
Abstract
Background:
Cardiovascular diseases are considered a leading factor in mortality and morbidity. The older adult population with cardiovascular diseases has a higher risk of falls as compared to a matched age healthy population.
Objective:
To investigate the effect of stability and coordination training within a cardiac rehabilitation programme on fall risk in older adults with cardiovascular diseases enrolled in cardiac rehabilitation.
Methods:
Twenty-six people with cardiovascular diseases (age 74±8) were divided randomly into intervention and control groups. The intervention group received 20 min of stability and coordination exercises as part of their 80 min cardiac rehabilitation programme, while the control group performed the traditional cardiac rehabilitation programme, twice a week, for 12 weeks. Balance assessment was based on three tests: the Timed Up and Go, Functional Reach and Balance Error Scoring System, which were measured twice before the intervention, once following the intervention and once four weeks after the termination of the intervention. A two-way analysis of variance (group × time) with repeated measures was performed to examine differences between groups and between assessments.
Results:
Seventy per cent of participants in the intervention group adhered to the programme, with significant improvement post-intervention in the Timed Up and Go (p < .01) and the Balance Error Scoring System (p < .05) with no changes among the control group.
Discussion:
Stability and coordination training alongside a traditional cardiac rehabilitation programme may improve static and dynamic balance, and muscle strength, skills that are considered major components in postural control. Clinicians who work in cardiac rehabilitation centres should consider including this training alongside the routine cardiac rehabilitation programme.
Introduction
The life expectancy of people with cardiovascular disease (CVD) has improved in recent years. Nevertheless, CVD is the number one cause of death in the developed world, 1 and prevention of morbidity and mortality following CVD events remains an important goal after hospitalization discharge.2,3 Drug therapy is the main intervention strategy of secondary prevention. At the same time, cardiac rehabilitation (CR) based on physical activity has also been recognized as an intervention which is as effective as drug therapy.3,4 Physical activity interventions as suggested by the American Heart Association (AHA) and the European Society of Cardiology (ESC) guidelines should include aerobic and resistance training for the improvement of heart function, endurance capacity of the skeletal muscle and muscle strength.3,4 However, there is no specific recommendation for stability and coordination training for people with CVD, a modality that may improve their balance control and potentially prevent falls.
Falls among the general older adult population are associated with high morbidity and mortality, and involve high costs of medical services. 5 Enhanced balance during activities of daily living may improve their confidence and efficacy which can consequently lead to higher participation in other activities and improved quality of life.6,7 In addition, improved balance may reduce injuries caused by falls. 8
While there is little evidence on the balance function of people with CVD, 9 there are several factors that place them at a particularly higher risk for falls than their healthy counterparts. For example, there are non-preventable occasions such as arrhythmia or sudden changes in blood pressure that increase the risk of falls due to loss of consciousness, while temporary amnesia and an acute decrease in cerebral blood pressure may cause temporary loss of balance and falling without loss of consciousness.10–12 Furthermore, the effect of polypharmacy, or changes in dosage might also increase the risk for falls,6,13 as some of these medications help to lower blood pressure and heart rate which may lead to weakness or dizziness. As such, while the literature linking CVD to falls is scant, it does point to a higher risk due to possible comorbidity. 7
While falls cannot be entirely prevented among older adults with CVD due to the comorbidity described above, the improvement of balance control can prove a beneficial tool for lowering the risk. While former studies have examined the effect of exercise intervention including aerobic exercise and strength exercises with the assumption these would improve balance and stability,7,8,14 Beauchamp et al. showed that specific balance exercise improved balance performance, self-reported physical function and lower-extremity muscle strength among people with chronic obstructive pulmonary disease (COPD) who were at risk of falling. 15 For CVD patients, three studies incorporated specific balance exercise into the CR programme.16–18 All three programmes were based on 36 sessions, three times a week, which is much more intensive than the traditional CR programme in most places (usually based on twice a week routine). The difficulty in adhering to such a long-term programme raises questions about its applicability. The current intervention examined the direct effect of specific exercises designed to improve balance and coordination among CVD patients, which were incorporated into the traditional twice-weekly, 12-week CR programme. The first aim of the current study was to investigate the feasibility of implementing stability and coordination training into a standardized CR programme. The second aim was to assess the effect of this programme on balance control and functional strength among people with CVD who participated in the experimental CR programme.
