compared between the groups with negative binomial regression and log gamma regression, respectively, following adjustment for length of follow-up (calculated as admissions or days of hospital stay per person-days of follow-up). All data were analysed using SPSS version 22.0 (SPSS, Chicago, Illinois, USA). A probability value of p<0.05 (two-sided) was considered statistically significant.
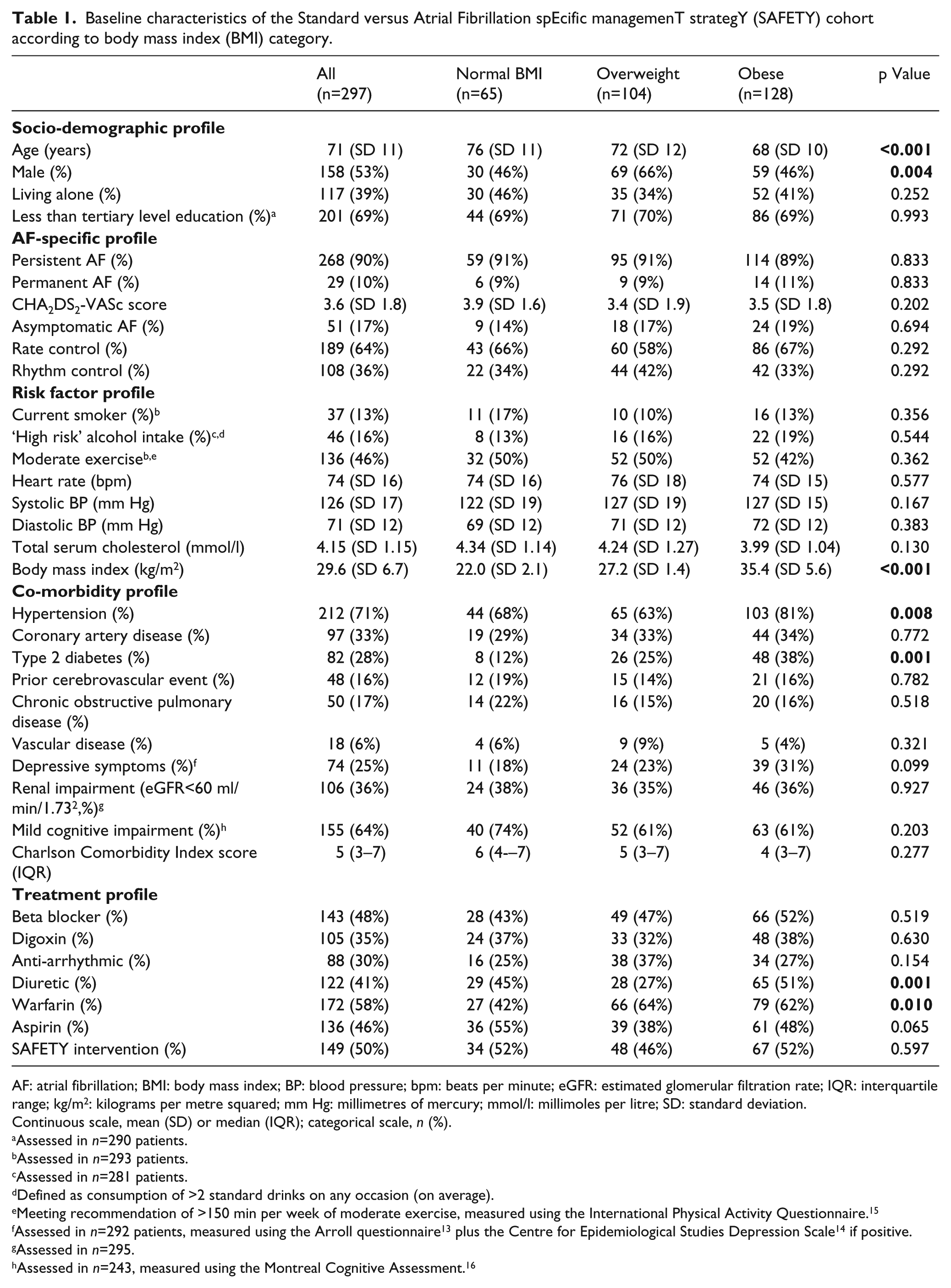
Baseline characteristics of the Standard versus Atrial Fibrillation spEcific managemenT strategY (SAFETY) cohort according to body mass index (BMI) category.
AF: atrial fibrillation; BMI: body mass index; BP: blood pressure; bpm: beats per minute; eGFR: estimated glomerular filtration rate; IQR: interquartile range; kg/m2: kilograms per metre squared; mm Hg: millimetres of mercury; mmol/l: millimoles per litre; SD: standard deviation.
