
Abstract
Background:
Sexual activity is an important element of quality of life for many individuals suffering from heart failure.
Aims:
The study investigated the influence of disease acceptance on sexual function in a population of male patients with chronic heart failure.
Methods:
The study included 80 patients with chronic heart failure (mean age 63.3±9.2 years) who filled in the Mell–Krat Scale questionnaire to evaluate sexual needs and reactions. We also used the International Index of Erection Function (IIEF-5) inventory and the Acceptance of Illness Scale (AIS).
Results:
The study showed that the acceptance of the illness was positively associated with all of the Mell–Krat components such as sexual need, F = (3.27), frequency of intercourse, F = (2.46), position and technique, F = (1.88). Also, according to the IIEF-5 questionnaire, 84.42% of respondents had erectile dysfunction. Taken together these indicated that psychological adjustments such as acceptance of disease increase quality of all aspects of sexual functions in heart failure patients, including their erectile functions.
Conclusions:
Our findings suggest that psychological adjustments to feelings of loss associated with the onset of heart failure disease is the important determinant of quality of sexual life among male adults. Our research implicates that effects of AIS on sexual functioning give reasonable information to tailor sexual counselling for males suffering from heart failure.
Introduction
Heart failure is a complex cardiovascular syndrome, for which the worldwide burden of disease is increasing while the prognosis for patients remains poor.1,2 The international prevalence of heart failure is over 25 million, and still increasing. In Europe about 75% of heart failure cases are of hypertensive or ischaemic aetiology.2,3 This increasing prevalence is partly due to improved survival.1,4 The long-term prognosis for heart failure patients is poor and patients present multiple co-morbidities.1,4 In addition, mortality is high among heart failure patients, and more than 50% of heart failure patients are at increased risk of mortality within five years of diagnosis.4,5
Heart failure is also known to have consequences for physical function, impacting daily life of the patient. Patients with heart failure may report a decrease in sexual performance, a loss of sexual pleasure or satisfaction, a decrease of sexual interest and a decrease in the frequency of intercourse. Recent research shows that approximately 31% of patients diagnosed with heart failure under 70 years have no sexual dysfunction. 6 In addition, male patients also mainly report erectile dysfunction. 6 According to Hoekstra et al. 7 approximately 60% to 87% of patients with heart failure report sexual problems. Recent studies have suggested that heart failure patients report more manifestations of erectile dysfunction and orgasmic difficulties than the general population.7,8 In fact, erectile dysfunction in heart failure is the most frequently reported sexual problem in heart failure and across a variety of populations. Both the disease process and comorbidities contribute to erectile dysfunction, making management of sexual dysfunction and sexual problems counselling more challenging.9,10 According to European Society of Cardiology Guidelines for heart failure, 2 erectile dysfunction is a common and important component of quality of life in men with heart failure. Reports of the rate of erectile dysfunction in heart failure range from 62% to 84%. 2
Moreover, several sexual problems may appear before the disease, but they may intensify as heart failure progresses. In previous studies, 27% of patients who were not diagnosed with sexual problems in one month after discharge from the hospital reported these problems in a later period. 8 In those patients who reported problems immediately after discharge, these problems have remained. 8 Importantly, heart failure patients and their partners usually do not openly point out sexual problems, but only some individuals have overt concerns about sexual activity. 11 Usually, they are concerned about possible insecurities related to their health.12,13 Both nurses and other health care workers are aware of the problems and concerns of heart failure patients regarding the sexual sphere, but are rarely able to deal effectively with the extent of the problem, resulting from little knowledge or embarrassment and fearing to agitate the patient. 11 Recent study on sexual concerns in a population of heart failure patients also showed that partner overprotectiveness, partner fear of sex, erectile problems or lack of sexual interest are hardly discussed with health care professionals. 14 Moreover, the return of heart failure patients to sexual activity and its timing is most often associated with unresolved patients’ concerns and requests about how to resume sexual activity, having such a medical condition.15,16
A growing body of cardiological research recognizes that a complex psychological response to chronic disease of heart failure patient should include a determinant of its acceptance, better compliance with treatment, implementation of lifestyle modifications and resultant improvement of outcomes and prognosis. 17 In fact, a recent study clearly suggests that heart failure patients might not accept their disease and they are not involved in the therapeutic process, which might lead to magnifying symptoms of heart failure. 18 Individuals suffering from heart failure symptoms with lower levels of illness acceptance more often present with lower energy, more severe pain, negative emotional reactions, sleep disorders, social isolation and limited mobility.18,19 Several clinical studies have also proven that the deterioration of disease acceptance may lead to an abandonment, a loss of self-esteem and a loss of independence. 20 Moreover, it is postulated that broadly understood acceptance of the disease can be an important element shaping the patient’s behaviour in relation to his/her disease. 21 It should be stressed that the significant decline in health caused by the onset and persistence of heart failure in middle age and later adulthood may have a significant impact on the psychosocial adjustments of older adults to the disease. Obviously, individual differences in psychosocial adjustments to disease are present; however, with some adults far more distressed reactions may be triggered by sexual problems than other physical and health conditions. In fact, physical health is strongly linked to the sexuality of older adults, as documented by several studies on sexual activity in late life.22,23
The term sexual health is not only related to a sexual dysfunction or illness, but is also described as a state of sexual well-being, including a positive attitude to sexual intercourse and expectation of a pleasant experience without feelings of fear, shame or violence. 22 There is a great deal of evidence that healthy sexuality improves the quality of life of the individual and relations between partners. 23 On the other hand, sexual concerns in heart failure patients may be manifested by anxiety and fear regarding sexual activity in general, the physical effort required for sexual activity, or physical symptoms that may result from engaging in sexual activity;9,14,24 as well as a lower quality of life in general. 25 For instance, Jaarsma and Stromberg 26 have found that the prevalence of sexual problems in two European populations was 42%.
