
Abstract
Background:
Self-care behaviours are important to improve health outcomes in patients with heart failure. However, little is known about the factors related to the subdimensions of self-care behaviours in these patients.
Aims:
To identify the factors associated with the subdimensions of self-care behaviours among South Korean patients with heart failure.
Methods:
The participants in this cross-sectional descriptive study conducted between October 2016 and January 2017 were 178 patients with heart failure. Self-care behaviours were measured using the EHFScB-9, which has three subdimensions: autonomy-based adherence; provider-directed adherence; and consulting behaviours. Demographic characteristics, experience of heart failure education, physical function, patient health questionnaire-9, Pittsburgh sleep quality index and self-care confidence were also measured. Descriptive statistics and multiple linear regression analysis were conducted.
Results:
The mean age was 62 ± 12 years, and 37% were women. Younger age (P=0.023), no experience of heart failure education (P=0.039), poor physical function (P=0.003), poor sleep quality (P=0.037) and lower self-care confidence (P=0.001) were significantly associated with poor autonomy-based adherence. Being employed (P=0.042), poor sleep quality (P=0.042) and lower levels of self-care confidence (P=0.001) were associated with poor provider-directed adherence. Younger age (P=0.001) and lower self-care confidence (P=0.001) were associated with lower engagement in consulting behaviours.
Conclusion:
The three subdimensions of self-care behaviours were associated with different psychosocial factors, necessitating the development of tailored interventions and educational materials based on unique self-care behaviour patterns in patients with heart failure.
Introduction
Heart failure (HF) is a chronic disease that is becoming increasingly prevalent worldwide. In Europe and the United States, respectively, approximately 15 million and 5.7 million (2.2%) adults have HF. With regard to Asia, while current prevalence estimates range from 1.26% to 6.7%, 1 overall, there are large information gaps in the context of HF. Considering South Korea specifically, between 2012 and 2017, the number of patients with HF increased from approximately 99,000 to 119,000 (i.e. approximately 20%). 2 Furthermore, the number of patients with HF in ageing societies is likely to increase sharply. 1
Despite medical and technological advances in HF treatment, symptoms such as dyspnoea, oedema, fatigue and poor sleep quality can increase patients’ physical limitations and depressive symptoms. 1 Furthermore, the repeated hospitalisations resulting from these symptoms increase patients’ financial burden. In this regard, the American Heart Association and the European Society of Cardiology (ESC) have recommended optimal medication therapy and involvement in self-care behaviours.1,3
As per the middle-range theory of self-care of chronic illness, self-care is the process of maintaining health through health-promoting practices and managing illness. This theory is based on three concepts: self-care maintenance (e.g. taking medication as prescribed); self-care monitoring (e.g. daily weight monitoring); and self-care management (e.g. contacting doctors or nurses in the case of dyspnoea).4,5 This theory focuses on both routine adherence behaviours and symptom response behaviours. Previous studies, including those conducted in South Korea, have reported lower readmission and mortality rates and higher quality of life in patients with HF with better self-care.6–8
However, despite these benefits, many patients with HF find it difficult to perform self-care behaviours. In particular, patients’ performance of routine adherence behaviours (regular exercise, weight checks, low sodium diet) has been demonstrated to be poor worldwide. 9 While prior studies on South Koreans with HF have presented similar results to other populations with HF, as per one report, the performance of consulting behaviours was worse than that of routine adherence behaviours.10,11 In addition, recent studies have identified the patterns of self-care behaviours in patients with HF,12–14 while previous studies have considered individual behaviours or self-care as a continuum. It is important to consider overall self-care as the continuum, and subdimensions of self-care are important to identify patterns of self-care.
