
Abstract
Visual comfort plays a central role in building occupants’ comfort, well-being and productivity. It is therefore fundamental to meet the occupants’ visual and lighting needs, carefully accounting for the room layout, usage and activities. In this framework, physiotherapy centres constitute a peculiar case since they are occupied by therapists and patients from different age groups, engaged in various activities performed in different positions in the rooms, and affected by different health issues. Lighting quality and satisfaction were monitored in four physiotherapy centres in Northern Italy and Denmark. Subjective assessments were compared with objective illuminance measurements at the task areas, and the sites were also analysed in terms of window and architectural features. Moreover, the interaction between visual and other environmental perceptions was studied. The results revealed: (1) positive influence of daylight access on the satisfaction of occupants; (2) occupants’ complaints about low lighting levels associated with artificial lighting being unable to provide 300 lx and natural light not balancing this lack of illumination; and (3) lower satisfaction among therapists, who also showed the tendency to assess their environmental perception more globally, since correlations between light and daylight satisfaction and other stimuli were observed when comfort issues were present.
1. Introduction and background
Many different parameters determine occupants’ well-being in an indoor environment. This should be considered when developing strategies to improve the overall indoor conditions, for instance by accounting for both visual and thermal aspects and reducing global energy demands, for example, lighting and cooling energy use.1–4 Particularly, when planning lighting in buildings, it is necessary to combine design criteria and human emotional preferences. 5 Lighting quality and balanced and integrated use of artificial light and daylight strongly influence psychophysical and psychological responses,6,7 the general perception of a space and physiological responses by regulating our circadian rhythm with subsequent effects on occupants’ performance and well-being.8–17 In environments like healthcare facilities, adequate lighting design may even contribute to the treatment by alleviating symptoms, improve well-being of patients and avoid medical errors.18–25
In recent years, lighting energy savings have been achieved through the installation of efficient lamps and luminaires, daylight exploitation and proper regulation of luminaires, for example, dimmable controls,26–30 with, however, a rebound effect due to higher consumption of such products and use of higher levels of artificial light when unnecessary. Potential energy savings can be achieved by optimising the design of the artificial lighting system and by the use of improved control strategies, especially by integration with natural light. As a whole, energy use of lighting can be moderated by the actions taken by the occupants and by the resulting quality of the visual environment, 31 which in turn can affect occupants’ productivity.32,33 Occupants’ productivity and satisfaction also depend on daylight availability, as determined by Day et al. 34 thanks to physical data and questionnaires collected in three large commercial office buildings. However, occupants’ needs for achieving higher performance and satisfaction levels depend on the functions of buildings. Accounting for occupants’ needs in relation to building functionality from the early design stages can help meeting requirements and improving their comfort and performance, also taking into account the potential energy savings of design solutions. Physiotherapy centres represent a particular environment since therapists, whose tasks need to be performed precisely and smoothly, and patients, whose well-being during the therapy is fundamental, share the spaces. These two groups of occupants perform different types of activities, occupy different positions in the rooms and have a large diversity in terms of age, fitness and health status. The positions and the activities performed also depend on the types of therapy, which can be either static or dynamic: static therapies consist of a series of treatments performed on patients while they are lying or sitting on a bed; dynamic therapies are categorised into callisthenics and other types of physical exercises. The two types of performed treatments cause physiotherapy centres to resemble both healthcare facilities and sports’ halls. 35 Such attributes related to these specific types of health centres introduce complexity in the design of the lighting conditions and visual environment that can accommodate all occupants in such centres. Moreover, the type of activity and privacy issues, stressed by the presence of partially undressed people in the treatment rooms, make it difficult to perform detailed long-term monitoring to be coupled with subjective assessments of the users, for instance with the usage of calibrated cameras for High Dynamic Range imaging analyses, luminance mapping and visual discomfort metrics calculation.
EN 12464-1 36 requirements in environments similar to static and dynamic therapy rooms of physiotherapy centres: illuminance lower threshold on the task area, Unified Glare Rating limit (UGRL) and uniformity (UO)
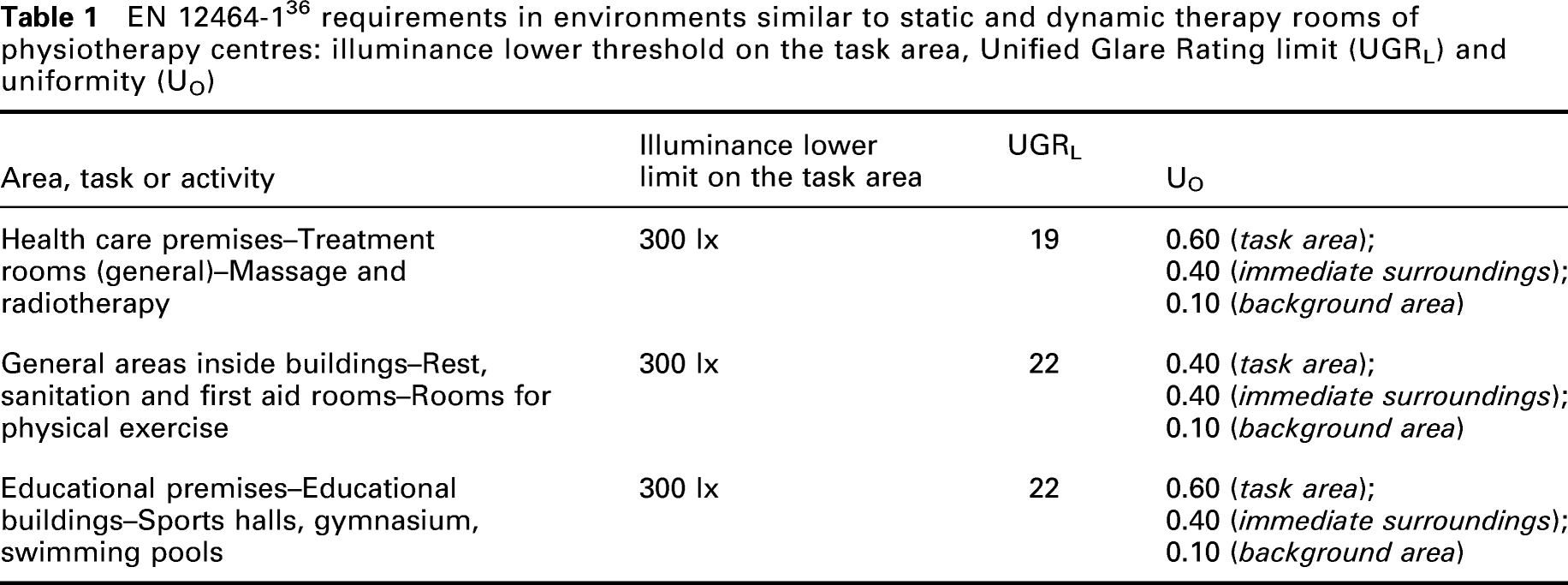
