
Abstract
Aim:
The use of the internet and newer activity monitors such as the Fitbit Charge HR to improve exercise adherence is limited. The primary aim of the Move on Virtual Engagement (MOVE-HF) was to investigate the effects of group social support by internet-based synchronized face-to-face video and objective physical activity feedback on adherence to recommended exercise guidelines.
Methods:
Thirty stable heart failure patients (New York Heart Association class I–III), aged 64.7±11.5 years, were randomly assigned to an experimental or comparison group. Participants were provided a handout on self-care in heart failure, an exercise routine, a Fitbit Charge HR and were asked to wear the Fitbit Charge HR daily, and record their exercise sessions using both the Fitbit Charge HR and exercise diaries. In addition, participants in the experimental group connected to Vidyo software, once a week, for 8 weeks, for a 45-minute face-to-face online group discussion/education session.
Results:
Overall Vidyo session attendance was 68%, with 73% of participants attending five or more sessions. Adherence to exercise was 58.8% in the experimental group and 57.3% in the comparison group. The experimental group perceived receiving social support through the internet-based synchronized face-to-face video meetings but due to a small sample size and lack of adequate power, no significant impact on exercise adherence was observed. Participants commented that feedback regarding physical activity from the Fitbit Charge HR was helpful and motivational.
Conclusion:
Delivering social support by internet-based synchronized face-to-face video is feasible with heart failure patients. However, more investigations are needed to understand its impact on exercise adherence.
Introduction
Heart failure (HF), with 24.7% hospital readmissions within 30 days, has the highest re-hospitalization rates among all chronic diseases. 1 Exercise training has been utilized to improve on these findings, with the physiological benefits of this resulting in reduced mortality and hospitalization rates in these patients. 2 Nonetheless, patient adherence to exercise in this population has been found to be low.2,3 Unfortunately, the primary aim in many of the studies purporting to describe adherence to exercise in patients with HF primarily focuses on the physiological and psychological effects of exercise, and leaves adherence to be described as participation or attendance to the exercise program. 4 Strategies and interventions to improve adherence to exercise in a community setting have not been adequately studied, although a multidimensional approach to address this problem has been suggested. 5 In addition, reports of exercise adherence in HF patients have been primarily based on subjective data from exercise diaries, and methods to validate these exercise diaries with objective exercise data, especially in a community setting have been lacking.4,6
Adherence to an exercise program is often difficult to achieve, as it requires one to make both behavioral and lifestyle changes. In addition, the effectiveness of interventions designed to improve adherence can be complex requiring focus on behavioral change, social support and reinforcement. 7 The provision of social support has demonstrated positive improvements in exercise adherence. 8 To this end, the use of the internet to provide synchronous face-to-face video peer group support, as a method to improve adherence to exercise in this population, is intriguing but has not yet been investigated. 4 The potential for information sharing and applied positive social pressure can positively impact behavior, 9 potentially reducing perceived social isolation, which has been shown to impact health-related behavior negatively including participation in physical activity.10,11 HF patients appear to experience social isolation; 12 however, the use and effectiveness of the internet to connect HF patients socially and impact exercise adherence are unknown.
The impact of providing regular objective feedback on physical activity including exercise and exercise adherence in HF patients, with the use of modern wrist-worn activity monitors such as the Fitbit Charge HR (FCHR; Fitbit, San Francisco, USA) has not been investigated. The Move on Virtual Engagement (MOVE-HF) is a theory-based intervention to improve exercise adherence in patients with HF that incorporates the use of the internet as a strategy to provide peer group support and feedback on physical activity to improve exercise adherence. For this study, the internet-based synchronized face-to-face video (IBSF2FV) group discussion/education and support was provided using Vidyo software. Objective feedback on exercise and daily activity was provided with the FCHR.
The purpose of this pilot study was to investigate whether adherence to exercise in a community setting could be improved using the MOVE-HF intervention in patients with HF. Study aims were to compare the experimental and comparison groups on: (a) adherence to recommended exercise guidelines (150 minutes/week of moderate intensity exercise); (b) intention to adhere to recommended exercise guidelines; and (c) outcomes including: functional status, self-efficacy for exercise adherence, and perceived social isolation.