In contrast with the expanding knowledge of factors related to overall self-care behaviours,15,16 we know relatively little about routine self-care behaviours (i.e. taking medication as prescribed, weight monitoring) and consulting behaviours (i.e. seeking prompt consultation for HF-related symptoms). 17 The determination of factors related to the subdimensions of self-care behaviours would help identify patients at risk of ineffective self-care behaviours and accordingly provide tailored education and targeted nursing interventions. This may provide the information necessary to develop educational interventions to improve individual self-care behaviour patterns. Therefore, the purpose of this study was to examine the self-care behaviours of South Korean patients with HF and identify the factors associated with the subdimensions of self-care behaviours.
Methods
Design and setting
The participants in this cross-sectional descriptive study were 178 patients with HF. Data were collected through self-reports of patients who visited the outpatient clinic of Severance Hospital in Seoul, South Korea between October 2016 and January 2017. The study received approval from the concerned institutional review board (IRB; no. 4-2014-0403) and was conducted in accordance with the principles outlined in the Declaration of Helsinki.
Sample and sampling criteria
Eligible participants met the following inclusion criteria: (a) age 18 years or over; (b) diagnosis of HF and stable dosage of HF medications for at least 3 months; (c) depressed left ventricular systolic function with left ventricular ejection fraction (LVEF) less than 50%; and (d) able to read and speak Korean. The exclusion criteria were as follows: (a) cardiovascular accident in the past 3 months; (b) obvious cognitive impairment (i.e. dementia or head trauma); (c) end-stage cancer; (d) severe thyroid disease; and (e) hepatic or renal failure (i.e. peritoneal dialysis or haemodialysis).
The required sample size was estimated using G*Power and the following specifications: significance level (α) = 0.05, medium effect size (f2) = 0.15, power (1–β) = 0.95 and number of independent variables = 8. The results revealed that a sample of at least 160 patients was required. A total of 189 patients were eligible for inclusion, but three patients declined to participate and the questionnaires of eight patients were incomplete. Finally, 178 patients were included.
Measures
Personal data questionnaire
We developed and used a personal data questionnaire to assess the following personal and clinical characteristics: sociodemographic characteristics (i.e. age, sex, educational level, employment status, income, living with family, experience of HF education, aetiology of HF, disease duration, HF-related hospitalisation within one year, current medications, LVEF and comorbidity (i.e. scores on the Charlson comorbidity index (CCI); altogether 19 comorbid diseases were weighted and characterised as representing low (1–2), medium (3–24) and high (5 or more) comorbid burden). 18
Self-care behaviours
Self-care behaviours were assessed using the European heart failure self-care behaviour scale (EHFScBS). 19 In this study, we used a nine-item version (EHFScBS-9), 19 on which responses to each item are recorded on a five-point Likert scale that ranges from 1 (completely agree) to 5 (completely disagree). Total scores can range from 9 to 45. In the original scale, higher scores are indicative of poorer self-care. Based on instruction of the EHFScBC-9, 20 we computed standardised scores (0–100) and reversed scores. The higher score indicates better self-care in this study.
The EHFScBS-9 consists of three subdimensions: autonomy-based adherence, provider-directed adherence and consulting behaviours. 20 Autonomy-based adherence assesses how often patients weigh themselves, if they drink an adequate amount of water and whether they exercise regularly. Provider-directed adherence assesses medication adherence and adherence to a low sodium diet. Consulting behaviours assess how often patients call their healthcare providers when they experience shortness of breath, ankle swelling, weight gain and fatigue. The Cronbach’s αs of the original scale and the Korean version were 0.81 and 0.72, respectively. 21 In this study, Cronbach’s α was 0.78.
Physical functional status
Physical functional status was assessed using the Korean activity scale index (KASI), 22 adapted from the Duke activity status index. Participants are required to indicate whether it is possible or impossible for them to engage in each of the 15 physical activities (e.g. climbing stairs, walking on a plane surface, mountain climbing, sexual activity). Total scores, ranging from 0 to 79, were weighted according to the grading guidelines and summed. The scores were interpreted as follows: high functional status (class I: ⩾46, II: 46>KASI⩽24, III: 24>KASI⩾4) and low functional status (class IV: <4). The reliability coefficient was 0.81 in the validation study and 0.83 in this study.