Concerning daylighting, the uniformity obviously decreases with the distance from the windows, but the standard considers this problem compensated by the additional benefits of daylight. In EN 12464-1, 36 daylight harvesting is strongly encouraged in order to improve energy efficiency and to facilitate contact with the outside environment. Nevertheless, the standard emphasises also the importance of not causing thermal or visual discomfort or a loss of privacy with windows. DS-EN 17037:2018 37 standardises how to provide daylight indoors and limit glare using relevant evaluation methods such as Daylight Glare Probability. It underlines the importance of the view out, which depends on a series of factors such as the size and distance of openings, the width of the view, the number of available layers (sky, landscape and ground) and the quality of environmental information of the view, and suggests several verification methods. Moreover, it highlights the influence of the exposition to sunlight on well-being, since dissatisfaction can result from its permanent exclusion or excess. Finally, an upper threshold of the illuminance level in indoor spaces is not directly provided by the technical standards. In this matter, Nabil and Mardaljevic 38 suggest not to exceed the threshold of 2000 lx on the work-plane in order to avoid glare. These values permit to define the Useful Daylight Illuminance (UDI) with the three ranges of UDI <100 lx, 100 lx < UDI <2000 lx and UDI >2000 lx. In addition, another threshold of UDI >3000 lx was proposed in recent publications. 39
Another important aspect to consider in studies related to lighting in the indoor environment is the interaction between different indoor environmental parameters. The reviews by Torresin et al. 40 and Schweiker et al. 2 highlight that studies regarding interaction and combined effects of different indoor environment domains (thermal, visual, indoor air quality and acoustics) are few. Moreover, they underline that the results of these research studies should be incorporated in standards on the indoor environment, including lighting ones, as positive effects on occupants’ performance and perception would be found. In fact, users are affected by their exposure to simultaneous stimuli from the four comfort domains, and their combination influences their well-being. This happens for both physical (e.g. effect of daylight on thermal perception, due to possible direct radiation) or psychological (e.g. personal parameters related with the subject considered) reasons. Human-centred design would be promoted by additional knowledge on stimuli interaction, improving positive and reducing negative effects of environmental stimuli on users’ well-being. 40
To our knowledge, there is not much literature with a focus on lighting quality and conditions in physiotherapy centres, as well as many field studies collecting both measurements and subjective data regarding lighting conditions and visual comfort in healthcare and sports facilities. However, several studies suggest that a faster healing and the well-being of patients depend on the access to daylight in hospitals.25,41–46 Ulrich 41 reported that in a hospital in Pennsylvania, shorter hospital stays, fewer negative evaluations by nurses and less use of strong analgesics were observed among after-cholecystectomy patients in rooms with a natural view. In their study about the dependence of the length of stay and the indoor lighting in a hospital, Choi et al. 25 observed that the hospitalisations in the South-East oriented area were shorter than in the North-West one. By means of a questionnaire survey on bedside lights in three hospitals, Bidikar and Bidikar 46 found that the main problems for patients were too high illumination and glare from light sources and reflective surfaces, together with some lack of uniformity due to light appearing in some spots close to the windows. Moreover, low illumination was found connected with difficulties to perform some normal tasks like eating and reading. Questionnaire surveys were made by Eijckelenboom et al. 47 among hospital outpatient staff of six buildings in the Netherlands. Widespread dissatisfaction (48% of workers) with daylight was found among staff. Moreover, about one-third of the employees were dissatisfied with artificial light and the overall quality of light, and two out of five of those having a window were dissatisfied with their view. Hauck et al., 48 in their test comparing the visual performance of visually impaired and normal-sighted individuals, found that special lighting conditions were required by most people with visual disabilities, who also showed higher glare sensitivity and adaptation problems related to non-uniform lighting. The latter ones are also highly related to the conditions in physiotherapy centres, where, in particular, elderly people with an increased risk of age-related visual defects, are likely to be present.
In order to address the specific conditions of physiotherapy centres and the lack of specialised knowledge about the lighting quality and visual comfort in such spaces with diverse types of occupants, this study evaluated lighting quality and satisfaction in such facilities. Extensive subjective evaluations were recorded by questionnaires answered by physiotherapists and patients in four different centres – two located in Bolzano (Northern Italy) and two in Copenhagen (Denmark). Due to the difficulties to perform luminance measurements, the questionnaires’ outcomes were analysed and compared with illuminance levels and observations taken in the different rooms, such as fenestration area, daylight availability, access to view to the outdoors and other lighting and architectonical characteristics, that is, uniformity, orientation, types and control of shadings. Moreover, light satisfaction and daylight satisfaction were statistically compared with the satisfaction with the other environmental factors (thermal, indoor air quality and acoustic). The study had the following objectives: 1. To identify the preferred levels of illuminance on the work-planes of the different rooms, considering both daylight and artificial light availability. 2. To highlight the main lighting issues depending on the type of environment and the type of occupant. 3. To evaluate the dependence of light and daylight satisfaction from patients on their gender, age and health status, as well as on environmental characteristics such as daylight access, and to highlight the difference between therapists and patients in the perception of the visual environment and their light and daylight satisfactions. 4. To associate light and daylight satisfaction of therapists and patients with other environmental stimuli (thermal, indoor air quality and acoustic) to take into account the combined effects of different indoor environment domains.2,40 This permits to highlight if and how light and daylight satisfaction of occupants also influences satisfaction with other comfort domains and vice-versa, studying the different effects of environmental well-being on therapists and patients and promoting, if necessary, a global approach in human-centred design of physiotherapy facilities.
