
Abstract
Background:
Symptom perception in heart failure has been identified as crucial for effective self-care that is a modifiable factor related to decreased hospital readmission and improved survival.
Aims:
To review systematically the heart failure symptom perception literature and synthesise knowledge on definition, description, factors and instruments.
Methods:
We conducted a scoping review including studies reporting patient-reported symptom perception in adults with heart failure. Structured searches were conducted in Medline, PubMed, Embase, CINAHL, PsychINFO, Web of Science, Cochrane, JBI and grey literature. Two authors independently reviewed references for eligibility. Data were charted in tables and results narratively summarised.
Results:
The search yielded 3057 references, of which 106 were included. The definition of heart failure symptom perception comprised body listening, monitoring signs, recognising, interpreting and labelling symptoms, and furthermore awareness of and assigning meaning to the change. Symptom monitoring, recognition and interpretation were identified as challenging. Symptom perception facilitators include prior heart failure hospitalisation, heart failure self-care maintenance, symptom perception confidence, illness uncertainty and social support. Barriers include knowledge deficits, symptom clusters and lack of tools/materials. Factors with inconsistent impact on symptom perception include age, sex, education, experiences of living with heart failure, comorbidities, cognitive impairment, depression and symptom progression. One instrument measuring all dimensions of heart failure symptom perception was identified.
Conclusion:
Heart failure symptom perception definition and description have been elucidated. Several factors facilitating or hampering symptom perception are known. Further research is needed to determine a risk profile for poor symptom perception – which can then be taken into consideration when supporting heart failure self-care.
Introduction
Symptom perception is a necessary antecedent of self-care management and has emerged as essential for effective heart failure (HF) self-care (i.e. patient activities to maintaining physiological stability, perceiving and responding to symptoms). 1 Symptom perception has been described as involving body listening, monitoring signs to detect physical sensations and recognising, interpreting and labelling symptoms. 1 Symptom perception is challenging for patients with HF,2, 3 and failure to detect or interpret symptoms appropriately can result in inappropriate3, 4 or delayed responses (e.g. seeking care), 4 and prolonged hospitalisation. 5 In contrast, symptom recognition combined with appropriate responses decrease emergency room visits, HF hospitalisation and all-cause mortality. 6 Self-care in HF remains suboptimal worldwide. 7 Symptom perception needs to be operationalised. Understanding the factors influencing symptom perception may help identify patients at risk of poor symptom perception and develop tailored strategies for improving symptom perception. Reviewing the available instruments for assessing symptom perception may help in measuring this construct.
HF self-care theory,1, 8 modifying factors9–11 and instruments measuring HF self-care12–15 have been summarised. However, an overview focusing specifically on symptom perception is missing as the literature is embedded in the larger body of work on self-care. Two integrative reviews16, 17 have synthesised the literature on symptom recognition, interpretation and response.16, 17 These reviews identify some factors associated with symptom recognition, 17 yet gaps remain regarding symptom perception definition, modifying factors and instruments measuring this construct.
This study aims to operationalise symptom perception by examining the scope of work on HF symptom perception relating to four research questions:
How has HF symptom perception been defined?
How has HF symptom perception been described?
What factors are associated with HF symptom perception?
What instruments have been used to measure HF symptom perception?
Methods
We conducted a scoping review and followed standard reporting guidelines for scoping reviews. 18 The sequential process included identifying the research question, identifying and selecting relevant studies, data charting and comprehensively summarising results. 19 The protocol is available on request from the corresponding author. Studies of symptom perception in adults living with HF were considered for inclusion along with expert opinion and position papers. Article eligibility criteria are detailed in Table 1.
Eligibility criteria applied to the scoping review.