Sleep quality
Sleep quality was assessed using the Pittsburgh sleep quality index (PSQI). 23 This 19-item self-report measure, which assesses sleep quality during the preceding month, consists of seven components: sleep quality, sleep onset latency, sleep duration, habitual sleep efficiency, overall sleep disturbances, use of sleeping medication and daytime dysfunction. Responses are recorded on a four-point Likert scale that ranges from 0 to 3. Total scores can range from 0 to 21, and higher scores are indicative of poorer sleep quality. Poor sleepers are those who obtain global scores of more than 5 on the PSQI. The Cronbach’s αs of the original scale and Korean version were 0.83 and 0.84, respectively. 24 In this study, Cronbach’s α was 0.70.
Depressive symptoms
Depressive symptoms were measured using the patient health questionnaire-9 (PHQ-9). 25 Responses are recorded on a four-point Likert scale that ranges from 0 to 3, and higher scores are indicative of greater symptom severity. Total scores are interpreted as follows: no (<5), mild (5–9), moderate (10–14) and severe (⩾15) depressive symptoms. 26 The Cronbach’s αs in the original and Korean validation studies were 0.88 and 0.95, respectively. 27 In this study, Cronbach’s α was 0.80.
Self-care confidence
The self-care confidence subscale of the self-care of heart failure index (SCHFI) version 6.2 was used. 28 Responses to the six items of this subscale can be recorded on a four-point Likert scale. Scores ought to be standardised, and they can range from 25 to100; higher scores are indicative of higher levels of self-care confidence. The Korean version was developed in accordance with the recommended guidelines. Two bilingual nurses independently translated the SCHFI from English to Korean to establish semantic equivalence and determine the cultural appropriateness of the items. A bilingual professional nurse translator back-translated the Korean version into English. Finally, the original authors approved the back-translated version. The reliability of the original scale was 0.82. The reliability of the translated scale was 0.80 in this study.
Data analysis
The collected data were analysed using SPSS for Windows 20.0 (SPSS Inc., Chicago, IL, USA). Descriptive statistics were computed to examine the participants’ characteristics. Spearman’s rho was computed to analyse the relationships between self-care behaviours and age, clinical characteristics, physical function, self-care confidence, depressive symptoms and sleep quality. Multivariable linear regression was used to explore the variables related to the subdimensions of self-care behaviour. The variables included in the model were as follows: age, employment status, experience of HF education, LVEF, physical function, depressive symptoms, sleep quality and self-care confidence. All variables were entered in the regression model as continuous variables, except for employment status (employed vs. unemployed), experience of HF education (yes vs. no), and sleep quality (good vs. poor). The significance level was set at P<0.05. There were no multicollinearity issues among the variables.
Results
Demographic characteristics
The demographic characteristics of the participants are presented in Table 1. Their mean age was 61.52 years (standard deviation (SD) 12.97) and 62.9% of the participants were men. The average disease duration was 45.99 months (SD 50.01). In employment status, 39 (21.9%) of 178 participants were unemployed and 62 (34.8%) were retired. In addition, almost 70% of the participants had been taking beta-blockers. The mean LVEF was 34.3% (SD 9.09). Furthermore, the average physical function score (KASI) was 43.85 (SD 18.43), while the mean CCI score was 2.14 (SD 1.32). Moreover, 46.1% of the participants had depressive symptoms and 59.6% of them reported poor sleep quality. The mean score on the self-care confidence subscale was 65.59 (SD 15.13) (Table 1).
Sociodemographic and clinical characteristics of the participants (N=178).