In particular, sexual problems are evident in men, triggering in their relationship with their partner feelings of anxiety, lack of self-confidence, depressive states or deterioration of commitment to the relationship.26,27 The presence of sexual dysfunction in heart failure is described in a variety of ways in the available studies, such as sexual problems, performance difficulties, orgasmic difficulties and erectile dysfunction. 27 In men, the most commonly reported sexual dysfunction is erectile dysfunction, defined as the ‘persistent inability to maintain penile erection sufficient for normal sexual activity’. 9 It is important to note that in Eastern Europe, sexual activity is mostly seen by men as a sign of their masculinity, which can also be a sign of their superiority.
As mentioned above, heart failure may be associated in male populations with increased sexual dysfunction, including loss of libido and erectile and ejaculation dysfunction. Given such a view on men’s sexuality and evident losses of sexual health it becomes important to study how heart failure patients are able to accept and psychologically adjust to such a source of concern, depression and anxiety. From the research perspective, the best way to prevent such psychological problems is to evaluate how acceptance of illness may affect sex activity in patients with chronic heart failure. To address this research problem, the present study investigated effects of acceptance of illness on sexual functions and quality of sexual life in a population sample of male adults with chronic heart failure.
Methods
Study settings and participants
The study was conducted in 2018–2019 at the Department of Cardiology, Wroclaw Medical University. The inclusion criteria for enrolling patients in the study were: age of 18 years or older, chronic heart failure diagnosed for at least one year and New York Heart Association (NYHA) I–III class allocation. Patients with NYHA class IV, and those requiring intensive cardiac care, were excluded, as sexual activity is absolutely not recommended in those health conditions according to the American Heart Association. 24 This was a prospective and observational study; thus the STROBE guidelines (Strengthening the Reporting of Observational Studies in Epidemiology) were followed. 28 The consenting patients underwent face-to-face interviews conducted by a trained cardiac nurse, who was a co-author of the present study. Clinical characteristics were obtained from patients’ medical records.
Ethical considerations
The protocol of the study was approved by the Local Bioethics Committee at Wroclaw Medical University (decision no. KB–153/2018). All patients gave their written informed consent after a thorough explanation of the procedures involved. The investigation conforms to the principles outlined in the Declaration of Helsinki. 29
Research tools and measurements
Mell–Krat Scale
We used the Polish version of the Mell–Krat Scale, which was adapted by Lew-Starowicz. 30 This is a questionnaire designed to assess sexual needs and reactions. There are two versions of the tool, the first of which is dedicated for men and contains 13 items and the second of which is dedicated for women and contains 20 items. In this study, we employed the Mell–Krat Scale version for men. The reliability of this Mell–Krat Scale version in the previous studies was proven to be at the satisfactory level, Cronbach’s alpha = 0.86.30,31 In our study, the reliability of the Mell–Krat instrument was high, since the Cronbach’s alpha yielded a value of 0.96. This questionnaire is widely used in empirical research related to sexuality, and was also employed in studies assessing the quality of sexual life and its sexual needs. 32 The version of this scale for men is made up of a total of 13 items forming measurements of key areas of sexual function. Each item includes statements which are assessed by participants on a five-point Likert-type scale from 0 to 4, with the lower results indicating problems in this aspect of sexual function (e.g. ‘The need for intercourse: 0 – never, not more than once a year; 1 – several times a year, at most once a week; 2 – several times a month, at most once a week; 3 – two or more times a week; 4 – daily, several times a day’; ‘frequency of reaching the peak (regardless of how it is reached): 0 – never, not more than once a year; 1 – several times a year, at most once a month; 2 – several times a month, at most once a week; 3 – two or more times a week; 4 – daily, several times a day’).
International Index of Erectile Function
The second tool was the International Index of Erectile Function (IIEF-5), which is considered to be a reliable and validated, self-administered, diagnostic five-item instrument for measuring erectile dysfunction.33,34 The scores of the IIEF-5 range from 1 to 25 (one item scores of 1–5) (e.g. ‘How do you rate your confidence that you could get and keep an erection? 1 – very low, 2 – low, 3 – moderate, 4 – high, 5 – very high; During sexual intercourse, how difficult was it to maintain your erection to completion of intercourse? 1 – almost never/never, 2 – a few times (much less than half the time), 3 – sometimes (about half the time), 4 – most times (much more than half the time), 5 – almost always/always’). The score above 21 was considered to be normal erectile function and at or below indicates erectile dysfunction classified into four levels based on the scores: severe (5–7), moderate (8–11), mild to moderate (12–16) and mild (17–21). 35 In our study, the reliability of the IIEF-5 scale was high, since the Cronbach’s alpha yielded a value of 0.96.