Methods
Design
The MOVE-HF study (Figure 1) is an 8-week experimental, randomized controlled two group (experimental and comparison) repeated measures design to pilot test the impact of the MOVE-HF intervention on improving adherence to the recommended exercise guidelines. A block randomization strategy, using sealed envelopes created by a statistician, was used for the random selection of participants. Thirty participants were recruited over a period of 3 months and all participants enrolled completed the study with no dropouts. To achieve a power of 80% with an effect size of 0.25, a sample size of 72 is desired. However, a sample size of 30 was determined to be adequate based on recommendations for feasibility studies. 13
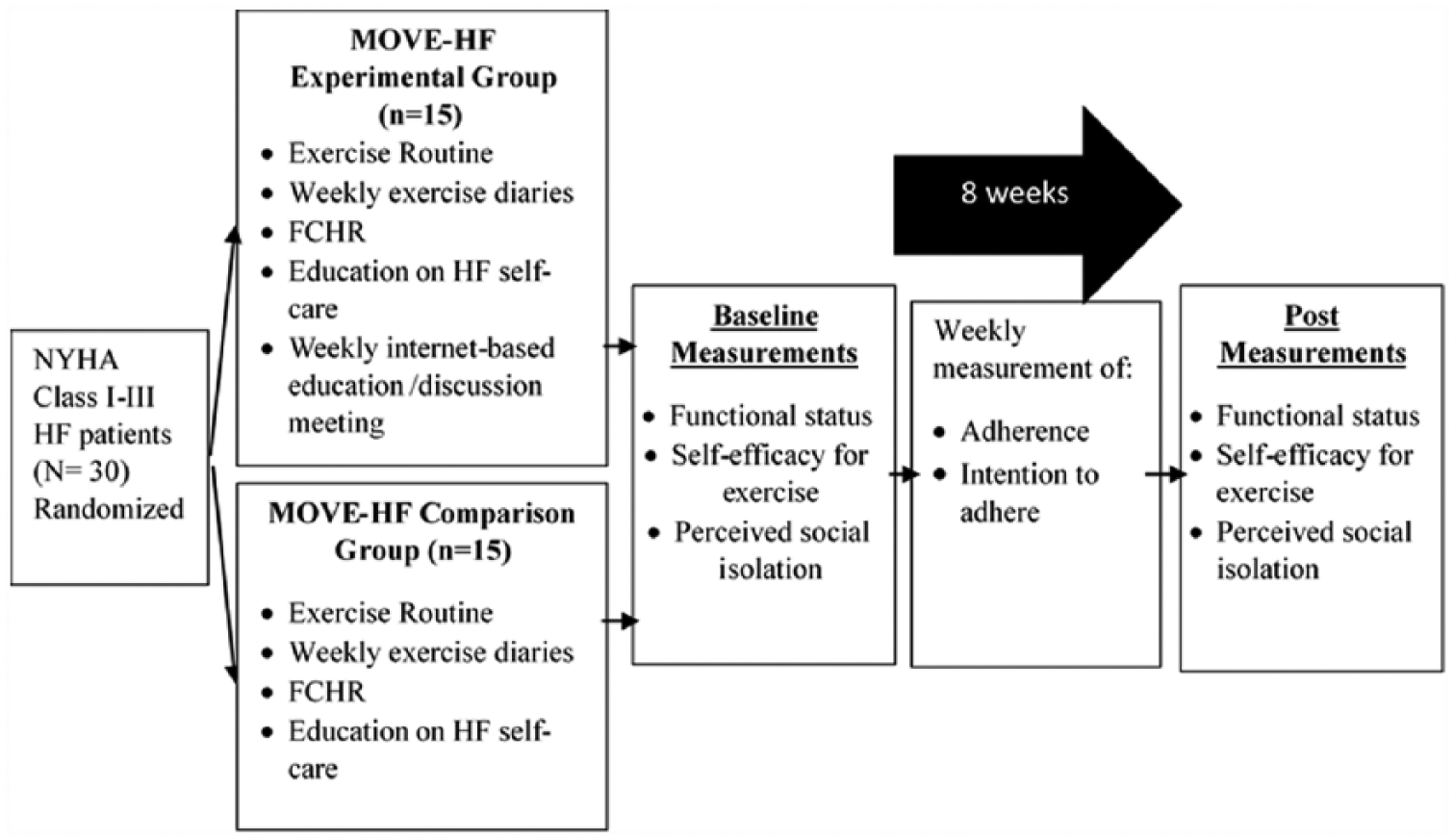
MOVE-HF study design. NYHA: New York Heart Association functional class; MOVE-HF: Move on Virtual Engagement – heart failure; FCHR: Fitbit Charge HR; HF: heart failure.
Participants
Patients were recruited from two cardiology practices in the midwest. Inclusion criteria required a diagnosis of New York Heart Association (NYHA) class I–III HF with no change in clinical history in the past 30 days and receiving standard pharmacological treatment with a stabilized dose of beta-blockers to elicit stable heart rate (HR) response, access to electronic devices (desktop/laptop/iPad/tablet/smartphone) with internet connectivity and cardiologist clearance to exercise. Participants were excluded if they were restricted from participating in aerobic exercise (orthopedic or neuromuscular disorders, and clinical evidence of decompensated HF) or were involved in any formal exercise (three times a week for 30 minutes or more) in the past 30 days.
Theoretical framework
The MOVE-HF intervention is based on Bandura’s social cognitive theory (SCT) and Ajzen’s theory of planned behavior (TPB), the most widely used theories in internet-based studies for behavioral change. 14 The TPB states that internal factors such as intention, which can be improved using the self-efficacy determinant of SCT,15–17 can influence performance of the behavior. 18 The theory-based intervention used in this study integrated the TPB and the SCT to study the impact of peer social support to improve self-efficacy and intention to adhere to exercise. Reduced perceived social isolation and verbal persuasion through the IBSF2FV group support is hypothesized to improve exercise adherence behavior.
MOVE-HF intervention
The components provided to participants in both the experimental and comparison group included the following.
Exercise routine
The exercise routine consisted of a community walking program to meet the recommended guidelines of 150 minutes a week of moderate intensity aerobic exercise.19–21 A Borg scale rating of perceived exertion (RPE) between 10 and 14 was primarily used to guide moderate exercise intensity. 22 To ensure safety during exercise, participants were provided with the average HR from their 6-minute walk test (6-MWT) at baseline. They were asked to monitor their HR during exercise and not to exercise at an intensity that caused the HR to exceed that number. Details regarding the exercise program and steps taken for the safety of the participants in a community setting have been described previously. 23
Fitbit Charge HR
The FCHR and the Fitbit software installed in the participants’ electronic devices were used to provide objective feedback on daily physical activity and objectively to validate the self-reported exercise diaries. The FCHR tracks, records and delivers information on step count, HR and active minutes in real time and provides the option of manually recording exercise sessions by way of an inbuilt stopwatch. Participants were asked to record all of their exercise sessions manually and to sync the FCHR to the Fitbit software to validate self-reported data. Details about the FCHR and objective validation strategies have previously been described. 23
Exercise diaries
All participants were provided with paper exercise diaries. For 8 weeks on a daily basis they were asked to record: exercise sessions (with date, duration and RPE), barriers faced, strategies used to overcome those barriers, and their intention to adhere to the recommended exercise guidelines on a scale of 1 to 5 at the beginning of the week.