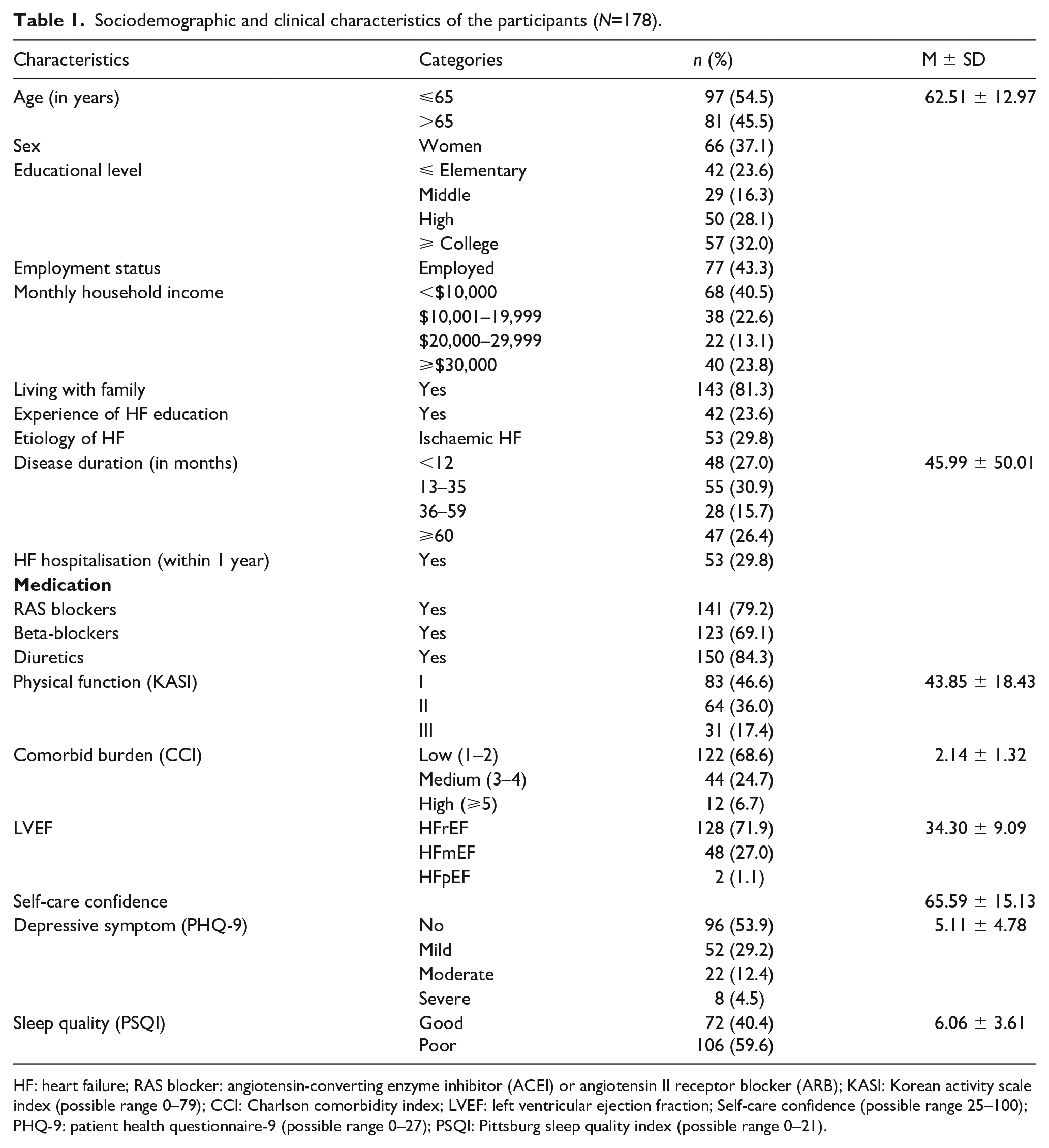
HF: heart failure; RAS blocker: angiotensin-converting enzyme inhibitor (ACEI) or angiotensin II receptor blocker (ARB); KASI: Korean activity scale index (possible range 0–79); CCI: Charlson comorbidity index; LVEF: left ventricular ejection fraction; Self-care confidence (possible range 25–100); PHQ-9: patient health questionnaire-9 (possible range 0–27); PSQI: Pittsburg sleep quality index (possible range 0–21).
