
Abstract
Background:
Low confidence to exercise is a barrier to engaging in exercise in heart failure patients. Participating in low to moderate intensity exercise, such as the six-minute walk test, may increase exercise confidence.
Aim:
To compare the effects of a six-minute walk test with an educational control condition on exercise confidence in heart failure patients.
Methods:
This was a prospective, quasi-experimental design whereby consecutive adult patients attending an out-patient heart failure clinic completed the Exercise Confidence Scale prior to and following involvement in the six-minute walk test or an educational control condition.
Results:
Using a matched pairs, mixed model design (n=60; 87% male; Mage=58.87±13.16), we identified a significantly greater improvement in Total exercise confidence (F(1,54)=4.63, p=0.036, partial η2=0.079) and Running confidence (F(1,57)=4.21, p=0. 045, partial η2=0.069) following the six-minute walk test compared to the educational control condition. These benefits were also observed after adjustment for age, gender, functional class and depression.
Conclusion:
Heart failure patients who completed a six-minute walk test reported greater improvement in exercise confidence than those who read an educational booklet for 10 min. The findings suggest that the six-minute walk test may be used as a clinical tool to improve exercise confidence. Future research should test these results under randomized conditions and examine whether improvements in exercise confidence translate to greater engagement in exercise behavior.
Introduction
Heart failure (HF) is a debilitating chronic illness associated with adverse physical, psychological, and economic burdens. 1 The European Cardiology Society guidelines recommend a multi-faceted approach for the treatment and management of HF that includes encouraging patients to undertake regular exercise, 2 which has been shown to reduce the risk of HF-related hospitalizations, 3 and improve quality of life. 4 Despite this, adherence to prescribed exercise programs is poor among individuals with HF.5,6 Some of the barriers to exercise include patient fatigue, lack of time and motivation, 7 and, perhaps crucially, low confidence to exercise.8,9
Confidence to exercise, otherwise known as self-efficacy, refers to an individual’s belief in their ability to initiate and maintain regular physical activity. 10 HF patients often report a lack of confidence to exercise, 7 which undermines engagement in, and maintenance of, physical activity. 10 Since exercise avoidance can lead to a cycle of deconditioning, finding ways to promote exercise confidence and physical activity are essential. 10
Participating in physical activities (that is, “learning by doing”) can increase exercise confidence. 10 Multi-session, moderate intensity exercise programs improve physical fitness and exercise confidence in HF patients.11–13 In contrast, single-session, high-intensity exercise, such as the treadmill test, does not appear to promote exercise confidence. 12 However, recent research has shown that completing a single-session, low to moderate intensity exercise task (namely, the six-minute walk test (6MWT)) was associated with improved exercise confidence in HF patients. 14 These findings are aligned with Bandura’s learning theory, suggesting that the intensity of the exercise should challenge, but not overwhelm, the patient to enable a sense of performance mastery and exercise confidence. The aim of this novel study was to confirm and extend these findings through the implementation of a quasi-experimental design which compares the effects of a 6MWT on exercise confidence with an educational control condition. It was hypothesized that HF patients who completed the 6MWT would report greater confidence to exercise than those who read about HF self-care practices.
Methods
Participants and study design
Participants (n=137, 83% male) were prospectively enrolled through a HF outpatient clinic at a major tertiary hospital between February 2016–November 2017, for which the recruitment methods have been described in detail elsewhere. 14 Participants previously recruited to the study and allocated to complete a single 6MWT 14 were matched to a new group of participants allocated to the education control condition. Participant age ranged from 31–89 years old (Mage=62.4±12.87). Inclusion criteria required that patients have a diagnosis of stable HF and included patients with reduced (<40%) and preserved (>40%) left ventricular ejection fraction (LVEF). Exclusion criteria included insufficient English language literacy, significant cognitive or physical impairment, severe osteoarthritis, and significant physical activity impairment (as indexed by a New York Heart Association (NYHA) class IV rating). A quasi-experimental, matched-pairs design was used whereby participants were prospectively allocated to the 6MWT condition (n=106) or an educational control condition (n=31) and retrospectively matched on the basis of age (±5 years), gender, and NYHA (where NYHA I – III indicates the absence, slight, or marked physical activity limitations, respectively) to ensure equal group size. The matched-pairs sample comprised a total of 60 HF patients (87% male; Mage=58.87±13.16).