Acceptance of Illness Scale
We also used the Acceptance of Illness Scale (AIS) for assessing the level of illness acceptance among cardiac patients. AIS was developed by Felton et al. 36 and adapted into Polish by Jurczyński. 37 This tool is employed to assess how the patient copes with the illness. It examines the level of ability to accept the illness without experiencing negative emotions or reactions. The questionnaire is composed of eight statements relating to the negative consequences of ill health related to the experienced limitations caused by the illness, a sense of dependence on others, lowered self-esteem and a lack of self-sufficiency. The AIS allows assessing the degree of acceptance of any disease. 37 The higher level of acceptance of the illness, the better adaptation and the lower psychological discomfort is experienced by the patient. Each item of the AIS is assessed by the respondent using the five-point Likert scale from 1 – (I strongly agree) to 5 – (I strongly disagree). Thus, the participant may receive scores from 8 up to 40. A low score indicates poor ability to accustom to illness and its acceptance which is accompanied by a strong psychological discomfort. On the other hand, higher scores of up to 40 points may be interpreted as the acceptance of the illness as well as a low level of negative emotions associated with the illness. The AIS instrument has been validated in several clinical studies on chronic illness such as cancer or rheumatoid arthritis, diabetes or hypertension.36–38 The instrument is characterized by satisfactory reliability, alpha = 0.83 at Time I (before treatment) and 0.81 at Time II (after treatment). Test–retest reliability coefficient was 0.69. 36 For patients with heart failure, the reliability of the AIS was proven to be high, producing Cronbach’s alpha values of 0.8517,18 and 0.82. 39
Statistical analysis
Qualitative data were presented in the form of numbers (n) and percentages (%). Quantitative data (e.g. disease duration) were presented in the form of mean (M) and standard deviation (SD), median (Me), lower (Q1) and upper quartiles (Q3) and extreme values (Min.–Max.). The normality of the distribution of continuous variables was assessed using the Shapiro–Wilk test. A Spearman’s correlation coefficient was employed to verify the relationship between the acceptance of the illness (AIS), Mell–Krat components and IIEF-5. The following criteria for the evaluation of the strength of the relationship between variables were used: +/−1: Perfect; from +/−0.9 to +/−0.7: Strong; from +/–0.6 to +/–0.4: Moderate; from +/−0.3 to +/−0.1: Weak; and +/−0: None. 40 A series of multiple regression analyses were performed using a hierarchical method to verify the possibility of predicting sexual function in patients with heart failure based on the degree of the acceptance of illness. In the first step, the following clinical and socio-demographic variables were introduced into the regression analysis: age; education (primary, vocational, secondary, higher); medications (diuretics, beta blockers, angiotensin-converting enzyme inhibitors, angiotensin II receptor blockers, digoxin); place of residence (towns > 300,000 inhabitants, towns < 300,000 inhabitants, rural areas); living (with wife/partner; with children/other family members; alone; health care institution); co-morbidity (diabetes mellitus, arterial hypertension, ischaemic heart disease, kidney failure, depression, other); operations around the pelvic region; urogenital tract infection; medicines for other illnesses; use of PDE-5 inhibitors, NYHA (class I–III), other treatments; frequency of medication intake (more than once a day, once a day, less than once a day); body mass index; left ventricular ejection fraction; number of hospitalizations in the last six months; duration of the disease.
The variables measured on the ordinal scale were recoded using the Dummy Coding method (coded variables: 0 = no, 1 = yes). In the second step, all designed models included a degree of disease acceptance (AIS) to make sure that sources of variability for both variables (reactivity in particular aspects of sexual function (Mell–Krat) and erectile dysfunction (IIEF-5) are explained. We also calculated the variance inflation factors (VIFs). These statistics provides a measure of multicollinearity between predictors in regression analysis by estimating artificial inflation of the variance of a regression coefficient. A rule of thumb for adjusting multicollinearity for the VIF parameter is that its value should not be greater than 10; the greater value indicates a high correlation with other predictors. 41 However, according to the other guidelines in the literature there is a potential multicollinearity problem even for VIF greater than 4. 42 In our study, the VIF values were ranged between 2.78 and 2.93 (all values are shown below). All statistical analyses were done with SPSS version 25 for Windows. The level of significance was set at p < 0.05 in all statistical tests.
In order to estimate a sample size for multiple regression analysis we employed SamplePower 3.0 software for SPSS. Our regression model included one variable in the set of interest (AIS) and 17 covariates (socio-demographic and clinical control variables). The power analysis was run with alpha set at 0.05 and required power of 80%. It was expected that the AIS would be clinically useful if it could explain 4% of the variance in the Mell–Krat. It was expected that the covariates would explain 70% of the variance in outcome. The program showed that a sample size of 71 yielded a power of 81% for the designed set.
Results
Socio-demographic and clinical characteristics
The study included 80 male patients with chronic heart failure, aged between 40 and 80 years (M = 63.36, SD = 9.21). The mean duration of the disease in this sample was 3.40 years (SD = 5.42) ranged 1–33 years. The socio-demographic and clinical characteristics are presented in Table 1.
Clinical characteristics of participants in the study (N=80).
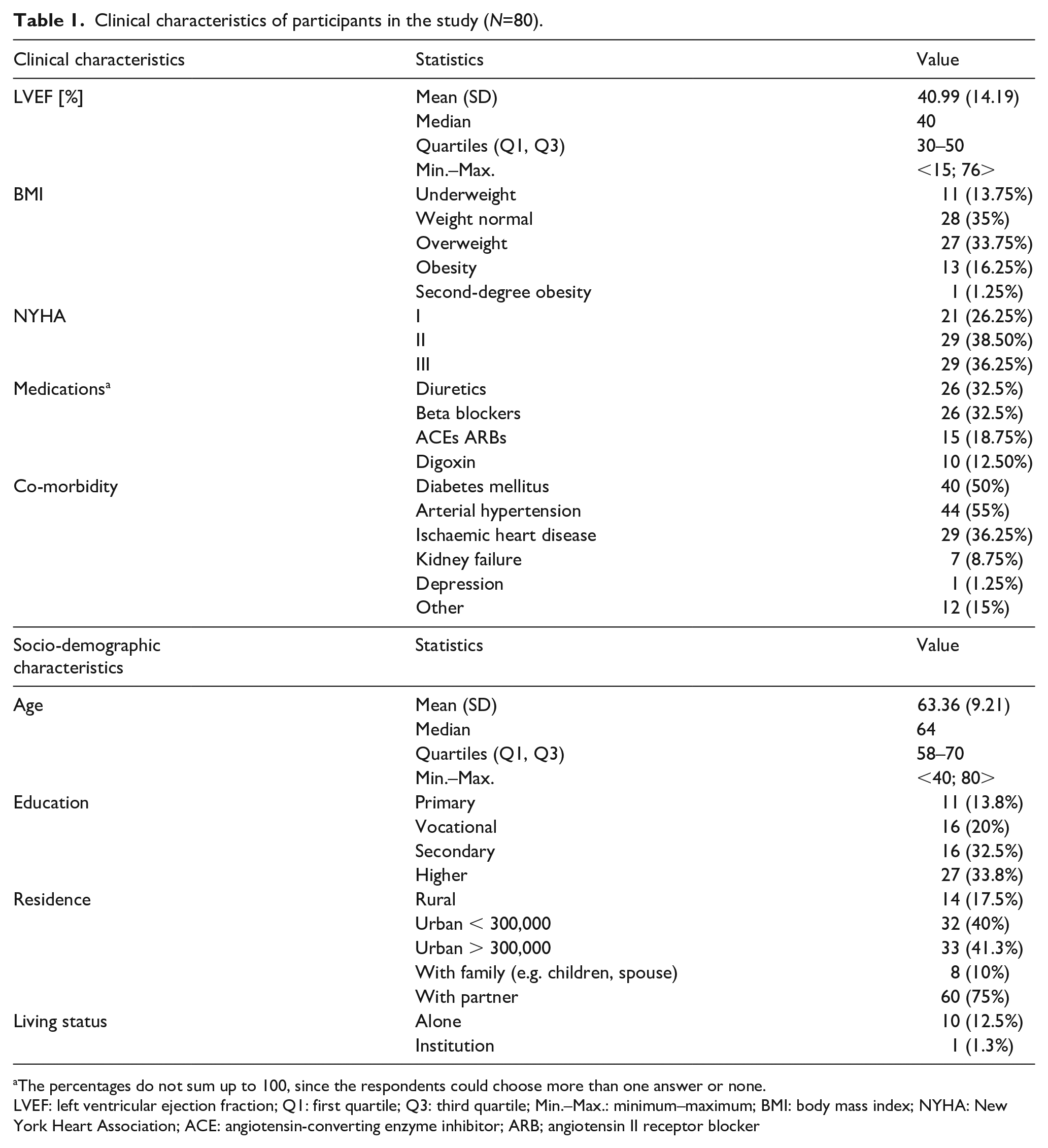
The percentages do not sum up to 100, since the respondents could choose more than one answer or none.