Self-care behaviours
The participants obtained a mean classic score of 22.37 (SD 6.45) on the EHFScBS-9. The reversed and standardised score was 49.71 (SD 14.34). With regard to the three subdimensions, self-care associated with provider-directed adherence (two items) was good (mean 4.79, SD 0.64) and the item that assessed medication adherence (mean 4.79, SD 0.64). Self-care associated with autonomy-based adherence (three items) was poor (mean 3.01, SD 0.86) and the item that assessed fluid restriction (mean 2.67, SD 1.25) (Table 2).
Item analysis of the European Heart Failure Self-care Behaviour Scale (N=178).
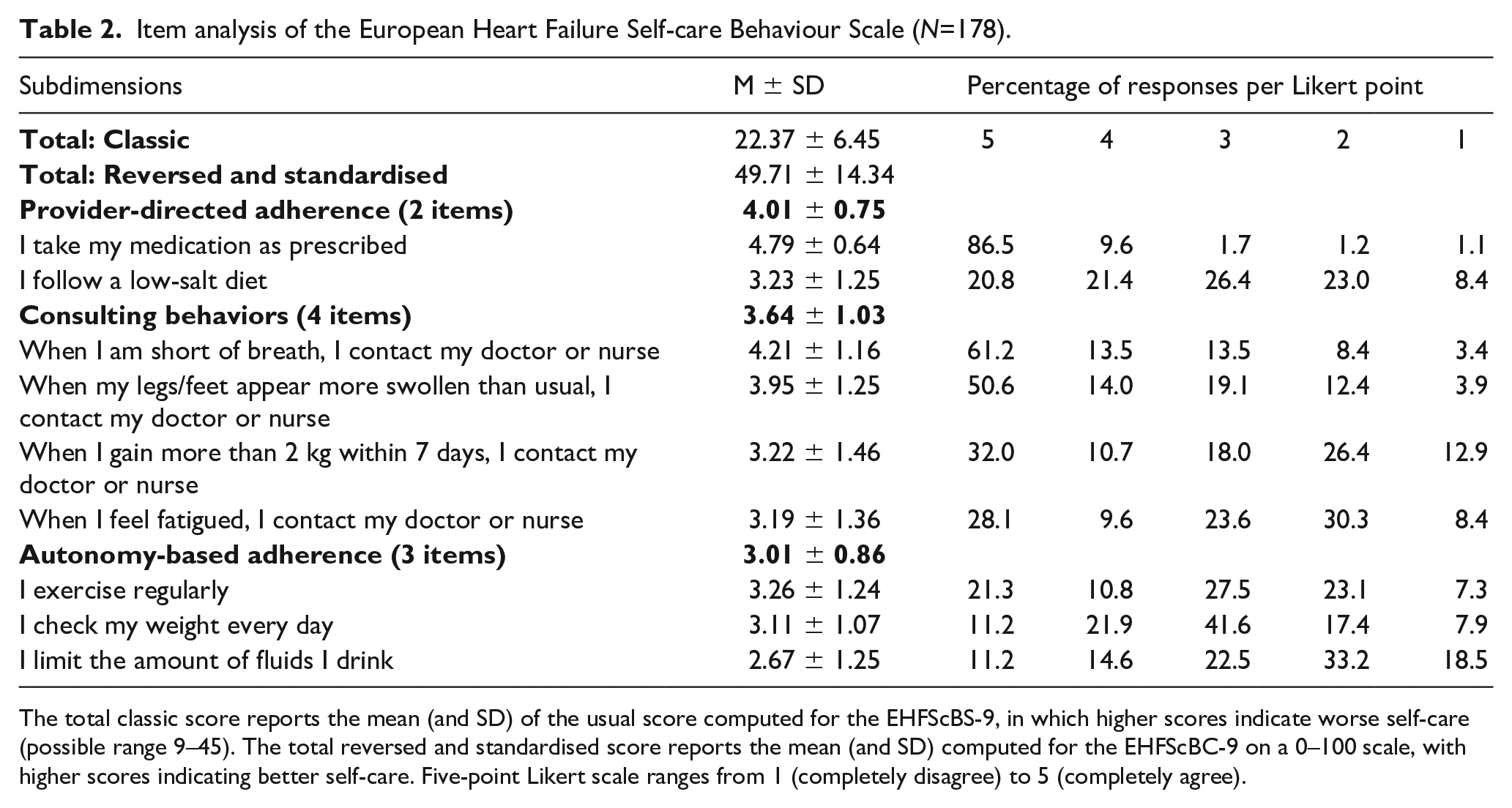
The total classic score reports the mean (and SD) of the usual score computed for the EHFScBS-9, in which higher scores indicate worse self-care (possible range 9–45). The total reversed and standardised score reports the mean (and SD) computed for the EHFScBC-9 on a 0–100 scale, with higher scores indicating better self-care. Five-point Likert scale ranges from 1 (completely disagree) to 5 (completely agree).
Correlates of self-care behaviours
Table 3 presents the factors associated with self-care behaviours: self-care confidence, higher age, good sleep quality, better physical function and being unemployed (variance explained 32.0%).
Results of multiple linear regression analysis examining the correlates of the subdimensions of self-care behaviours.
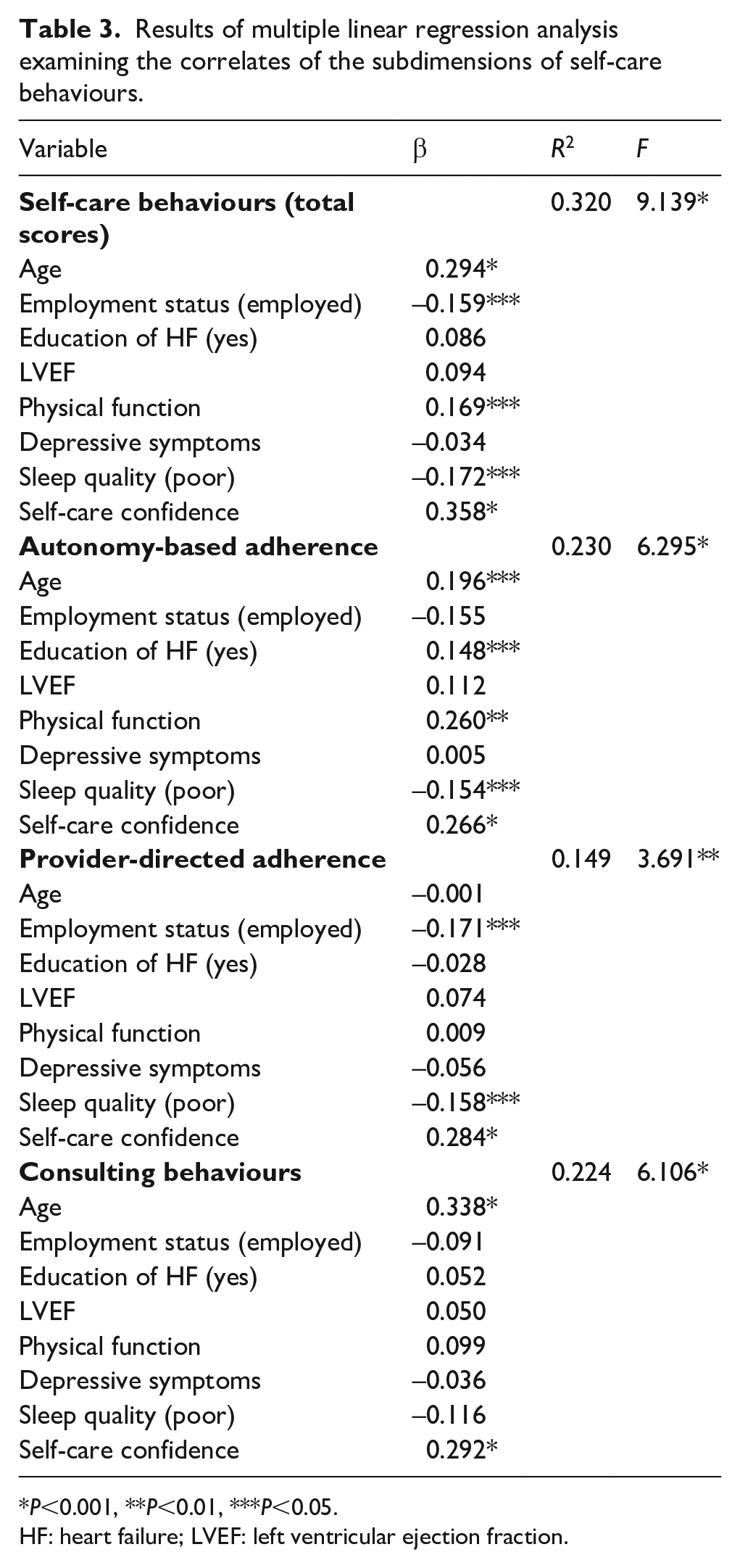
P<0.001, **P<0.01, ***P<0.05.
HF: heart failure; LVEF: left ventricular ejection fraction.
Higher levels of self-care confidence, better physical function, higher age, good sleep quality and experience of HF education were associated with better autonomy-based adherence (variance explained 23.0%). Higher levels of self-care confidence, being unemployed and good sleep quality were associated with better provider-directed adherence (variance explained 14.9%). Higher age and higher levels of self-care confidence were associated with greater engagement in consulting behaviours (variance explained 22.40%).
Discussion