This study provided a first contribution in terms of lighting conditions and preferences in physiotherapy centres. If integrated with similar research, it can help to develop guidelines to adequately address the requirements of therapists and patients in terms of visual comfort.
2. Method
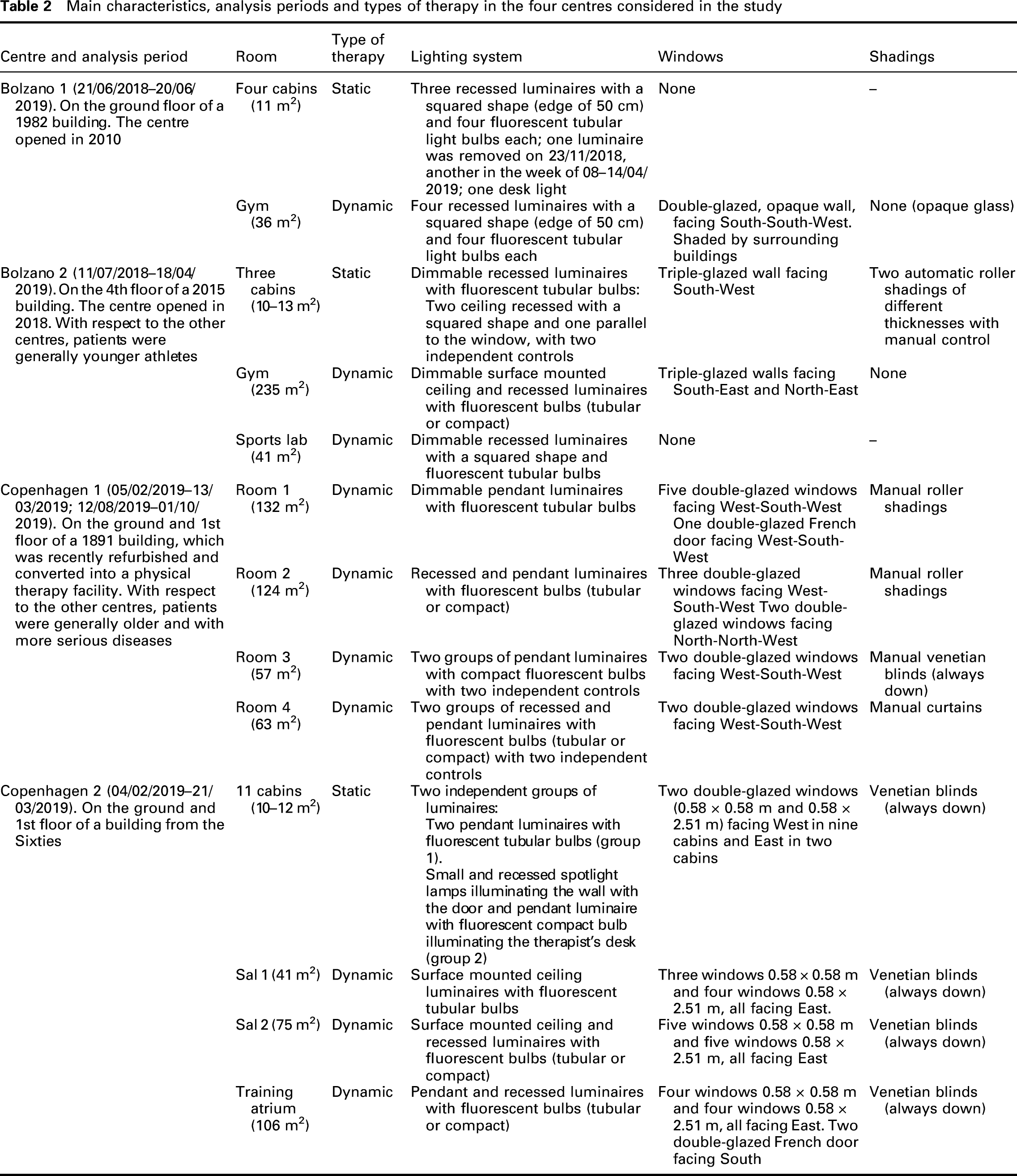
Main characteristics, analysis periods and types of therapy in the four centres considered in the study
2.1 Case studies
Four physiotherapy centres were chosen for the study. Two of them (Bolzano 1 and Bolzano 2) are located in Bolzano, Northern Italy, and two of them (Copenhagen 1 and Copenhagen 2) are in the suburbs of Copenhagen, Denmark. Table 2 shows the main architectonical characteristics of the four centres from a lighting point of view, together with the types of therapy performed and the periods of investigation. Pictures of the centres are shown in Figure 1. The four facilities were selected as they resemble a broad range of architectonical and lighting characteristics: both cabins and gyms are present, with different illuminance conditions and daylight access, as well as different weather conditions due to the two locations and various analysis periods. Moreover, depending on the specific centre, several types of patients in different age ranges were present. Both static therapies, involving massages and treatments with the patient lying or sitting on a bed, and dynamic therapies, with patients performing physical exercises in gym-like rooms, were performed in the four facilities. Rooms for static therapies are small cabins (approximately 10–13 m2) with a therapy bed about 2 m long and 0.6–0.7 m large in the centre of the room and with a desk. Beds’ heights were always regulated between 0.45 m and 0.60 m. On the other hand, rooms for dynamic therapies are larger, with variable dimensions depending on the facility. Exercise machines are generally present in these rooms. The work-planes to be considered in the lighting measurements and evaluations were chosen according to the task areas: beds in rooms for static therapies and floors in rooms for dynamic therapies. The cabins of Bolzano 1, Bolzano 2 and Copenhagen 2 are almost symmetrical from an architectonical point of view and identical from a lighting point of view. Therefore, their measurements and analyses were grouped when reporting measurements and results. There were no windows in the cabins of Bolzano 1 (Figure 1(a), left and centre) or in the Sports’ Lab of Bolzano 2. Also, the glazed walls in Bolzano 2 (Figure 1(b)) and in the gym of Bolzano 1 (Figure 1(a), right) should be noticed. Moreover, shadings were always kept down in Copenhagen 2 (Figure 1(d)), as well as in Room 3 of Copenhagen 1 (Figure 1(c), right). Daylit or window glare control was possible in Copenhagen 1 and cabins of Bolzano 2, by means of shadings and curtains. In the gym of Bolzano 1, there were no shadings due to the presence of opacified glass. Interior of the four physiotherapy centres: (a) Bolzano 1 (left to right) – a cabin with the desk light on, the three recessed luminaires of the cabins, the gym with recessed luminaires and the opacified glass wall; (b) Bolzano 2 (left to right) – a cabin with the triple-glazed wall and the roller shadings, a cabin recessed luminaire, the gym with surface mounted ceiling luminaires and the triple-glazed walls; (c) Copenhagen 1 – Room 1 with pendant luminaires and the double-glazed windows and door with roller shadings, Room 2 with pendant luminaires and double-glazed windows with Venetian blinds, Room 3 with pendant luminaires and always down Venetian blinds; (d) Copenhagen 2 (left to right) – a cabin with pendant desk luminaires, Sal 2 with surface mounted ceiling and recessed luminaires, the Training Atrium with pendant and recessed luminaires, all with the double-glazed windows with always down Venetian blinds
2.2 Measurements
Window-to-floor ratio (WFR), measured illuminance ranges and uniformity in the different rooms of the four centres considered, both with artificial and natural lights and with only artificial lights. Measurements with completely dark outside were not possible in Copenhagen 1 and Sal 2 of Copenhagen 2 due to opening times and therapy schedules: the hypothetical levels of illuminance with only artificial light were obtained obscuring the windows during low light hours or overcast weather outside; therefore, the illuminance ranges with only artificial light are marked with an ‘∼’ in these rooms, indicating a value estimated with low daylight
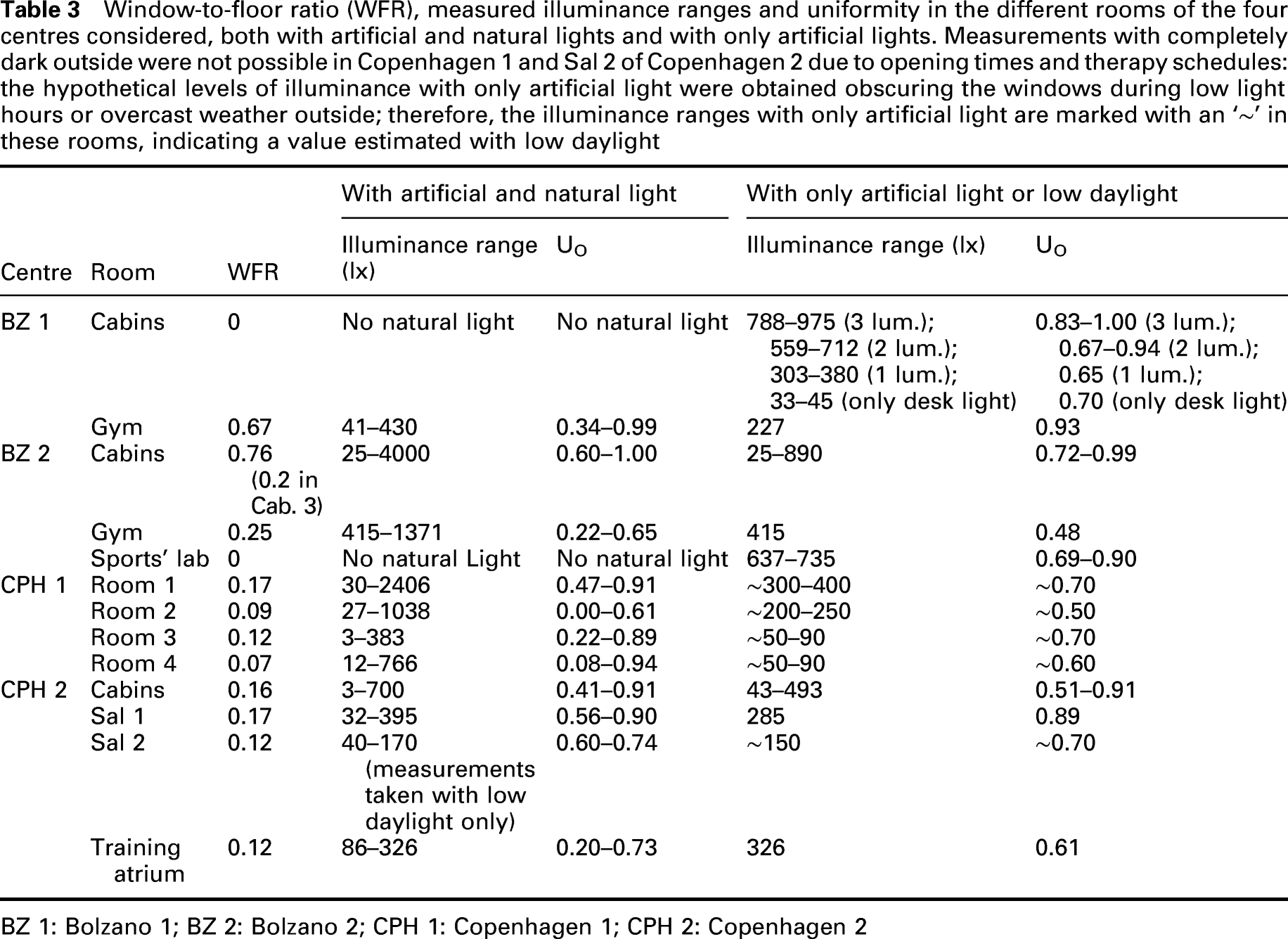
BZ 1: Bolzano 1; BZ 2: Bolzano 2; CPH 1: Copenhagen 1; CPH 2: Copenhagen 2
In Room 1 of Copenhagen 1, also long-term measurements of illuminance were made by means of five Extech SDL400 light meters. Not to interfere with therapy sessions, the five illuminance meters were positioned on the walls of the room approximately at equal distance and at 1 m height (height chosen not to disturb the cleaning operations of the room), with the sensors all horizontal (see Figure 2). The instruments were set to log the instantaneous values of illuminance every 15 min. Long-term measurements were also made periodically in Cabins 1, 2 and 3 of Copenhagen 2, locating one illuminance meter per cabin, horizontal and hanging on the wall at bed height. These measurements were used to estimate long-term illuminance on the task areas (as will be explained in Section 2.4), allowing to assess its daily variation and to associate light and daylight satisfaction with the estimated illuminance level in Room 1 of Copenhagen 1 (analysis in Section 3.5). Positioning of Extech SDL400 light meters for long-term measurements in Room 1 of Copenhagen 1 (first three pictures from left to right) and one cabin of Copenhagen 2 (last picture on the right). The sensors were located on the walls not to interfere with the therapy sessions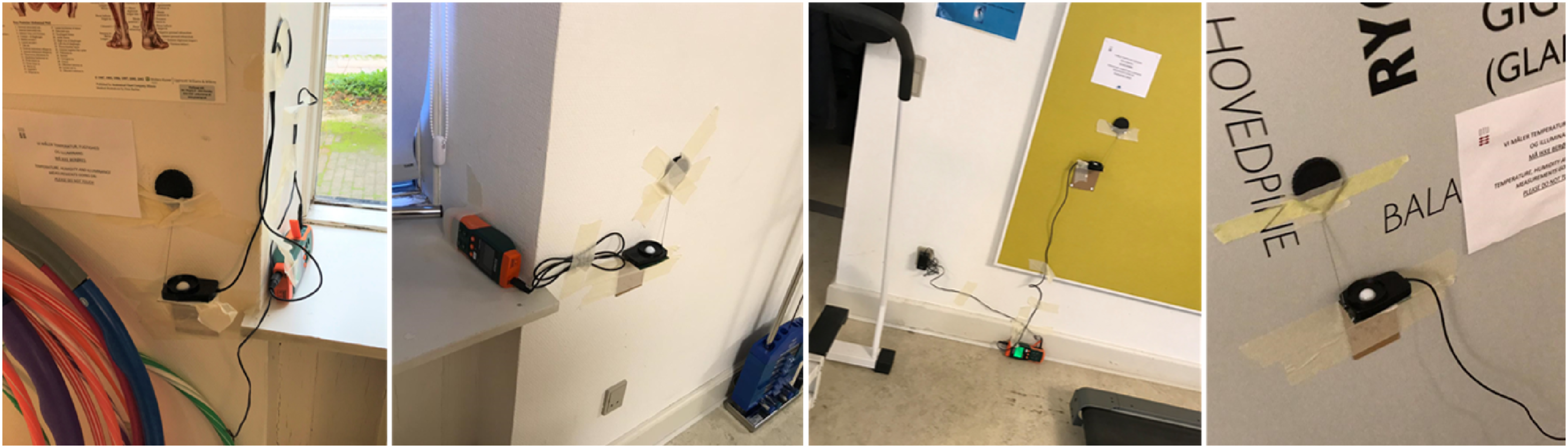