Measures
Demographic and clinical data
Age, gender, HF etiology, NYHA class, LVEF, current medications, implantation of pacemaker and/or cardioverter defibrillator, and comorbid illness were retrieved from hospital medical records and survey forms.
Exercise Confidence Scale (ECS)
The 18-item ECS assesses perceived confidence to perform a range of physical activities and was adapted with permission. 15 The ECS comprises four subscales (i.e. Walking, Running, Climbing and Lifting), each with three or four items. Participants are asked to report their perceived confidence to perform these physical activities using a confidence index ranging from 0–100 (e.g. confidence to walk 50 m on level ground in one minute; 0=“Quite uncertain”, 50=“Moderately certain” and 100=“Completely certain”). Mean confidence subscale scores were computed as the average across all items within each physical activity subscale. A global score was estimated by averaging across all subscale scores. The ECS has excellent internal consistency 16 and good face validity. 17
Cardiac Depression Scale (CDS)
The 26-item CDS assesses depressive symptomology in cardiac patients. 18 Participants are asked to indicate their level of agreement with each statement on a seven-point Likert-type scale (e.g. “I have dropped many of my interests and activities;” 1=strongly agree, 7=strongly disagree). A total score is estimated by summing items, with higher scores indicating greater depressive symptomology. The CDS has excellent internal consistency (Cronbach’s α=0.90) and a cut-off score of ⩾95 provides 97% sensitivity, and 85% specificity, for the detection of major depression. 19
6MWT
The 6MWT is a self-paced test of sub-maximal, steady-state exercise capacity. 20 Participants are asked to walk up and down a long hallway (usually no more than 30 m) for six minutes at a sustainable pace, with the aim of walking as far as possible during that time. Patients may rest as necessary during the test, but timing continues. The six-minute walk distance (6MWD) is the number of meters walked in total. The 6MWT has excellent test-retest reliability (intra-class correlation=0.97) and is correlated with maximum metabolic equivalents in cardiac rehabilitation populations. 21
Procedure
Ethics approval for the study was granted by the institute’s Human Research Ethics Committee (LNR14Austin329). The investigation conforms with the principles outlined in the Declaration of Helsinki. 22 Participants waiting for their HF outpatient clinic consultation were approached and those interested in participating provided informed consent. All participants completed the CDS and the ECS for baseline index. Participants allocated to the experimental condition then completed the 6MWT under standardized, supervised conditions according to the American Thoracic Society guidelines. 20 Participants allocated to the control condition were asked to read the Living well with chronic heart failure educational booklet for 10 min, which was designed for patients and describes the treatment and management of HF (available for download at http://www.heartonline.org.au/media/DRL/Living_well_with_heart_failure_booklet.pdf). 23 Participants in both conditions then completed the post-intervention ECS within approximately 5–10 min of completing their intervention.
Statistical analyses
Data were analyzed using IBM SPSS Statistics (Version 24). Analysis of variance (ANOVA) and multiple ANOVA (MANOVA) tests were used to detect changes in exercise confidence as a function of group allocation, with bivariate correlations used to identify covariates for analysis of covariance (ANCOVA). Participants with >10% missing data on any given scale were not included in analyses. In this regard, three participants had >10% missing ECS data and one participant had >10% missing CDS data; subscale/total scores were not calculated for these participants. One univariate outlier for body mass index (BMI) was Winsorized. All baseline continuous data were normally distributed (ratio of skewness to the standard error (SE) for skew <2) with the exception of Climbing confidence and Lifting confidence, which were significantly negatively skewed. These variables were improved by square root transformation and used in Pearson’s correlation coefficient analyses, however, the original variables were used in ANOVA/ANCOVA which are robust to deviations from normality. Post-intervention Walking confidence, Climbing confidence, Lifting confidence and Total confidence were significantly negatively skewed. Given the robustness of ANOVA and ANCOVA, untransformed variables were used in these analyses. Post-running confidence was normally distributed. Continuous data are presented as mean±standard deviation unless otherwise specified while categorical data are presented as count percentages (%).
