
Abstract
The prevalence of metabolic syndrome was determined as a cross-sectional study among 600 healthy Saudi adults (52% males and 58% aged 35–50 years) attending National Guard clinics using the definition proposed by National Cholesterol Education Program Adult Treatment Panel III. The prevalence of metabolic syndrome was 21%. Only one third of the participants had normal weight (body mass index = 18.5–24.9). Central obesity based on waist circumferences was noted in 21% of males and 22% of females. Low high-density lipoprotein-C showed the highest prevalence (29%) followed by high triglyceride (24%). About 14% of participants had impaired fasting blood glucose (≥ 110 mg/dl). Only 6% had high blood pressure (≥ 130/85 mmHg). More than three quarters (77.3%) of the respondents had
Abbreviations and acronyms
BMI body mass index
CI confidence interval
CVD cardiovascular disease
FBG fasting blood glucose
HDL high-density lipoprotein
NCEP-ATP III National Cholesterol Education Program – Adult Treatment Panel III
OR odds ratio
Introduction
The metabolic syndrome is a cluster of risk factors that predispose to CVD morbidity and mortality. 1 Metabolic syndrome is associated with a three- to fivefold greater risk for the development of type 2 diabetes. 2 Based on the NCEP-ATP III diagnostic criteria for metabolic syndrome, 3 there was a 24% prevalence among adults in the USA. 4 In the Gulf region, the prevalence estimates are 21% in Oman 5 and 18% in Kuwait 6 . In Saudi Arabia where the economic and social changes have brought sedentary lifestyle changes the prevalence of obesity is increasing and estimates of metabolic syndrome vary from 20.8–39.3%.7-9 Here we determine the prevalence of metabolic syndrome and individual risk components among healthy Saudi adults attending National Guard clinics in the Western Region.
Methods
A randomised cross-sectional study between January and December 2010 included Saudi adults aged between 20 and 50 years who attended for routine check up at our clinics in Jeddah. Attendees with any chronic illness and pregnant females were excluded. The subjects were National Guard employees and their dependants. Sociodemographic characteristics, relevant history, physical examination and laboratory investigations were undertaken.
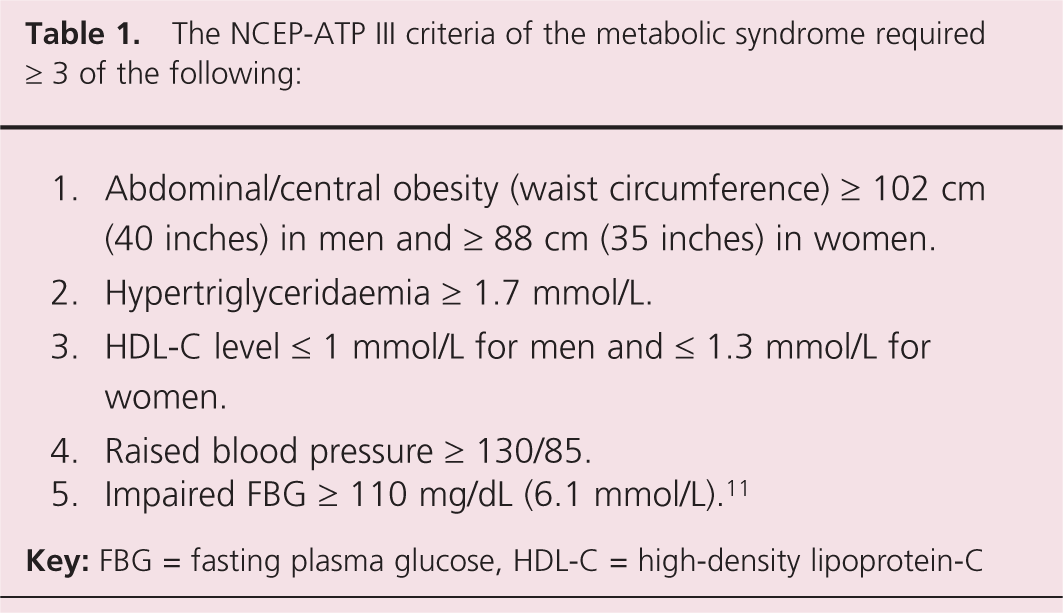
The cut points for the components of metabolic syndrome and mandatory inclusion criteria required for a diagnosis vary between definitions of the syndrome. 10 In the present study we elected to use NCEP-ATP III criteria to define metabolic syndrome (table 1). 11
The NCEP-ATP III criteria of the metabolic syndrome required ≥ 3 of the following:
A venous blood sample was taken in the morning, after a 12-hour fast, to determine plasma glucose, triglycerides, total and HDL cholesterol concentrations.