LVEF: left ventricular ejection fraction; Q1: first quartile; Q3: third quartile; Min.–Max.: minimum–maximum; BMI: body mass index; NYHA: New York Heart Association; ACE: angiotensin-converting enzyme inhibitor; ARB; angiotensin II receptor blocker
Sexual functioning of the men with heart failure and acceptance of their illness
As was mentioned above, the Mell–Krat Scale allows to assess the sexual needs and reactions of 13 aspects of sexual functioning. To evaluate each area, participants used the scale from 0 to 4, with 0 indicating no satisfaction and 4 indicating the highest level of satisfaction.
In this sample of heart failure patients, the most satisfying aspects were libido (M = 2.63, SD = 1.16) and assessments by the partner (M = 2.11, SD = 1.18) as well as self-assessment (M = 2.10, SD = 1.32). The patients were least satisfied with mood before sexual intercourse (M = 1.33, SD = 0.85) and the frequency both of the sexual acts (M = 1.62, SD = 1.02) and orgasm (M = 1.62, SD = 1.19). The descriptive statistics related to Mell–Krat results are presented in Table 2.
The descriptive statistics of Mell–Krat Scale results.
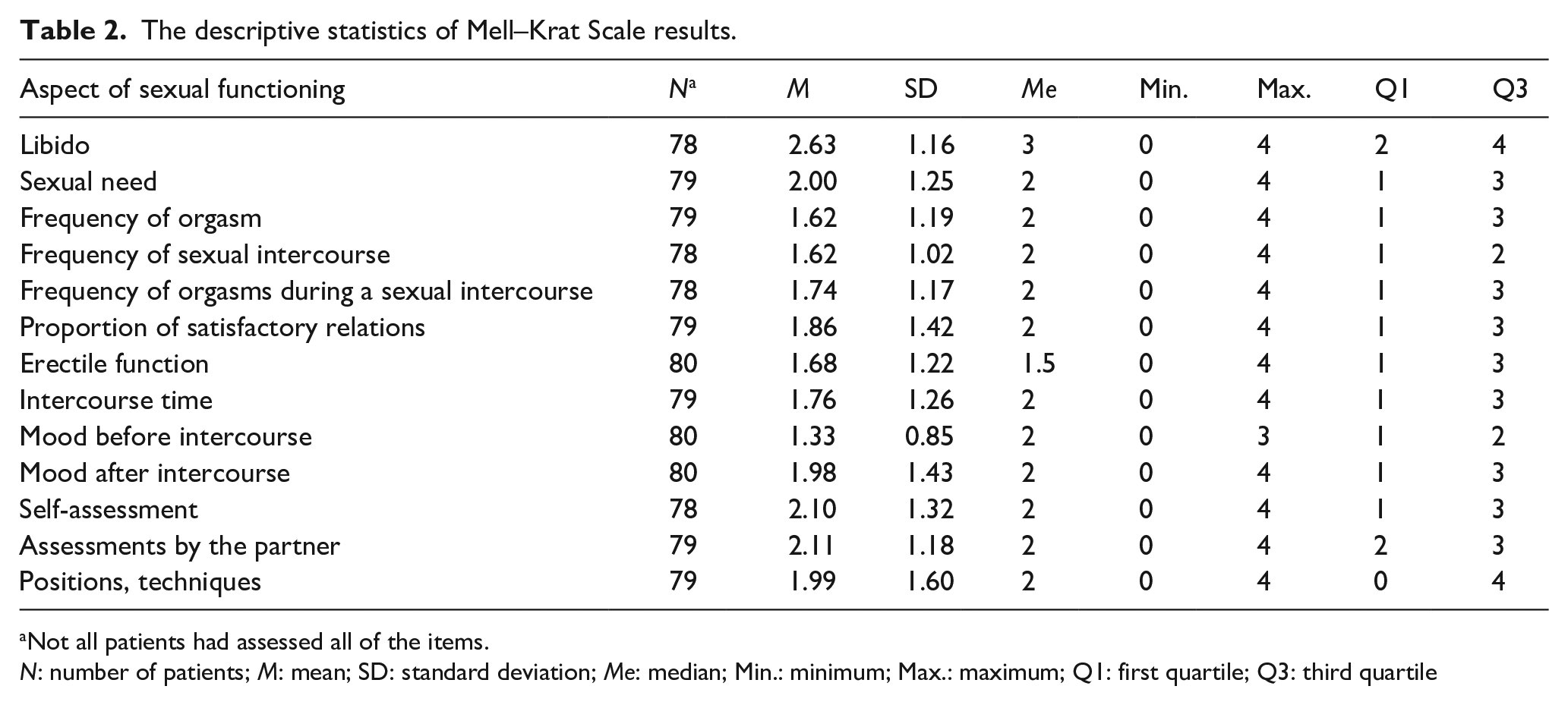
Not all patients had assessed all of the items.