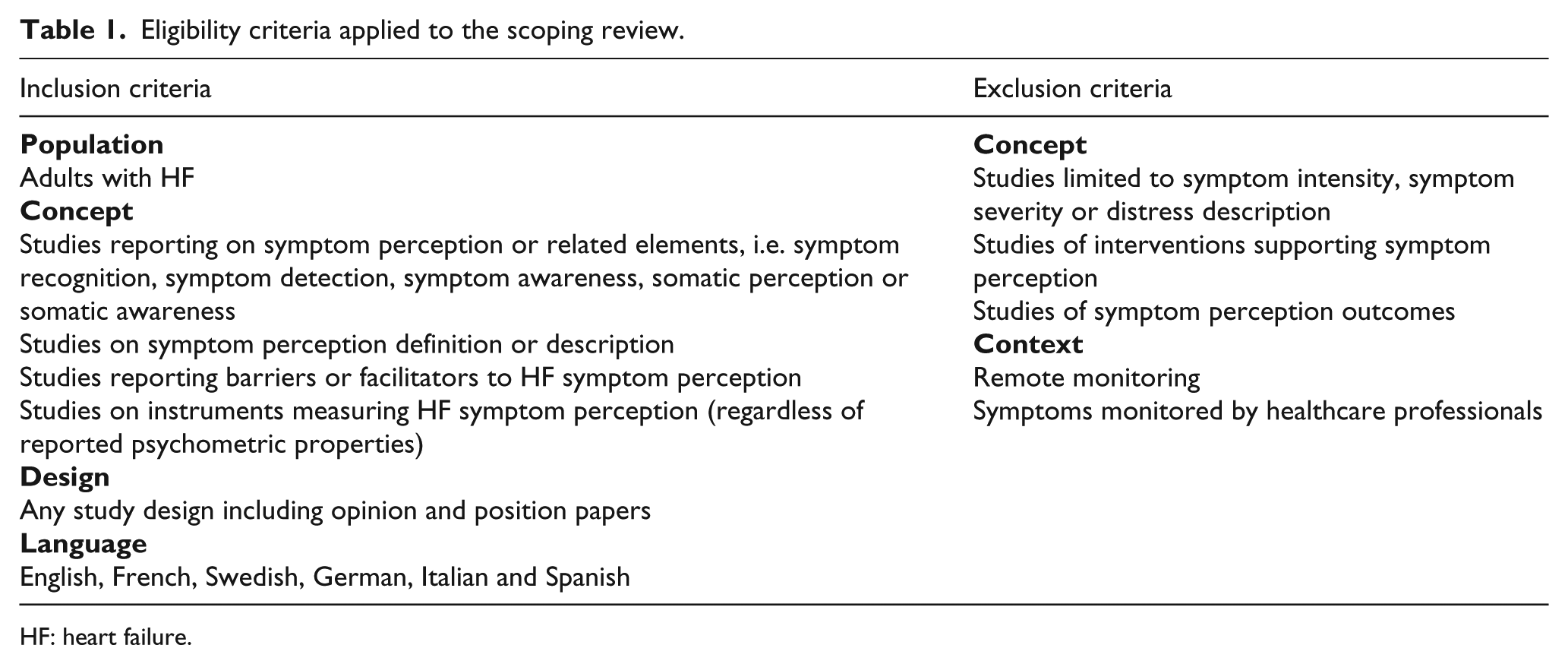
HF: heart failure.
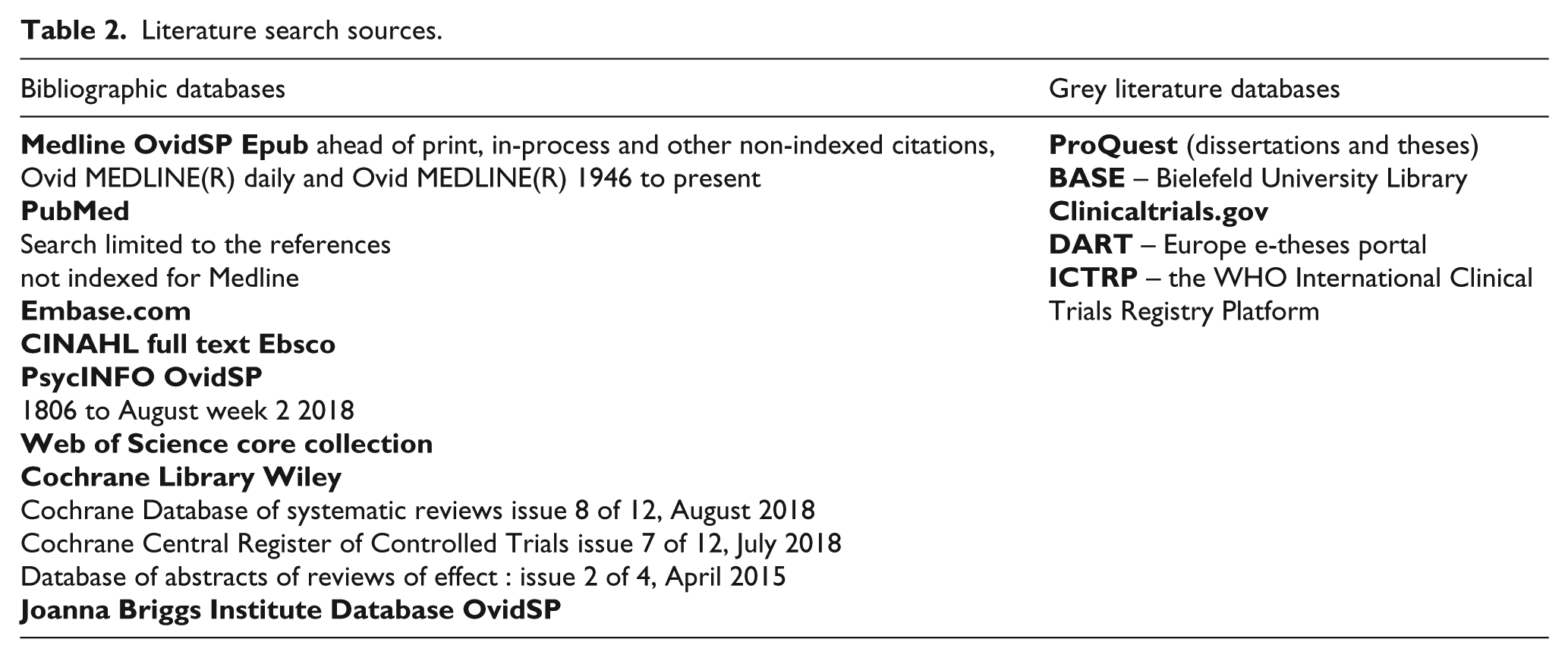
Literature searches were developed with a medical librarian (CJ). An initial limited search was conducted in Medline OvidSP. Relevant articles were identified (GCS) and discussed with the second reviewer (ML). Subsequently, keywords and index terms of the retrieved papers were analysed and finalised for a full search in eight bibliographic databases and five unpublished grey literature databases in October 2017 (Table 2). Full descriptions including keywords and search strategies are provided in the Supplementary files. The search was actualised on 21 August 2018 in the seven major bibliographic databases (Medline, PubMed, Embase, CINAHL, PsychINFO, Web of Science, Cochrane). During article review and data charting, additional articles were identified in the reference lists of retrieved articles and included in the review process. Authors were contacted to obtain full text articles as needed.