Method
Study design
The current study was an exploratory study, which was based on a prospective, double-blind, randomised controlled trial. It comprised four assessment sessions and twelve weeks of intervention. The assessment sessions were conducted in the following order: two pre-intervention assessments at four weeks and two weeks (baseline 1 and baseline 2, respectively) prior to the initiation of the intervention, 48 hours post-intervention, and retention assessment that was conducted four weeks after the termination of the intervention. The values of the dependent variables measured in the two pre-intervention assessments were used for establishing baseline values. These two assessments were performed in order to keep track of changes that were independent of the intervention, such as familiarization with the test or natural aging-related processes. Participants were randomly assigned to an experimental or control group and they were not informed of their treatment allocation. Data collection was performed by an examiner who was blinded to the group allocation. The investigation conforms with the principles outlined in the Declaration of Helsinki. The regional ethics committee of Hillel Yaffe Medical Centre approved this study (protocol no. 0083-16-HYMC). Each participant signed an informed consent form prior to taking part in the study.
Study population
Based on an a priori power analysis using the Timed Up and Go (TUG) test as a primary outcome for fall risk assessment, 20 and the following parameters: effect size f > 0.38; α = 0.05; power (1-β err prob) = 0.8; number of groups = 2, 40 volunteers from an inpatient CR centre were recruited for the study (20 participants in each group). The inclusion criteria were a CVD diagnosis, age over 65 years, registration to the CR centre, and ability to execute physical activity over 80 min. Exclusion criteria included an orthopaedic disability, a neurological or cognitive impairment, and an inability to sign an informed consent due to lack of sound judgment. During the intervention period fourteen participants (seven from each group) dropped out due to health or other personal issues. As such, data analysis was conducted on data collection from 26 participants (see Appendix A in the supplementary material online). The demographic and clinical characteristics of the participants are presented in Table 1.
Demographic and clinical characteristics of participants.