N: number of patients; M: mean; SD: standard deviation; Me: median; Min.: minimum; Max.: maximum; Q1: first quartile; Q3: third quartile
The IIEF-5 for men allowed to identify manifestation of erectile dysfunction, yielding the mean erectile dysfunction values of M = 12.68 (SD = 7.56). The total score indicating the presence of erection disorders was equal to or lower than 21. We observed that 68 of 80 heart failure patients (85%) had erectile disorders.
The lowest score of acceptance of the illness among participants was eight points, indicating loss of adaptation and non-acceptance of illness as well as mental discomfort. The maximum result in this sample was 40, which suggests the acceptance of cardiovascular disease and the absence of negative emotions related to it. For the group of men who participated in the study, the mean value was 26.75 points (SD = 9.59). There are no available measures of established cut-off points indicating no acceptance or acceptance of the disease for a Polish population of patients. Nonetheless, the mean scores in the sample of cardiovascular patients are comparable to the results among a variety of the Polish patient samples, including cancer patients (M = 27.56, SD = 8.52) and patients with diabetes (M = 29.6, SD = 8.1) and peripheral diabetic neuropathy (M = 26.6, SD = 8.4).
The correlations between acceptance of the illness and sexual functioning
In the present study the acceptance of the illness was significantly positively associated with all of the Mell–Krat components as well as with the measure of IIEF-5. These results suggested that the greater the acceptance, the more satisfaction with all aspects of sexual function and less erectile dysfunction (see Table 3).
The relationships between the Acceptance of Illness Scale, Mell–Krat Scale components and IIEF-5.
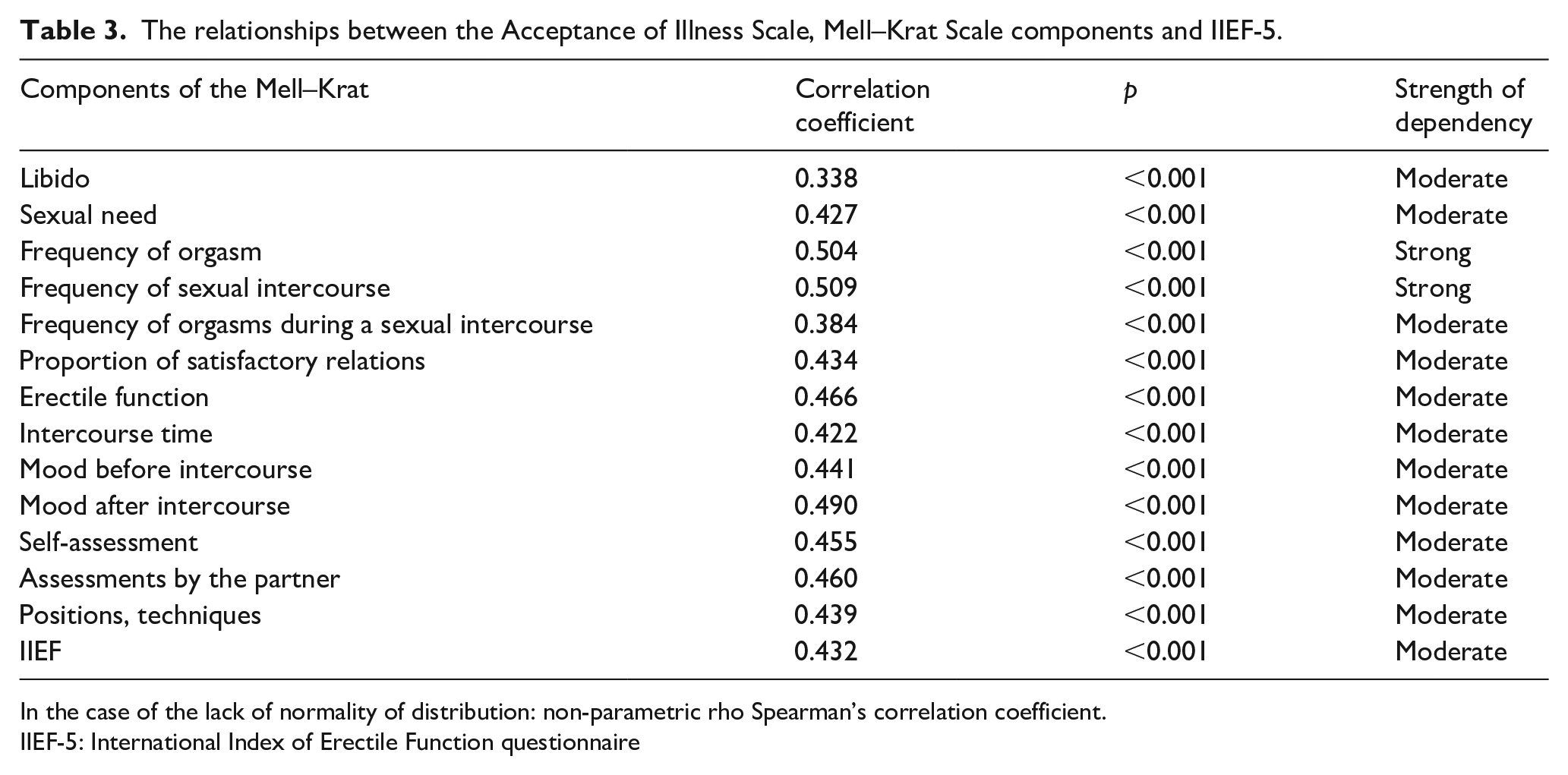
In the case of the lack of normality of distribution: non-parametric rho Spearman’s correlation coefficient.