The purpose of this study was to examine self-care behaviours in South Korean patients with HF and identify the factors associated with its various subdimensions. The key findings of this study can be summarised as follows. First, the participants performed best in order of provider-directed adherence, consulting behaviours and autonomy-based adherence among the subdimensions of self-care. Second, sleep quality was the primary factor associated with autonomy-based and provider-directed adherence. Third, older participants reported greater engagement in consulting behaviours. Experience of HF education was the primary factor associated with autonomy-based adherence.
This study presented engaging in a moderate level of self-care, which was greater than that reported by the study of Giezeman et al. 29 but lower than that reported by Lee et al. 30 Among the subdimensions of self-care behaviours, the poorest subdimension was autonomy-based adherence (i.e. exercise, weight monitoring), which was related to habits or daily routines in our sample. This result is consistent with the finding regarding patients with HF in several countries, in which more than 50% reported inadequate exercise and less than half weighed themselves regularly. 9 Furthermore, the item with the poorest self-care was the assessment of fluid restriction to alleviate symptoms and congestion. As the participants had relatively good physical functions, they might not have felt the need to restrict their fluid intake or understand its necessity. However, recent findings suggest that further evidence is needed to substantiate the claim that patients with HF should restrict their fluid intake. Randomised studies on fluid restriction have found no significant differences in the rehospitalisation and mortality rates of patients with stringent and liberal fluid intake regimes (except for greater thirst). 31 The ESC guidelines, which are based on weight, suggest that fluid restriction should be carefully undertaken by patients with mild to moderate HF, and that it is necessary continually to verify and revise the EHFScBS-9 for use within this population. 3
Sleep quality was significantly associated with autonomy-based and provider-directed adherence. In addition, approximately 60% of the participants reported experiencing sleep disturbances. A past study found that the prevalence of sleep disturbances among patients with HF ranges from 10% to 70%. 