
Abstract
The increasing prevalence of type 2 diabetes is of great public health concern. In the state of Victoria, Australia, a group-based lifestyle intervention programme, Life! – Taking Action on Diabetes, was developed for people over the age of 50 years who are at high risk of diabetes. It aims to reduce the risk of diabetes by providing practical skills, including goal setting and problem solving, to encourage participants to adopt a healthy diet and active lifestyle. The programme is delivered by specially trained facilitators who have undergone an accredited three-stage training programme. A quality assurance process is also in place to ensure that it is delivered to a consistently high standard. The Life! program is a direct progression from the Finnish randomised controlled trial and the Greater Green Triangle Diabetes Prevention Project implementation trial. This paper describes how a diabetes prevention programme was implemented at a state-wide level and the training of facilitators to conduct the group sessions. Future studies are needed to examine the cost effectiveness and development of specific programmes for diverse population groups.
Abbreviations and acronyms
AUSDRISK Australian Diabetes Risk Test
BMI body mass index
DPS Diabetes Prevention Study
GGT DPP Greater Green Triangle Diabetes Prevention Project
HADS Hospital Anxiety and Depression Scale
HAPA Health Action Process Approach
Introduction
The prevalence of type 2 diabetes is increasing dramatically and is a public health concern worldwide. In Australia, diabetes is the second highest contributor to the burden of disease and is expected to be the leading contributor by 2023. 1 Type 2 diabetes is associated with major health complications including cardiovascular disease, retinopathy, renal failure, neuropathy, and subsequent premature mortality. Clinical trials have consistently demonstrated that lifestyle changes are effective in reducing the risk of developing the condition.2,3 The challenge is to translate diabetes prevention research into ‘real world’ health services implementation.
Life! – Taking Action on Diabetes
In 2007, the Victorian Department of Health launched a programme, Life! – Taking Action on Diabetes, for people over 50 years of age who were at high risk of developing diabetes. The structure of the programme is based on the GGT DPP, which examined the feasibility of a six-session group-based lifestyle intervention in primary care. 3 GGT DPP post-intervention results at 12 months showed significant improvements in weight and waist measurements, glucose and lipid levels, as well as improvements in psychological measures. Using the changes in waist measurements, the reduction in risk of diabetes of participants was imputed from the results of the Finnish DPS and US DPP. It was estimated that the GGT DPP reduced the risk of diabetes by 40%, cardiovascular disease by 16%, and metabolic syndrome from 60% to 45%. 3 While the GGT DPP did not include a control group, the Finnish DPS reported a greater diabetes risk reduction in the intervention group, compared to in controls. 4 The findings from both the DPS and GGT DPP highlighted the benefit of lifestyle interventions in reducing the risk of type 2 diabetes in high-risk individuals. The GGT DPP was developed further for large-scale state-wide roll-out as the programme Life! – Taking Action on Diabetes.