Blood pressure was measured with a standard mercury sphygmomanometer on the left arm after at least five minutes of rest. Mean value was determined from two independent measurements. Waist circumference was measured midway between the iliac crest and the lower costal margin. Body weight and height were recorded in light clothes and no shoes. BMI
Data analysis used the Statistical Package for Social Sciences (SPSS) version 14. Student t-test, Chi-square test, ANOVA test and binary logistic regression tests were used to determine the gender differences in the prevalence of metabolic syndrome and the predictors contributing for its occurrence. The level of significance was p<0.05, at 95% CI. Ethical approval and patients’ informed consent were obtained.
Results
A total of 600 healthy adults were enrolled. The sociodemographic and metabolic syndrome characteristics are shown in table 2. The prevalence of the risk factors and biochemical indices for diagnosing metabolic syndrome according to NCEP-ATP III criteria are illustrated in figure 1; 21% of patients had
Distribution of metabolic syndrome among participants according to their characteristics and habits.
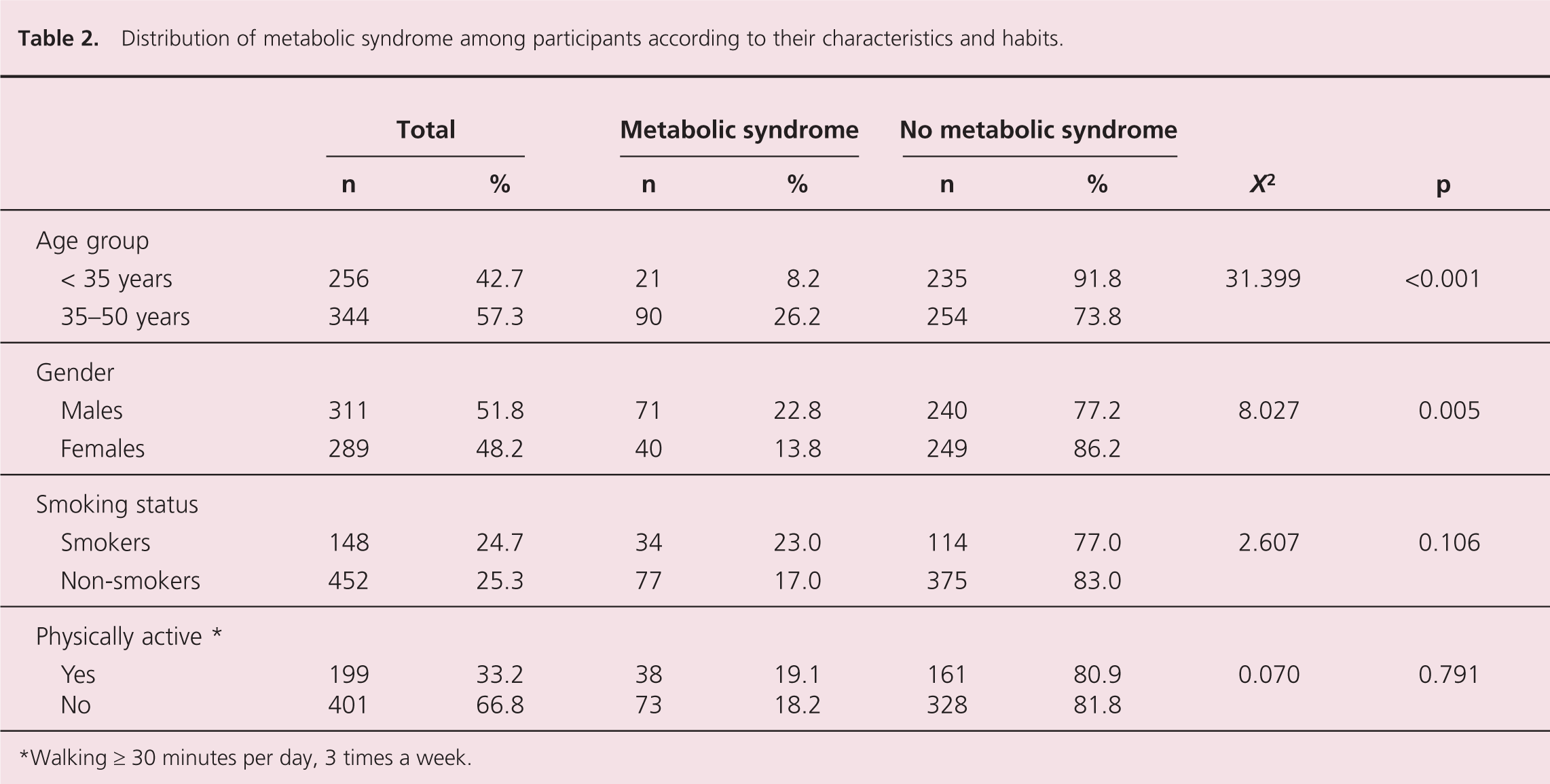
Walking ≥ 30 minutes per day, 3 times a week.