Results
Patient baseline characteristics
Patient baseline demographic, clinical and psychosocial characteristics are displayed in Table 1. Most patients were male (86.7%), with a mean age of approximately 60 years, and were either NYHA class I (56.7%) or class II (40.0%). Thirty per cent of the 6MWT patients and 16.7% of educational control patients were depressed (CDS⩾95). There was no significant difference between the intervention and control group on CDS scores (t (57)=0.78, p=0.437). For those in the 6MWT group, the mean distance walked (6MWD) was 458.93±104.50 m.
Baseline patient characteristics by study condition (n=60).
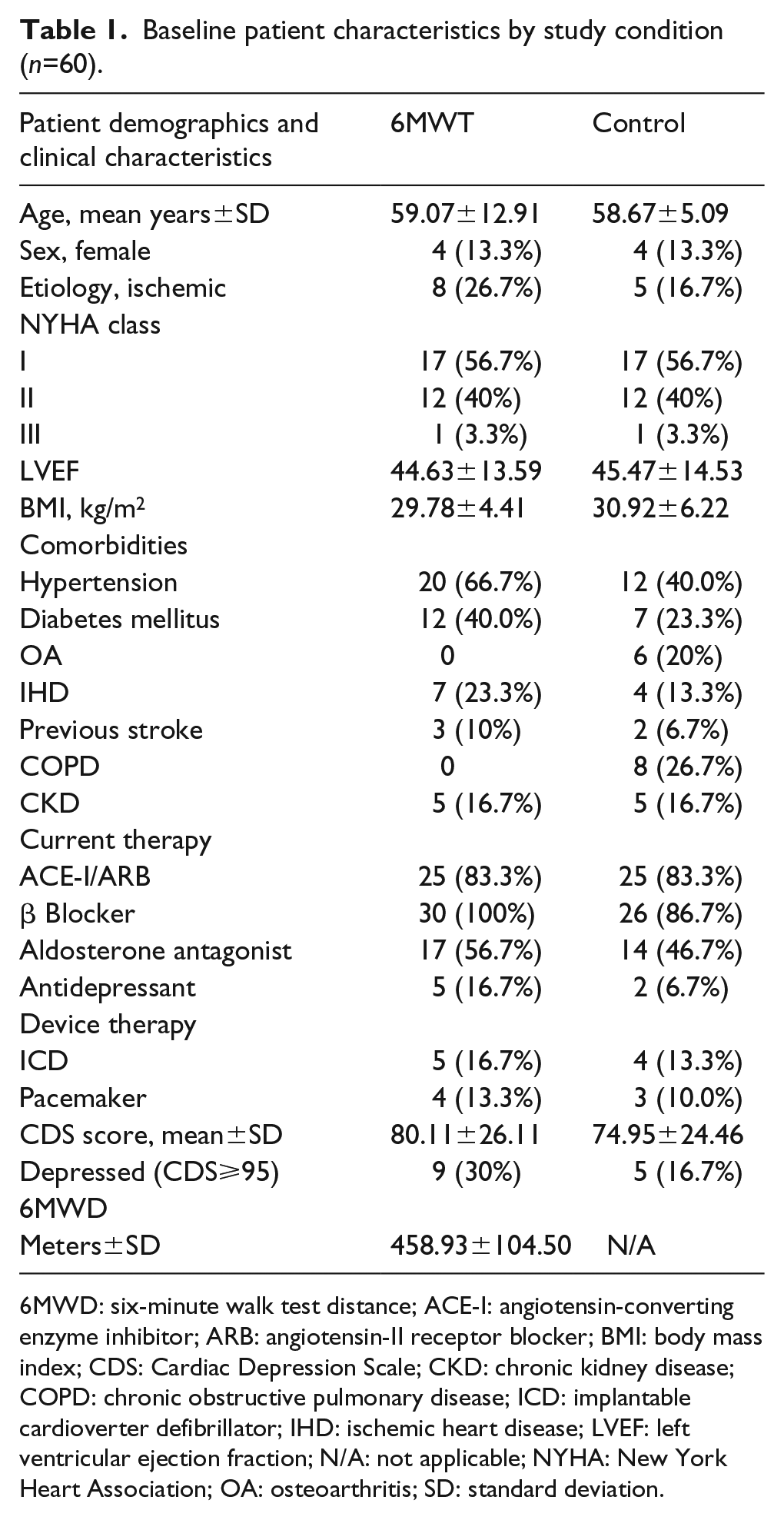
6MWD: six-minute walk test distance; ACE-I: angiotensin-converting enzyme inhibitor; ARB: angiotensin-II receptor blocker; BMI: body mass index; CDS: Cardiac Depression Scale; CKD: chronic kidney disease; COPD: chronic obstructive pulmonary disease; ICD: implantable cardioverter defibrillator; IHD: ischemic heart disease; LVEF: left ventricular ejection fraction; N/A: not applicable; NYHA: New York Heart Association; OA: osteoarthritis; SD: standard deviation.
Baseline exercise confidence: comparisons between treatment groups and across ECS subscales
A between-subjects MANOVA showed that there was no difference between the intervention and control group on baseline Walking, Running, Climbing, Lifting and Total confidence, (Wilks’ Λ=0.85, F(4,52)=2.29, p=0.073), but that baseline confidence across these subscales differed significantly for the sample as a whole, with greater confidence associated with lower intensity exercise (Wilks’ Λ=0.25, F(3,54)=53.03, p<0.001, partial η2=0.747). In this regard, planned contrasts revealed that participants reported