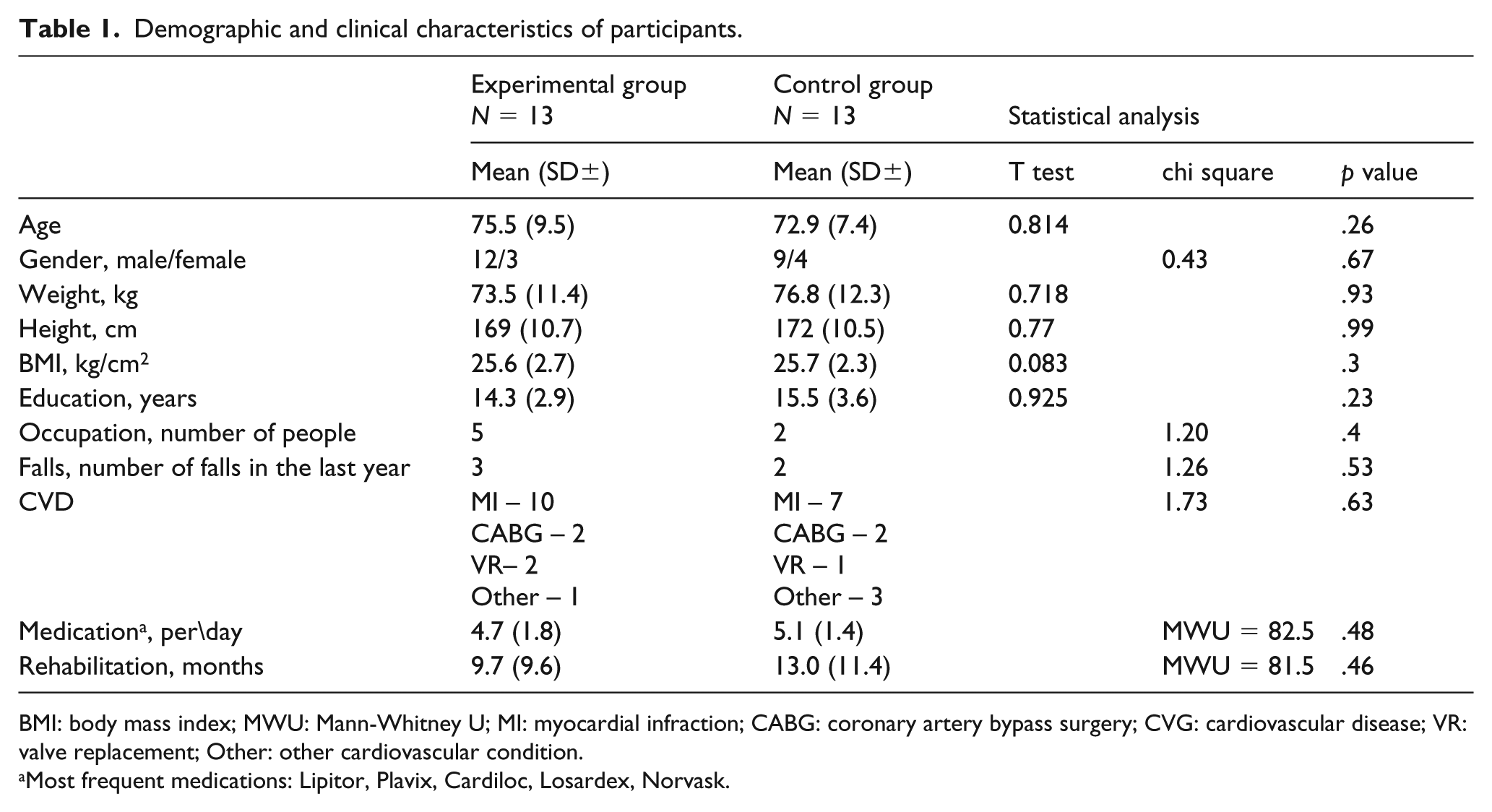
BMI: body mass index; MWU: Mann-Whitney U; MI: myocardial infraction; CABG: coronary artery bypass surgery; CVG: cardiovascular disease; VR: valve replacement; Other: other cardiovascular condition.
Most frequent medications: Lipitor, Plavix, Cardiloc, Losardex, Norvask.
Intervention
The intervention for both groups lasted 12 weeks and included 80 min of physical activity training, twice a week, at the CR centre. Each training session was instructed by a qualified physical education teacher and included the following: (a) 20 min warm-up; (b) 45 min of aerobic exercise at moderate intensity, based on each participant’s personal aerobic fitness and programme (on treadmill, bike, rowing device or hand bike); (c) 10 min resistance training at moderate intensity, based on each participant’s personal programme, using designated machines in the gym; (d) 5 min cool-down.
In the first part of the session, while the control group performed a traditional warm-up, which was composed of stretching exercises for both the upper and lower limbs, and light walking, the intervention group performed stability and coordination training exercises. These training sessions were developed based on fall prevention strategies,19,20 and were delivered in small groups of 5–8 participants. Each session was designed to challenge stabilization ability. Exercises included reducing the base of support, changes in the height of the centre of gravity, changes in the standing surface, reducing the source of visual information, eye–hand coordination and dual-tasking exercises. 21 All exercises were performed next to a chair that could be used for support in case the participant felt loss of balance or confidence. The programme progressed as the participants increased in confidence in performing each exercise. For example,
Standing barefoot on one leg on a firm surface, the other leg bent at the knee; moving one hand to a certain point (‘imagine your hand is a hand on a clock and it is pointing to six o’clock’) and keeping it there for 3 s, then moving the hand to another point and keeping it there for 3 s.
Standing barefoot on one leg on a firm surface, moving the other leg and the unilateral hand to a certain point (or to different points at an advanced level).
Standing barefoot on one leg on a firm surface, the other leg bent at the knee; holding a soft ball in both hands, throwing it up and catching it several times.