IIEF-5: International Index of Erectile Function questionnaire
The strongest association of the AIS scores was with frequency of orgasm (rs = 0.504, p < 0.001) and frequency of sexual intercourse (rs = 0.509, p < 0.001).
The results of two-step hierarchical regression analysis for acceptance of the illness predicting aspects of sexual functions
In order to verify the possibility of predicting sexual function in patients with heart failure based on the degree of the acceptance of illness, a series of multiple regression analyses were performed using a hierarchical method. In the first step, the clinical and socio-demographic variables were introduced into regression equations. The variables measured on the ordinal scale were recoded using the Dummy Coding method. In the second step, a degree of disease acceptance (AIS) was added to each model to take variability of the explained variables (particular aspects of sexual function (Mell–Krat) and erectile dysfunction (IIEF-5) into consideration.
The analysis indicated that the factor acceptance of disease (AIS), when clinical and socio-demographic variables were included in the model, was an important predictor of satisfaction with Sexual need, F(33,36) = 2.76; p < 0.01.
The hierarchical multiple regression at step 1 revealed that all controlled variables contributed to the regression model significantly, F(32,36) = 2.83; p < 0.01, and accounted for 73.9% of the variance of the Sexual need (Mell–Krat 2) variable. Furthermore, the analysis indicated that inclusion of the Acceptance of the illness variable into the model had explained an additional 2.8% of variation in the factor of Sexual need and made a significant change in the R² parameter, ∆F(1,36) = 4.38; p < 0.05 (see Table 4).
Summary of two-step hierarchical regression analysis for acceptance of the illness predicting aspects of sexual functions.
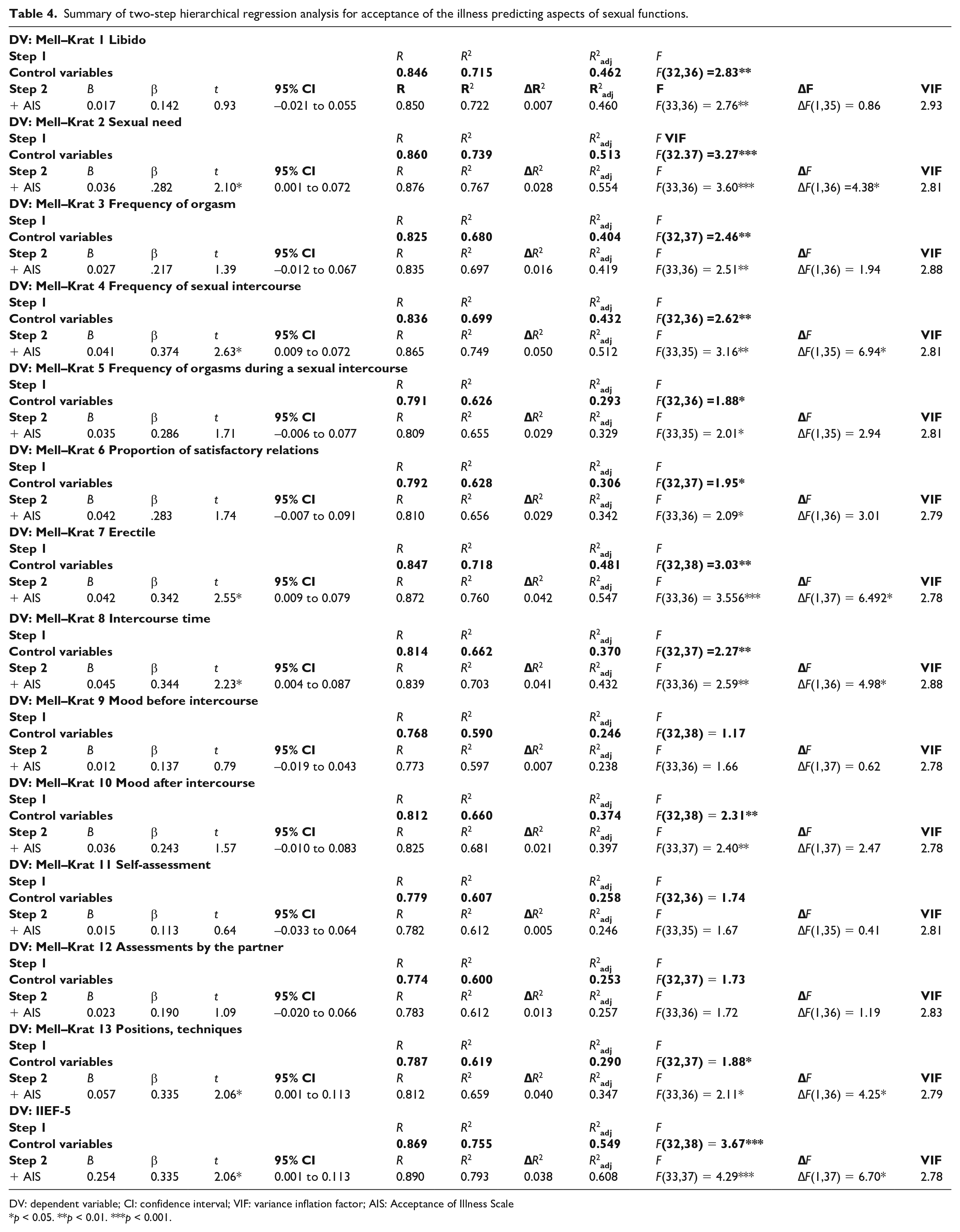
DV: dependent variable; CI: confidence interval; VIF: variance inflation factor; AIS: Acceptance of Illness Scale
p < 0.05. **p < 0.01. ***p < 0.001.
Frequency of sexual intercourse
The regression analysis indicated that controlled variables can explain 69.9% of the variance in Frequency of sexual intercourse (Mell–Krat 4). Adding the AIS additionally had explained 5% of variation in Mell–Krat 4, ∆F(1,35) = 6.94; p < 0.05.