significantly higher baseline exercise confidence for walking (73±24, F(1,56)=132.35, p<0.001, partial η2=0.703 ), Climbing (84±21, F(1,56)=127.50, p<0.001, partial η2=0.695) and Lifting objects of graded weight (77±24, F(1,56)=104.55, p<0.001, partial η2=0.651) in comparison to confidence for Running (42±31). Total exercise confidence exceeded the mid-point of the ECS, indicating greater than “moderate certainty” of capacity to complete exercise activities overall (62±21).
Association between baseline exercise confidence and demographic/psychosocial characteristics
Age was inversely associated with Total exercise confidence and each of the exercise confidence subscales (Table 2). Additionally, depression (indexed by CDS score) was inversely associated with Walking, Running, Lifting and Total exercise confidence. BMI was not significantly associated with Total exercise confidence or any subscale of exercise confidence. In comparison to females, males had significantly higher scores for Total exercise confidence (71±20 versus 49±17, p=0.004) and across the exercise confidence sub-scales of Walking (77±21 versus 50±27, p=0.002), Running (46±30 versus 19± 25, p=0.024) and Lifting (81±23 versus 54±17, p=0.002). Participants who were in NYHA class I had significantly higher exercise confidence scores compared with those in classes II and III for Total exercise confidence (78±16 versus 57±21, p<0.001) and across the exercise confidence sub-scales of Walking (81±19 versus 63±25, p=0.002), Running (55±29 versus 26 ±26, p<0.001) and Lifting (85±20 versus 67±26, p=0.004).
Bivariate correlation coefficient for the association between demographic, clinical and psychosocial characteristics, and baseline exercise confidence.