Standing barefoot on one leg on a firm surface, the other foot placed on a soft ball; Performing round circles with the ball on the surface.
Sitting on a chair, standing up and catching a ball which is thrown from different directions by the clinician.
For exercises 1–4, each exercise is also performed while standing on the other leg, after performing it on the first leg. Advanced level involves performing the same exercise on an unstable surface (boso, stability disc, sponge cube), performing it with eyes closed or conducting cognitive tasks, such as counting down numbers (i.e. 100–7) (see Appendix B in the supplementary material online).
Measurements
In their first assessment session, participants completed a general demographic questionnaire, and a more detailed questionnaire about their medical status. In addition, two types of primary outcomes were applied in each assessment session:
Balance assessments
TUG is a measure of the duration of time it takes to stand up from a seated position in a chair, walk 3 m, walk around a plastic cone, and return back to sit on the chair, measured in seconds. 22 A shorter duration indicates better stability. The test was performed twice. The average score was used for data analysis. The TUG is considered an indicator of fall risk, 23 and its reliability and validity are high (r = .99 and r = .93, respectively). 24 The minimum clinical change required for improvement is 0.8–1.4 s. 25
Functional Reach (FR) refers to the distance a participant can reach forward beyond arm’s length, 26 while standing aside a wall, without touching it, at 90° of shoulder flexion with a closed fist and maintaining a standing fixed base of support, measured in centimetres. Participants were instructed to reach forward as far as they could without taking a step. The test was performed twice. The average score was used for data analysis. The reliability and validity for this test are high (r = .92) and medium (r = .64–.71), respectively. 27 Values lower than 18.5 cm indicate fall risk. 28 The minimum clinical change required for improvement is 4–8 cm. 27
In the Balance Error Scoring System (BESS), 29 participants were instructed to stand in three positions (narrow double leg stance, single leg stance and tandem stance) on two different surfaces (firm surface/floor or medium density foam). Each position was maintained, with hands on hips and eyes closed, for 20 s. Scores were given for specific errors, including opening eyes, lifting hands off hips, stepping or stumbling. If the participant was unable to stand without an error for 5 s, he/she received 10 points (out of 10). Therefore, a higher total score reflected poorer static stability. Reliability and validity for the BESS were found to be high (r = .88) and medium (r = .31–.79), respectively. 29 The minimal significant clinical change for this test is 3 points. 27
Functional strength assessment
In the Five Time Sit to Stand Test (FTSST), 30 participants sat on a standard armless chair (with a seat height of 43 cm), their back upright and their feet flat on the floor 10 cm behind their knees. The participants were instructed to stand up with their hips and knees in full extension and then to sit down five times as quickly and safely as they could without using their arms. The time from the command ‘Go’ until the participants’ back touched the backrest of the chair on the fifth repetition was recorded in seconds, and the average time from two trials was used for data analysis. The test is considered a measure of functional lower limb muscle strength. Reliability and validity for the FTSST were found to be high (r = .89 and r = .92), respectively. Significant minimal clinical change is 2.3 s. 27
Adherence
Prior to each intervention session an attendance list with the participants’ names was checked for adherence assessment.
Statistical analysis
The assessments of the dependent variables measured during baseline 1 and baseline 2 were performed for establishing baseline values and to keep track of changes that were independent to the intervention (such as familiarization with the tests or health status changes). Differences in those two baseline assessments were tested by using a paired t-test. A one-way analysis of variance (ANOVA) was performed to examine differences between groups in the first assessment. A two-way ANOVA (group × time) with repeated measures on the last factor, was performed to examine differences between groups and between assessments, for each variable separately. Two-tailed p < .05 was considered statistically significant. Contrast comparisons were used for post hoc analysis. In addition, the effect size of the differences was calculated using Cohen’s d procedure (the differences in means divided by the standard deviation in either group). Values lower or equal to 0.2 are considered a small effect size, values between 0.21 and 0.8 are considered a medium effect size, and values higher than 0.81 are considered a large effect size. 31
Results
Demographic and clinical characteristics of the participants
As can be seen in Table 1, no significant differences in characteristics were found between the two groups at baseline.