2.3 Questionnaires
Questionnaires were developed in order to be user-friendly and understandable without the presence of the researchers during completion. Considering the bilingualism of the area, the questionnaires for Bolzano were developed in Italian and German. Similarly, the questionnaires used in Copenhagen were translated into Danish and English, taking into account the presence of non-Danish speakers living in the area. Zaniboni et al. 35 report details on how the questionnaires were created and used.49–60 Questions about the date, time and room where the therapy was performed were asked to therapists and patients before therapy, together with personal information such as gender, age and self-evaluation of their health status. No traceable information was asked. Preliminary tests showed how using a 7-point scale of brightness sensation caused misunderstandings: terms like ‘bright’ and ‘too bright’ (respectively referred to the ‘+2’ and ‘+3’ levels) were interpreted as positive features by the respondents instead of too high luminous fluxes. Therefore, a 7-point scale (from 1, totally unsatisfied, to 7, totally satisfied) was used to record the light and daylight satisfaction to evaluate the light sources’ general qualities. Light satisfaction referred to the whole electrical and natural lighting scenario, while daylight satisfaction referred only to the natural one. These two questions were followed by a multiple-choice question, which permitted to identify the main sources of discomfort (‘too low light’, ‘too high light’, ‘glare’, ‘flash blindness’ and ‘other: …’). When relevant, the artificial lighting state (‘On’/‘Off’) and the shading state (‘Up’/‘Half’/‘Down’) were asked. The satisfaction scale was also used for the thermal, indoor air quality (IAQ) and acoustic comfort. Dynamic therapies were performed with groups of patients in Copenhagen 1 and sometimes in Copenhagen 2; in these cases, separate questionnaires were used for therapists and patients, permitting many patients to simultaneously complete the questionnaires. 35
2.4 Data processing and analysis methods
Spatial averages of illuminance values measured in different positions of the task areas were calculated during each point-in-time measurement campaign in order to have a representative illuminance value for each considered condition. The average hourly long-term measurements of illuminance on the floor of Room 1 of Copenhagen 1 were estimated using linear regression between the instantaneous spatial average of the point-in-time measurements of the sensors positioned on the walls and of instruments positioned on the floor. The linear regression obtained by all the sets of point-in-time measurements permitted to calculate the long-term floor-average illuminance in the whole period of analysis starting from the measurements of the illuminance meters, which were located on the walls, not to disturb the therapy activities (Section 2.2). The same approach was used to assess the long-term illuminance on the beds of Cabins 1, 2 and 3 of Copenhagen 2 by means of wall-located sensors. Instantaneous values of illuminance were also estimated in the cabins of Bolzano 1, without any windows. Luminaires were progressively removed from these rooms on dates that were communicated by therapists (Table 2). Moreover, it was also known by questionnaires when only a desk light was used. For all these reasons, it was possible to estimate the instantaneous values of illuminance on the dates and at the times at which the questionnaires were completed, using averages of point-in-time measurements of illuminance.
The questionnaire answers were grouped separately for therapists and patients and further divided according to the environment in which they were completed (Sections 3.1–3.3). The Mann–Whitney test was used to determine if light and daylight satisfaction was different between therapists and patients. The test was chosen as the two samples were independent. In order to evaluate if and when the answers on light satisfaction and daylight satisfaction were similar, the Wilcoxon Signed-Rank test was applied separately for employees and patients. This test was chosen because, being the answers given by the same occupant types, the two samples were dependent. The Mann–Whitney test was also used to evaluate the association between light and daylight satisfaction of patients and their gender, age and self-evaluated health status. To evaluate the influence of age, patients were divided into younger and older than 65 years of age 49 ; also, they were grouped into ‘rating themselves as healthy’ and ‘not rating themselves as healthy’ as done in Zaniboni et al. 35 In order to further evaluate the magnitude of the differences between groups, Mann–Whitney and Wilcoxon tests were accompanied with Cliff’s effect size (Cliff’s δ) analyses and the absolute value of median differences.61,62 Spearman correlation was used to study the interaction of light satisfaction and daylight satisfaction of therapists and patients on the satisfactions about the other environmental parameters (thermal, IAQ and acoustics). The following conventional levels were used to define the magnitude of the correlations: (1) 0.000–0.199 ‘negligible’; (2) 0.200–0.399 ‘weak’; (3) 0.400–0.599 ‘moderate’; (4). 0.600–0.799 ‘strong’; and (5). 0.800–1.000 ‘very strong’. 63 For control purposes, also the answers about daylight satisfaction in rooms with no windows were reported.