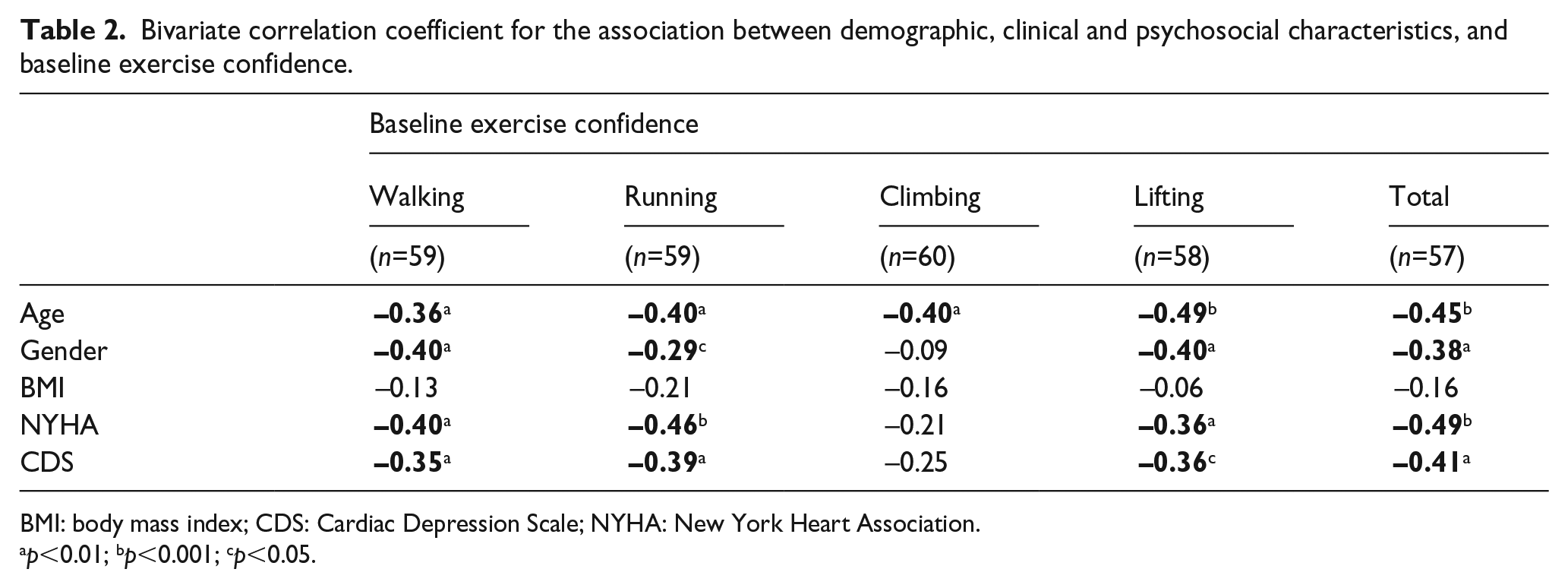
BMI: body mass index; CDS: Cardiac Depression Scale; NYHA: New York Heart Association.
p<0.01; bp<0.001; cp<0.05.
Association between study condition (6MWT or educational control) and exercise confidence
Baseline and post-intervention mean scores for exercise confidence (subscales and total) by study condition are displayed in Table 3. Univariate, mixed-design ANOVA revealed a statistically significant interaction between experimental condition and pre-to-post Total exercise confidence and Running confidence, with those participating in the 6MWT showing greater improvement in Total exercise confidence (F(1,54)=4.63, p=0.036, partial η2=0.079) and Running confidence (F (1,57)=4.21, p=0.045, partial η2=0.069) compared with those in the educational control condition (see Table 4). Similarly, multivariate, mixed-design ANCOVA revealed a significantly greater improvement in Total exercise confidence (F(1,49)=4.93, p=0.031, partial η2=0.091) and Running confidence (F(1,52)=4.24, p=0. 045, partial η2=0.075) for those who completed the 6MWT compared with the control condition, after adjustment for age, gender, NYHA, and CDS (see Table 4).