Continuous scale, mean (SD) or median (IQR); categorical scale, n (%).
Assessed in n=290 patients.
Assessed in n=293 patients.
Assessed in n=281 patients.
Defined as consumption of >2 standard drinks on any occasion (on average).
Meeting recommendation of >150 min per week of moderate exercise, measured using the International Physical Activity Questionnaire. 15
Assessed in n=292 patients, measured using the Arroll questionnaire 13 plus the Centre for Epidemiological Studies Depression Scale 14 if positive.
Assessed in n=295.
Assessed in n=243, measured using the Montreal Cognitive Assessment. 16
Results
Baseline profile
Table 1 provides a summary of the demographic and clinical profile of the cohort according to BMI category and Figure 1 shows the study flow chart. Overall, 104/297 (35.0%) participants with BMI profiling were classified as overweight and 128/297 (43.1%) participants were classified as obese. There was a decreasing gradient in age across the BMI categories with obese individuals being, on average, eight years younger than those of normal BMI (p<0.001). There was a higher proportion of males in the overweight category compared to the other BMI categories (66% versus 46%, respectively). Significant differences in the proportion of individuals with co-morbid hypertension (p=0.008) and type 2 diabetes (p=0.001) were observed with increasing BMI associated with higher proportions of these conditions. Prescription of diuretic and warfarin therapy differed between BMI groups with a higher proportion of obese individuals being prescribed diuretic therapy (51% versus 45% and 27%; p=0.001) and a significant proportion of both overweight and obese individuals were prescribed warfarin for stroke prevention (62% and 64%, respectively, versus 42%; p=0.010) despite being younger and having a lower mean CHA2DS2-VASc score than those of normal BMI.
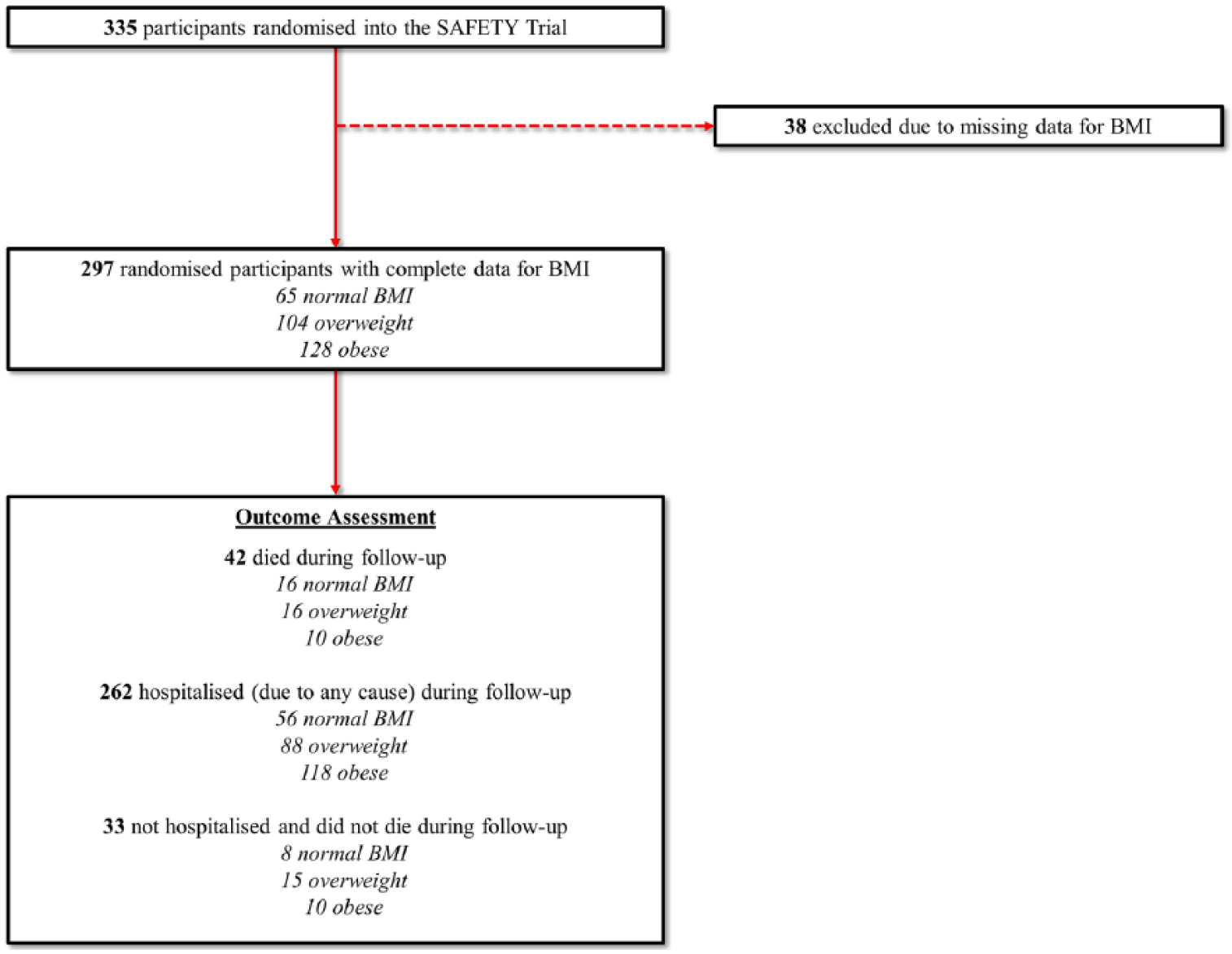
Study flowchart. BMI: body mass index.
