
Abstract
Current evidence shows that type 2 diabetes can be effectively prevented and delayed by lifestyle modification. After careful development and pilot testing, a rigorous evaluation of such programmes is crucial to assess their effectiveness prior to large scale implementation. Integrating the patient perspective in this evaluation is essential. In principle, Patient-Reported Outcomes (PRO) questionnaires can address this key question. However, researchers and clinicians lack a clear framework to make a sound selection of appropriate measures among the large set of possible questionnaires. As a consequence, it is unclear what is the most useful information to be captured from patients when assessing a new programme, so that it can be determined whether the programme can be generalised to a larger population: is it health-related quality of life, satisfaction or something different which could predict the long-term success of the programme? We recommend a specific approach, better adapted to the nature of the intervention, and suggest a selection of a few existing PRO measures that could satisfy the requirements.
Keywords
Abbreviations and acronyms
ADS Appraisal of Diabetes Scale
ATT Psychological Adjustment to Diabetes Scale
DES-SF Diabetes Empowerment Scale, Short Form
DMSES Diabetes Management Self-Efficacy Scale
HbA1c glycated haemoglobin
HCP healthcare professional
MEI Motivation and Energy Inventory
PAID Problem Areas in Diabetes
PRO Patient-Reported Outcomes
ProQolid Patient-Reported Outcome and Quality of Life Instruments Database
Introduction
Type 2 diabetes has reached epidemic proportions throughout the world. In 2010, approximately 285 million people worldwide had diabetes; this number is projected to increase to 438 million by 2030. 1 Major prevention studies have shown that diabetes can be effectively delayed or prevented in individuals with impaired glucose tolerance using lifestyle intervention and/or treatment.2-4 We have learned from these studies that sustained changes in lifestyle in terms of physical activity and diet are crucial for successful type 2 diabetes prevention. Despite evidence of their effectiveness, it is questionable whether implementing diabetes prevention programmes is feasible at a population level.5,6 Economic evaluation has demonstrated the cost effectiveness of primary prevention of type 2 diabetes using lifestyle interventions. 7 However, effective implementation of diabetes prevention programmes into clinical practice remains challenging and requires significant financial and human resources. 6
Rigorous scientific evaluation of the programmes, prior to large scale implementation, is fundamental for demonstrating programme effectiveness and feasibility, determining whether or not they are cost effective and providing information for improving existing programmes and designing new ones. Lifestyle modification programmes are usually evaluated through randomised controlled trials that compare the effects of the lifestyle programme versus standard diabetes education using objective measures such as HbA1C, weight reduction and exercise measurement. Unfortunately, many of these evaluation studies do not integrate the patient perspective in their measurement; however, this perspective is fundamental to fully understand the benefits of the intervention programme for patients, increase patient engagement in their care and, ultimately, to maintain behaviour change. Incorporating well-designed PRO instruments is the best way to assess the effect of intervention from a patient perspective. 8 However, to be credible measures, PRO instruments have to be developed and validated following a rigorous and standardised process as recommended in recent US Food and Drug Administration guidelines 8 and a European Medicines Evaluation Agency reflection paper. 9
This paper addresses two questions, firstly what are the relevant outcomes of diabetes lifestyle intervention programmes from a patient perspective, and secondly what are the most appropriate existing PRO instruments to assess these outcomes?
Assessing diabetes lifestyle programmes from a patient perspective
To successfully assess the outcomes of lifestyle intervention programmes from a patient perspective, relevant key patient outcomes most attributable to the programme must first be identified, followed by a critical review of PRO instruments that would best allow their measurement.
Key patient outcomes should be identified with careful consideration of the programme-based theory, the programme objectives, the expected outcomes perceptible by patients, and the target population.