The uniformity (UO) was calculated for the point-in-time measurements by dividing the minimum by the spatial average illuminance value.64,65 This indicator was also used with both artificial and natural light to show the contrast between various areas of the rooms, which might lead to discomfort issues such as glare.
3. Results and discussion
The results start with observations from measurements and questionnaires, followed by statistical analyses where Mann–Whitney, Wilcoxon and Spearman tests were used to quantify the significance of the different conditions on occupants’ satisfaction.
3.1 Characteristics of the rooms: illuminance, uniformity and fenestration area
Sources of visual discomfort detected by therapists and patients in the different centres and rooms
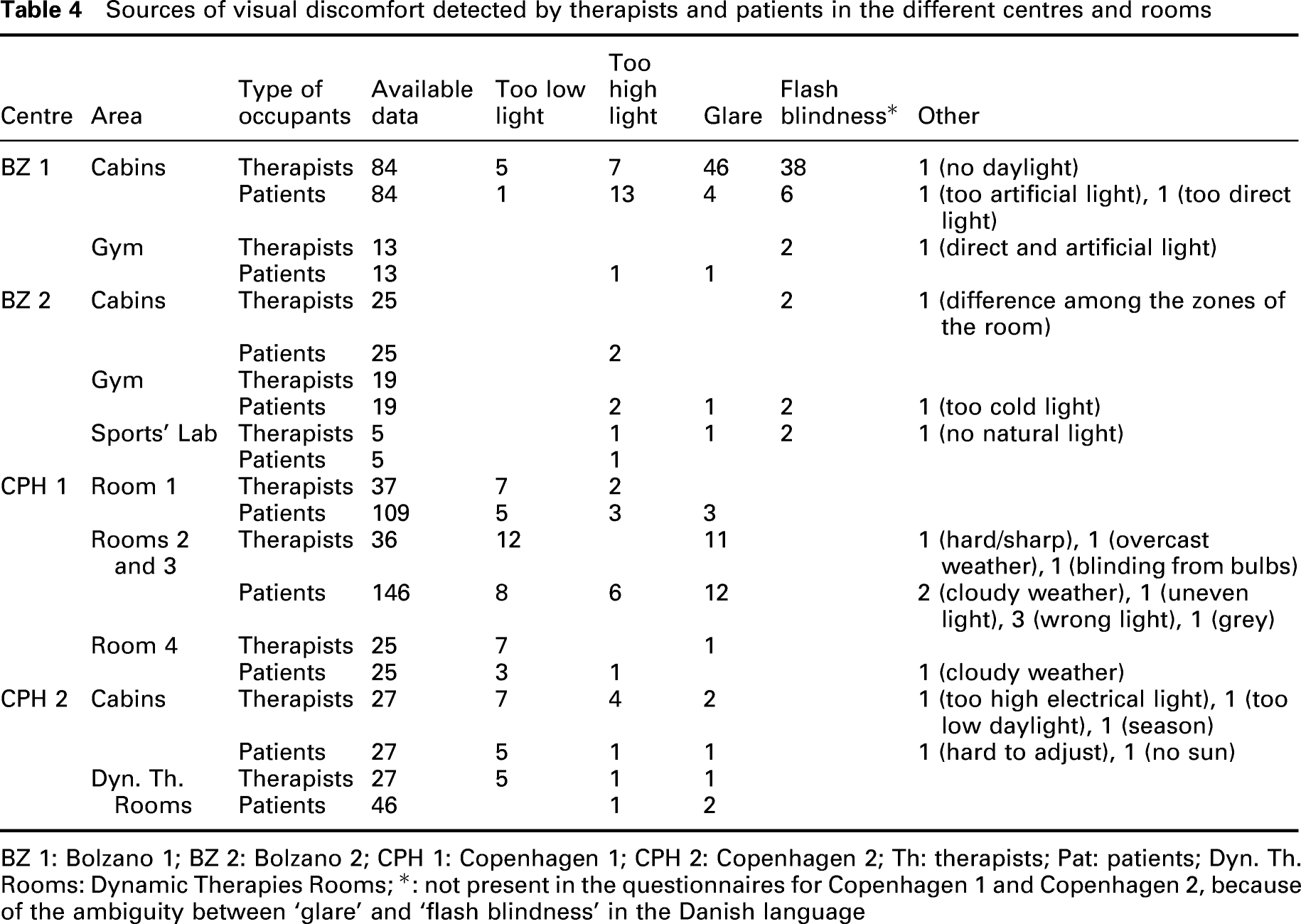
BZ 1: Bolzano 1; BZ 2: Bolzano 2; CPH 1: Copenhagen 1; CPH 2: Copenhagen 2; Th: therapists; Pat: patients; Dyn. Th. Rooms: Dynamic Therapies Rooms; *: not present in the questionnaires for Copenhagen 1 and Copenhagen 2, because of the ambiguity between ‘glare’ and ‘flash blindness’ in the Danish language
In the rooms with no windows (cabins of Bolzano 1 and Sports’ Lab of Bolzano 2), the illuminance levels by means of artificial light exceeded the recommended threshold of 300 lx according to EN 12464-1, 36 reaching 975 lx in Bolzano 1 and 735 lx in Bolzano 2. These illuminance levels provided by artificial light resulted in visual discomfort for the occupants. Some therapists of Bolzano 1 used an alternative desk light, which allowed for keeping the illuminance at 30–50 lx. Moreover, as occupants often reported discomfort due to ‘too high light’ (details will be discussed in Section 3.4), the managers of Bolzano 1 decided to progressively remove 1 and 2 luminaires from the cabins (see Table 2), resulting in lower levels of illuminance measured after November 2018 (2 active luminaires out of 3) and April 2019 (only 1 active luminaire). The gym area of Bolzano 2, with large-glazed walls and a large floor surface, was characterised by an uneven distribution of overall light levels across the room (UO level reaching 0.22 with natural light available) due to the difference of illuminance close and far from the natural light source. From the comparison of the values with natural light and with low natural light, it is possible to see that in Rooms 2, 3 and 4 in Copenhagen 1, artificial light was not sufficient to reach the minimum illuminance threshold of 300 lx as suggested by EN 12464-1. 36 Moreover, detailed measurements in Tables A2.13–A2.20 in Supplementary Appendix 2 (supplementary file) show that orientation issues are present in this centre: due to the West-South-West and North-North-West facing windows (Table 2), low illuminance values were measured in the morning with lights off. On the contrary, high illuminance was present in the afternoon with sunny weather. Additionally, in daylit hours and without artificial lights on, uneven distribution of overall light level was present in Room 2 (UO < 0.4), with illuminance levels in the back of the room significantly lower than near the bright glazing surfaces at the window area. Room 3 had a low level of daylight availability since shadings were always down. Tables A2.17–A2.18 in Supplementary Appendix 2 (supplementary file) show that there was low illuminance with shadings down and no artificial lighting (3–116 lx, with higher values only when the sun was directed to the windows). In Room 4, the window-to-floor ratio was low (0.07), and lower uniformity values (0.08–0.54) were detected when one or both the light groups were off (see Table 3 and Tables A2.19–A2.20 in Supplementay Appendix 2). Despite the low daylight access due to shadings always being down, in Copenhagen 2, the artificial illuminance respected the 300 lx requirement in all the rooms except Sal 2, where the spatial average of illuminance was no higher than 170 lx when daylight was low (see Table 3). The long-term illuminance measurements made in the cabins of Copenhagen 2 are reported in Figure A2.3 in Supplementary Appendix 2 (supplementary file). Two modes of illuminance levels set by artificial lighting were observed (around 100 lx and around 500–700 lx) due to the two independent groups of lamps in these rooms (see Table 2). Light levels did not exceed 820 lx indicating that the illuminance thresholds for glare risks of 2000 lx and 3000 lx38,39 were not reached in these rooms. A similar trend was seen during different days. Moreover, Tables A2.21–A2.23 in Supplementary Appendix 2 (supplementary file) show low values of the illuminance when artificial lights were off: due to the permanent use of shadings, little daylight was available in these rooms. A similar issue was present in rooms for dynamic therapy (Table A2.24).