Overview of the Life! program
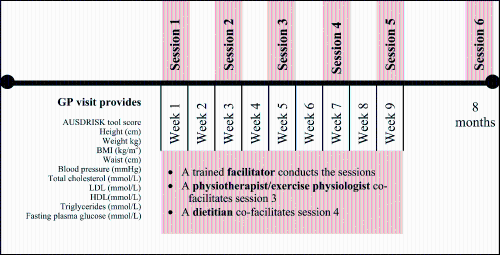
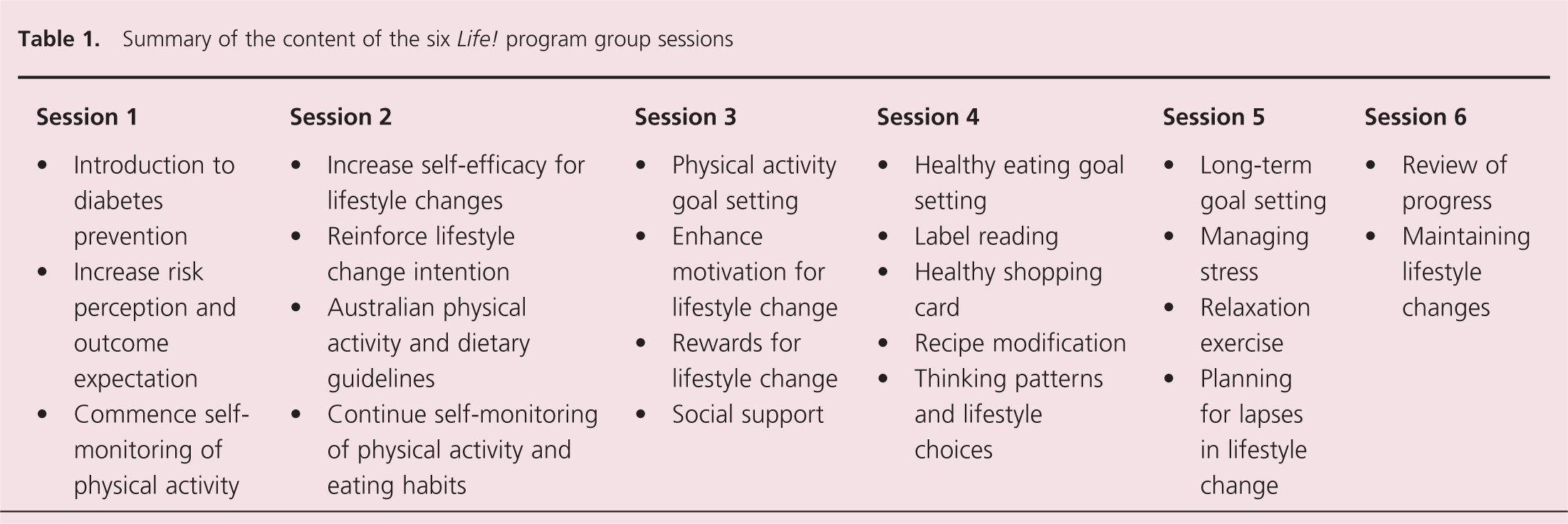
The Life! program was developed using health psychology theories focused on behavioural change, including the HAPA model and self-regulation theory. 5 Its aim is to reduce the risk of developing type 2 diabetes by encouraging participants to adopt a healthy diet and active lifestyle. It consists of six sessions conducted in groups of six to 15 participants with each session lasting 1.5 to 2 hours. The first five sessions are conducted fortnightly, and the final session is conducted 8 months after the first (figure 1). All sessions are delivered by the same facilitator, although dieticians and physical activity experts co-facilitate one session each. The content of the Life! sessions are summarised in table 1.
Overview of the Life! – Taking Action on Diabetes program
Summary of the content of the six Life! program group sessions
Life! referral pathway
Eligibility to participate in the Life! program is based on the AUSDRISK. 6 Individuals over the age of 50 years who have a score of ≥ 15 on the AUSDRISK are considered to be at high risk of developing diabetes and are eligible for the group sessions. All participants entering a Life! course must have diabetes excluded, usually by a general physician, and a referral form completed. Specific details relating to referral pathways have been given elsewhere. 7
Characteristics of Life! participants
The characteristics of participants who entered the Life! program in the first 21 months are presented in table 2. The average score on the AUSDRISK was 19.7, indicating a high-risk group, i.e. approximately one in seven individuals is expected to develop diabetes within five years. The majority of participants were women (63%), and the median age for both males and females was 64.0 years. Participants were largely English speaking from an Australian cultural background (79.6%), not currently working or retired (32%) and in the low-medium income bracket (80%).
Characteristics of participants enrolled in the Life! group sessions within the first 21 months
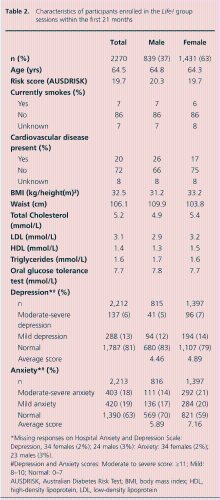
Missing responses on Hospital Anxiety and Depression Scale: Depression, 34 females (2%); 24 males (3%): Anxiety: 34 females (2%); 23 males (3%).
Depression and Anxiety scores: Moderate to severe score: ≥11; Mild: 8–10; Normal: 0–7
AUSDRISK, Australian Diabetes Risk Test; BMI, body mass index; HDL, high-density lipoprotein; LDL, low-density lipoprotein
Overall, 20% of participants reported a history of cardiovascular disease. Over half of those enrolled in the programme (56%) were obese (BMI > 30) and the average waist circumference was > 103 cm for females and > 109 cm for males. Using the HADS at the first Life! session, 37% of all participants reported higher than normal levels of anxiety and 20% reported higher than normal levels of depression. Previous research using the HADS to investigate levels of depression and anxiety in an Australian sample found that 11% reported higher than normal levels of anxiety and 8% higher than normal depression. 8 The higher than expected rates of depression and anxiety among the Life! participants suggests a need for a research and clinical focus on psychological health for individuals at high risk of developing diabetes.