Literature search sources.
References were imported into citation management software (Endnote X7.7.1, Clarivate Analytics) and duplicates were removed. Two reviewers (GCS, ML) independently reviewed titles and abstracts of retrieved references and determined eligibility per inclusion/exclusion criteria without conducting a quality appraisal. Selected references underwent full text review to determine final inclusion. Web-based software (Rayyan), 20 was employed to document and track the study selection process. Both reviewers independently labelled each included reference according to the related research question(s). Data were extracted using structured forms for each research question (see categories used for data extraction in the Supplementary files). Articles were randomly assigned to three independent reviewers (GCS, ML, JG) for charting the data. Data charting quality was assessed by dual extraction and charting. In total, 10% of manuscripts underwent parallel data extraction by independent reviewers. Examination revealed that data extracted in parallel were comparable for all the references. Data on each research question were summarised narratively by GCS and results were discussed with both reviewers and PSK. Disagreements were resolved through discussion during monthly meetings throughout the review and extraction process.
Results
Following removal of duplicates, 3057 references were identified and screened by title and abstract. After initial review, 2544 references were excluded per inclusion/exclusion criteria. The remaining 513 references underwent full text review and 106 references were included for data extraction and charting. Reasons for excluding the 407 references are reported in the Prisma flow diagram (Figure 1). 18
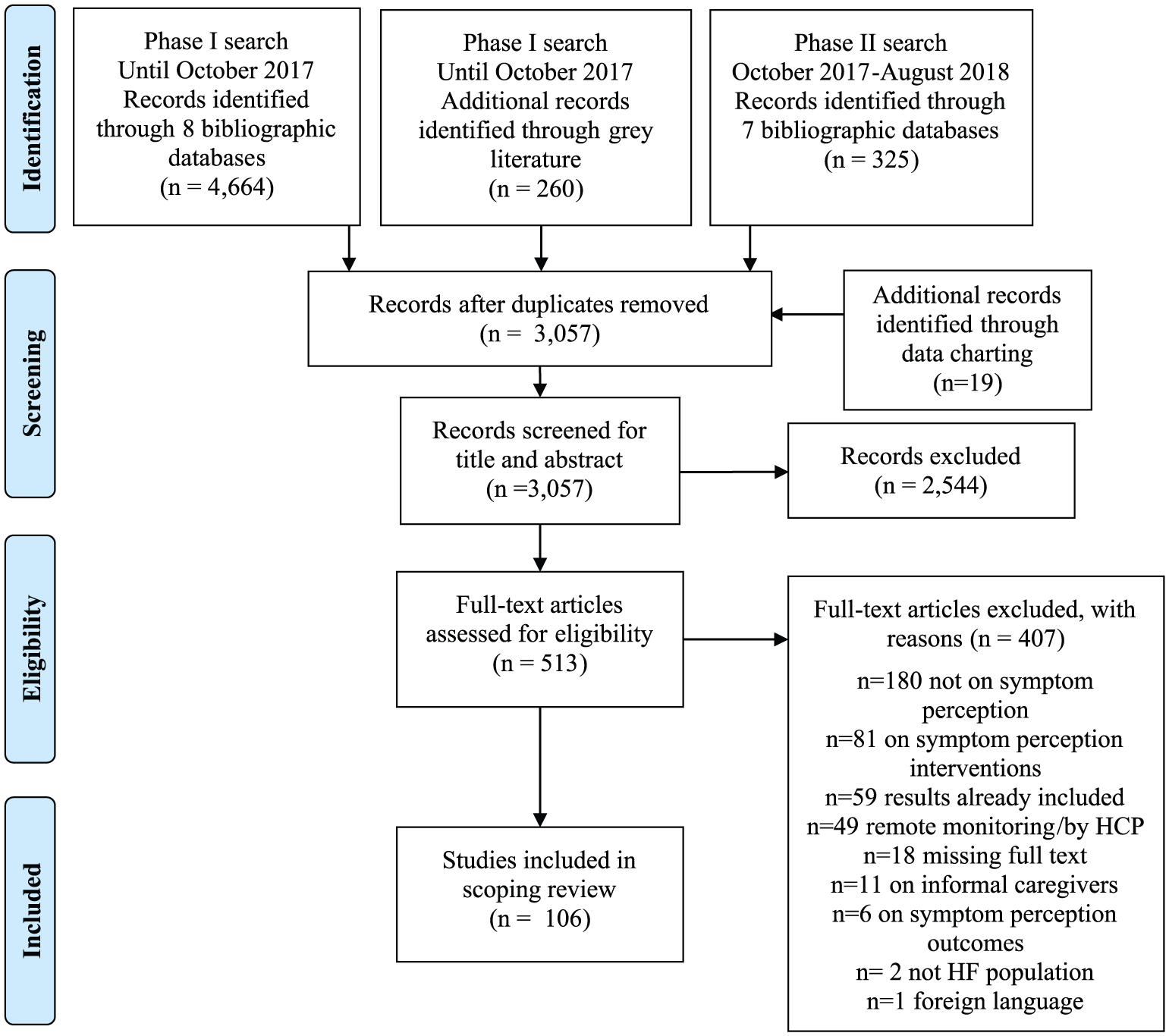
Prisma flow diagram 18 of study selection process.