Baseline assessments
No significant differences were found between the two baseline assessments in three (FR, FTSST and BESS, p > .05) out of the four measured variables. On the TUG variable, a significant difference was found, indicating an average improvement of 0.32 s in the performance from baseline 1 to baseline 2. This improvement is considered to be clinically negligible; 25 therefore the mean of the values from the first and the second assessment prior the intervention was calculated for each variable, and was considered to represent the baseline average (pre-intervention values).
The statistical analysis of this new baseline value revealed no significant differences between the two groups (p > .05 for each variable separately).
Adherence
Participants in the intervention group attended a mean of 16.8±2.4 stability and coordination training sessions (out of 24 sessions), implying a compliance of 70%. It is important to note that participants were not informed of their treatment allocation from the start of the study until its termination. As participants from the groups trained on different days, they had no opportunity to share experiences, or find out to which group they belonged.
Intervention effect
All variables were found to be normally distributed at each assessment point (as was assessed by Skewness & Kutosis z-values). As no significant differences of age were found between the groups, the analysis was not adjusted for age. The differences in the fall risk assessment variables between pre-intervention, post-intervention and follow-up for the intervention group and the control group are presented in Figures 1–3.
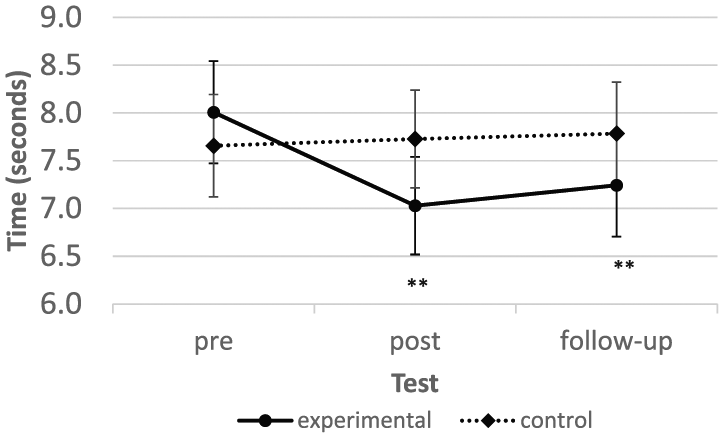
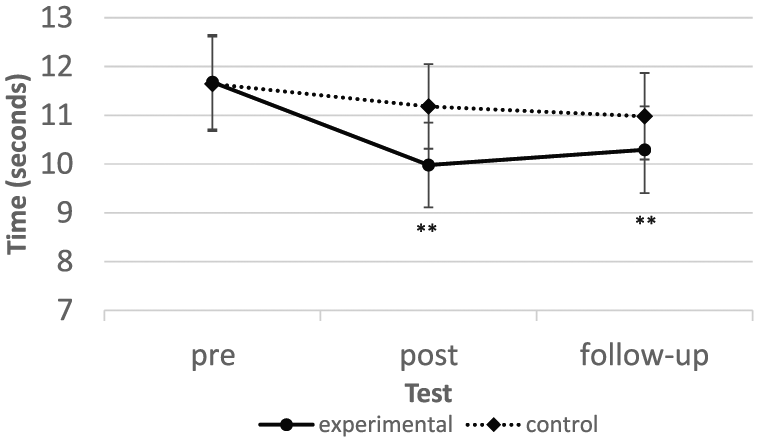
Mean TUG scores (s) ± SE for experimental and control groups in three testing sessions: pre, post and follow-up.
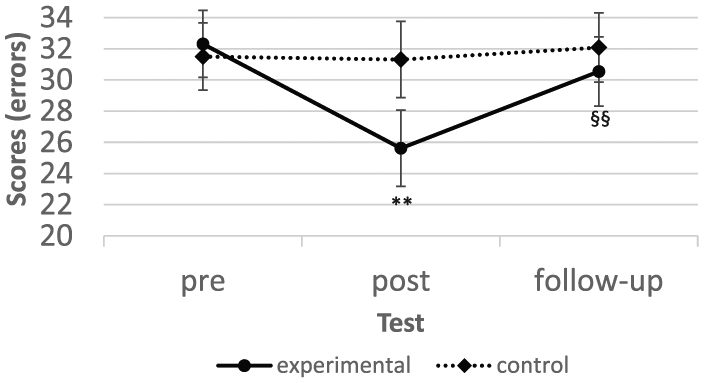
Mean BESS scores (au) ± SE for experimental and control groups in three testing sessions: pre, post and follow-up.