Facilitator training
The results of clinical trials aimed at examining the effectiveness of diabetes prevention programmes have provided evidence for their success,4,9 but there is limited information on the training provided for health professionals facilitating these prevention programmes or the evaluation of the training programmes. Based on findings from focus groups, Kreinter and colleagues 10 reported that the key competencies required for professionals working in chronic disease prevention included a thorough understanding of the disease being targeted, analytical knowledge, critical thinking and communication skills. Furthermore, providing information to patients and increasing motivation are perceived to be the main responsibilities of health professionals in the treatment of lifestyle-related diseases. 11 Interestingly, the provision of information is not seen as a significant barrier to the treatment of chronic disease, unlike enhancing patient motivation. 11 The ability to focus on motivation is an important skill for facilitators of chronic disease prevention programmes because assisting people to maintain their motivation is more successful in behaviour change than traditional advice giving. 12
The Life! facilitator training programme
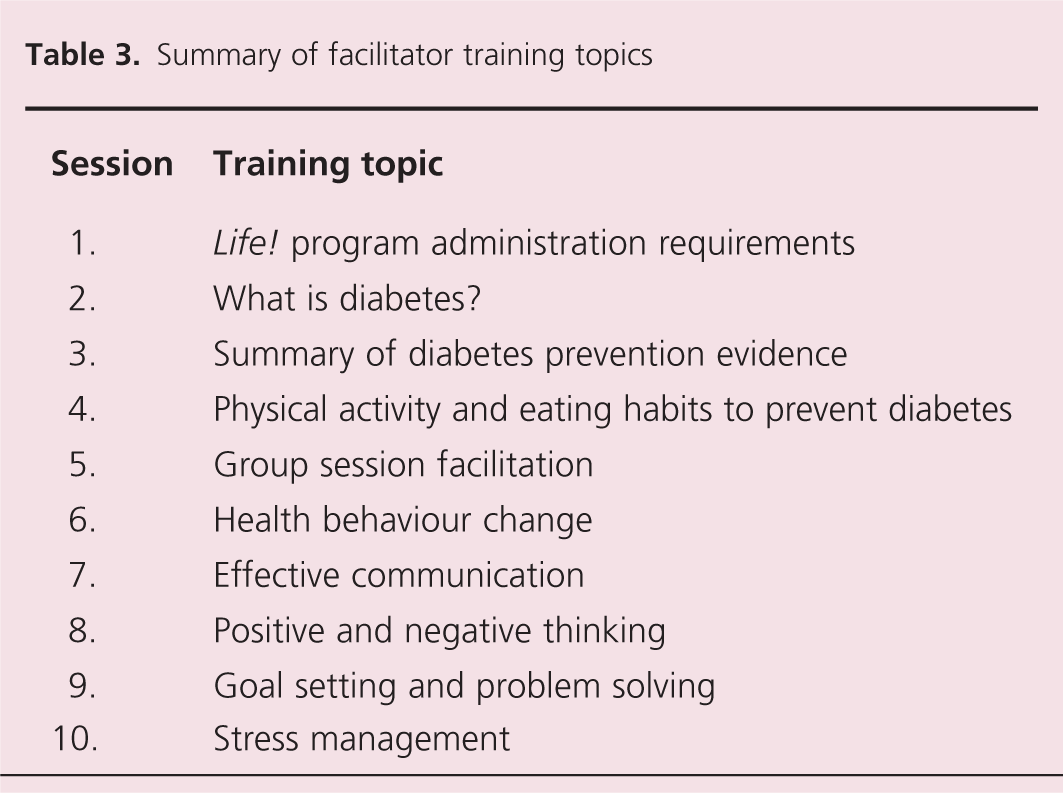
The Life! program is facilitated by health professionals who have undergone a three-part training programme. To be eligible to attend, candidates require registration with a recognised organisation for health professionals (e.g. nursing, psychology). All stages of the facilitator training are underpinned by adult learning principles and, as such, the training is self-directed, collaborative, builds on prior experience, and objectives are tailored to cater for different learning styles. 13 The specific training objectives and outcomes, together with associated course materials (e.g. DVDs, manuals and workshop activities) focus on 10 training topics (see table 3).
Summary of facilitator training topics
Overview of the training programme
The Life! training consists of three parts: (a) an orientation session; (b) a self-learning period; and (c) a face-to-face two-day workshop.
Part 1: Orientation session
The orientation session provides an opportunity to explain the operational aspects of being a Life! facilitator, including the service agreements and record keeping. In addition, information about the referral pathways, recruitment and availability of resources is provided. The self-learning tasks and pre-training questionnaires, which form part of the self-learning period, are also distributed at the orientation session.
Part 2: Self-learning period
The self-learning period is a prerequisite to attending the two-day workshop. Its purpose is to provide facilitators with the opportunity to improve their knowledge of diabetes and to familiarise themselves with the Life! participant activities. During this period facilitators are required to complete a number of self-learning tasks, including reading the facilitator manual and undertaking some of the Life! participant activities (e.g. AUSDRISK test, goal-setting activities and complete nutritional and activity diaries). In addition, all trainee facilitators are required to complete a pre-training questionnaire and an online open-book multiple choice test.