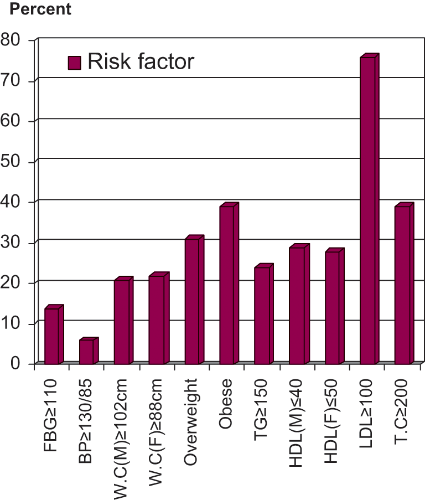
Prevalence of components of metabolic syndrome among study participants
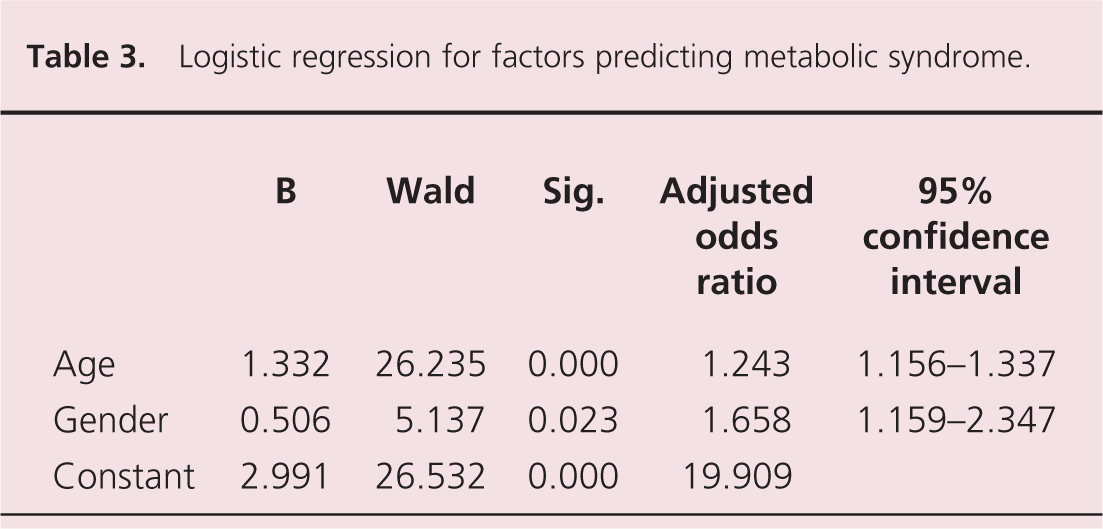
Logistic regression for factors predicting metabolic syndrome.
Discussion
A prevalence of metabolic syndrome of 21% among healthy adults in the western region of Saudi Arabia was considered similar to those observed in other studies in the Gulf region.5-7 The prevalence was 20.8% among Saudi soldiers 7 and 21% in healthy adults in Oman and 18% in Kuwait (by ATP III criteria).5,6 However, an overall age-adjusted prevalence of 39.3% was reported in a community-based epidemiological survey of > 17,000 Saudi subjects aged between 30 and 70 years. 8 This study also used ATP III criteria, but it was undertaken in the general population rather than only among healthy subjects. It also noted a significantly higher prevalence of metabolic syndrome among subjects from urban areas (44.1%) than those living in rural areas (35.6%) We, like Barrimah et al., 9 noted that about 20% of our study population had two ATP-III risk factors putting them at greater risk of developing metabolic syndrome and cardiovascular disease. The prevalence of metabolic syndrome was higher with age and male gender, which is consistent with other studies.9,12,13
More than 20% of our participants had central obesity and 70% were overweight or obese. Dyslipidaemia was also very common (figure 1), consistent with a lack of exercise, with only one third of participants undertaking regular exercise. The prevalence of metabolic syndrome in the general Saudi population cannot be estimated based on our study, since the participants were National Guard employees and their dependants. They generally have good incomes and a more sedentary lifestyle which negatively influences most components of metabolic syndrome.
Key messages
Adoption of healthy lifestyles should be encouraged
Presence of a metabolic syndrome component should increase vigilance for the presence of other components
Early detection and treatment should reduce morbidity and premature mortality
Footnotes
This work received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
The authors declare that they have no conflicts of interest.