All-cause mortality
Figure 2 shows the unadjusted survival curves of participants stratified by BMI category. Over a median follow-up of 919 (IQR 780–1062) days, 42 individuals died including 16/65 (24.6%) classified as normal BMI, 16/104 (15.4%) classified as overweight and 10/128 participants (7.8%) classified as obese. Median follow-up time in these groups was 898 days (IQR 743–1028 days), 899 (IQR 777–1040 days) and 946 days (788–1138 days), respectively. On an unadjusted basis, those classified as obese had a markedly (more than 70%) reduced risk of dying (all-cause) during follow-up compared to those of normal BMI. Survival of those classified as overweight was not significantly different to those of normal BMI on an unadjusted basis.
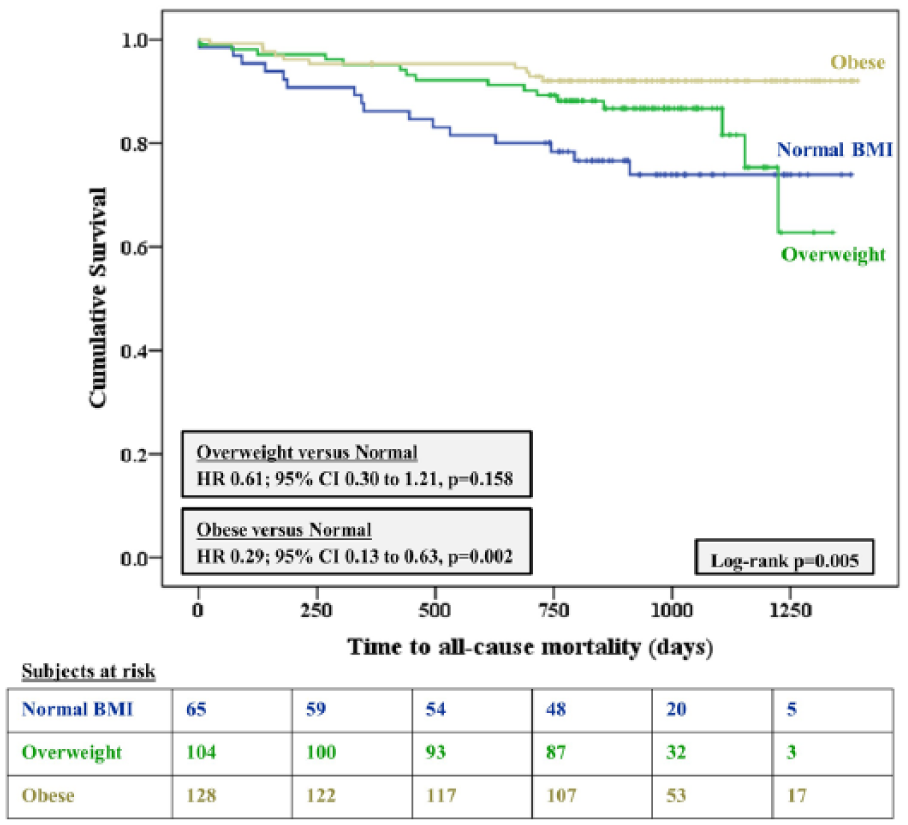
Unadjusted event-free survival of normal body mass index (BMI) versus overweight versus obese individuals at baseline in the SAFETY cohort. CI: confidence interval; HR: hazard ratio.
