
Abstract
Background
It is well known that blood glucose levels are increased in the first 12 hours after the onset of acute stroke. The magnitude of the rise is supposedly related to the severity of the stroke and this is in turn associated with a worse prognosis. Several guidelines advocate the use of insulin sliding scales in the acute stroke setting but these are only implemented with varying degrees of success. There is no clear evidence base as to the glycaemic level at which to intervene and the significance of the intervention on outcomes.
Methods
We prospectively reviewed the treatment of 229 patients admitted to a stroke unit and compared admission blood glucose results with stroke prognostic/neurological deficit score (National Institutes of Health Stroke Scale) at 30 days. Inter-physician practice variability allowed us to observe the outcomes when different levels for intervention were used (and allowed us to calculate an optimum level of glucose at which insulin sliding scale treatment would lead to most benefit).
Results
We showed that glucose is a modifiable factor that has implications for long-term stroke outcomes.
Conclusion
The suggested level for intervention with insulin (admission blood glucose of ≥ 10.1 mmol/L) is lower than previously thought.
Introduction
It is well known that blood glucose levels are increased in the first 12 hours after the onset of acute stroke. 1 The magnitude of the rise in blood glucose levels is supposedly related to the severity of the stroke. 2 Studies report that hyperglycaemia occurring at the onset of stroke is associated with a worse clinical prognosis, irrespective of the patient's age, severity of the condition or stroke sub-type. 3,4 Hyperglycaemia exacerbates the ischaemic lesion and is associated with an increase in brain oedma. It is also associated with a decrease in cerebral blood flow. The precise pathological process underlying deterioration is as yet poorly understood but is thought to involve an increased immune response, and a generalised stress reaction (stimulation of the HPA axis, increased levels of catecholamines, cortisol and glucagon). A systematic review by Capes et al. 5 highlighted the significance of stress hyperglycaemia in both diabetic and non-diabetic patients, irrespective of the diagnosis of diabetes per se, in relating to worse outcomes. It has been shown that patients with transient hyperglycaemia have larger ischaemic lesions on CT brain scans and higher 30-day mortality than those of normoglycaemic stroke patients. The worse outcome manifests itself in terms of longer hospital stay, higher inpatient hospital charges and increased short and long-term mortality.
There are already several acute stroke guidelines, most notably the Royal College of Physicians stroke care guidelines in the UK and the European Stroke Organisation, which recommend the use of iv insulin sliding scales in hyperglycaemic patients, when the blood glucose level is ≥ 11.0 mmol/L. 6,7 However, this is perhaps a rather arbitrary figure as there is no clear evidence to support this cut off and there are suggestions that a lower level may be even better. One study in particular has shown that plasma glucose concentration above 8 mmol/L after acute stroke predicts a poor prognosis after correcting for age, stroke severity, and stroke subtype. 8 Raised plasma glucose concentration is therefore unlikely to be solely a stress response and should be treated actively. 9 This is because it is known to be an independent modifiable risk factor with a bearing on post-stroke prognosis. Caution, however, is necessary. Landmark trials which led to the worldwide introduction of tight glycaemic control for critically ill patients on ICUs demonstrate the improvements in outcomes when normoglycaemia is achieved, but treatment effects are often worsened when blood glucose is driven too low; 10,11 there may be an increase in hypoglycaemic events and no effect on mortality. Therefore the cut off and efficacy of blood glucose lowering therapy in acute stroke needs to be established.
The purpose of the current study is to analyse prospectively collected data regarding the outcomes of hyperglycaemic patients presenting with acute stroke, in an attempt to calculate the most significant level of glucose upon which to swiftly act. We hope to aim for a more rigorous approach following the DIGAMI model for acute coronary syndromes which have received much more attention previously. 12
To examine association between blood glucose on admission and clinical outcomes (NIHSS scale at 30 days).
To examine association between 30-day NIHSS score for those who did and did not receive iv insulin.
Patients and methods
This was an observational study in which we prospectively reviewed the treatment of all confirmed stroke patients admitted to an urban stroke unit between February and October 2008 in a large teaching hospital. We aimed to analyse the medical records (observation charts, biochemical results, case notes) of all patients found to be hyperglycaemic on admission as we wanted to compare admission blood glucose results with stroke prognostic/outcome score (NIHSS) at 30 days.