32 The sleep quality of our participants was better than that of the participants of past studies assessing sleep quality with the same scale.33,34 This difference may be attributable to differences in the physical function of the participants of the two studies; our participants reported better physical function. This indicates that they may have experienced fewer HF symptoms. Sleep disturbances are associated with cardiovascular events such as orthopnoea, paroxysmal nocturnal dyspnoea, Cheyne–Stokes respiration, cough, palpitations, fatigue and nocturia, 35 which can interfere with autonomic regulation and affects the daily functioning of patients with HF. A deterioration in physical function has an adverse effect on interpersonal relationships, cognition and, ultimately, psychological wellbeing.33,36 In the present study, we did not examine the relationships with other variables, but poor sleep quality was found to be associated with poor physical function and psychosocial status. Further research is needed to examine whether this relationship is mediated or moderated by self-care behaviours (e.g. medication adherence, adherence to a low sodium diet, regular exercise, weight monitoring). Sleep quality has been found to be correlated with quality of life, cardiac-related admission and mortality among patients with HF. 37 To alleviate sleep disturbances, nursing interventions for patients with HF should be customised in accordance with one’s sleep quality.
Finally, consistent with past findings, consulting behaviours were associated with age and self-care confidence. It is well accepted that seeking the counsel of healthcare providers when experiencing worsening HF symptoms is a critical symptom response behaviour. Regarding consulting behaviours, mild cognitive impairment, type D personality, anxiety level, living with someone and poor physical function have previously been shown to be associated with poor behaviours.13,30,38 There are several factors influencing the decision to engage in self-care behaviours, including knowledge, experience and skills. 5 If patients acquire adequate knowledge, they can make the necessary plans and set goals regarding self-care behaviour. 4 In the case of older participants, because of their life experience, they may have had the ability to make use of the necessary information and apply it to their lives. Self-care confidence was also an important factor associated with all subdimensions of self-care behaviours, as in previous studies. 39 In this study, about 60% of the participants had above high school education and 45% of the participants were over 65 years old. These demographic characteristics might have been related to the results regarding the level of self-care behaviours.