According to the measurements in Table 3 and in-situ observations, the gym of Bolzano 1, cabins of Bolzano 2 and Room 1 of Copenhagen 1 were well served by daylight. In the gym of Bolzano 1, the illuminance was lower than 300 lx when daylight was not available. The cabins of Bolzano 2 were well lit with both natural and dimmable artificial light. Despite high illuminances (4000 lx) that could be reached because of daylight, the 2-layer roller blinds installed in these rooms allowed for glare control. Similarly, Room 1 of Copenhagen 1 was found well served with both natural and dimmable artificial light. However, in this case, the high level of daylight might give some glare problems: indeed, the large West-South-West facing windows resulted in peaks of illuminance in the early afternoon, as shown in Figures A2.1 and A2.2 in Supplementary Appendix 2 (supplementary file). These peaks exceeded the level of 2000 lx 38 during winter because of the lower position of the sun. The glare risk level of 3000 lx 39 was exceeded only one time.
Eventually, with the exception of gym of Bolzano 2 and Room 2 of Copenhagen 1, the required level of uniformity of 0.60 (Table 1) was generally met when only artificial lighting was used.
3.2 General data on collected questionnaires and population
Results of the statistical analyses performed to identify the differences between the satisfactions of therapists and patients (Test 1) and the dependence between light satisfaction and daylight satisfaction of the same category of occupants, either therapists or patients (Test 2) on the four different centres' samples.
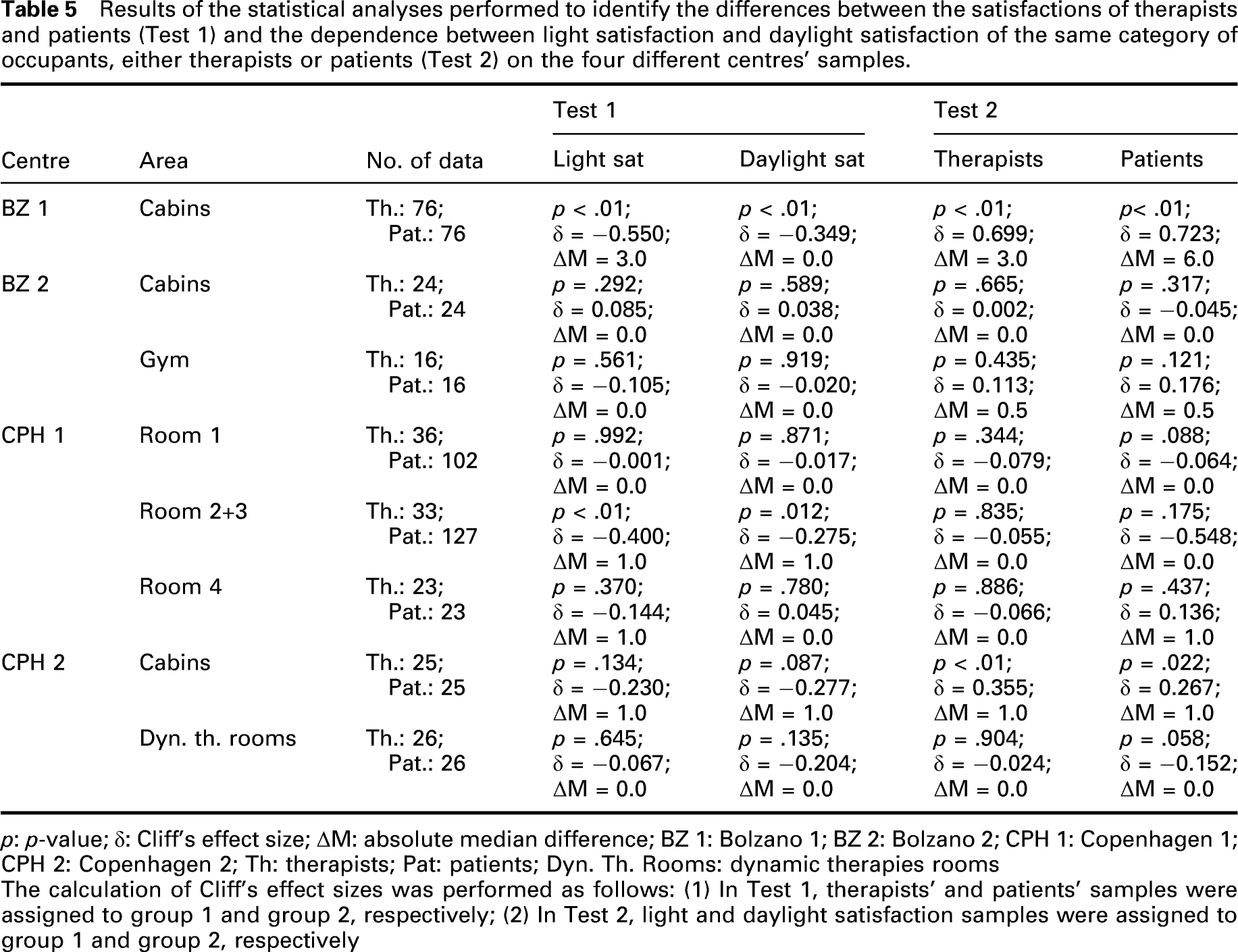
p: p-value; δ: Cliff’s effect size; ΔM: absolute median difference; BZ 1: Bolzano 1; BZ 2: Bolzano 2; CPH 1: Copenhagen 1; CPH 2: Copenhagen 2; Th: therapists; Pat: patients; Dyn. Th. Rooms: dynamic therapies rooms
The calculation of Cliff’s effect sizes was performed as follows: (1) In Test 1, therapists’ and patients’ samples were assigned to group 1 and group 2, respectively; (2) In Test 2, light and daylight satisfaction samples were assigned to group 1 and group 2, respectively
3.3 Correlation of patients’ gender, age and self-evaluated health status with their light and daylight satisfactions
Results of the Spearman test on the correlations of light and daylight satisfaction with thermal, IAQ and acoustic satisfaction on the four different centres' samples of therapists. ‘Light Sat’ and ‘Daylight Sat’ are the light and daylight satisfaction, ‘T. Sat’ is the thermal satisfaction, ‘IAQ Sat’ is the satisfaction for the Indoor Air Quality and ‘Acoustic Sat’ the acoustic satisfaction. Correlation Coefficients ρ and p-values are reported.