The NIHSS examines for level of consciousness, vision, gaze, facial palsy and extremity weakness, limb ataxia, sensory loss, language, dysarthria and neglect. A completely normal patient with no deficit will have a score of 0. In an acute stroke setting a patient with hemiparesis, hemianopia, hemineglect and aphasia the score is 31. The maximum score is 42, severe disability. 13
We then assessed whether an iv insulin sliding scale had been used in the treatment of hyperglycaemic individuals and at what blood glucose level it had been initiated.
Inter-physician practice variability acted as the factor which allowed us to observe the different outcomes when different interventions were utilised. For example, there was major variance over the level of blood glucose at which insulin sliding scale treatment was initiated by different doctors. Some patients with significant hyperglycaemia, such as > 15 mmol/L did not receive insulin, whereas some physicians used a plasma glucose level of 9 mmol/L as a cut-off. This therefore produced two discrete patient groups: one group whose hyperglycaemia was optimally managed and another group whose hyperglycaemia was not addressed as thoroughly.
By comparing blood glucose levels on admission with clinical outcomes we hypothesised that this would allow us to calculate an optimum level of glucose at which insulin sliding scale treatment would lead to the most benefit for patients.
Information was recorded in a prospective manner on patients with a confirmed diagnosis of stroke and included preexisting diagnosis of diabetes and insulin therapy, patient age, sex, stroke severity and subtype, level of capillary blood glucose on admission, plasma glucose level, decision to initiate iv insulin sliding scale therapy, baseline NIHSS score and NIHSS score at 30 days. We then analysed the results using Microsoft Excel and SPSS statistical programs to assess the relationship between the data sets.
Results
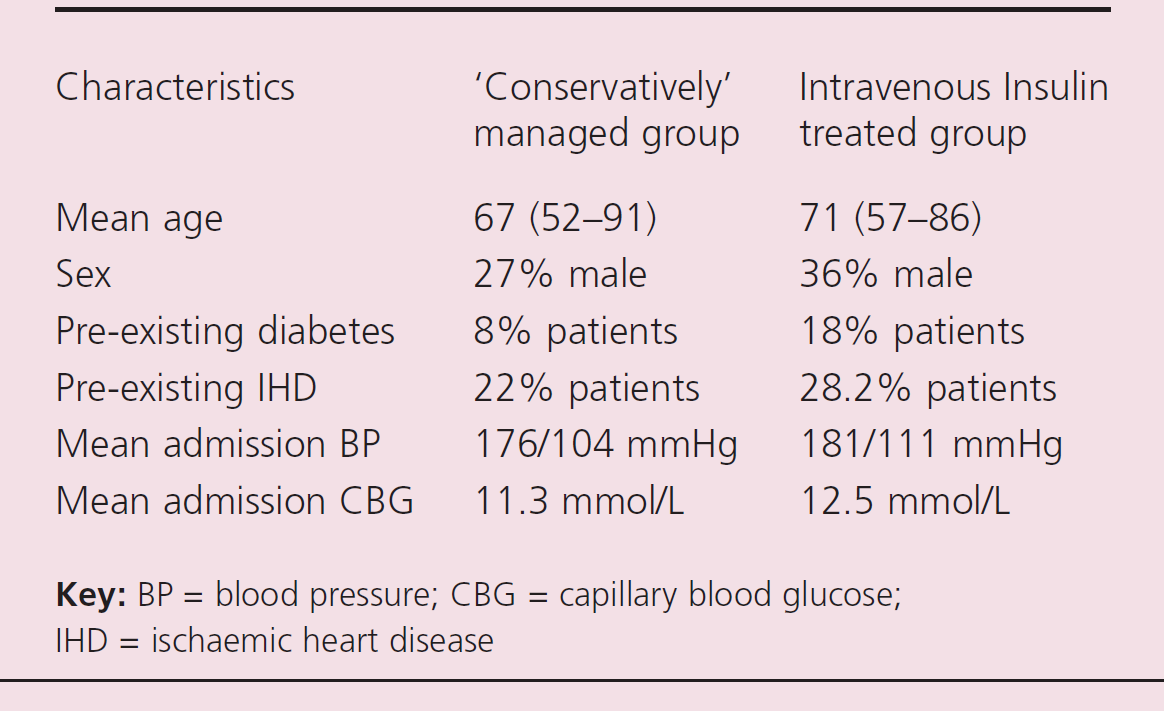
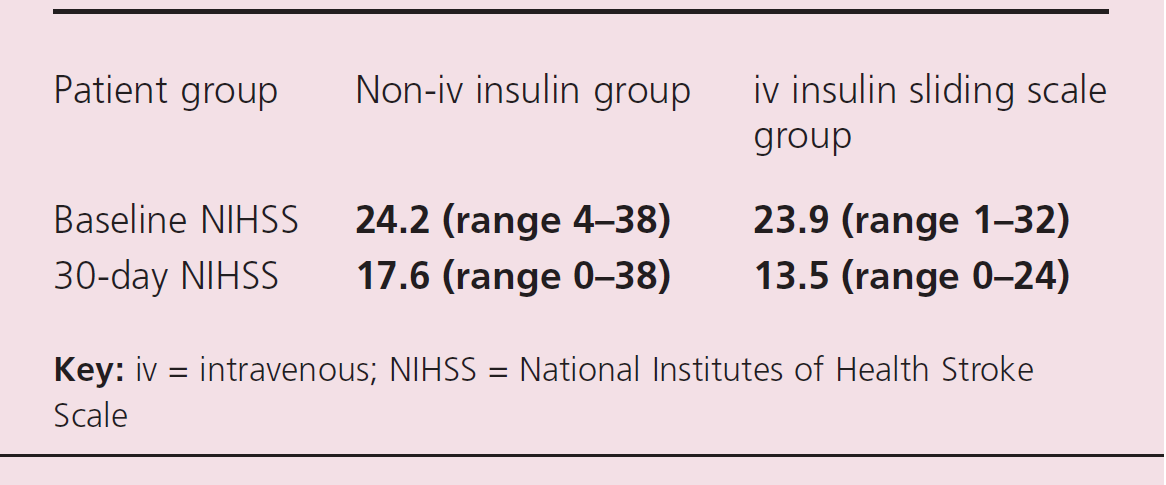
For the 229 patients in this study, 74% (n = 70) had a pre-existing diagnosis of type 2 diabetes. Of the confirmed stroke patients, 53% had admission hyperglycaemia (mean plasma glucose 11.7 mmol/L). Of this group of hyperglycaemic stroke patients only 47% were commenced on an insulin sliding scale within the first 48 hours of admission. The mean plasma glucose level at which this was commenced was 12.5 mmol/L. Observation of the variability in clinical practice produced two distinct groups: acute stroke patients with hyperglycaemia commenced on iv insulin and those without iv insulin. We attempted to determine the effect of sliding scale use on outcomes. Baseline and 30-day NIHSS scores for both groups are shown in table 1.
Demographic/patient data of confirmed stroke patients
Relationship between admission hyperglycaemia and stroke score 30-day outcome in a group of acute stroke patients treated with intravenous sliding scale insulin
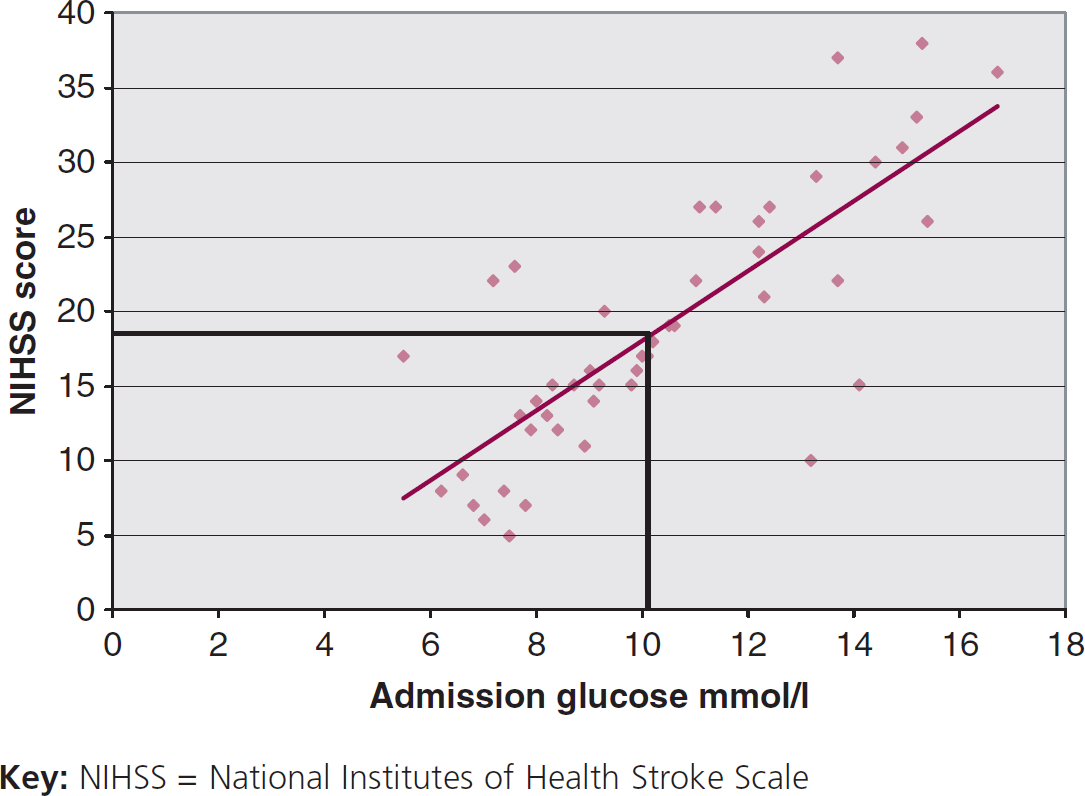