Manuscript types included 46 observational studies,2, 7, 14, 21–63 27 qualitative studies,4, 64–89 12 literature reviews,16, 17, 90–99 eight mixed-methods studies,3, 13, 100–105 six manuscripts without a reported study design,106–111 two pilot studies,112, 113 two theories,1, 8 one quasi-experimental study, 114 one conceptual framework 10 and one case study. 115 Some of the 106 references related to more than one of the research questions. Twelve included references related to HF symptom perception definition,1, 8, 17, 27, 34, 43, 54, 75, 80, 100, 102, 106 68 to description,2–4, 7, 10, 16, 17, 21–42, 49, 64–74, 76–79, 81–87, 89–98, 100–102, 107, 108, 115 41 to factors1, 3, 10, 16, 17, 21, 22, 24, 26–29, 36, 37, 39, 44–48, 50, 66, 73–75, 88, 89, 93, 95, 96, 98, 99, 102–105, 107–111 and 23 to instruments.3, 13, 14, 32, 39, 44, 50-63, 112–114 An overview of symptom perception definition, description, factors and instruments is shown in Figure 2.
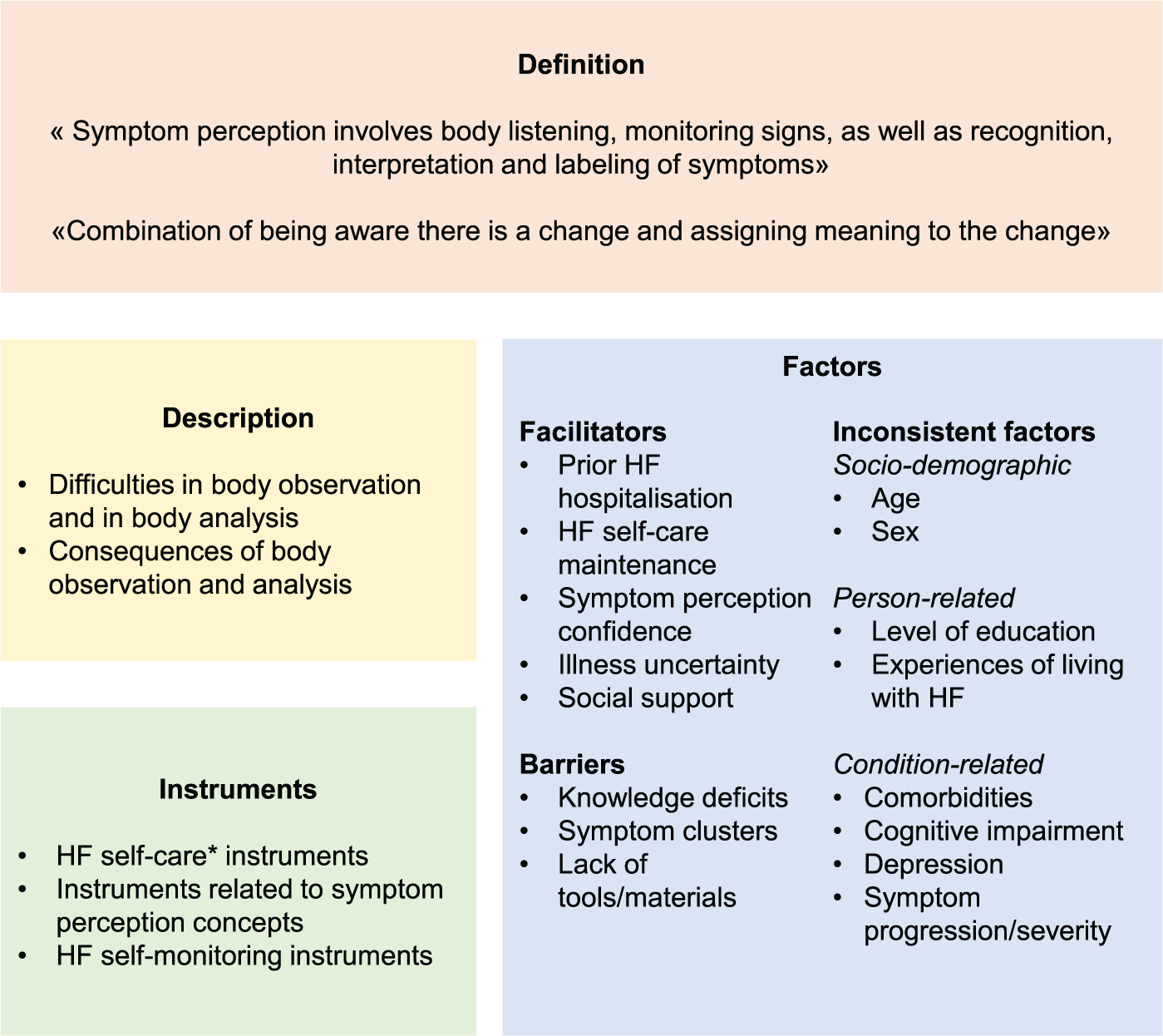
Heart failure (HF) symptom perception definition, description, factors and instruments.
