
Abstract
Background:
Diabetes prevalence in Scotland is increasing at approximately 4.6% annually, with figures currently at 247,278 (4.7%). Internet-based interventions have the potential to enhance self-management and shift the balance of power towards the patient. Electronic personal health records (ePHRs) have been identified as an ideal route to deliver these interventions, as outlined in the Department of Health Information Strategy.
Methods:
We developed a diabetes-focused, population-based ePHR for NHS Scotland. Data are sourced from primary, secondary and tertiary care via the national shared-electronic record, SCI-DC. Data are displayed alongside lay-descriptions and information links tailored to the patient’s needs.
Results:
3,391 individuals have registered to access their clinical data. In this largely self-selecting group, 31% have type 1 diabetes and 61% are male. 2,015 have completed the enrolment process and 861 have successfully logged in. By the end of 2012, the number of distinct users per month had risen to nearly 300.
Conclusions:
The system is now a useful additional component for the self-management of diabetes. Although the system has been developed for, and by, stakeholders from across Scotland, it has the potential to connect to any electronic medical record. The current project is expected to reach over 5,000 patients by the end of 2013.
Abbreviations:
CAS Citizen Account Service
ePHR electronic personal health record
MDMW My Diabetes My Way
PHR personal health record
SCI-DC Scottish Care Information – Diabetes Collaboration
Background
A recent report in Diabetic Medicine 1 predicts that NHS annual spending on diabetes will increase from £9.8 billion to £16.9 billion over the next 25 years (17% of the entire NHS budget). A focus on early management and complication prevention could therefore have a huge economic impact. In its report ‘Delivering for Health’, NHS Scotland set out a fundamental shift in its health delivery strategy, focusing on providing care which is quicker, more personal and delivered closer to home. 2
The prevalent national diabetes population of Scotland has increased from 103,835 (2%) in 2002 to 247,278 (4.7%) in 2011. 3 The Scottish Diabetes Action Plan 4 and the Healthcare Quality Strategy for NHS Scotland 5 emphasise the importance of ‘putting people at the heart of the NHS’, with high quality, evidence based and patient-focused care. 6 In reality, healthcare provision is organised around healthcare staff availability with little support between infrequent clinic appointments.
The internet and electronic personal health records have the potential to change the balance of power from healthcare providers to health care users and reduce the burden of care by engaging patients in managing their own health and illness.7,8 Interactive behaviour change technology and online tools can be a cost effective option for the management of people with diabetes.9-11 At least 80% of households in the UK have internet access, with further growing trends in the use of mobile devices. 12 Despite demands for innovative technology within healthcare and great potential to empower patients, 13 it is currently underdeveloped and under-utilised.
Personal health records have been defined as:
an electronic application through which individuals can access, manage and share their health information in a secure and confidential environment
14
a tool for collecting, tracking and sharing important, up-to-date information about an individual’s health or the health of someone in their care
15
While there is no universal agreement in these definitions, they contain broadly similar themes: focusing on data repositories that can be used to securely store and manage personal medical information. These data repositories can be further classified into three distinct sub-categories based around their integration and communication with provider systems:
stand-alone: solely patient-recorded and maintained
tethered: a read-only link to an electronic medical record
integrated: asynchronous communications to/from an electronic medical record.
The Department of Health Information Strategy 16 aims to allow access to general practitioner records for patients by the end of 2015. EMIS Access 17 and Renal PatientView18,19 allow access to a subset of clinical data from primary and secondary care respectively. Kaiser Permanente’s My Health Manager 20 is one of largest and most advanced patient access systems. It has reported significant decreases in primary care office visits and telephone contacts 21 .
These and most existing PHR systems focus on single silos. Until now, there have been no systems worldwide offering a fully population-based, focused ‘shared electronic record’ for diabetes.
Methods
SCI-DC 22 is a real time web-based clinical information system, supporting the care of all people with diabetes in Scotland. Launched in 2002, the SCI-DC team have demonstrated sustained development and implementation of clinically useful tools for the care of people with diabetes in Scotland using data captured from approximately 1,050 general practices, 40 hospital clinics, screening services and laboratories across Scotland. SCI-DC supports inter-disciplinary team-working, patient education, professional education, a national retinal screening programme and a suite of audit functionality for individual, practice, regional and national reporting. It is the main source of data for the annual Scottish Diabetes Survey, 3 but prior to this new development, this rich information resource has only been accessible by members of the healthcare team.
MDMW (www.mydiabetesmyway.scot.nhs.uk) 23 was launched in October 2008 as the NHS Scotland information and interactive educational resource for people with diabetes and their carers. The project is co-ordinated by a multidisciplinary project board consisting of patients, healthcare professionals and information technology specialists from across Scotland. The information held on the website is based on nationally agreed and verified educational advice in a variety of multimedia formats. The combination of a rich information resource and a strong and established brand identifies the MDMW website as the ideal platform upon which to build a system to allow patients access to their information (figure 1).
The My Diabetes My Way website.
We designed a system to link MDMW to SCI-DC data to allow patients access to their clinical information, sourced from all relevant diabetes information sources. This personal health record is available to every individual with diabetes in Scotland aged 16 or older, regardless of their geographical location or demography.