Statistical analysis using paired Student's t-test demonstrates that although baseline stroke scores were similar, there was a significant difference in outcomes after 30 days in the insulin treated group p = 0.041 (95% CI 4–7) compared with the non-insulin treated group. We then went on to statistically determine the specific level of plasma glucose that most benefit may be derived. This was based on the recognised standard that an NIHSS level of ≥ 17 at 30 days carries a worse long-term prognosis. Figure 1 displays graphically the correlation between admission glucose level and NIHSS score. The correlation coefficient of this relationship is r = 0.65 (p = 0.042). Using this linear relationship (worsening glycaemia with worsening outcome) we were able to plot the optimum point at which to initiate iv insulin sliding scale therapy in hyperglycaemic acute stroke patients. This result is plasma glucose of 10.1 mmol/L in our patient group and is slightly lower than previously recommended levels.
A multivariate analysis was subsequently performed on the data and included age, sex, previous diagnosis of diabetes and stroke type. Using chemometrics software for discriminant functions we have shown that the different levels of blood glucose are independent of the above variables (F10,12 = 4,32, p < 0.04). This confirmed the above findings regarding outcomes between the two groups, i.e. hyperglycaemic stroke patients treated with iv insulin have better 30-day stroke outcomes.
The trend line demonstrates correlation between admission glucose level and 30-day outcome. The additional intersecting lines subsequently demonstrate that in terms of using glucose level as a modifiable risk factor, one would need to intervene at a level of 10.1 mmol/L to achieve a NIHSS of ≤ 17 (this being the cut-off for serious impairment/worse function).