Part 3: Two-day training workshop
Once trainees have achieved a satisfactory standard on the self-learning tasks, they are invited to attend the two-day workshop. The workshop is conducted in groups of ≤ 30 with one lead trainer. About six to seven trainees are placed with a group facilitator at circular tables. The aim of the workshop is to develop trainees’ facilitation skills, as well as to rehearse Life! sessions.
Effectiveness of the training programme
To evaluate the effectiveness of the Life! training programme, pre- and post-training questionnaires were developed to assess facilitator knowledge of diabetes prevention and confidence in facilitating group sessions. Analysis of 175 trainee facilitators revealed a significant improvement in self-rated diabetes knowledge and confidence in group facilitation after completing the training. Most of the trainees (93%) rated the self-learning period as ‘moderately useful’ or ‘very useful’, and 89% strongly agreed or agreed with the statement ‘overall the training course was worthwhile’. 14 The training structure and content may be useful for training health professionals in related programmes using lifestyle modification interventions.
Quality assurance
An important component of any training is the quality assurance process. The Life! facilitator training programme has incorporated an annual professional development and review day that active facilitators are required to attend to maintain their certification. The professional development and review day provides an opportunity for facilitators to receive feedback about conducting the sessions and suggestions for improvement.
If facilitators do not complete at least two Life! courses after undertaking the facilitator training programme, they are required to participate in a one-day refresher course to ensure that their knowledge and facilitation skills are maintained.
This development process has been well received by facilitators, with all key aspects of the day consistently being rated highly (average > 7 out of 10). These review days are seen as an important opportunity to network and share experiences with other facilitators.
Conclusions
In Victoria, Australia, a large-scale state-wide diabetes prevention programme, Life! – Taking Action on Diabetes, has been implemented for high-risk individuals. Life! progressed directly from the Finnish randomised controlled trial and GGT DPP implementation trial.3,4 It is a unique methodological pathway from randomised trial through implementation trial to full scale roll-out. The content of the Life! group sessions was developed using health psychology theories of behaviour change, and is underpinned by adult learning principles.5,15 A number of lessons have been learnt in the development of the programme. It is important that the training programme and recruitment proceed in step with each other. Many diabetes prevention programmes have experienced difficulty recruiting. Too few trained facilitators may result in participants waiting too long for the intervention, whereas too few participants may result in newly trained facilitators unable to gain sufficient practice to maintain their skills. The training programme has been crucial in transferring the successful approaches of the GGT DPP to Life!. Linking the quality assurance programme to the training programme through review days has created a self-improving programme in which the performance of Life! is known in many aspects to stakeholders, including facilitators, service providers, and the primary funder, the Victorian Department of Health. 7 Through each facilitator knowing about their individual performance and the performance of the overall programme, there are opportunities to learn and improve at professional development review days. By spreading the good practices of the best performers it is expected that the rogramme will continue to improve. It is unknown whether scaled-up diabetes prevention programmes can achieve the results of randomised controlled trials particularly since they have problems of context and resource, but the methodology of linking training to quality assurance is the best chance.
Questions remain about how best to scale-up diabetes prevention programmes. In seeking to do the ‘greatest good for the greatest number’ we need to examine whether the programme has to be delivered by health professionals or whether it could be delivered by lay facilitators. Also one can impute from the results of European and American diabetes prevention programmes that there is a clear relationship between the number of sessions attended and reduced risk of progression to diabetes. In other words, we need a number of cost-effectiveness studies to assess different models before we are able to answer the question about the ‘greatest good for the greatest number’. There has been great progress since the publication of the Finnish and US randomised controlled trials of diabetes prevention but much remains to be discovered about scaling-up these programmes to regional and national levels.
There are two remaining developmental requirements of diabetes prevention programmes: adaption for women who have had diabetes in pregnancy and people of culturally diverse backgrounds. About 80% of women who had gestational diabetes will develop type 2 diabetes. Several ethnic groups in Australia have cultural factors that make uptake of physical activity and dietary advice different from participants in the mainstream programme. Adaptations need to recognise the specific enablers and barriers and for these to be reflected in the training of the facilitators, quality indicator measures and the course materials for participants. Adaptation for specific groups requires rigorous experimental design and assessment. This work is now underway.
Key messages
The Life! – Taking Action on Diabetes program was launched in Victoria, Australia, to reduce the risk of developing diabetes among high-risk individuals
To ensure that the Life! program is delivered to a high standard, facilitators are required to undergo a three-stage training programme and participate in a structured annual quality assurance process
Future studies are needed to examine the cost effectiveness of large-scale diabetes prevention programmes
Specific programmes are needed for high-risk groups including women with gestational diabetes and people of culturally diverse backgrounds
Footnotes
Acknowledgements
Funding for Life! – Taking Action on Diabetes was provided by the Victorian Department of Health.