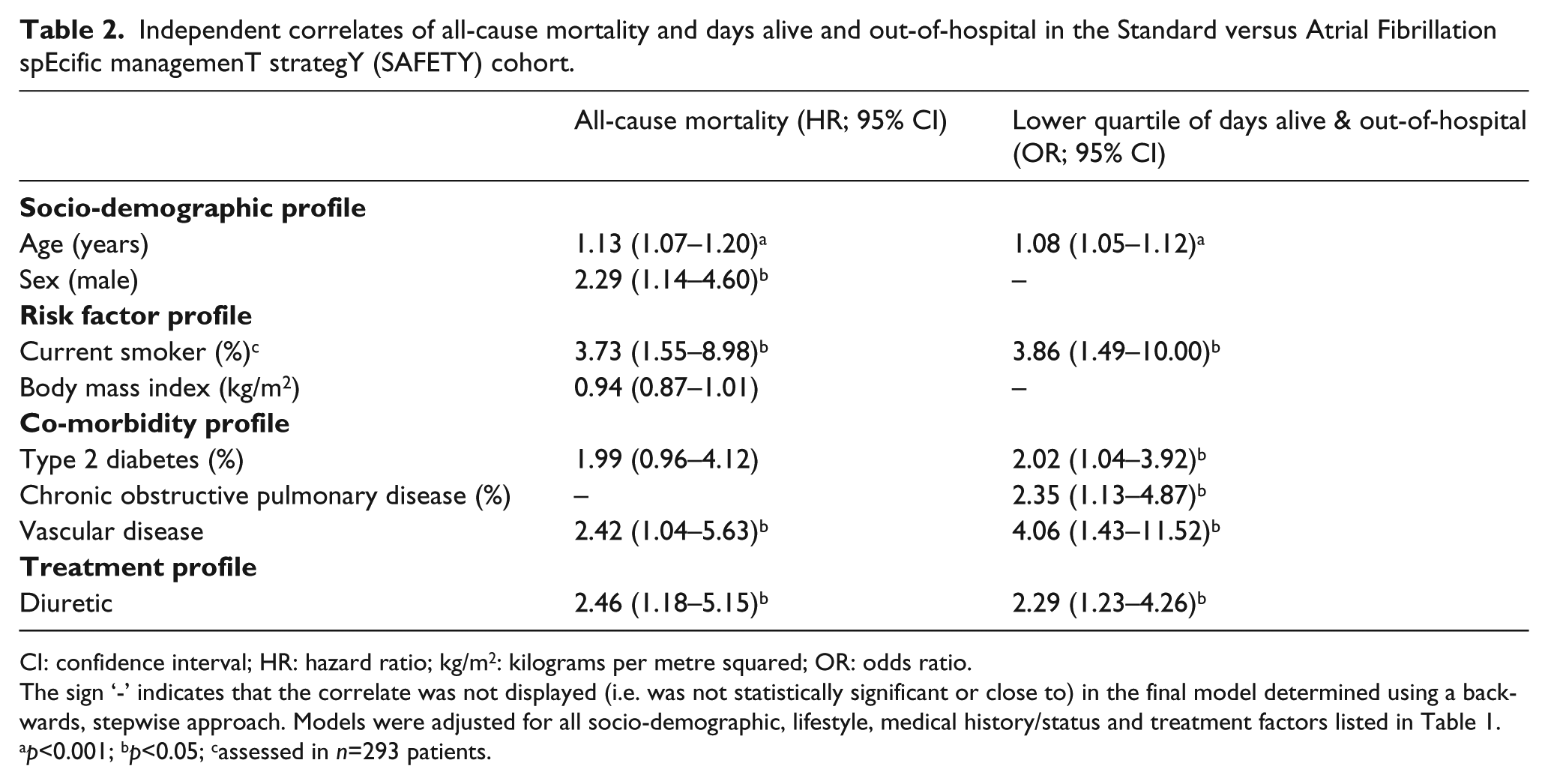
Table 2 shows the results of adjusted analysis of all-cause mortality. Following adjustment, a trend for increasing BMI to positively influence survival was revealed with the 95% CI being close to significance. All-cause mortality was significantly associated with increasing age, male gender, smoking, co-morbid vascular disease and diuretic treatment. For every year increase in age, death was more likely (HR 1.13; 95% CI 1.07–1.20, p<0.001). Males were greater than two-fold more likely to die from any cause than females (HR 2.29; 95% CI 1.14–4.60, p=0.020). Those who smoked, had co-morbid vascular disease and were prescribed diuretic treatment were 3.7, 2.4 and 2.5 times more likely, respectively, to die from any cause.
Independent correlates of all-cause mortality and days alive and out-of-hospital in the Standard versus Atrial Fibrillation spEcific managemenT strategY (SAFETY) cohort.
CI: confidence interval; HR: hazard ratio; kg/m2: kilograms per metre squared; OR: odds ratio.