Descriptive statistics for pre- and post-exercise confidence by study condition.
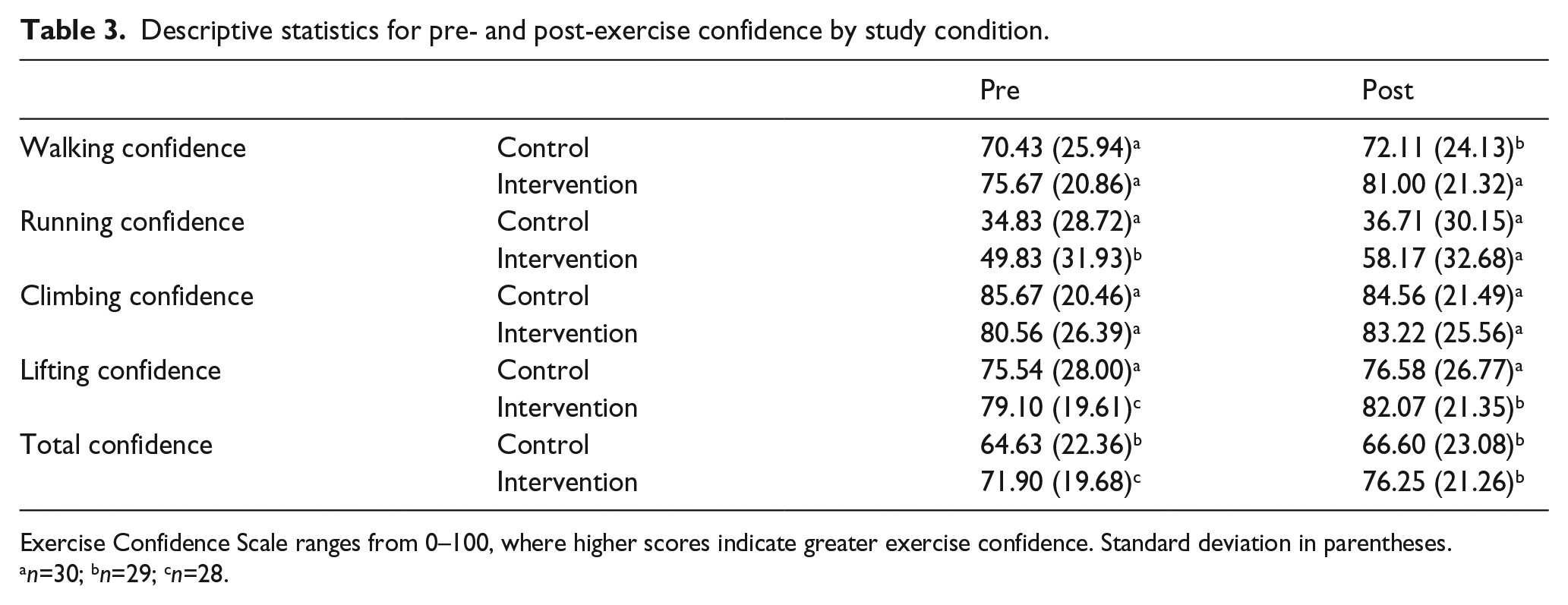
Exercise Confidence Scale ranges from 0–100, where higher scores indicate greater exercise confidence. Standard deviation in parentheses.
n=30; bn=29; cn=28.
Association between condition (six-minute walk test (6MWT) or educational control) and change in exercise confidence.