The relationship between age and self-care confidence remains unclear. However, it is possible that younger patients find it difficult simultaneously to manage employment and self-care. 40 Indeed, younger individuals are more familiar with modern devices such as smartphones and the internet. 41 To educate younger patients with HF, educational materials that can be accessed online or through modern technological devices should be developed. In this manner, they can receive accurate information at the appropriate time, even if they do not visit hospitals. 41
Habits or daily routines are known to be powerful determinants of self-care. 4 In this study, experience of HF education was associated with autonomy-based adherence. However, only 23.6% of the participants had received such education. According to the results, the greater the experience of HF education, the more likely participants were to engage in autonomy-based adherence. Some patients have problems in forming habits or integrating self-care in their daily lives. 42 To do so, based on the results, healthcare providers should seek to provide patients with HF with educational opportunities regarding how to implement healthcare recommendations in their daily lives.4,42
This study has some limitations. First, because of the use of convenience sampling, a cross-sectional design, recruitment from only one hospital, and the small sample size, the findings cannot be generalised to all patients with HF. Second, self-care behaviours were assessed using self-report measures, which are vulnerable to recall and social desirability biases. Despite these limitations, the present study paints a detailed portrait of the self-care behaviours of patients with HF and identifies the factors that are related to this variable. Therefore, the findings can be used to develop tailored interventions that enhance self-care behaviours in this population.
Footnotes
Sociodemographic and clinical features help identify at-risk patients. Nurses should assess the subdimensions of self-care behaviours and their correlates. Sleep quality is important for self-care behaviours. Younger patients need customised interventions. Education aids habit formation and daily self-care.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.