The sign ‘-’ indicates that the correlate was not displayed (i.e. was not statistically significant or close to) in the final model determined using a backwards, stepwise approach. Models were adjusted for all socio-demographic, lifestyle, medical history/status and treatment factors listed in Table 1.
p<0.001; bp<0.05; cassessed in n=293 patients.
Event-free survival (days alive and out-of-hospital)
When assessing the shortest duration of event-free survival (on an adjusted basis), BMI was not correlated (Table 2). Instead, increasing age, current smoking, co-morbid type 2 diabetes, chronic obstructive pulmonary disease, vascular disease and treatment with diuretic therapy were most predictive of patients having fewer days alive and out-of-hospital.
Re-hospitalisations and hospital stay
Table 3 shows the pattern of recurrent hospitalisations between the BMI groups. The median number of cardiovascular-related admissions per patient and all-cause admissions per patient were lower in those with a normal BMI compared to those who were obese. Individuals of normal BMI had 0.42 times less cardiovascular-specific admissions and 0.37 times less all-cause admissions compared to individuals who were obese. The only significant difference between the overweight and obese BMI groups was in the number of unplanned re-hospitalisations per patient; overweight individuals had 0.29 times less unplanned admissions compared to individuals who were obese. No differences were identified between the groups relating to the number of days spent in hospital per patient or per hospital admission.
Pattern of recurrent admissions in normal, overweight and obese participants in the Standard versus Atrial Fibrillation spEcific managemenT strategY (SAFETY) cohort.
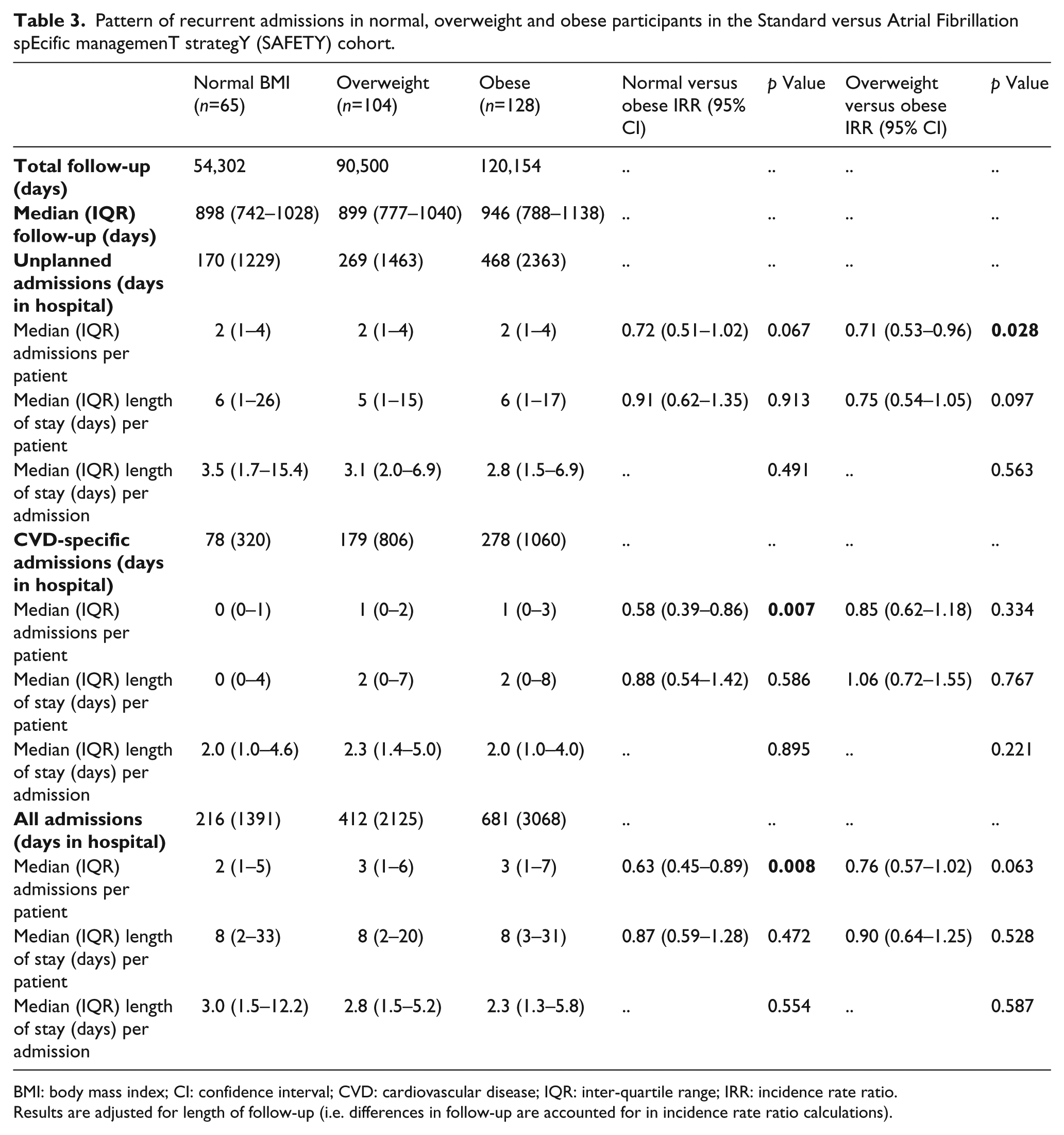
BMI: body mass index; CI: confidence interval; CVD: cardiovascular disease; IQR: inter-quartile range; IRR: incidence rate ratio.