Education on HF self-care
A web-link along with a handout on eight modules of HF self-care from the Heart Failure Society of America (HFSA) 24 were provided. These modules included: understanding HF, exercise and activity with HF, how to follow a low sodium diet, HF medication, dealing with HF symptoms, depression and anxiety with HF, managing lifestyle changes along with other chronic conditions and heart rhythm problems.
Social support through Vidyo (provided only to the experimental group)
The 15 participants in the experimental group were further subdivided into three cohort groups with five members each. For 8 weeks, each cohort met weekly for a 45–60 minute-long IBSF2FV education/discussion session using Vidyo. Vidyo is a software-based video conferencing application used to connect participants in distant locations for a face-to-face group audio/video conference. Each week, education was provided on one topic of self-care from the handout provided to the participants. Participants were encouraged to interact with other group members. These social interactions, targeted towards exercise performance and achieving adherence to the recommended guidelines, were intended to influence self-efficacy for exercise in the group members. The primary investigator (PI), who moderated these education/discussion sessions, provided encouragement to follow the exercise routine and suggestions on overcoming exercise barriers.
Measures
Adherence to exercise was measured by calculating mean adherence achieved over the 8 weeks based on self-report documentation (exercise diaries). Exercise adherence was calculated using the formula [(actual no. of min/wk)/(150 min/wk target goal) × 100]. 25 Participants were categorized as adherent (>80%), partially adherent (20–80%) and non-adherent (<20%) 26 based on mean adherence scores.
Intention to adhere to the recommended exercise guidelines was measured from subjective reporting from exercise diaries using a 5-point Likert rating scale with 1 indicating ‘weak’ and 5 indicating ‘very strong intention to adhere’.
Attendance to Vidyo group meetings was derived from PI maintained attendance records and overall attendance in percentage was calculated out of the possible 120 group meetings (15 participants × eight scheduled meetings).
Participant perception of the MOVE-HF intervention was measured using an investigator-developed survey completed at the end of the study. The survey captured: (a) participants’ perceptions of participating in the MOVE-HF study; (b) their experience in using the Vidyo software to connect with other participants; and (c) their experience on the use of the FCHR.
Functional status was measured using the 6-MWT. The test is valid and reliable for measuring physical function in cardiac patients in general (Cronbach α 0.97; r=0.687; P<0.001) 27 and more specifically, for patients with HF (r=0.579; P=0.001). 28 Participants were asked to walk laps in a 30 m long hallway and cover as many laps as possible in 6 minutes. The total distance walked in meters in 6 minutes was recorded.
Self-efficacy for exercise was measured using Bandura’s exercise self-efficacy scale (BESES) containing 18 potential barriers to exercise. The tool has documented reliability with a Cronbach α of 0.95 and validity with change in 6-MWT distance score (r=0.28; P=0.035). 29 Participants indicated their confidence level, on a scale of 0–100%, for exercising 30 minutes a day for five or more days a week when facing those barriers.
Perceived social isolation was measured using the Friendship scale for perceived social isolation. The tool contains six questions in Likert scale format and has been found to be reliable (Cronbach α 0.83) and valid (r=0.44; P<0.001). 30 A lower score indicates a higher perceived level of social isolation.
Procedures
The study complied with the Declaration of Helsinki and was approved by the institutional review board at the University of Nebraska Medical Center. Informed consents were signed and cardiologist approval was obtained prior to enrollment, which happened in three phases. In each phase, enrollment started after at least 10 participants met screening criteria. This was done to ensure that the experimental group participants, after random assignment, did not have to wait more than a week to attend the first IBSF2FV meeting. At baseline, all participants were asked to bring their electronic devices for the PI to set up the Fitbit and Vidyo software. They were trained on using the FCHR, performed the 6-MWT wearing the FCHR, and responded to two questionnaires (BESES and the Friendship scale). The average HR during the walk was recorded using the FCHR and provided to the participants. After providing adequate rest, the PI performed a 10 minute long walk with the participants to familiarize them with using the FCHR to record exercise sessions, and regulating exercise intensity using the Borg scale and the HR from the FCHR and to download data using the Fitbit software.
Apart from two participants who used desktop computers at home, the participants were able to set up all electronic devices during the PI baseline visit. Participants in the experimental group were trained on using the Vidyo software. To ensure that participants were competent in operating the software, a handout containing operational instructions was provided and the PI connected with them by means of Vidyo within 2 days of enrollment. Participants having difficulty connecting for this session were provided with instructions over the phone. The PI asked the 15 participants to indicate several times during the week their availability for the IBSF2FV group meetings and the time that worked best for each cohort was selected. The first week of the meeting was considered to be the start of the 8 weeks of intervention for each cohort.
All participants were also provided with educational materials (web link and handout) on eight educational modules on self-care in HF from the HFSA. Participants were asked to follow the exercise routine for the 8 weeks. At the end of 8 weeks, all participants performed the 6-MWT, responded to the two questionnaires (BSES and the Friendship scale), returned the FCHR to the PI and completed the survey describing their experience of participating in the study.
Data analysis
Exercise adherence and intention to adhere to recommended exercise guidelines across 8 weeks was analyzed using repeated measures analysis of variance (RMANOVA), with ‘week’ as the measure of time. In total there were eight time points. Effect size was calculated from the between-group differences. Functional status from 6-MWT scores was analyzed using RMANOVA with two repeated measures across time (baseline and post-8 weeks). Self-efficacy for exercise and perceived social isolation was analyzed using the non-parametric Mann–Whitney U test with change scores (post–baseline) to compare experimental and comparison groups for differences. Analysis was done using IBM SPSS 23. The level of significance was set at α=0.05.