HF symptom perception definition
Several definitions of HF symptom perception are reported in the literature. The situation-specific theory of HF self-care 1 and related publications17, 102 defined symptom perception as ‘. . .body listening, monitoring signs, as well as recognition, interpretation, and labeling of symptoms’.1(p. 227) This definition was supported by moderate relationships between symptom monitoring and symptom recognition and evaluation (r=0.34, P<0.01). 43 Another definition of symptom perception was: ‘. . .a combination of being aware there is a change and assigning meaning to the change’.80(p. 93) One may consider HF symptom perception is defined by body observation and body analysis. Body observation includes body listening and monitoring HF signs/symptoms (i.e. a behavioural process) while body analysis relates to recognising, interpreting and labelling symptoms – as well as assigning meaning (i.e. a cognitive process). Next, we identified several concepts including symptom perception elements. Awareness, interpretation and measurement composed self-care monitoring; 54 body listening and coherence related to symptom recognition; 100 sensitivity to physical sensations and bodily activity secondary to physiological change 27 related to somatic awareness while symptom recognition and interpretation of its severity composed situation awareness. 75
Difficulties in body observation and body analysis and consequences
Most studies report that body observation is not systematic in patients with HF.4, 10, 17, 24, 25, 28, 29, 39, 41, 66, 67, 70, 83, 90, 96, 98 Only a minority of patients monitor symptoms regularly24, 64, 80 and considered symptom monitoring to be important 86 for controlling HF.64, 74, 78 In a large study, 16 of 22 studies (from 15 countries) reported irregular weight monitoring in more than half of patients. 7 Physical and/or cognitive difficulties were reported in monitoring/recording weight without assistance. 82 Furthermore, adherence to symptom monitoring was difficult2, 73, 92 and challenges include insufficient knowledge of HF signs/symptoms,42, 93, 100 poor oedema assessment skills,17, 39 forgetfulness,39, 49 worry about HF,39, 49 lack of time 49 and lack of trust in health professionals’ expertise and support. 93 Some patients did not recall having monitored their symptoms during the period preceding a HF exacerbation 80 and most patients experiencing weight gain did not report changes. 22
Body analysis following body observation is often poor because patients have difficulty recognising signs and symptoms related to chronic HF4, 21, 31, 33, 36, 66, 67, 74, 81, 83, 93, 98, 101, 107 as well as signs of decompensation.17, 23, 34–36, 42, 65 Patients have difficulty quantifying subtle changes in dyspnoea 108 and noting changes in symptom status.10, 26, 32, 97 In fact, objective and subjective reports of thoracic fluid retention (i.e. pleural fluid accumulation measured through intrathoracic impedance-derived fluid index vs. daily reported signs and symptoms) is discordant in 44% of cases. 102 Cumulatively, these factors contribute to inaccurate interpretation of symptoms.17, 71, 73, 74, 76, 80, 93, 102 Body analysing made patients uncertain, 89 as some patients find it challenging to determine whether a symptom is clinically meaningful 100 – particularly for vague or non-specific symptoms. 87 Patients are often uncertain in situations when symptoms require interpretation 30 when clinical status deteriorates warranting medical attention.34, 72, 80, 90 Moreover, discrimination of HF symptoms from symptoms related to other comorbidities remains a challenge66, 79, 92–94, 102 and many patients inaccurately attribute their symptoms to something other than HF23, 81, 85 such as age,16, 27, 31, 84, 89, 91, 96, 107 comorbidities,4, 27, 31, 37, 38, 79, 93 medication,76, 91, 93 stress, 102 fatigue 38 or the weather. 102
Response to body observation and body analysis varies. Some responses are more active in nature and may include resting, relaxing or changing their daily routine.25, 31, 38, 80, 82 Other responses are more avoidant in nature such as ignoring symptoms68, 74, 81 or adopting a ‘wait and see’ strategy 102 in hopes that symptoms will resolve spontaneously.3, 4, 72, 81 These strategies can delay help-seeking,38, 97 or patients may only seek medical support if symptoms do not resolve, 82 or symptoms escalate interfering with daily life activities, 27 or become unmanageable,76, 80 leading to emergency situations67, 79, 115 and hospitalisation. 107 Only some patients seek medical attention to understand or interpret the significance of symptoms 70 and learned about it when seeking care. 77
Factors impacting symptom perception
Facilitators
Identified facilitators of HF symptom perception include prior HF hospitalisation, HF self-care maintenance, symptom perception confidence, uncertainty about the meaning of illness-related events and social support. Somatic perception improved with the overall number of hospital admissions (r=0.42, P<0.001) as well as cardiac-related admissions within the past 6 months (r=0.36, P=0.002). 17 Symptom monitoring and treatment-seeking were poorer in patients without prior HF hospitalisations (sβ=−0.21, P=0.02). 29 Self-care maintenance and symptom perception confidence has been shown to help explain variability in symptom perception. 46 The frequency of symptom monitoring predicts symptom monitoring at one month follow-up (odds ratio (OR) 9.18, 95% confidence interval (CI) 2.15–39.3). 24 Furthermore, patients with higher illness uncertainty were shown to pay more attention to somatic changes (r=0.36, P<0.01).17, 27 In addition, social support was reported to improve symptom perception as patients living with others are more likely to report dyspnoea 45 and are able to recognise changes in signs and symptoms better compared to patients living alone (P=0.014).17, 36 Informal caregivers may also assist with weight monitoring and symptom recognition. 88