Results are adjusted for length of follow-up (i.e. differences in follow-up are accounted for in incidence rate ratio calculations).
Table 4 shows the relationship between patterns of hospital stay (all-cause and cardiovascular) according to BMI profile. BMI was not an independent correlate of all-cause hospital stay and typical risk factors that influence health significantly induced longer hospital stay (increasing age, co-morbid coronary artery disease, type 2 diabetes and treatment with diuretic and warfarin therapy) during follow-up. Higher BMI was, however, associated with length of cardiovascular-related hospital stay; for every one unit increase in BMI (kg/m2), the likelihood of experiencing a hospitalisation for CVD involving a length-of-stay in the upper quartile was increased by 5%.
Independent correlates of all-cause and cardiovascular-related hospital stay in the Standard versus Atrial Fibrillation spEcific managemenT strategY (SAFETY) cohort.
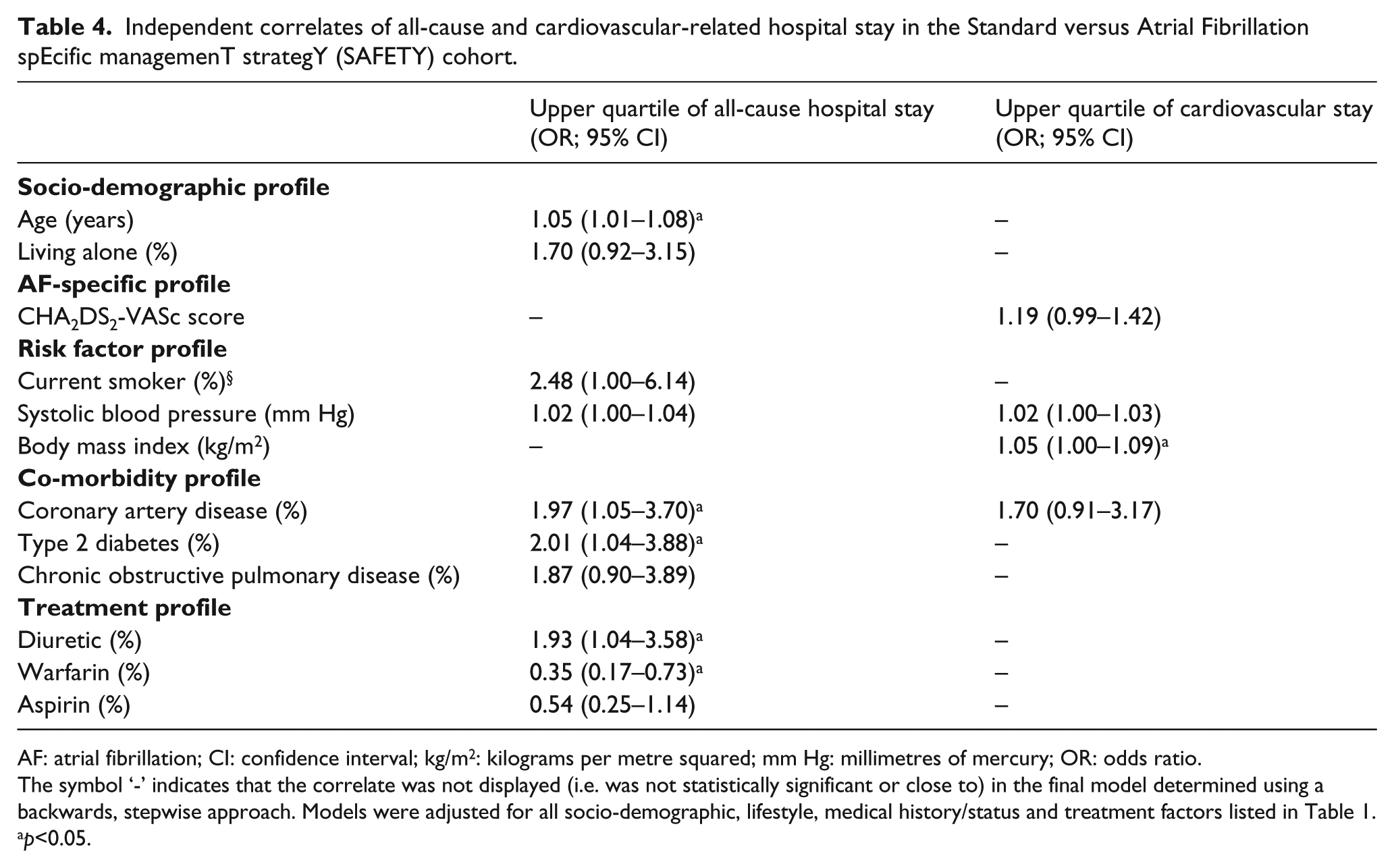
AF: atrial fibrillation; CI: confidence interval; kg/m2: kilograms per metre squared; mm Hg: millimetres of mercury; OR: odds ratio.