The enrolment process required for the patient to register and gain access to their diabetes record consists of 4 main steps:
A novel collaboration is involved in the above process. The CAS 24 is a secure authentication platform that can be embedded within any public service web application requiring strong security. MDMW works with CAS, who supply and manage user authentication details required for each user to log in. This infrastructure is supported by secure printing facilities allowing usernames and passwords to be generated and posted separately to the patient.
With this approach, MDMW doesn’t hold any information about the user credentials, reducing the proliferation, and therefore increasing the security of authentication information. The trust relationship between CAS and MDMW means that successfully authenticated users are simply redirected to the requested application along with a unique citizen identifier. This delegation of user provisioning removes considerable administrative overhead. A single, centrally managed user account also makes it easier for the citizen as they do not have multiple user accounts to remember for different systems, while potentially accessing multiple online public services from the CAS portal. The MDMW records access system made use of this collaboration to provide the first healthcare interaction with the CAS infrastructure, expanding the existing public service portfolio covered.
The MDMW ePHR builds upon the existing look and feel of the website with the data presented split into manageable sections such as ‘my personal details’, ‘my lifestyle’, ‘my foot screening’ and ‘my medication’. Within these sections, key diabetes data are displayed alongside supporting, text avoiding clinical jargon. The design of the system was built on a strong user-focus, with patients involved in each stage of the design, review and testing. Patient engagement was essential to ensure the usability and accessibility of the system, particularly considering the wide age range of potential users.
The links on the right side of each screen are tailored to the patient’s clinical measurements, with the example in figure 2 showing a patient at high risk of foot-related complications, such as ulceration. The links in this example signpost the individual to information on appropriate footwear, management of ‘high-risk’ feet and the routine care that should be expected from the healthcare team.
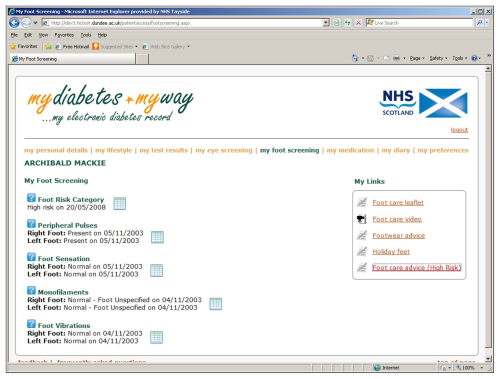
Example screen showing links tailored to the individual.
Results
The records access module was launched on 15 December 2010 and at the end of March 2013, 3,391 patients had registered to access their own clinical data. Thirty-one percent of these registrants had type 1 diabetes, showing a much higher uptake in this group compared with the background population of around 10%. 3 Sixty-one percent were male, 2,015 had completed the enrolment process and 861 had successfully logged in to the system. By the end of 2012, the number of distinct users per month had risen to nearly 300 (figure 3). This is due, in part, to an advertising campaign launched in collaboration with the Scottish Government and Diabetes UK in August 2012. Posters signposting people with diabetes towards MDMW were displayed in all community pharmacies and leaflets were included with diabetes prescriptions for a 6-week period.
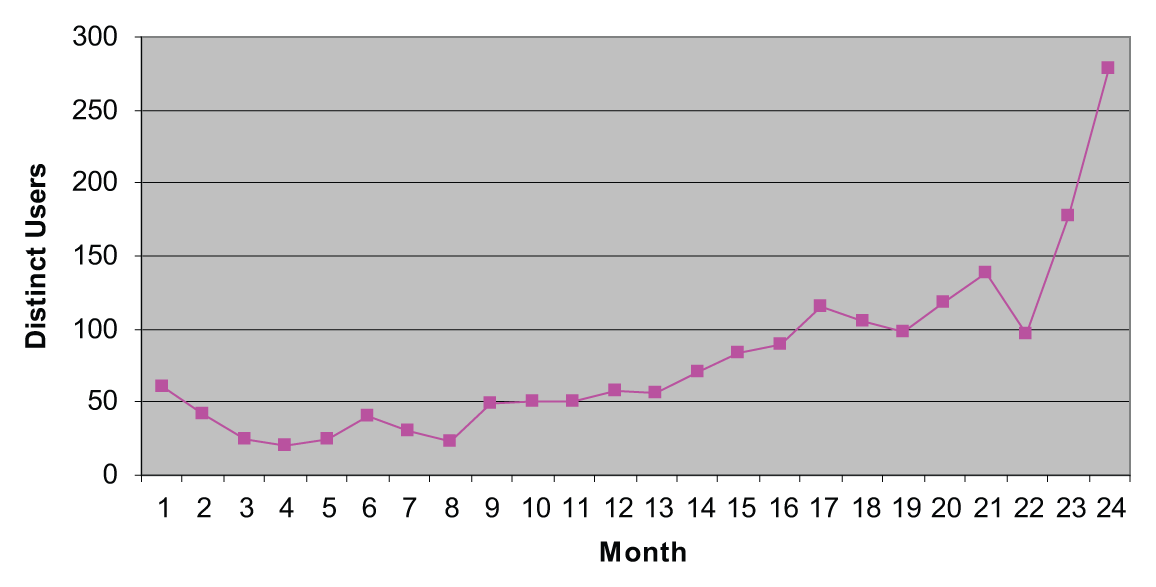
Distinct users per month since launch.