Results
Participants’ ages ranged between 43 and 87 years and were predominantly Caucasian, married, retired and living in urban areas. At baseline, the two groups were comparable for demographic and clinical characteristics (Table 1).
Demographic and clinical characteristics of participants at baseline.
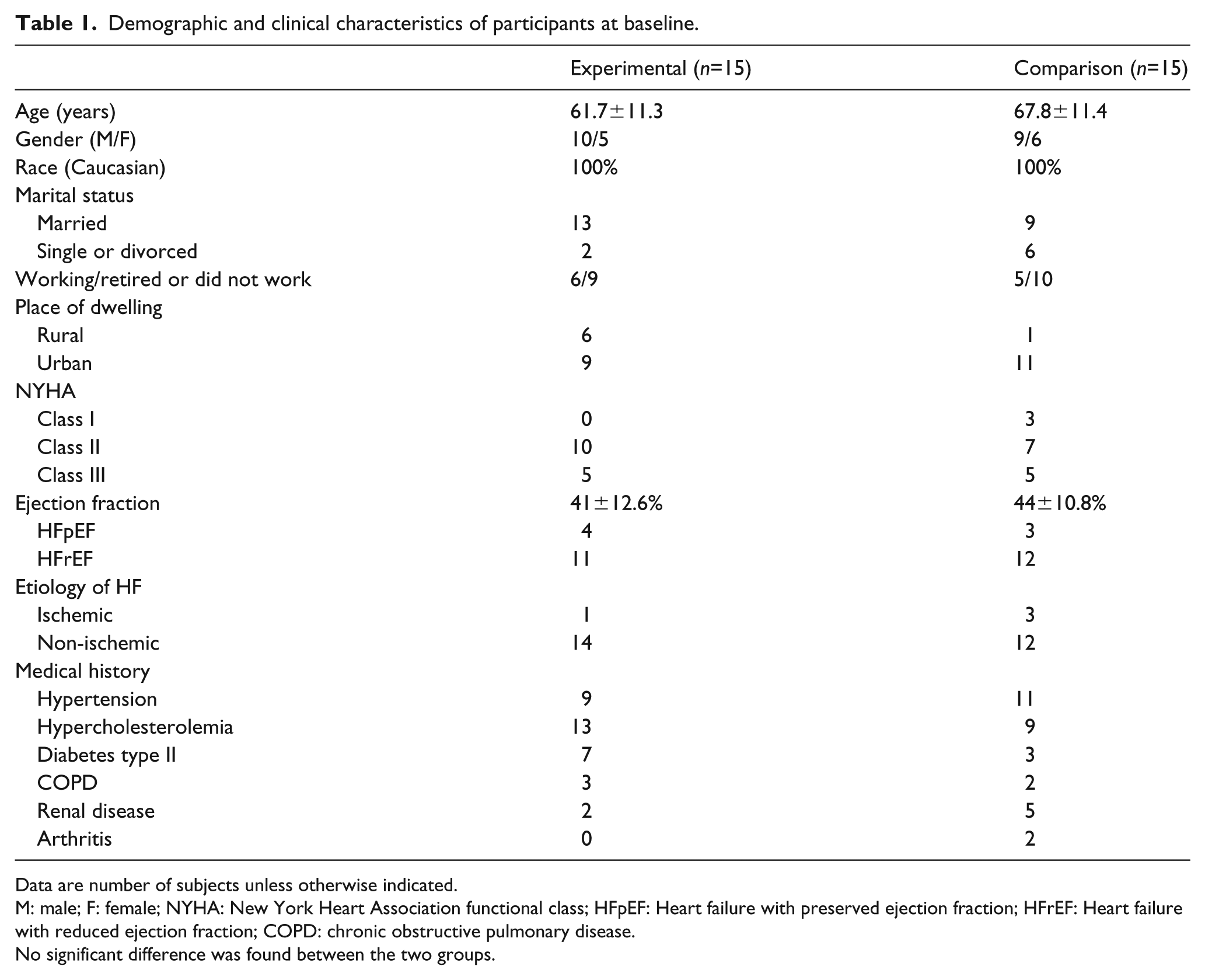
Data are number of subjects unless otherwise indicated.
M: male; F: female; NYHA: New York Heart Association functional class; HFpEF: Heart failure with preserved ejection fraction; HFrEF: Heart failure with reduced ejection fraction; COPD: chronic obstructive pulmonary disease.
No significant difference was found between the two groups.
The overall attendance to the IBSF2FV meetings was 68%, with 73.3% of participants attending five or more of the eight possible sessions. Reasons for absence included: being busy, forgot meeting time, on vacation, audio/video problems, internet issues, being sick and not interested in attending group meetings. It is worth noting that six of the 15 participants in the experimental group lived in rural areas and reported that the ability to attend the meetings from their homes was immensely helpful for attending the meetings on a weekly basis. Two participants, aged 83 years and 87 years, respectively, required spousal support to connect to the Vidyo platform or to operate the Fitbit software. These participants used desktop or laptop devices instead of smartphones or iPhones. Software updates for the FCHR and Windows 10 software created some technical problems but the PI was able to address those issues for the subjects. No participant reported safety concerns with the walking program and no hospitalization was reported relating to the study itself.
Aim 1: Table 2 and Figure 2 show the results of the MOVE-HF intervention on adherence to exercise between the two groups. No significant difference was observed in the interaction and individual effects of group and time.
RMANOVA results of mean duration of exercise (minutes/week) across the 8 weeks.