The identification and selection of PRO instruments should then follow a structured approach:
identification of PRO instruments from a literature review and consultation with experts;
development of appraisal criteria from published documents on the development and validation of health status measures10,11 and with expert psychometric advice;
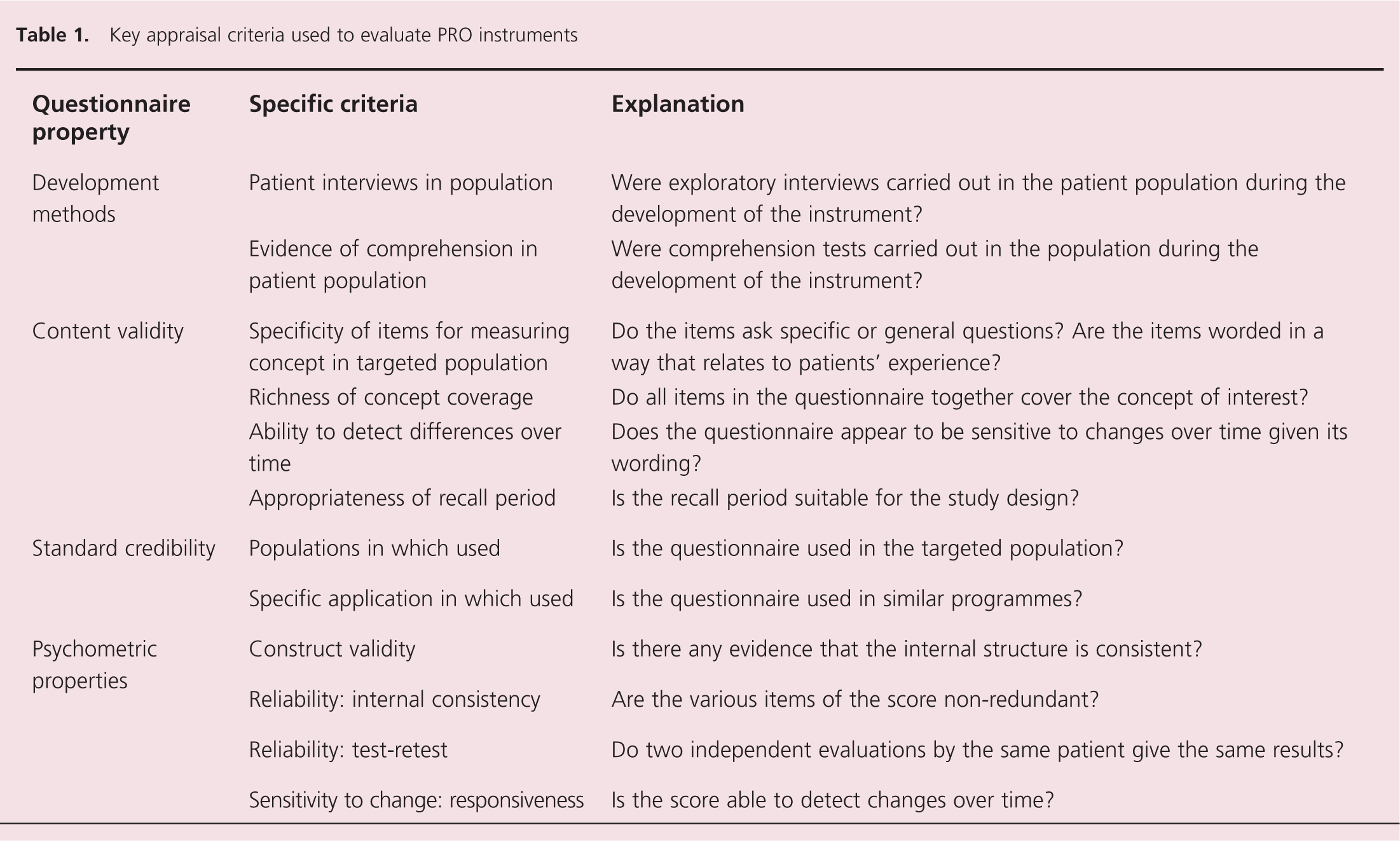
critical appraisal of the identified instruments for relevance, content validity and credibility of quantitative and qualitative methods used for its development and validation. The key appraisal criteria are summarised in table 1.
Key appraisal criteria used to evaluate PRO instruments
Question 1: What are the relevant outcomes of diabetes lifestyle programmes from a patient erspective?
For diabetes lifestyle modification programmes based on empirically-supported theoretical models such as Prochaska’s transtheoretical model of behaviour change, 12 the behavioural change theory should drive the hypotheses to test for programme evaluation. Prochaska and DiClemente suggest that behavioural change occurs in five distinct stages (precontemplation, contemplation, preparation, action and maintenance) and that movement through these stages is a cyclical or spiral process that involves both progress and periodic relapse. The stabilisation of behaviour change and the avoidance of relapse are characteristic of long-term maintenance of lifestyle behaviour change.
Such transtheoretical model-based lifestyle interventions in diabetes aim to:
prepare and motivate patients for taking an active role in changing their lifestyle (preparation phase);
support them in making good choices and positive changes in their lifestyle (action phase);
support them in maintaining behaviour change (maintenance phase). These interventions are generally proposed to patients ready to change their lifestyle (patients in the preparation or action phases).
In this context, the key patient-relevant outcomes identified as most predictive of such programme success and sustained behaviour change are psychological adjustment to diabetes, motivation to change and self-efficacy.
Psychological adjustment is the mental response of a person to a dreadful life situation. This concept covers the cognitive and behavioural strategies patients may use to deal with and manage their disease. 13 A positive change on psychological adjustment to diabetes is expected as a result of lifestyle modification programmes.
Motivation is the psychological feature that stimulates a person to action toward a desired goal. Motivation plays an important role in successful behavioural change 12 and is thus identified as a key concept to evaluate the benefit of a lifestyle programme on patients.
Self-efficacy is a person’s perception of their ability to plan and take action to reach a particular goal. 14 Self-efficacy was identified as a key concept in order to document and monitor patients’ perceptions of their ability to plan and take action to reach their goals, in this case, eating a healthy diet and increasing physical activities.
Question 2: What are the most appropriate PRO instruments to assess lifestyle programmes in type 2 diabetes?