Barriers
Identified barriers of HF symptom perception are knowledge deficits as well as symptom clusters and lack of tools/materials. Insufficient HF knowledge is associated with poor symptom monitoring and treatment-seeking (P=0.028). 29 Symptom clusters refers to the experience of several concurrent symptoms, 116 and such clusters may complicate symptom perception. 1 Lack of tools/materials (e.g. patients without scale for weight monitoring) 28 poses additional barriers to symptom perception.
Factors with inconsistent impact on HF symptom perception
Age, sex, level of education, patient experiences of living with HF, comorbidities, cognitive impairment, depression as well as symptom progression/severity are inconsistently associated with HF symptom perception.
Sociodemographic factors
Results are inconsistent with regard to the relationship between older age and symptom perception. Several studies have demonstrated that older patients experience more difficulty in symptom perception.10, 16, 27, 46, 66, 96, 98, 104, 107 Some reported that older patients are challenged to discriminate HF from age-related changes.89, 95, 98 Furthermore, older persons perceive lower symptom severity, 50 are less likely to detect, interpret 104 or report dyspnoea. 45 However, younger patients appear less able to detect changes in thoracic fluid. 102 Similarly, there is no clear association between age and either somatic awareness, 17 body awareness,44, 95 monitoring activities24, 29, 39, 66 or symptom recognition. 36 There is no consensus on age as a determinant of symptom perception.24, 29, 46
With regard to the role of sex on symptom perception, one study found better HF symptom interpretation in men compared to women. 105 However, other studies failed to identify sex differences in body awareness,44, 95 symptom awareness, 110 sign/symptom change recognition, 36 attribution of symptoms,37, 48 symptom monitoring and treatment-seeking, 29 or in detecting changes in thoracic fluid levels. 102 Furthermore, sex did not predict symptom monitoring. 24
Person-related factors
Data on the impact of educational level are inconsistent. One study has found that education did not predict symptom monitoring 24 while others suggest that higher educational levels facilitate symptom recognition.17, 36
Patient experiences of living with HF have been proposed to affect symptom perception. Longer disease duration was associated with increased somatic perception, 103 symptom recognition 21 – as experience may facilitate symptom interpretation. 10 Also, prior personal experience with the situation and situation awareness seem to influence mental simulation. 75 Another study failed to identify a relationship between HF duration and thoracic fluid detection. 102
Condition-related factors
Comorbidities may reduce patients’ ability to identify HF symptoms.3, 74, 107, 111 Sensory problems (e.g. hearing loss, 99 impaired vision)10, 99 and disturbed body balance 10 hamper symptom monitoring and recognition. Fatigue and sleepiness, may negatively affect symptom monitoring, 10 recognition and interpretation.37, 75 Again, one study failed to identify an association between comorbidities and perception of thoracic fluid accumulation. 102
Regarding cognitive impairment, some studies indicate cognitive impairment results in poor symptom recognition and interpretation.1, 10, 98, 99, 109–111 In contrast, some studies report no relationship between cognition and either symptom monitoring, 22 thoracic fluid detection 102 or symptom recognition. 26
Regarding depression, compared to HF patients without depressive symptoms, patients with depression are less likely to monitor body weight (P=0.041). 47 Depression also appears to hamper symptom recognition,75, 111 while mania, alexithymia and psychotic illness may diminish symptom perception. 108 However, other studies have found no relationship between depression and either body awareness 44 or thoracic fluid detection. 102 Moreover, others reported contrasting results, with anxiety and depression associated with even increased symptom perception, 108 likelihood to report dyspnoea 45 and symptom recognition. 110
For symptom progression/severity, some authors have reported that slowly progressing symptom severity impairs somatic awareness 17 and symptom recognition.3, 17, 73, 107 Study results based on functional performance data (i.e. New York Heart Association (NYHA) class), however, have been heterogeneous. Several studies report that worse functional ability (higher NYHA class) is associated with increased somatic perception 17 and symptom recognition, 36 yet others report no association with symptom monitoring, 24 decreased symptom recognition 48 and no difference in thoracic fluid detection. 102
In summary, while a substantial number of factors have been identified in relation to symptom perception (Table 3), the key drivers of symptom perception have yet to be determined.