The symbol ‘-’ indicates that the correlate was not displayed (i.e. was not statistically significant or close to) in the final model determined using a backwards, stepwise approach. Models were adjusted for all socio-demographic, lifestyle, medical history/status and treatment factors listed in Table 1.
p<0.05.
Discussion
In a typical cohort of high-risk patients with a chronic and a previous hospitalisation with a principal or secondary diagnosis of AF, we found no significant influence of BMI on mortality but increasing BMI was associated with re-hospitalisation. This cohort consisted of older AF patients who had significant co-morbidity profiles (as indicated by high Charlson Comorbidity Index scores) that likely contributed to the potentially high number of deaths observed. We identified a large proportion of overweight and obesity which reflects similar findings within comparable AF patient cohorts from large randomised controlled trials.8,18 On an unadjusted basis, those who were obese demonstrated an association with improved survival over those with BMI profiles considered to be normal. However, upon adjustment for age, sociodemographic factors, comorbidities and prescribed pharmacotherapies, only a trend in the same direction as survival analysis (towards increasing BMI positively influencing survival) was demonstrated. Those with increasing BMI were also more likely to be re-hospitalised due to CVD and for every unit increase in BMI, the likelihood of experiencing a cardiovascular-specific re-hospitalisation with a length-of-stay in the upper quartile significantly increased.
It has been clearly established that being overweight or obese is a risk factor for incident AF and increases cardiovascular risk in patients with established AF.4,6,19 Recent studies have also demonstrated the value of weight loss on reduction of AF burden in patients with symptomatic paroxysmal and persistent AF.9,10 However, data about the association of BMI with outcomes of patients with chronic AF who are typically older with multiple comorbidities and strict treatment regimens are not definitive and potentially suggest that this patient population is different. In 2016, Senoo and Lip published results of a post-hoc analysis of data from older (≥75 years) anticoagulated AF patients from the AMADEUS (Evaluating the Use of SR34006 Compared to Warfarin or Acenocoumarol in Patients with Atrial Fibrillation) Trial in which a gradient in cardiovascular mortality and stroke/systemic embolism according to BMI category was identified; obesity being associated with the lowest risk and normal BMI associated with the worst outcomes. 20 Apixaban for Reduction in Stroke and Other Thromboembolic Events in Atrial Fibrillation (ARISTOTLE) investigators also identified that higher BMI was associated with a more favourable prognosis in anticoagulated AF patients. 18 Similarly, overweight and obesity were associated with a lower risk of all-cause and CVD-related mortality on post-hoc analyses compared with AF patients of normal weight in the Atrial Fibrillation Follow-Up Investigation of Rhythm Management (AFFIRM) Trial. 8 The current study goes somewhat towards confirming the findings of these clinical trials however, unlike these trials, the current study was pragmatic in nature and included a representative patient cohort who suffered only from chronic AF and were typically older, clinically complex and on multiple concurrent pharmacotherapies. It is these characteristics which may also provide an explanation for the increase in hospitalisations (unplanned, CVD-related and all-cause) and length-of-stay seen with increasing BMI and specifically for obese patients that has not been demonstrated previously.