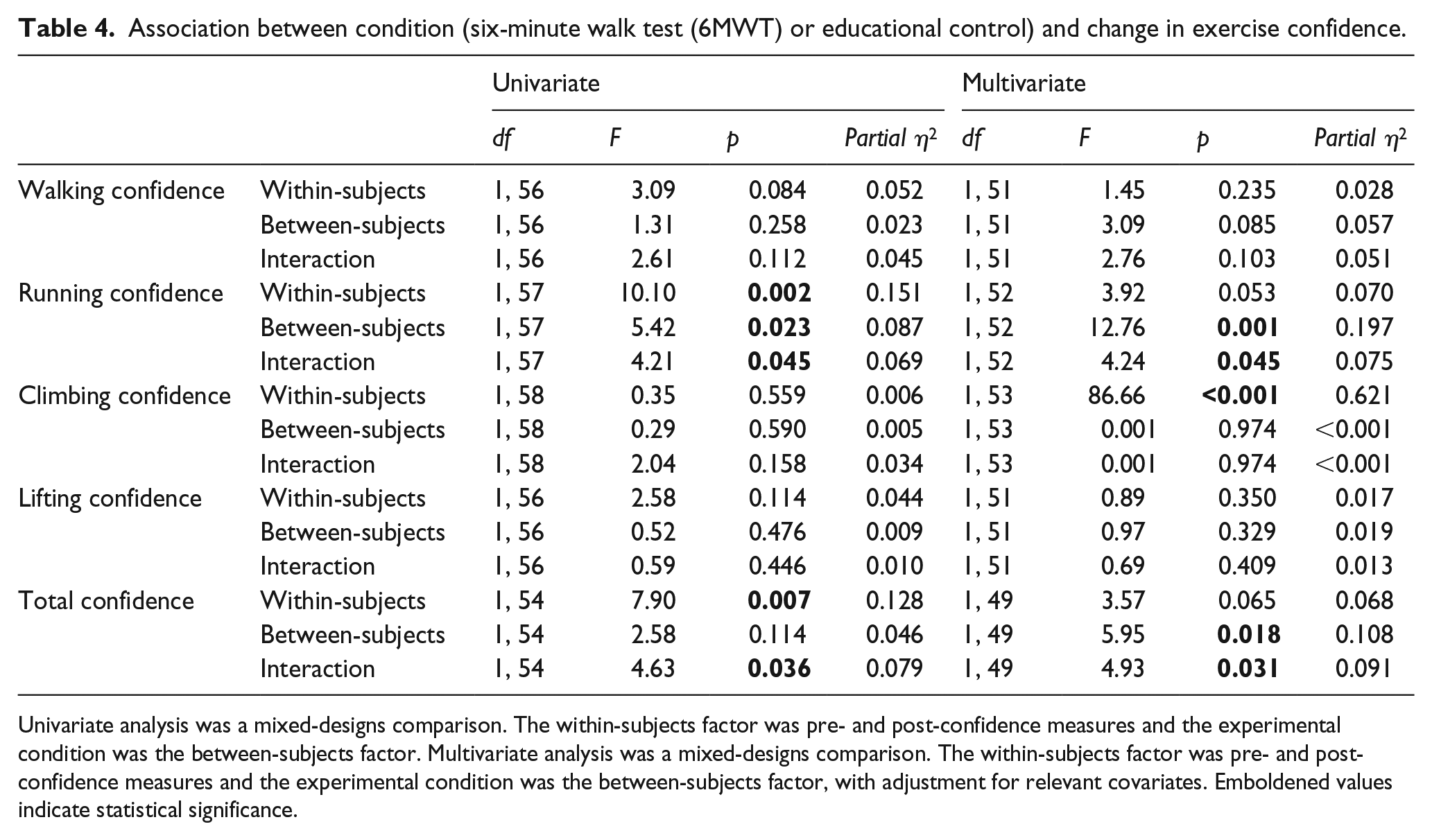
Univariate analysis was a mixed-designs comparison. The within-subjects factor was pre- and post-confidence measures and the experimental condition was the between-subjects factor. Multivariate analysis was a mixed-designs comparison. The within-subjects factor was pre- and post-confidence measures and the experimental condition was the between-subjects factor, with adjustment for relevant covariates. Emboldened values indicate statistical significance.