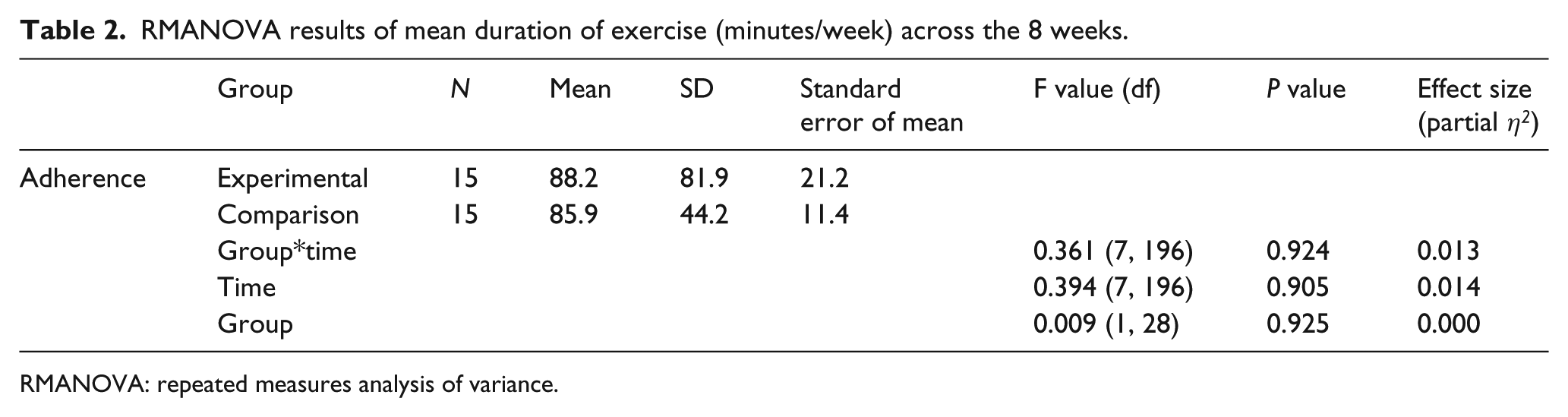
RMANOVA: repeated measures analysis of variance.
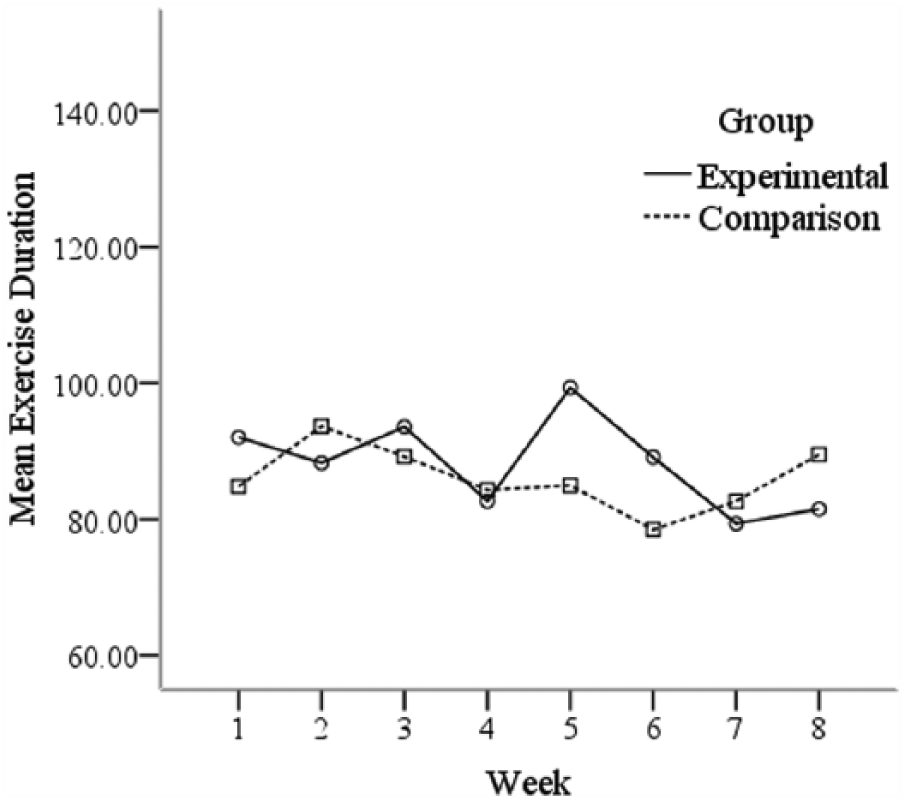
Mean duration of exercise (minutes/week) across the 8 weeks between the two groups.
Aim 2: Table 3 and Figure 3 show the results of the intervention on the intention to adhere to the recommended guidelines. No significant difference was observed in the interaction and individual effects of group and time. A separate analysis, examining the relationship between mean intention and adherence scores, showed a significant positive correlation (r=0.488; P=0.006).
RMANOVA results of mean intention scores for the two groups.