References relating to symptom perception factors.
Table 3 provides a summary of the study characteristics of all articles included reporting on factors related to symptom perception.
HF: heart failure; LVEF: left ventricular ejection fraction; NYHA: New York Heart Association classification; OR: odds ratio; RCT: randomised controlled trial; v: version.
HF symptom perception instruments
HF symptom perception instruments intend to measure one or several dimensions of HF symptom perception (Table 4). Several instruments used for HF self-care assessment contain items related to symptom perception dimensions.13, 14, 51, 53, 59, 60 The 39-item self-care of heart failure index v.7.2 contains the 11-item symptom perception subscale dedicated to HF symptom perception. This subscale aligns with the self-care situation-specific theory definition of symptom perception 51 and covers all dimensions of the HF symptom perception definition. It comprises nine items on monitoring behaviours and two symptom recognition items, and has demonstrated adequate construct validity using a two-factor model (CFI 0.96, RMSEA 0.050, 90% CI 0.039–0.062) and good internal consistency (multidimensional scale global reliability index 0.85). 51
HF symptom perception instruments and related symptom perception dimensions.
Other instruments relate to concepts of symptom perception. The HF somatic awareness scale 55 and the HF somatic perception scale56, 58 measure patient awareness of signs and symptoms and perceived symptom severity. The body awareness questionnaire includes a scale on body attentiveness that has been tested in patients with HF. 44 The revised HF compliance scale includes an item on daily weighing. 39 The self-evaluation of symptoms, signs and compliance to therapy for HF surveillance identifies worsening HF symptoms and discriminates between chronic and acute volume overload. 32 The modified response to symptoms questionnaire contains items related to the cognitive response to symptoms. 3 The dyspnoea visual analogue scale uses a 100 mm visual analogue scale to quantify perceived dyspnoea severity. In the latter, meaningful changes (i.e. a little less or a little more difficulty) correspond to 21.1 mm (95% CI 12.3–29.9 mm). 63
Nine HF self-monitoring instruments were found.50, 52, 54, 57, 61, 62, 112–114 The evaluation scale for self-monitoring by patients with chronic HF measures self-monitoring. 54 The heart health diary was developed to monitor common signs and symptoms of HF (i.e. weight, blood pressure, pulse, blood sugar, fatigue, shortness of breath, cough, oedema and chest pain). 114 We identified several mobile health applications:52, 62, 113 HeartMapp can be used to monitor weight and vital signs, 52 the HF symptom-tracker mobile application was designed to monitor weight and symptoms and was tested for acceptability in patients older than 60 years of age, 62 another smartphone application for self-monitoring and interpreting HF signs and symptoms has acceptable usability scored in 75-year-old and older adults with HF. 113 Other instruments focusing on specific HF signs and symptoms are the fluid overload symptoms scale, 50 weight management scale 61 and HF monitoring instruments 112 to facilitate HF symptom recognition and reporting of dyspnoea and weight gain to providers. The HF symptom tracker (HFaST) supports ongoing evaluation of symptom changes over the previous 24 hours compared to usual patient experiences. 57
Discussion
This scoping review maps the literature on HF symptom perception to report on definition, description, related factors and instruments, and updates the state of the science provided in previous reviews. Importantly, HF symptoms often undetected by patients lead to negative health sequelae. 16
In line with previous reviews, this scoping review highlights facilitators of HF symptom perception including more prior HF hospitalisation, higher levels of illness uncertainty and living with others. 17 We report further that both self-care maintenance and symptom perception confidence facilitate symptom perception, while symptom clusters represent a barrier to accurate symptom perception. Importantly, this scoping review identified sociodemographic, person-related and condition-related factors with inconsistent findings across studies with regard to their impact on symptom perception. Younger age, 46 higher education, 17 longer duration of HF, 46 shorter symptom duration, 17 worse functional class 17 were previously reported as facilitators; aging, 17 comorbid conditions, 17 gradual symptom progression 17 were previously reported as barriers. The greater number of references included in this scoping review and the different dimensions of HF symptom perception considered may have allowed these findings.
This review reports on several studies that did not identify a relationship between sociodemographic factors (i.e. age and sex) and HF symptom perception.36, 44 Several studies on the relationship between age and symptom perception are reported with conflicting results. Concerning sex, only one study reported men to be better than women in symptom interpretation, 105 while five studies24, 29, 36, 44, 48 – all with larger sample sizes – report no relationship between sex and symptom perception. Also, person-related factors such as education were not found to be related to symptom perception. 24 Patient experiences of living with HF seem to facilitate symptom perception,21, 46, 103 but one study found no relationship between HF duration and thoracic fluid detection. 102 Yet we know that congestion is not readily detected by patients. 117 Similarly, condition-related factors such as comorbidities and cognition were not reported to be associated with patients’ detection of thoracic fluid accumulation. 102 With regard to comorbidities, sensory problems and fatigue/sleepiness that are plausible barriers to symptom perception negatively affect symptom perception.10, 75 None of the primary studies included in our scoping review22, 26, 102 found any relationship between cognitive impairment and symptom perception. Further research should elucidate the role of depression as well as symptom progression/severity in symptom perception. Overall, further research is needed regarding the impact of sociodemographic, person-related and condition-related factors on symptom perception to determine a patient risk profile.