Erectile function
For the erection satisfaction variable, the control variables explained 71.8% of the variance with respect to this sexual function. Inclusion of the AIS variable into the model allowed to explain an additional amount of the variance (4.2%) for the satisfaction with the erection.
Intercourse time
The regression analysis indicated that the socio-demographic and clinical control variables contributed to the regression model significantly, F(32,37) =2.27; p < 0.01, explaining 66.2% of the variance for the intercourse duration variable. By adding the AIS factor into the model the variance of Mell–Krat 8 had increased by 4.1%, ∆F(1,36) = 4.98; p < 0.05.
Positions and techniques
The results indicated that the variances of satisfaction with positions and techniques during intercourse variables were significantly explained both by the control variables (61.9%; F(32,37) = 1.88; p < 0.05) and AIS (4%; ∆F(1,36) = 4.25; p < 0.05).
Erectile dysfunction (IIEF-5)
The hierarchical regression had showed that controlled variables contributed to the regression model significantly, F(32,38) = 3.67; p < 0.001, accounting for 75.5% of the variance of IIEF-5. Inclusion of the Acceptance of illness variable into the model had increased by an additional 3.8% of variance, explained in IIEF-5, ∆F(1,37) = 6.70; p < 0.05.
Taking all these results together, it turned out that the variable Acceptance of the illness is the most important predictor for the factor of Frequency of sexual intercourse (B = 0.041, β = 0.374; t = 2.63, p < 0.05; 95% confidence interval (CI): 0.009–0.072). This indicates that an increase in AIS scoring by one point more resulted in increasing the Frequency of sexual intercourse by about 0.04 points. Similar results were obtained for the following variables: Sexual need (B = 0.036, β = 0.282; t =2.10, p < 0.05; 95% CI: 0.001–0.072), Satisfaction with erection (B = 0.042, β = 0.342, t = 2.55, p < 0.05; 95% CI: 0.009–0.079), Intercourse time (B = 0.045, β = 0.344; t = 2.23, p < 0.05; 95% CI: 0.004–0.087) and Positions and techniques (B = 0.057, β =0.335; t = 2.06, p < 0.05; 95% CI: 0.001–0.113). The increase in AIS scoring by one point resulted in higher scoring in IIEF-5 by about 0.25 points (B = 0.254, β = 0.335; t = 2.06, p < 0.05; 95% CI: 0.001–0.113).
Discussion
The present study indicates a significant relationship between the acceptance of the disease and sexual functions measured by Mell–Krat Scale and the IIEF-5 among men with heart failure symptoms. In particular, the analysis of the sexual functions showed that the participants reported the best sexual functions on two dimensions of sexuality, specifically: libido, assessments by the partner and self-esteem. However, the observed level of libido in heart failure patients in our study was lower than in men with other physical conditions, for example, after a stroke. 43 In contrast, our results showed that self-esteem and assessments by the partner were rated higher among patients with heart failure in comparison with males after a stroke. 43
The presence of sexual dysfunction in heart failure is described in a variety of ways in the available studies, such as sexual problems, performance difficulties, orgasmic difficulties and erectile dysfunction. 27 In men, the most commonly reported sexual dysfunction is erectile dysfunction, defined as the ‘persistent inability to maintain penile erection sufficient for normal sexual activity’. 9 Our results confirm the high prevalence of erectile dysfunction among men with heart failure. About 84% of respondents in this study had erectile dysfunction. In the presented study, the percentage of heart failure patients reporting erectile dysfunction was high. This may be also due to the fact that the study group was older than in other studies. However, erectile dysfunction problems are reported in almost 81% of cardiac patients, which is consistent with our results.44,45 It should also be noted that the IIEF, which was used in this study to assess erectile dysfunction, has overestimated the level of erectile dysfunction in previous studies. 46 Moreover, some drugs applied for heart failure therapy (e.g. thiazide diuretics, spironolactone and beta-blockers) may contribute to erectile dysfunction. It should be noted that sexual dysfunction may persist over time, with 70% of those who had sexual difficulties at discharge later reporting persistent sexual problems after 18 months. 8 Factors associated with sexual dysfunction include, for example, worse functional NYHA class, more comorbid conditions,33,47 living with a partner, male gender. For that reason, we controlled socio-demographic and clinical variables in the regression model.
This study clearly shows that acceptance of the illness is an important factor involved in sexual functions and erectile dysfunction among heart failure male patients. Therefore, we believe that including psychological interventions aimed at enhancement of acceptance of the disease may significantly contribute to improving the quality of sexual life among males with heart failure. It turned out that acceptance of the illness is involved in predicting sexual need, frequency of sexual intercourse, quality of erection, intercourse time, positions and techniques and erectile dysfunction. Changes in sexual activity in patients with cardiovascular disease impair intimate relationships with partners, their communication leading to anxiety and depression and perpetuating sexual concerns for both.14,24,47 Indeed, in the past, psychological diagnosis for patients with heart failure used to be limited to assessing depressive symptoms, anxiety and levels of health-related quality of life. 9 Recent guidelines for sexual counselling indicate that assessment of psychological concerns of sexual activity in patients with cardiovascular disease should include fears, anxiety and depression, but also sexual self-concept factors underlying the desire and physical activity of heart failure patients to be sexually active. 9 For instance, sexual anxiety and sexual self-efficacy (i.e. a person’s belief about being able to address their own sexual issues) as central self-concept factors were demonstrated to have an impact on sexual activity in a combined sample of those with heart failure and healthy elders9,47 and also less frequent hospitalizations, occurrence of symptoms with daily activities and very poor prognosis. 48
Our study provides empirical evidence that acceptance of the illness should be included in the guidelines for sexual counselling of heart failure patients and their partners. In this way, the complex assessment of psychological aspects of cardiac patients’ functioning when undergoing sexual counselling may possibly improve patient knowledge, awareness about sexual activity and better sexual desire, satisfaction and quality of sexual activity. 9
Researchers are interested in the quality of sexual life in relation to various physical diseases. For example, studies using the IIEF questionnaire and AIS scale have shown that also among patients with diabetes mellitus type 2, higher adaptation to illness is associated with better sexual functioning. 47 These results confirm the influence of acceptance of the illness on various areas of quality of life and its universal relation to widely chronic diseases. Some studies concern satisfaction with sex life, people with depression and diabetes, and sexual dysfunctions. 10 Recent studies have shown that heart failure patients have reported engaging in a variety of intimate activities besides sexual intercourse. These include kissing and hugging, petting and fondling, self-masturbation, mutual masturbation with their partner and oral sex. 14 Sexual activities beyond sexual intercourse can be enjoyed by heart failure patients and their partners and that discussion of intimate activities should not be limited to sexual intercourse. This can be helpful for heart failure patients who have decreased exercise tolerance and must avoid more intense physical and sexual activities. 14 Management of sexual dysfunction in heart failure is a complex issue that may involve a multidisciplinary team when seeking solutions.