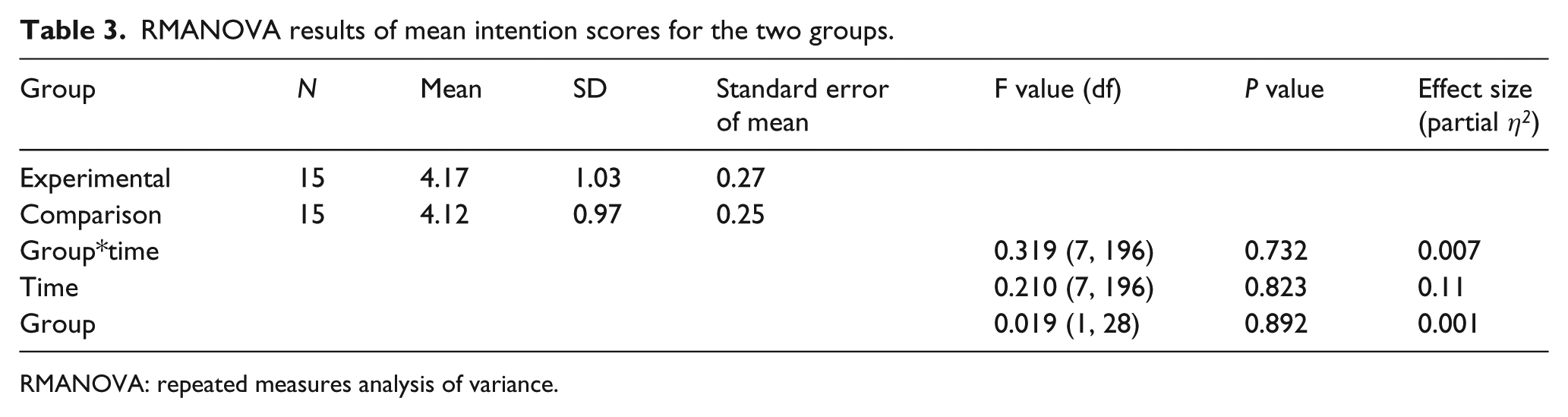
RMANOVA: repeated measures analysis of variance.
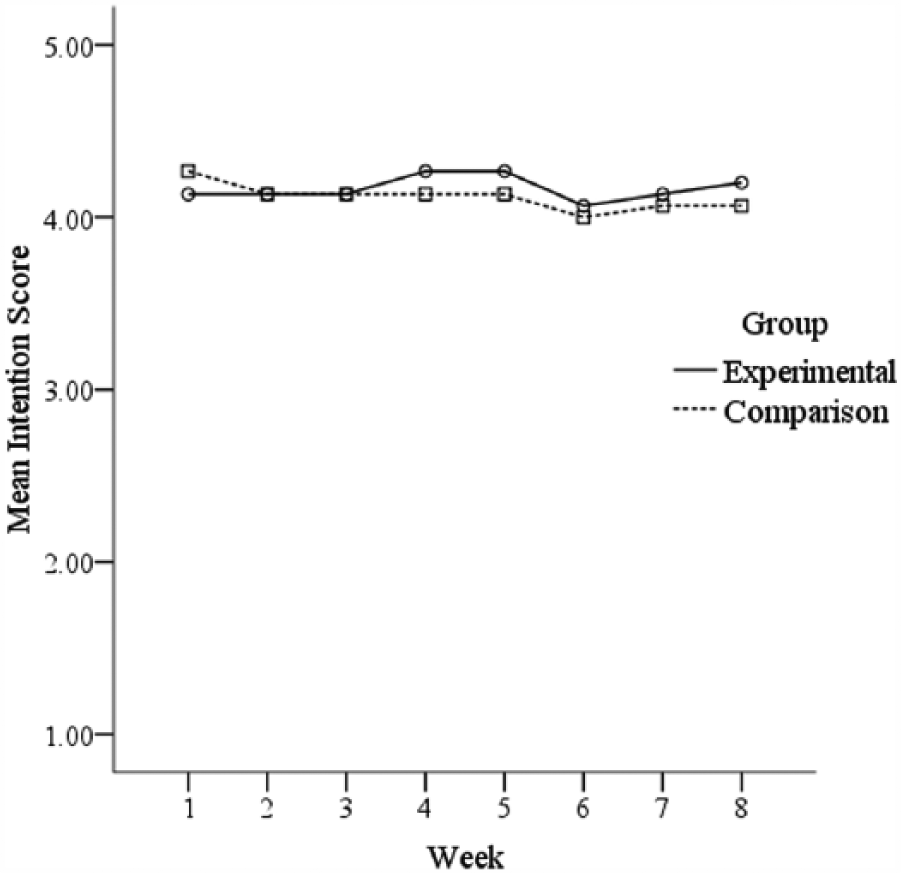
Intention to adhere to recommended exercise between the groups across the 8 weeks.
Aim 3a: Two participants did not perform the 6-MWT at the post-8 week assessment and were excluded from analysis. No significant difference was observed between the groups over time but RPE scores were reduced in both groups at post-intervention assessment (Table 4).
RMANOVA results of the 6-MWT score (meters) and RPE scores.
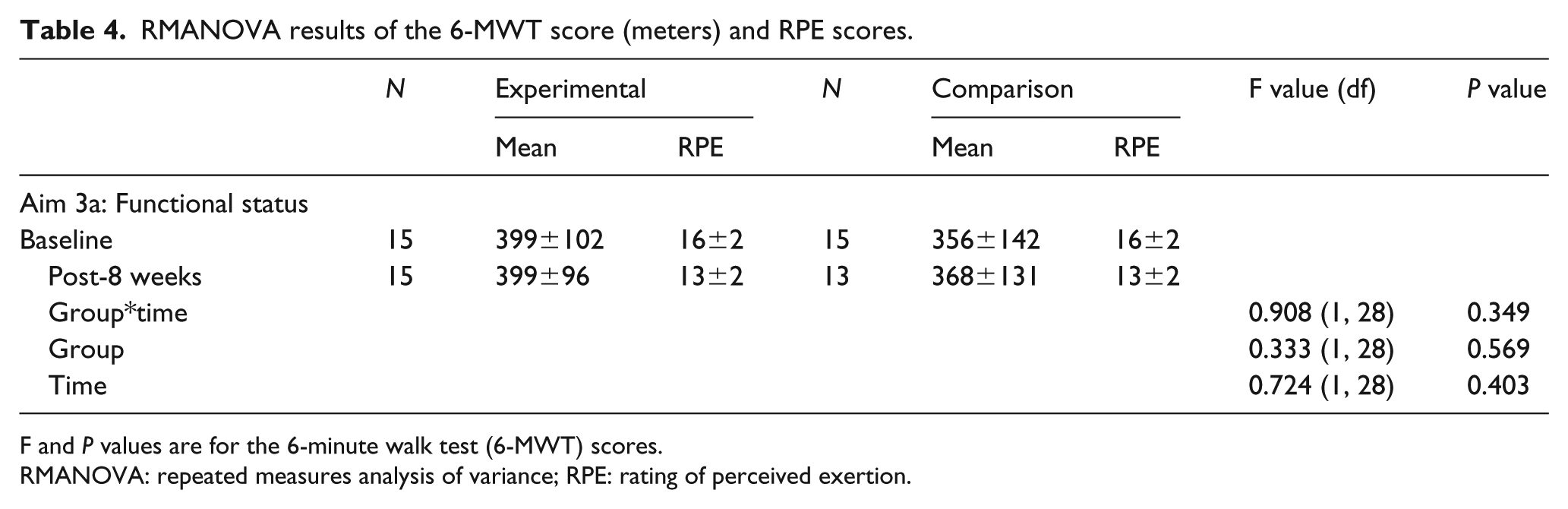
F and P values are for the 6-minute walk test (6-MWT) scores.