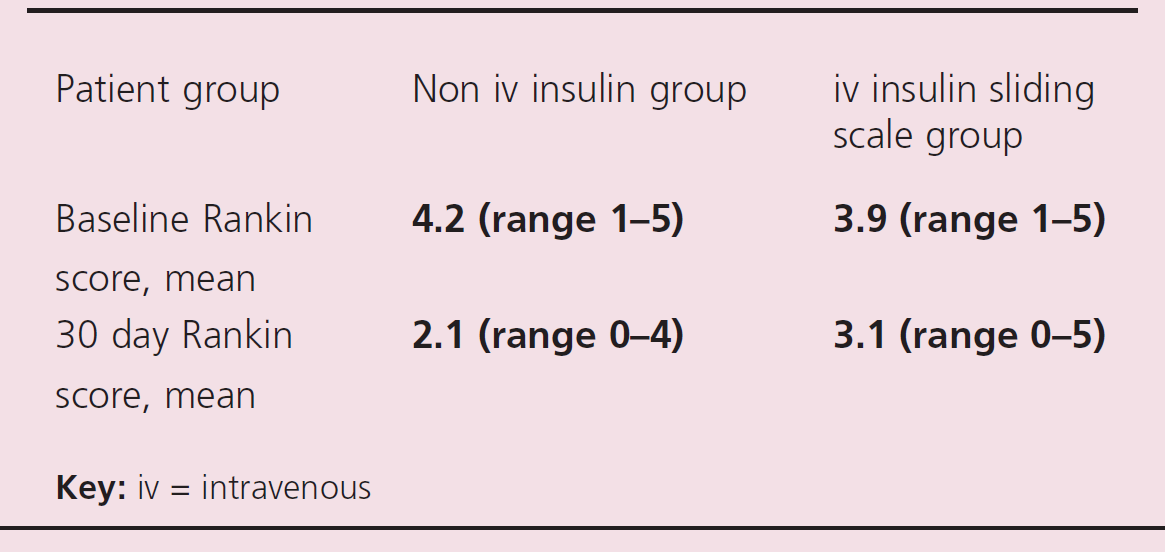
Using the NIHSS as an outcome variable is relatively uncommon; it was used in this study as it offers better granularity when assessing clinical, physical impact. Most stroke studies use the modified Rankin score as an outcome variable (Rankin 0–2, favourable, meaning independent; Rankin 3 or more means unfavourable or dependent). It was originally introduced by Rankin in 1957 14 and modified to its current accepted form by Warlow's group for use in the UK-TIA study. 15 We therefore recalculated the data using the Rankin score and again performed a logistic regression analysis to evaluate the impact of admission blood glucose values on outcomes after 30 days.
Mean NIHSS data for acute stroke patients with hyperglycaemia
Mean Rankin stroke score data for hyperglycaemic stroke patients
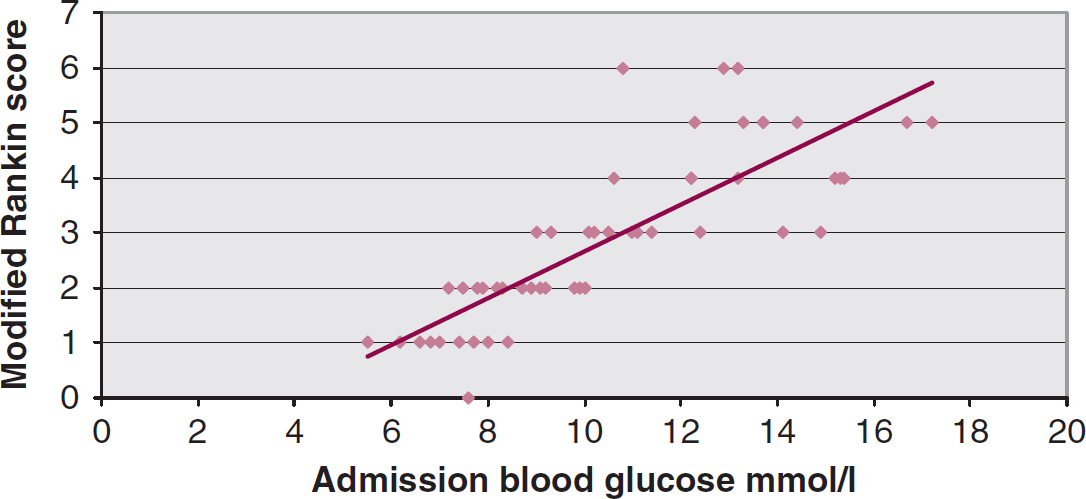
Relationship between admission blood glucose and modified Rankin scale result at 30 days in hyperglycaemic acute stroke patients
Therefore in this second analysis, the correlation coefficient of the trendline is r = 0.71 (p = 0.047) which is confirmed using a logistic regression analysis on SPSS; here the intercept point for better 30-day stroke prognosis (below a Rankin score of 3) is an admission blood glucose of 10.4 mmol/L.