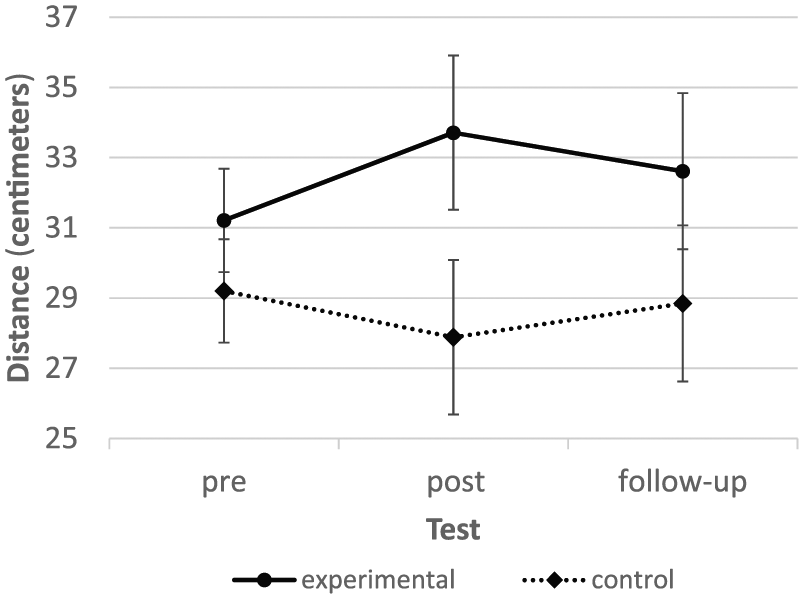
Mean FR scores (cm) ±SE for experimental and control groups in three testing sessions: pre, post and follow-up.
As can be seen in Figure 1, a significant time effect (F2,48 = 9.18, p < .01) and a time × group effect (F2,48 = 13.51, p < .01, d = 0.54) were found in the TUG. In post-hoc analysis it was found that while significant improvement was found in the intervention group between pre- and post-assessments (p < .01), and between pre- and follow-up assessments (p < .01), no differences were found between assessments in the control group (p > .05).
As can be seen in Figure 2, a significant time effect (F2,48 = 5.36, p < .01) and a time × group effect (F2,48 = 4.29, p < .05, d = 0.84) were found in BESS. Post-hoc analysis indicated that while a significant improvement was found in the intervention group between pre- and post-assessments (p < .01), and between pre- and follow-up assessments (p < .01), no differences were found between assessments in the control group (p > .05). It is important to note that in the intervention group, pre- to post-assessment indicated an improvement, but from post- to follow-up assessment a significant decrease in performance was found.
As can be seen in Figure 3, no significant time effect or interaction was found (F2,48 = 0.19, p = .83) for FR.
For FTSST, differences in the functional strength assessments can be seen in Figure 4. Statistical analysis revealed a significant time effect (F2,48 =8.49, p < .01), with no time × group effect (p > .05). However, as can be seen in the figure, post-hoc analysis revealed a significant improvement from pre-assessment to post-assessment and to follow-up, only for the intervention group.
Mean FTSST scores (s) ± SE for experimental and control groups in three testing sessions: pre, post and follow-up.