RMANOVA: repeated measures analysis of variance; RPE: rating of perceived exertion.
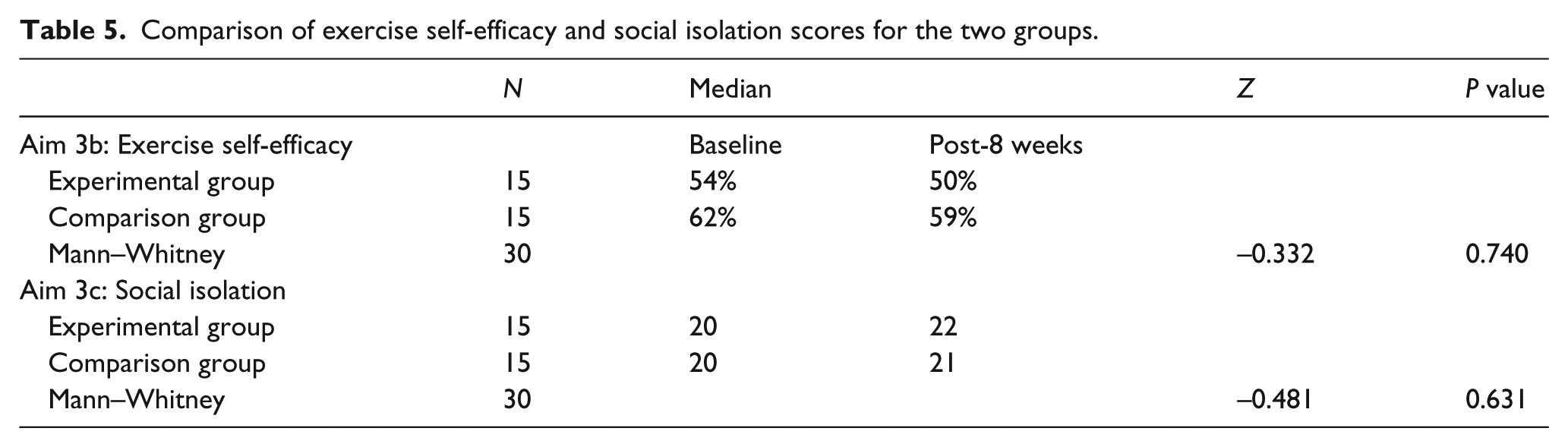
Aims 3b and 3c: No significant differences were observed between the groups on exercise self-efficacy and social isolation as outlined in Table 5.
Comparison of exercise self-efficacy and social isolation scores for the two groups.
Discussion and conclusion
This study investigated the use of a theory-based intervention to improve adherence to exercise in patients with HF by providing feedback on physical activity and an IBSF2FV group discussion/education meeting. Based on the recommended guidelines of 150 minutes a week of exercise, 20 the study found participants in both the experimental (88 minutes/week; 58.8%) and comparison (86 minutes/week; 57.2%) groups to be partially adherent with no significant difference in the mean weekly exercise time with an effect size of 0.013. Other studies that prescribed exercise programs of 90 minutes a week of low to moderate intensity exercise have reported higher levels of adherence than found in this study. 4 It may be that barriers experienced by HF patients can make adherence more difficult to achieve when exercising 5 days a week. Health, the use of diuretics, personal and professional issues and weather were identified as barriers to adherence to exercise by participants. During enrollment, most participants reported not being active, with two participants in the comparison group reporting inconsistent exercise about 1–2 days a week. The 6-MWT scores for both the groups at baseline were greater than 300 m, a considerable distance for HF patients, which may also be a factor for not observing significant differences in exercise adherence.
It may be that the dose of once a week for the group meeting was not strong enough and the experimental group participants, mostly leading sedentary lives, needed more group meeting sessions to facilitate full adherence to the recommended exercise guidelines. Thirteen of the 15 participants in this group mentioned no previous interaction with anyone with HF, and found it valuable to get to know and engage with other HF patients. Learning about the unique and common barriers to exercise other participants faced and being able to learn more about their own disease condition during the discussion/educational sessions are aspects of the MOVE-HF intervention that participants reported as beneficial. For example, five of the 15 participants also indicated that the weekly group meetings made them ‘accountable’ towards the other members of the group. In addition, during the 6th week of the intervention, two participants in the experimental group exchanged telephone numbers and connected with each other to walk together at a local mall. These anecdotal testimonies indicate that participants did perceive receiving some social support, although the sample size was too small to detect any significant change in behavior.