Several facilitators and barriers of HF symptom perception converge with the broader literature on HF self-care 9 as well as factors relating to self-care in chronic conditions. 118 In line with findings of this scoping review, confidence and social support have been reported to facilitate HF self-care 9 and self-care in other chronic conditions. 118 Habits integrated into daily routines are important for self-care 118 – that may relate to HF self-care maintenance thereby facilitating symptom perception (e.g. weighing oneself regularly). Experience and skills, as well as functional and cognitive abilities, influence HF self-care 9 and self-care in chronic illness more broadly. 118 In the present review, prior HF hospitalisation facilitates symptom perception. Furthermore, greater experience of living with HF, as well as cognitive impairment, are inconsistent factors of symptom perception – which contrasts with the broader literature. 118 Nevertheless, disparate results across studies on symptom perception factors neither provide insight into experience nor cognitive abilities as a potential facilitator of symptom perception.
Overall, we identified one instrument 51 measuring all dimensions of HF symptom perception, yet further psychometric testing in other HF patient samples and additional languages seem warranted.
For other chronic conditions, these results may contribute to address current research gaps related to self-care monitoring, 119 describing symptom perception challenges and related behaviours. As in other chronic conditions, 120 HF symptom perception is related to emotional distress which may guide symptom response. 80 Symptom response is challenging in other chronic conditions such as atrial fibrillation 121 and stroke. 122 Some have postulated that difficulty interpreting non-specific symptoms results in delays in seeking care.121, 122 Definitions of HF symptom perception converge on the concepts of detecting and interpreting symptoms in chronic conditions. 119
Limitations of this scoping review include the lack of a structured quality appraisal of included articles, which is appropriate for scoping reviews. 19 A quality appraisal could be useful for supporting interpretation of data in further reviews. Also, we did not consider studies reporting on symptom intensity, severity or descriptions of distress relevant to be included as they do not directly relate to symptom perception within the HF self-care process.
Relative strengths of this review include the systematic searching process that included unpublished (grey) literature thus minimising publication bias. Including grey literature as well as conference abstracts allowed us to identify articles not yet published in August 2018 which we tracked for inclusion in this report. In particular, the first author (GCS) reran the search in August 2019 in the three major bibliographic databases (i.e. Medline, Embase, Web of Science) yielding the majority of the references included in the initial search. After screening the new references published in 2018 and 2019, five additional references123–127 were identified. Importantly, the five additional references were not deemed to alter significantly the overall synthesis findings of the scoping review and are not included in this review as the screening deviated slightly from the structured systematic search process. Furthermore, references in multiple languages were included providing a comprehensive, broad and culturally inclusive perspective. References were screened and selected by independent reviewers and data charting as well as results reporting followed a structured, systematic way – helping to ensured internal validity.
Symptom perception in HF is established, has been described and well defined. Several symptom perception factors are known, and further work is needed to dissect the relative effect of factors and elucidate inconsistent results related to the facilitators and barriers to HF symptom perception. This will be important to determining patient risk profiles related to poor symptom perception. In addition, further work is needed on symptom perception measurement in HF for both research and clinical use. Deepening our understanding of symptom perception, its factors and measurement will be important for strengthening person-centered self-care support in HF and reducing negative health sequelae resulting from unravelled limitations to symptom perception.
Supplemental Material
Supplemental_material – Supplemental material for Symptom perception in heart failure: a scoping review on definition, factors and instruments
Supplemental material, Supplemental_material for Symptom perception in heart failure: a scoping review on definition, factors and instruments by Gabrielle Cécile Santos, Maria Liljeroos, Andrew A Dwyer, Cécile Jaques, Josepha Girard, Anna Strömberg, Roger Hullin and Petra Schäfer-Keller in European Journal of Cardiovascular Nursing
Footnotes
Acknowledgements
The authors would like to acknowledge Dr François Mooser for his support with administrative issues along the study and related to the submission of this work. GCS is grateful for expert feedback received during presentations of this work during doctoral seminars at the Institute of Higher Education and Research in Healthcare (IUFRS), University of Lausanne and during Swiss PhD in nursing science education (SPINE) doctoral days as well as during research seminars at the University of Applied Sciences and Arts Western Switzerland (HES-SO) School of Health Sciences, Fribourg.
Heart failure symptom monitoring, recognising and interpreting is challenging for persons. Persons’ characteristics can be detected to identify those at risk for poor heart failure symptom perception. The self-care of heart failure index v.7.2 and its symptom perception subscale can be used to measure self-care and symptom perception in heart failure.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this work was supported by the School of Health Sciences Fribourg, HES-SO University of Applied Sciences and Arts Western Switzerland (to GCS, PSK, JG) and county council Sörmland Sweden (to ML) to dedicate a part of their positions’ time to the scoping review.
Supplementary material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.