Discussion
The results of the current study indicated that 20 min of balance exercises, incorporated within a traditional CR programme, improved the balance of older adult CVD patients. These results imply a reduction in the risk of falls among this population which is vulnerable to falls. 15
Risk of falls was assessed by strongly validated tests: the TUG and the FR, as representing risk of falls among older adults.23,28 The significant improvement of 0.98 s that was found in the TUG among the intervention group in the current study is considered a minimal clinical improvement. 25 That is, the change in the time to perform this task, although small, is significant, as it implies improvement in the ability to perform simple tasks during activities of daily living and has significant importance to quality of life.8,14,27 No significant changes were found in the control group, and as such, there was a significant interaction between the measurement time × group with a medium effect size (d = 0.54); that is, participation in the stability and coordination training programme led to a significantly greater improvement than the routine exercise programme performed by the participants in the control group. It is likely that the improvement found in this test was a result of the training exercises which included stimulation of the vestibular organ through changes in the direction of the body and in the heights of the centre of mass. 21
Similar results were shown by Chen et al., 16 who found a significant improvement of 1.3 s in the TUG test among the intervention group which practised 36 sessions with 60 min of strength and balance exercises in addition to 50 min of cardiopulmonary exercises, compared to the control, which received only medical management. Such improvement was also found by Busch et al., 17 who assessed the effect of an additional 30 min of balance training to a traditional 30 min of aerobic exercise, five times a week for three weeks, among people with CVD. They found a significant improvement of 2.0 s in the TUG test in the intervention group, compared with a significant improvement of 1.0 s in the control group which participated in the traditional CR programme.
The greater improvement found in both studies of 1.3 and 2 s,16,17 respectively, compared to 0.98 s in the current study may be explained by the amount and frequency (36 sessions, three times a week) of the balance programme which was higher in comparison to the programme that was performed in the current study (24 sessions, twice a week). Nevertheless, the improvement in the current study was also clinically significant. Therefore, it is reasonable to suggest that people with CVD who are at their chronic phase of rehabilitation may achieve meaningful improvement by 20 min of balance training during the traditional CR programme.
Unlike the TUG, no significant changes were found in the FR test among either group in the current study. It is possible that the exercises used in the stability programme did not sufficiently train the limits of the base of support, a skill which is needed for better performance in the FR test. It is also possible that the duration of the current intervention or the amount of practice was insufficient. In contrast to the findings of the current study, Taylor-Piliae et al. found that 12 weeks of tai chi practice, 18 three times a week, led to a significant improvement in the FR test among participants with cardiovascular risk factors by almost 3 cm. This improvement was probably due to the greater frequency of practice (36 in comparison to 24 in the current study), but also due to the tai chi training routines which are based on increasing the joints’ range of motion while shifting body weight from one leg to the other.
The BESS test was used in the current study to assess static stability, which is also important for postural control among older adults. A significant improvement of 6.7 points, which is considered a minimal clinical change, 27 was found in the intervention group, with no significant changes in the control group, resulting in a significant interaction between the time × group, with a high effect size (d = 0.84). This test is based upon three positions (narrow double leg stance, single leg stance and tandem stance) performed with eyes closed on two different surfaces (firm surface/floor and medium density foam). Thus, the improvement found in the intervention group is probably due to exercises that included stimulation of the proprioceptive system through the use of different surfaces on which the participants stood, and the combination of exercises with eyes closed. According to Iverson and Koehle, 29 this improvement may help prevent future falls, as the assessment is based on the functions required when performing basic activities of daily living. It is important to note that the BESS test scores were relatively low in the current study (24–33) when compared to the average scores (16–24) presented in the study by Iverson and Koehle, 29 who assessed older adults at an average age of 65 with no illnesses. This finding indicates that adults with CVD are indeed deficient in postural control and are, therefore, more prone to falls. In addition, when comparing the follow-up assessment to the post-test, there was a significant decrease of almost 5 points, among the intervention group, which suggests that the stability and coordination systems should be continuously stimulated. Chen et al. examined the effect of a training programme that included strength training and aerobic exercise for 12 weeks, three times a week, on static stability in people diagnosed with one or more of the following chronic diseases: CVD, osteoporosis and type 2 diabetes. 32 They assessed static balance using a single leg stance test. In their study, no significant improvement was observed in the one-leg stance, indicating that specific training, as supported by the intervention in the current study, is an important factor for improving stability and reducing the risk of falls.