Much of the anecdotal feedback received via email and website comments has highlighted the usefulness of the system in supporting self-management:
‘The knowledge provided helps me understand the normal parameters and where I stand/can improve …’
‘more information available to me means I can play a more positive role in my treatment …’
‘Great site and like having the long term history available to put current results in perspective …’
‘It is great to be able to view all of my results so that I can be more in charge of my diabetes …’
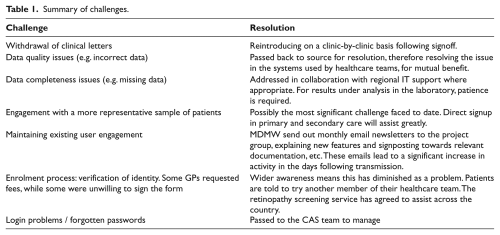
Despite the rising popularity of the system, a number of challenges have been faced and these are summarised in table 1. The most significant of these has been access to clinical letters sent from secondary care to primary care. During an initial 3-month pilot, these letters were available, but following concerns from the clinical teams regarding potential references to third parties who had not consented, these letters were removed. This understandably caused significant discontent amongst patients, and has highlighted shortcomings in the detailed understanding of data protection legislation amongst clinical staff. As a result, a guidance and signoff form was sent to all hospital diabetes consultants with a covering letter reinforcing patient rights, the fact that record sharing is good practice and explaining that the guidance should be displayed in all consulting rooms so that new, junior staff are aware of their responsibilities. To date, two hospital diabetes clinics have now agreed to share letters once again, but challenges remain in convincing the remaining 38 across NHS Scotland.
Summary of challenges.
Patient access has led to queries regarding the quality and completeness of some data, ultimately leading to corrections and the resolution of data interfacing issues. Patients are much more likely to demand a completely accurate clinical record that reflects their precise diagnosis information, including date of diagnosis and in some cases less common diabetes sub-types. One incident of data quality resolution highlighted a fundamental flaw in the way in which default values were being used in a hospital clinic system. This led to changes in working practice and more accurate data recording.
While it is acknowledged that the current registrants are largely a self-selecting group of individuals with a keen interest in their own self-management, work is underway to raise awareness and offer access much more widely. All hospital diabetes clinics are now encouraged to sign patients up as they attend routine appointments and many now take advantage of this approach. Much more challenging, but nonetheless important is engagement with primary care using similar approaches – something that the Department of Health Information Strategy 16 aims to address.
New developments
While the system began as a ‘read-only’ system, the ability to enter home-recorded results was implemented in January 2013. This allows users to manually enter home blood glucose results, blood pressure, cholesterol, weight and smoking status (figure 4). While this has enhanced user involvement, the project team are working towards automatically integrating with home-recording devices so that this data can be automatically uploaded into the system.
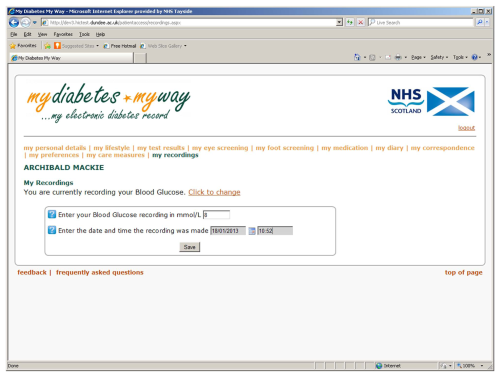
Recording of home-recorded results
Further developments underway include printable reports covering the main summary pages, a 15 care measures page that links to the Diabetes UK campaign 25 and a ‘home-recorded data summary’ for sharing with healthcare teams during appointments in order to assist the consultation. Finally, parent and carer access is soon to be made available, particularly to support the parents of young children.
Conclusions
The MDMW records access system is now a useful additional component for the self-management of diabetes in Scotland. Users report that it helps them to monitor their results and prioritise areas in which they need to improve, while indicating that it leads to a more productive consultation with healthcare professionals.
The project is currently due to run until the end of 2013, by which time a target of 5,000 registrants is expected to be achieved. By then a more representative sample of patients will have been recruited, however this will likely be influenced by the interest generated in primary care.
Although the system has been developed for, and by, stakeholders from across Scotland, it has the potential to connect to any electronic medical record. Work will continue to evaluate and report on the system in order to enhance the relatively spare evidence base currently available for personal health records.
Footnotes
Funding
This work was funded by the Scottish Diabetes Group. Thanks are extended to SCI-DC, diabetes healthcare teams and all patients participating in the My Diabetes My Way programme.
Declaration of conflicting interest
The author declares that there is no conflict of interest.
Information Governance
Ethical approval for data analysis has been obtained from the East of Scotland Research Ethics Service (EoSRES): 12/ES/0015. Anonymised data shown.