PRO instruments were identified using ProQolid and published literature reviews.15,16 The search was supplemented with instruments recommended by clinical and PRO experts.
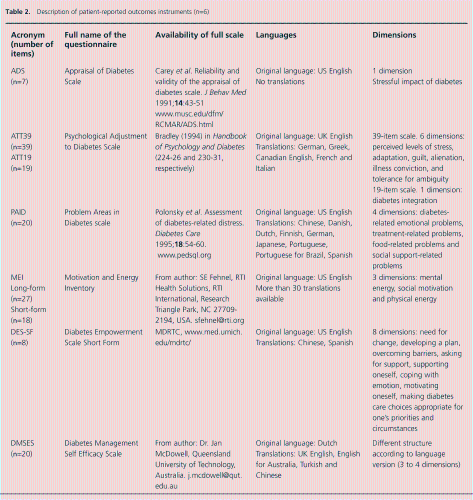
Of the numerous questionnaires identified, only six instruments were found that addressed psychological adjustment, motivation and self-efficacy and had documented evidence of development methodology and psychometric properties. Three of these assessed indicators of psychological adjustment: the PAID scale,17-19 the ADS 20 and the ATT-39/ATT-19.21,22 One measure assessed motivation: the MEI. 23 Two measured self-efficacy: the DES-SF24,25 and the DMSES.26-29 These instruments are briefly described in table 2.
Description of patient-reported outcomes instruments (n=6)
Measures assessing psychological adjustment
Of the three measures of psychological adjustment, only the PAID satisfies all criteria. The PAID demonstrates evidence of adequate psychometric testing, responsiveness to change through similar educational intervention19,30-32 and appropriateness to the targeted type 2 diabetes population. In addition, patients were involved in its development and comprehension testing. The ADS and ATT-39/19 are acceptable tools and meet all except one or two key appraisal criteria. The ADS has interesting content; however, its development did not involve patients and no responsiveness and sensitivity to change data following similar educational interventions are available. The ATT-39 is relatively long (39 items), which can be a burden for patients; it has an item scaling that is often criticised, as respondents are faced with cognitively complex tasks (such as disagree that weight-control is not a problem for them). The ATT-19 is at a relatively early stage of development and more information is needed to assess its sensitivity to detect change in patient psychological adjustment following educational intervention.
Measures assessing motivation
The MEI instrument is the only identified instrument that assesses motivation. It is created to be both responsive to treatment effects and able to discriminate among patients with different clinical characteristics. 23 Although the MEI was developed through focus groups and cognitive interviews with individuals being treated for depression, all items are carefully worded to be applicable across various populations, including diabetes patients. The MEI short form, with a recall period of the previous 7 days, is expected to be sensitive to behavioural modification programmes and can be used to compare the motivation levels of type 2 diabetic patients over the course of lifestyle intervention programmes.
Measures assessing self-efficacy
Two potential candidates to assess self-efficacy were found and meet most of the appraisal criteria: the DES-SF and the DMSES. Although the DES-SF offers comprehensive and coherent coverage of the self-efficacy concept and shows interesting results in educational programme assessment,33-35 the item wording and the item scaling are complex and require considerable cognitive effort from the patients to answer the questions. The DMSES is preferred for its simplicity, although further research on this instrument is warranted to assess its responsiveness over time. This instrument showed a small improvement in confidence in self-care following an educational intervention in primary care in patients with type 2 diabetes. 32
Conclusion
Health-related quality of life, patient satisfaction, and patient adherence to treatment are important PROs that should improve when using well-designed lifestyle modification programmes. However, when assessing the effectiveness of a new programme, the primary focus of assessment should be measurable observable changes at the patient level, which are specific and direct outcomes of the intervention.
Psychological adjustment, motivation and self-efficacy are key patient-relevant concepts to consider when evaluating transtheoretical model-based lifestyle interventions in diabetes from a patient perspective. Specific validated instruments exist, which reliably assess these key concepts. Of the instruments identified in our work, the PAID, the MEI and the DMSES questionnaires are the best existing candidates to assess psychological adjustment, motivation to change and self-efficacy, respectively.
After evaluation, programmes that have shown beneficial effects at patient level and that have proved to be well-designed and cost effective can be generalised and implemented in clinical practice settings. Indeed, setting goals, providing patient education for achieving these goals, and monitoring the patient’s progress using PRO instruments adapted to the context of clinical practice, are critical in clinical practice for maintenance of healthy behaviours, as well as supporting patient adherence and persistence to pharmacological therapies.
Key messages
Integrating the patient perspective into lifestyle rogramme evaluation is fundamental to demonstrating the benefits of the programmes for patients. It also provides valuable feedback for HCPs and helps them collaborate with patients to manage diabetes over the course of the disease
Key patient-relevant concepts of greatest interest for lifestyle programme evaluation from a patient perspective are psychological adjustment to diabetes, motivation to change and self-efficacy
Among existing, well-validated instruments, the PAID, MEI and DMSES scales appear to be the instruments of choice to assess the effect of type 2 diabetes lifestyle programmes on patients’ behaviours and perceptions