Discussion
The aim of this study was to compare the effects of the 6MWT with an educational control condition on exercise confidence. As hypothesized, HF patients who completed the 6MWT reported greater improvement in exercise confidence than those who read an educational booklet for 10 min. This was still the case following adjustment for relevant demographic, clinical, and psychosocial characteristics. These findings confirm past research that identified a benefit of the 6MWT on exercise confidence. 14 This is the first time that those benefits have been compared with a control condition, suggesting that the improvements in exercise confidence following the 6MWT cannot be attributed to practice or placebo effects alone.
Improvements in exercise confidence following the 6MWT were not uniform, with benefits observed in Total exercise and Running confidence, but not Walking, Climbing or Lifting confidence. Notably, participants reported significantly higher baseline confidence for Walking, Climbing and Lifting compared with Running confidence, indicating greater opportunity for improvement in the latter. In keeping with Bandura’s proposition that confidence is best enhanced when a task challenges, but does not overwhelm, pre-existing performance perceptions, 17 future research should consider increasing the level of physical capacity assessed in the Walking, Climbing and Lifting subscales. For example, at baseline, 68% of the sample had 100% confidence in their capacity to walk 50 m in one minute; this item could be replaced with a more challenging item in future studies to reduce ceiling effects.
The results confirm that exercise confidence is associated with relevant participant characteristics, such as demographic, clinical, and psychosocial factors. These findings are consistent with those of past research that have identified lower exercise confidence in older, community-dwelling, healthy populations.24,25 Moreover, as reported in Ha et al. 14 the results of the current study confirm lower exercise confidence in women and in those with depression and greater functional limitation. These findings may have important implications for managing aspects of patient self-care in HF, such that patients potentially “at risk” of low exercise confidence may benefit from greater health service support, such as that provided in cardiac rehabilitation programs.
Limitations pertaining to the lack of validation of the ECS as reported in Ha et al. 14 are applicable here. Moreover, as reported above, improvements in some exercise confidence subscales may have been obscured by ceiling levels at baseline. To address these limitations, future research should seek to validate the ECS by exploring a broader array of items ranging from low to high physical demand to increase the sensitivity of the scale. Second, the findings reported here were drawn from a quasi-experimental design, whereby 106 participants were allocated to the treatment condition (i.e. 6MWT), following which a further 31 patients were allocated to the control condition. While there were no differences in baseline demographic, clinical or 6MWT variables between groups, future research should implement a randomized controlled trial to confirm these findings. Moreover, longitudinal designs could be employed to examine the durability of the association between the 6MWT and exercise confidence and how it may translate into actual exercise behavior in the long-term.
Conclusions
HF patients who completed the 6MWT reported significantly greater improvement in exercise confidence than those who read an educational booklet for 10 min, providing preliminary evidence of a causal effect. The current study provides evidence that the 6MWT can extend beyond its original role as a test of functional capacity and act as a clinical tool to improve exercise confidence. Future research should test these results under randomized conditions and examine whether improvements in exercise confidence translate to greater engagement in exercise behavior.
Footnotes
Acknowledgements
The authors would like to thank all the staff and volunteers at the heart failure outpatient clinic who assisted with patient recruitment and data collection.
Declaration of conflicting interests
The authors declare that there are no conflicts of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Exercise confidence is inversely associated with age, functional limitation, and depression. Exercise confidence is higher in low intensity activities in heart failure patients. The six-minute walk test (6MWT) improves exercise confidence in heart failure patients. Heart failure patients (New York Heart Association (NYHA) class I–II) should complete a 6MWT as a component of usual cardiac care. The 6MWT can be used as a test of functional capacity and as a clinical tool to improve exercise confidence in heart failure patients (NYHA class I–II).