Functional lower extremity strength was assessed in the current study by the use of the FTSST test. This function is an important component in determining the quality of life of an adult. 30 The FTSST test is based on both explosive power and endurance of the lower extremity muscles. The test simulates some of the basic skills in daily life, such as getting up from a chair as fast as possible to get to the toilet. Its success demonstrates the degree of independence among older adults. Increased time on this test reflects disability and a decreased ability in daily function. 30 In the current study, the intervention group showed a significant improvement of 1.7 s following the intervention. Although this improvement did not achieve the minimal clinical change of 2.3 s, 27 a significant interaction of time × group with a moderate effect size (d = 0.35) was found; that is, participation in the stability and coordination programme was significantly better than the routine CR programme performed by participants in the control group. It is important to note that the improvement of the intervention group was not maintained in the follow-up test, and yet the results were significantly better than the pre-test. Dos Anjos et al. examined the effect of aerobic exercise on functional strength using FTSST among 43 women over the age of 65 with a type 2 diabetes diagnosis. 33 The participants performed a three-week training programme based on only aerobic exercise (on a treadmill at 65–85% of the heart rate reserve for 40 min) for 12 weeks. Similar to the current study, there was a significant improvement of 1.4 s in the FTSST test. In both studies the results did not meet minimal clinical change, despite their significance.
In general, the improvements found in the current study among the intervention group, in two balance measurements (TUG and BESS) combined with the improvement in functional measurement (FTSST), may imply a decrease in risk of falling.17,20,23,30 As was suggested in a meta-analysis conducted by Whitney et al., 31 the risk of falls among older adults is due to several risk factors (e.g. poor muscular strength, impaired balance and walking performance) that can be addressed by exercise. Improvement of one parameter does not necessarily reduce the risk of falling. 34 However, improvement in both balance parameters as well as muscular leg strength have higher potential to reduce the risk of falling.30,34
Several limitations to the current study should be addressed. First, participants in both groups had different types of CVD, as well as different rehabilitation periods in the CR centre. Consequently, they had different baseline conditions. It is possible that more homogenous characteristics of the participants would have led to more significant differences between groups. Second, the fact that 14 participants dropped out from the study statistically reduced the strength of some of our findings. Attrition occurred due to several reasons, including hospitalization, deterioration in health, and personal issues. In a future study, a larger initial number of participants should be recruited. Third, the risk of falling in the current study was assessed by balance ability tests. It is known that there are additional factors that affect the risk of falling, such as sarcopenia or fear of falling. It is reasonable to assume that participants in the current study did not suffer from sarcopenia, as they all showed normal day-to-day functions; however, it is possible that some of them had fear of falling. Future studies should consider assessing fear of falling using psychological measures that were not used in the current study.
In conclusion, the results of this study indicate that for older adults with CVD undergoing CR, the inclusion of stability and coordination training within the traditional CR programme improves static and dynamic balance as well as functional lower extremity strength, compared to the traditional CR programme. Inclusion of balance and stability training need not exceed the traditional CR programme time frame increasing its applicability. Thus, it is suggested for clinicians in CR centres to consider incorporating stability and coordination training into the traditional CR programme, for a possible contribution to the reduction of the risk of falls.
Supplemental Material
Supplemental_Material – Supplemental material for The effect of a stability and coordination training programme on balance in older adults with cardiovascular disease: a randomised exploratory study
Supplemental material, Supplemental_Material for The effect of a stability and coordination training programme on balance in older adults with cardiovascular disease: a randomised exploratory study by Daria Segev, Devora Hellerstein, Rafi Carasso and Ayelet Dunsky in European Journal of Cardiovascular Nursing
Footnotes
Acknowledgements
The authors would like to thank the Prolife Healthcare Centre, Herzliya, Israel, and in particular Dr Yaron Gershovitz, for permitting the study to be conducted at the CR centre.
Fall prevention for older adults with cardiovascular disease is of high importance. Balance improvement is significant for fall prevention. Cardiac rehabilitation programmes should incorporate stability and coordination.
Declaration of Conflicting Interests
The authors declare that there are no conflicts of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplementary material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.