Both groups received a FCHR for objective feedback on physical activity and an educational handout on self-care in HF, which included a module on exercise in HF. The transtheoretical model refers to these interventions as ‘awareness raising’, which leads to contemplation about making behavioral change. 31 It may be that the interventions, which participants in the comparison group received, were significant in leading to exercise adherence levels comparable to the experimental group. It is also possible that the 8-week timeframe was too short to be able to detect a benefit from the IBSF2FV component of the intervention group due to the initial ‘awareness raising’ that occurred in the comparison group, which may wane over time. The survey showed that the feedback on step count and heart rate received from the FCHR made participants in both groups more conscious of their activity levels and accountable to themselves, and was instrumental in helping them become more active. Participants in both groups found the target of walking 30 minutes a day to be a motivator, while others found the step count information to be motivating. Twenty-seven of the 30 participants indicated that, even on days that they did not exercise, the FCHR provided them with a constant reminder of their activity levels and prompted them to follow the exercise routine. Of note, participants were required to return their FCHR at the end of the study, and nearly 83% of participants had already bought their own FCHR or a similar activity monitor or were planning to buy one by the time they completed the study.
No significant difference in intention to adhere to exercise was observed between the two groups. A significant positive correlation existed between strength of intention and exercise adherence validating the assertions made by the TPB. However, the high mean intention scores did not translate into achievement of the desired outcome behavior of high exercise adherence. Factors may exist that prevent HF patients from adhering to exercise in spite of having strong intentions. In this study, two participants in the experimental group self-reported depression in the survey. One among them stated that his strong intentions did not result in exercise behavior because of being acutely depressed. Depression is a prevalent comorbidity in HF32–34 that influences functional decline 33 and has been identified as a barrier to exercise adherence in this population. 26 In fact, the presence of depression is associated with a threefold increase in non-adherence to medical treatment. 35 HF patients suffering from depression may require additional support to become adherent to exercise.
HF patients may require personalized interventions to overcome unique barriers in achieving exercise adherence. Unfortunately, in the present study the effect of social support in the form of an IBSF2FV group discussion/education on exercise adherence and intention to adhere to recommended exercise guidelines could not be determined because of inadequate power.
Functional status, determined by the 6-MWT, was not significantly different between the groups. Although the mean 6-MWT score did not change significantly from baseline in either group, the 6-MWT RPE scores post-completion did change (P=0.0001). These findings indicate that participants were less fatigued and perceived less exertion when walking a similar distance. Although the study purpose did not focus on improving exercise capacity, as RPE improved, it may be that a longer intervention with a larger sample size might have led to measurable functional improvement. Also, performing the 6-MWT on two separate days at baseline and at 8 weeks may have also helped to negate any error that occurred in conducting the test.
Self-efficacy scores for adhering to recommended exercise guidelines were not significantly different within and between groups pre and post-intervention. It is possible that the educational material and exercise monitoring devices in both groups had an impact on self-efficacy. Initial overestimation of self-efficacy has been shown to affect performance negatively 36 and it is possible that participants overestimated their confidence scores at baseline. These claims are made cautiously due to the small sample size and lack of adequate power.
Similarly, no difference was observed in perceived social isolation scores between groups. The lack of difference or effect may be related to the low levels of perceived social isolation found in the sample at baseline. Unlike NYHA class IV HF patients, who were not included in the present study, NYHA class I–III HF patients may experience less social isolation. A study to evaluate perceived loneliness in HF patients found that the vast majority of NYHA class I–III HF patients and HF patients even with an ejection fraction of less than 30% may not report perceived loneliness. 37 From the anecdotal comments on the survey completed by participants, it appears that participants did perceive some aspect of social support from the intervention. However, due to lack of power with the small sample size, it is unclear whether the intervention was actually not effective in improving social isolation or whether the tool used to measure social isolation was not sensitive to the changes.
With the calculation of adherence at eight different time points, a sample size of 30 did not provide sufficient power to detect between-group differences in exercise adherence, and resulted in only a small effect size. A mean difference of greater than 115 minutes of exercise time between the two groups would have been required to observe a significant difference. It is noteworthy that the comparison group also received a FCHR and educational material. Had the comparison group not received this intervention, the effect size may have been larger. Activity levels at baseline were determined from subjective response to inclusion criteria during screening. As such, it is unknown whether there was any difference in activity levels between the two groups at baseline. The length of the intervention of 8 weeks may not have been long enough for the study purpose. As a post-intervention follow-up was not performed, the long-term effects on adherence after completion of the intervention are unknown.
In conclusion, this pilot study was designed to improve exercise adherence in patients with HF and is the first to test whether social support provided through IBSF2FV group discussion/education can help these patients become adherent to recommended exercise guidelines. The long-term impact of an IBSF2FV intervention on exercise adherence using a larger sample should be investigated. Future research should also incorporate strategies for overcoming unique exercise barriers in HF and goal setting for minutes per week of exercise or step count over time to help progress participants towards meeting recommended exercise guidelines. It is important to investigate ways to help patients with HF become more adherent to exercise. Providing objective feedback on exercise and physical activity may be an important factor for promoting adherence to exercise.
Footnotes
Based on this research, internet-based synchronized face-to-face video interventions to provide social support and education are feasible in the heart failure population. Patient engagement can be an essential component for developing exercise adherence that can be delivered through internet-based synchronized face-to-face video. Interventions using the internet can help to provide access to heart failure patients living in both urban and rural areas. Challenges faced with the use of technology can be overcome with adequate training. Heart failure patients appreciate objective feedback on physical activity, specifically information on heart rate and step count, with the use of wrist activity monitors such as the Fitbit Charge HR. Such objective feedback can be a motivator for heart failure patients to adhere to exercise.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
The study was funded by the Midwest Nursing Research Society/Center for the Advancement for Nursing Sciences (MNRS/CANS) dissertation grant for 2016. No funding was received from Fitbit for the project.