In psychology, it has been proposed to extend the concept of sexual satisfaction to psychological factors that are significantly related to a close relationship. For example, according to the theory by Plopa 49 sexual satisfaction should be related not only to the biological aspect of intercourse, but also to the aspect of emotional value and the value of a close relationship. Therefore, the factors that make up sexual satisfaction relate to closeness, caressing and sex. In fact, two questions from the inventory by Plopa 49 (the scale contains 10 questions) are relevant to intercourse and orgasm. The studies conducted by Plopa 49 have demonstrated significant relationships between the sense of quality of life and satisfaction with sex life. These studies also have provided significant evidence for links between physical health and sex life as well as indications that the acceptance of disease is an important category for sex life. It brings an interesting question about the significance of acceptance of the illness in the quality of other sexual activities among heart failure patients.16,50
What is extremely important is that most patients perceive the symptoms of the disease (shortness of breath, fatigue, use of medication, limited circulation) as causes of sexual problems. As previously highlighted48,8 in other studies, the level of disease acceptance may have an impact on better compliance, lifestyle changes, improved treatment outcomes and prognosis. The present study may contribute to further consideration of whether better disease acceptance may possibly cause heart failure patients to deal with negative emotions towards their health condition. Thus, it has a positive effect on the level of satisfaction with sex life. To the best of our knowledge, this study is the first one to analyse acceptance of illness and impact on sexual function in patients with chronic heart failure. Previous studies have centred mostly around the level of acceptance of disease and the influence on quality of life. The present study demonstrates the impact of acceptance of illness on sexual function where acceptance of illness is the only independent predictor of sexual function in Mell–Krat domains such as the frequency of sexual intercourse, sexual needs, intercourse time, and positions and techniques, as well as erectile dysfunction measured by IIEF-5.
Conclusions
Disturbances in sexual activity in patients with heart failure cause this cardiac population to face not only severe medical conditions but also impairments in their psychosocial condition linked with intimate relationships with partners, anxiety and depression and perpetuating their sexual concerns. The present study demonstrated that acceptance of the disease may play an important role in helping patients with heart failure to deal with their reported sexual problems. We showed that the better the acceptance of illness, the greater the quality of each aspect of one’s sex life and the less erectile dysfunction it causes. Acceptance of illness may exert significant effects on sexual needs, frequency of intercourse, intercourse time, positions and techniques and erectile dysfunction. For the population investigated we showed that patients with the higher levels of AIS were most satisfied with their libido and their partner’s evaluation and self-evaluation, and least of all with their mood before intercourse, frequency of intercourse and orgasm. Our findings from this study emphasize that evaluation of disease acceptance in heart failure patients should be an important element of the clinical assessment in cardiology. Therefore, we suggest that this psychological factor should be reflected in the development of further guidelines for the treatment and counselling of patients with heart failure symptoms.
Indications of the research
The present study clearly suggests that increasing psychological adjustments to feelings of loss associated with the onset of heart failure disease should be taken into consideration in sexual counselling. Therefore, routine assessment of sexual problems and counselling of heart failure individuals can be beneficial to effective management by health care professionals. The present research outcomes, in turn, indicate that an advanced health care system dealing with heart failure patients diagnosed with sexual problems should be interdisciplinary, taking into account the following aspects: (1) there are individual differences between male patients with chronic heart failure in coping with sexual health; (2) the important area of knowledge to be addressed in sexuality of heart failure patients is their acceptance of the illness; as well as (3) management of sexual dysfunction in heart failure should involve a multidisciplinary team of physicians, nurses and other health workers when seeking effective solutions.
In everyday practice, health care professionals may hold stereotypical views on ageing and sexuality and avoid providing sexual counselling to heart failure patients. Current evidence from our research showed that indicating area of knowledge on psychosocial adjustments based on psychometric measures is a reliable tool in getting a thorough understanding in order to overcome myths and misperceptions of sexual activity in adult age in heart failure populations.
Limitations
We are well aware of potential limitations of this study. The most important of them stems from the fact that our sample was relatively small and recruited from a single centre. Moreover, we determined patients’ sexual function using the Mell–Krat Scale and thus our analysis may not reflect some heart failure specific aspects of sexual life.
Footnotes
Acknowledgements
There were no other contributors to the article than the authors, as well as there was no writing assistance regarding our paper. We want to thank all participants for their contribution in this research.
Analysis of the impact of acceptance of illness on sexual functioning may give reasonable information to tailor sexual counselling to individual patients’ needs. Routine assessment of sexual problems and counselling of individuals with heart failure can be beneficial to effective management by health care professionals. Management of sexual dysfunction in heart failure should involve a multidisciplinary team of physicians, nurses and other health workers when seeking effective solutions.
Declaration of conflicting interests
The authors have no conflicts of interest to declare.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ministry of Science and Higher Education of Poland as a part of a statutory grant of the Wroclaw Medical University for maintaining research potential (grant no. SUB.E020.19.003).