Discussion
Increasing evidence suggests that disordered physiological variables following acute ischaemic stroke adversely affect outcomes. Of these, post-stroke hyperglycaemia is the most frequently recognised abnormality and is documented in up to 50% of patients at the time of stroke presentation. 16 In reversible ischaemia models, hyperglycaemia is associated with lactic acidosis and conversion of penumbral tissue to infarction. 17 Acute hyperglycaemia predicts poor outcome in terms of mortality and functional status even in thrombolysed patients. 18
In trials of the use of iv insulin sliding scales in acute stroke we already know that elevated glucose levels adversely affects outcomes. What we do not know, however, is the appropriate or optimal level at which to initiate treatment. Variation in clinical practice and differing standards of treatment are happening every day in our hospitals as the acute medical on-call rotates a new set of junior doctors through the emergency department and medical assessment unit on a daily basis, all with different practices, knowledge, thresholds for treatment and compliance with stroke care guidelines.
We took advantage of this variability in this prospective, observational study and analysed outcomes consequent to hyperglycaemia treatment (or lack thereof) in a population of acute stroke patients.
Several guidelines, such as the widely used Royal College of Physicians stroke guidelines in the UK, suggest implementing insulin sliding scales when the venous or capillary blood glucose level is ≥ 11.0 mmol/L; this previously was thought to be a rather arbitrary figure. 6 The two groups (treated and untreated, irrespective of whether they had diabetes or not) demonstrate that the untreated patients do significantly worse at 30 days. In reality a randomised controlled trial is needed to confirm this finding. Future trials should have an end-point of 90 days not 30 days, as 90 days is the conventional stroke outcome endpoint in the literature.
Very recent studies looking at tight glycaemic control in acutely unwell patients have confirmed that hyperglycaemia has an effect on both short- and long-term outcomes. 18,19 The caveat, however, is that too tight control is also potentially dangerous, one study by Finfer et al. 20 even reported an increase in mortality by intensive glucose control. This therefore reflects the difficult balancing act that clinicians have to undertake — avoidance of the extremes.
In practice, decisions to initiate insulin will be based on multiple factors other than admission blood glucose; these include use of thrombolysis, nil by mouth status, previous diabetes therapy, concomitant sepsis or cardiac disease.
In our study we sought to correlate admission blood glucose level with a longer term outcome measurement; the NIHSS score is perfect for this. 21 If we take ≥ 17 out of a total of 42 as a marker of worse prognosis then we can translate this back to an average admission glucose score of 10.1 mmol/L. Below this level outcomes are better. Therefore we have shown that this is a suitable glucose level at which to intervene; in practice this means that any acute stroke patient with a plasma glucose of ≥ 10.1 mmol/L needs to start on insulin directly as this appears advantageous. The results of this study need to be disseminated widely to emergency departments and medical assessment units to help reduce the burden of chronic stroke deterioration.
 Key messages
Key messages
Hyperglycaemia in acute stroke is an independent, modifiable risk factor for worse stroke prognosis at 30 days
Insulin therapy should be initiated in acute stroke patients if plasma glucose ≥ 10.1 mmol/L
In conclusion, post-stroke hyperglycaemia represents an important physiological target for acute stroke therapies with potential application across broad time windows, stroke subtypes and stroke severity. We have demonstrated in a prospective study that not only is hyperglycaemia an independent predictor of poor outcome post-stroke but that it is also a modifiable entity and that the limit for initiating intensive glucose control may be lower than previously anticipated. We need to be managing acute stroke patients aggressively in much the same manner as acute myocardial infarction patients. 12 To clarify the optimal blood glucose level and the effects of treatment, a randomised and placebo controlled trial is necessary — such as the encouraging preliminary data from the GRASP pilot. 22 Most clinicians currently do agree that strict glycaemic control for hospitalised stroke patients is associated with improved outcome compared with poor control. Insulin treatment protocols need to be developed and implemented by local multidisciplinary teams to allow for rapid and effective control of hyperglycaemia, supported by the evidence and clinical leadership.
Contributors
P.S.G. and K.A. jointly worked on this study and wrote this report. Data and statistics were reviewed by the clinical governance team at RSCH.
Footnotes
Acknowledgments
Many thanks to Dr Martin Jones and Dr Andrew Smith at Princess Royal Hospital, Haywards Heath.