Although the current study did not confirm the existence of an apparent survival advantage for overweight or obese AF patients, findings suggest a trend towards this and confirm that these individuals experience more morbidity (as indicated by increased hospitalisations and length-of-stay related to CVD). As hospitalisations in general are associated with increased mortality despite patient treatment being optimised during this time, it is expected that overweight/obese patients would in fact have worse survival than those of normal BMI but this was not the case in the current study. In patients with chronic AF, overweight/obesity may confer a better metabolic reserve compared to patients who are lean with either poor nutrition and/or cachexia that could lead to intolerance of metabolic stress. 21 Overweight/obese patients are also more likely to experience comorbid conditions that require treatment (e.g. hypertension, hypercholesterolemia), medications for which may prolong survival due to prevention of disease progression and reduction of likelihood of poor outcomes. Overweight/obese patients may also be biologically advantaged; these individuals show lower levels of natriuretic peptides (which are predictive of mortality and stroke in AF patients), and have increased production of tumour necrosis factor α-receptors in adipose tissue, contributing to a decrease in inflammation and structural cardiac changes.22,23
Clinical implications
Findings of the current study have confirmed the significant impact that overweight and obesity can have on the health outcomes of patients with AF. Experiencing more and longer hospitalisations can significantly impact the wellbeing and quality of life of patients as well as their caregivers. The increased hospitalisations that overweight and obese patients demonstrated in the current study may be overcome with more individualised assessment and stratified care conducted by cardiovascular nurses and physicians according to patient risk factor profile and comorbid status. The focus for patients should be on improving lifestyle factors, for example, diet, physical activity and functional capacity 4,24 and the role of cardiovascular nurses and caregivers in promoting a healthy and active lifestyle for patients with AF is critical. 25 Patients and their caregivers should, of course, be central in all decision-making in this regard. 26
Limitations
There exist some limitations of this study that require comment. Firstly, if last recorded measurements were not available at the time of baseline assessment, data on height and weight were collected via self-report, potentially resulting in the under- or over-estimation of results. Furthermore, due to baseline weight being measured at each participating hospital, there is the potential for variability between study sites with the use of different scales and different protocols. We also only used baseline measurements and were not able to assess the change of BMI over time or the influence of changes in adiposity on outcomes. Additionally, BMI was measured after the diagnosis of AF. Therefore, reverse causality may exist whereby AF affects body weight. BMI also potentially does not accurately distinguish between body fat and lean mass and also is limited in its accuracy in certain body compositions. We were also unable to analyse the influence of underweight on outcomes due to only a small number (n=5) of individuals in the SAFETY cohort being classified as such. We also did not assess cardiorespiratory fitness which influences prognosis; focus should perhaps be placed on increasing physical activity and relative cardiorespiratory fitness in these patients. Age, co-morbid hypertension and diabetes, diuretic and warfarin prescription was significantly different at baseline between the BMI groups with normal BMI individuals being older on average and less likely to be prescribed warfarin therapy which are known drivers of mortality. The finding that diuretic prescription is associated with increased mortality is potentially the result of indication bias rather than a true association, particularly given the significant difference in hypertension and diuretic prescription identified between the BMI groups. The number of events was also relatively small in the current cohort potentially affecting the accuracy and/or generalisability of results. Generalisability may also be uncertain due to this study being conducted within the Australian context with the inclusion of participants principally of European descent. Furthermore, this was a selected population of AF patients who did not have heart failure, a common comorbidity. Finally, some of the identified independent correlates (e.g. smoking and vascular disease) had low prevalence within the study cohort and wide confidence intervals and this should be taken into consideration when interpreting the results.
Conclusions
We found that increasing BMI was potentially associated with improved survival in patients with chronic AF, although being overweight or obese was associated with re-hospitalisation and longer length-of-stay, particularly for CVD. Future studies in larger population cohorts (including randomised controlled trials involving weight loss manipulation) with longer follow-up, multiple measures of adiposity and cardiorespiratory fitness and individualised care are required to truly assess the impact of BMI on the morbidity and mortality of patients with chronic AF.
Footnotes
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
The SAFETY Trial was funded by a National Health and Medical Research Council of Australia Program Grant (519823). JB (APP1112829) is supported by the National Health and Medical Research Council of Australia and is also supported by a Postdoctoral Fellowship (Award Reference 100950) from the National Heart Foundation of Australia. MC is supported by a Future Leader Fellowship (Award Reference 100802) from the National Heart Foundation of Australia. Supported in part by the Victorian Government’s Operational Infrastructure Support Program.
Overweight and obesity may impact the health outcomes (particularly hospitalisation) of patients with chronic atrial fibrillation. Personalised management and stratified care of these patients should incorporate the assessment of body mass index and shared decision-making. Patients with chronic atrial fibrillation who are overweight or obese should be encouraged by cardiovascular nurses to live a healthy lifestyle, engage in physical activity and lose weight if possible to improve their health outcomes.