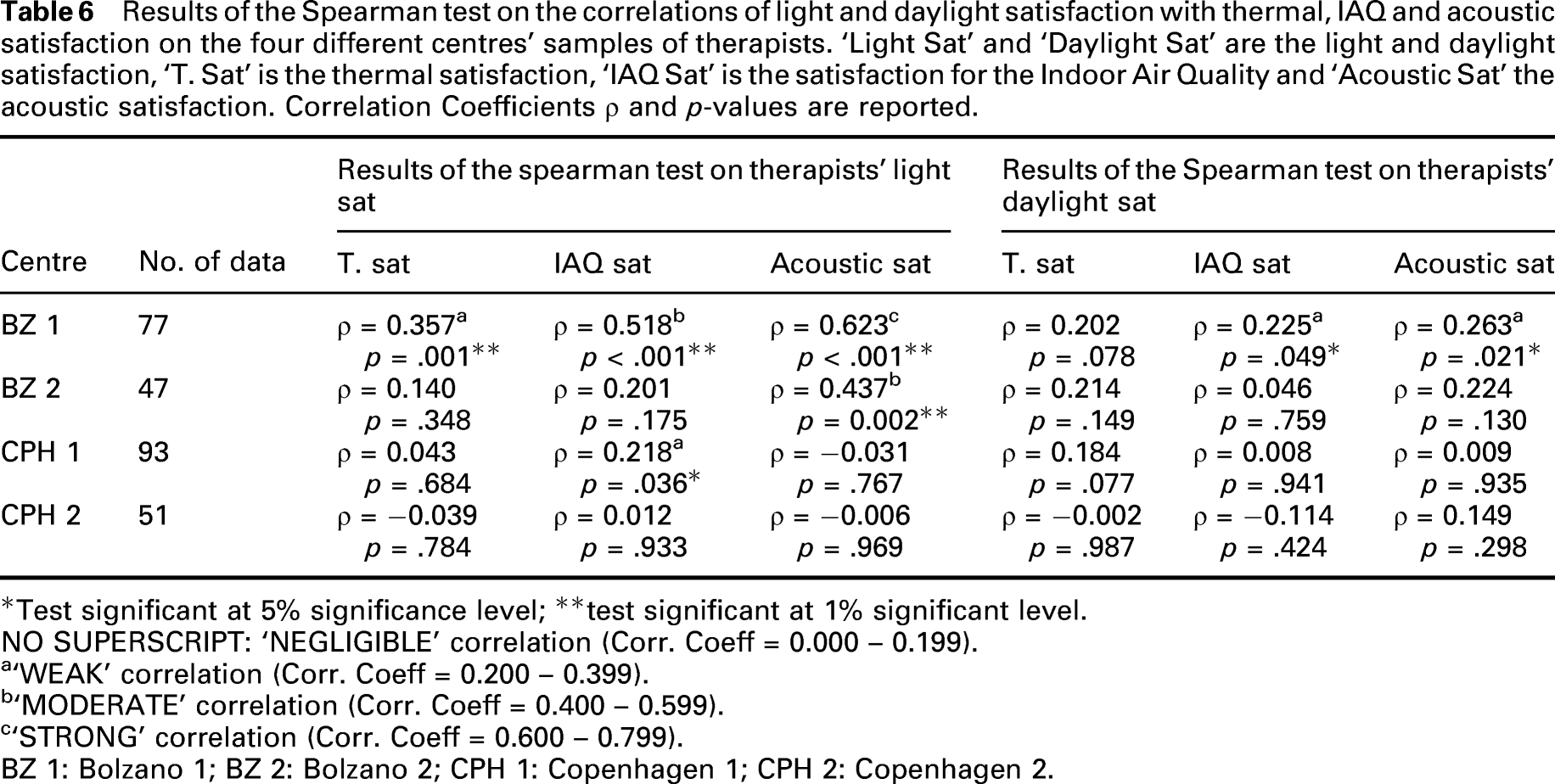
*Test significant at 5% significance level; **test significant at 1% significant level.NO SUPERSCRIPT: ‘NEGLIGIBLE’ correlation (Corr. Coeff = 0.000 – 0.199).
a‘WEAK’ correlation (Corr. Coeff = 0.200 – 0.399).
b‘MODERATE’ correlation (Corr. Coeff = 0.400 – 0.599).
c‘STRONG’ correlation (Corr. Coeff = 0.600 – 0.799). BZ 1: Bolzano 1; BZ 2: Bolzano 2; CPH 1: Copenhagen 1; CPH 2: Copenhagen 2.
3.4 Perception of the visual environment
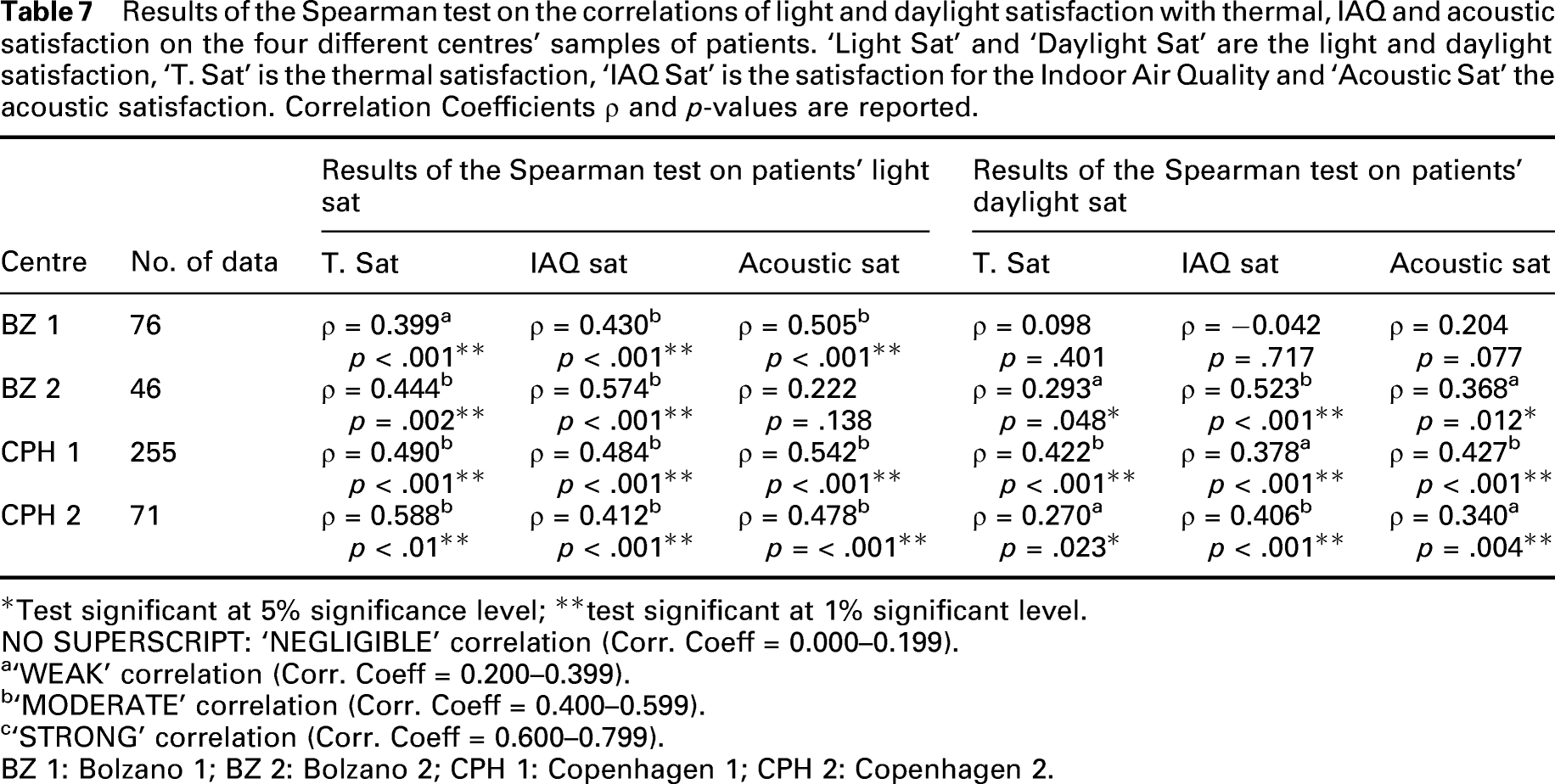
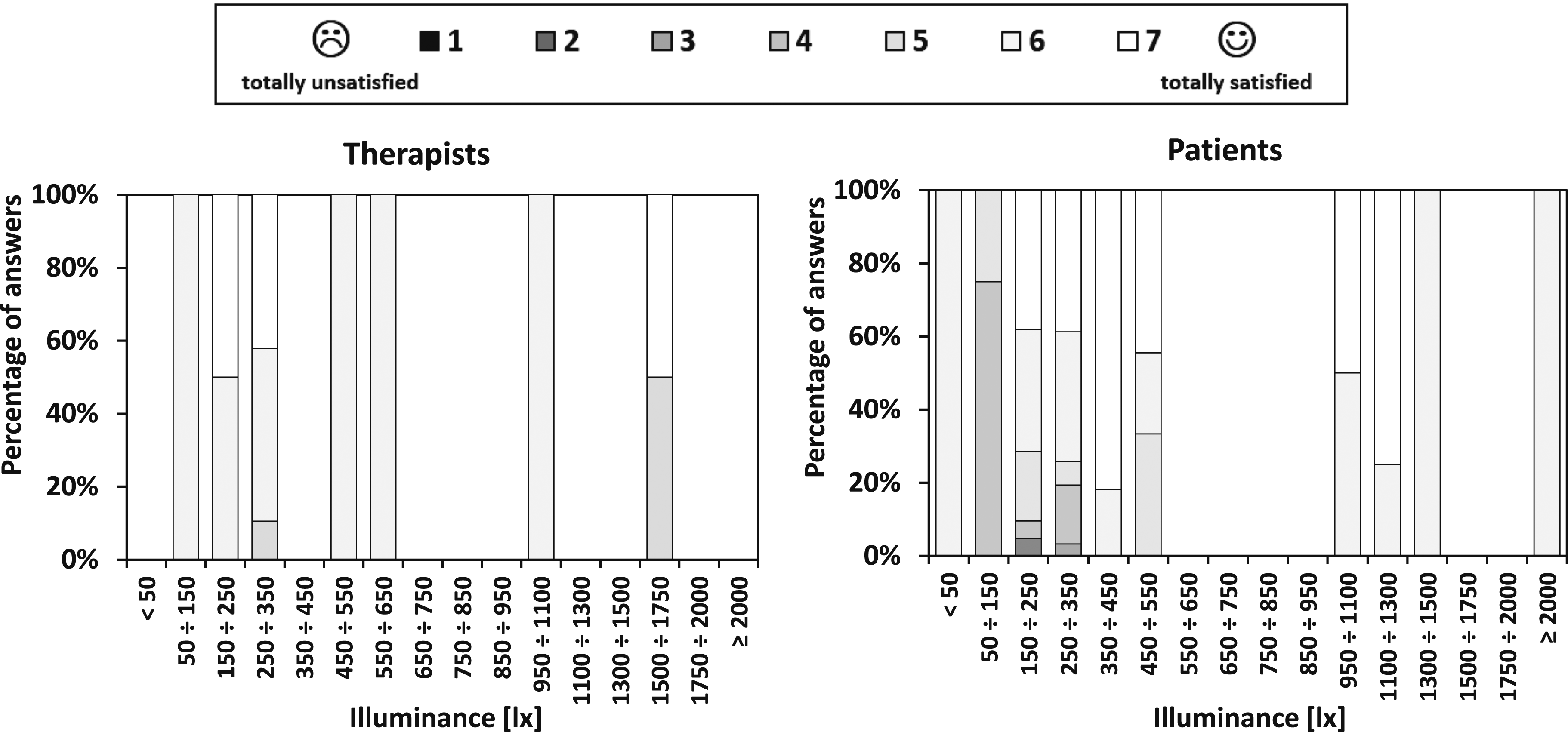
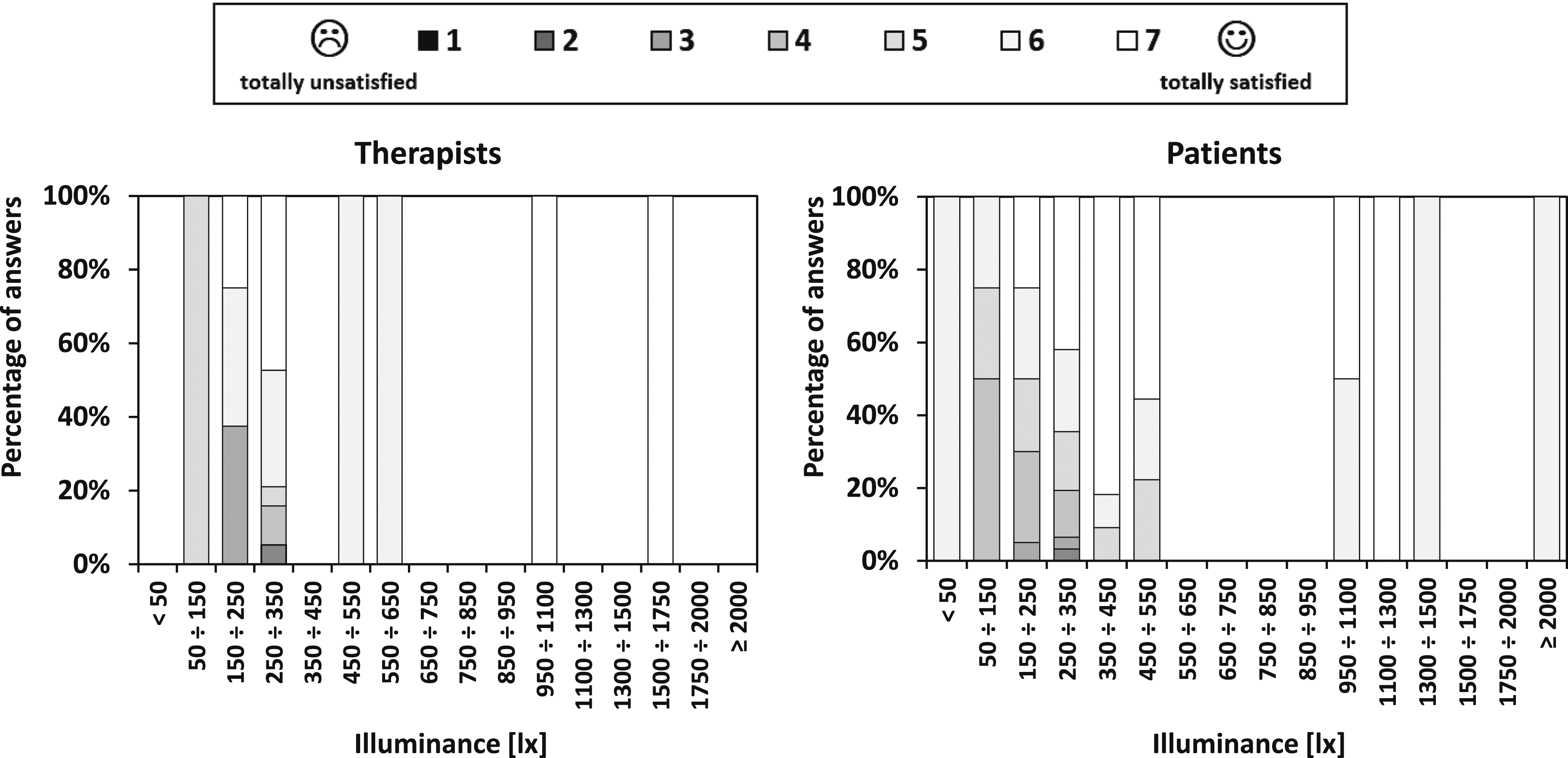
Figures 3–6 show the light satisfaction and the daylight satisfaction perceived by therapists and patients in the different rooms. The main sources of visual discomfort detected by occupants are reported in Table 4 in terms of the ‘number of therapists or patients reporting a source of discomfort’. Distribution of satisfaction ratings for light and daylight of therapists and patients in Bolzano 1. N = sample size Distribution of satisfaction ratings for light and daylight of therapists and patients in Bolzano 2. N = sample size Distribution of satisfaction ratings for light and daylight of therapists and patients in Copenhagen 1. N = sample size Distribution of satisfaction ratings for light and daylight of therapists and patients in Copenhagen 2. N = sample size Results of the Spearman test on the correlations of light and daylight satisfaction with thermal, IAQ and acoustic satisfaction on the four different centres’ samples of patients. ‘Light Sat’ and ‘Daylight Sat’ are the light and daylight satisfaction, ‘T. Sat’ is the thermal satisfaction, ‘IAQ Sat’ is the satisfaction for the Indoor Air Quality and ‘Acoustic Sat’ the acoustic satisfaction. Correlation Coefficients ρ and p-values are reported. *Test significant at 5% significance level; **test significant at 1% significant level.NO SUPERSCRIPT: ‘NEGLIGIBLE’ correlation (Corr. Coeff = 0.000–0.199). a‘WEAK’ correlation (Corr. Coeff = 0.200–0.399). b‘MODERATE’ correlation (Corr. Coeff = 0.400–0.599). c‘STRONG’ correlation (Corr. Coeff = 0.600–0.799). BZ 1: Bolzano 1; BZ 2: Bolzano 2; CPH 1: Copenhagen 1; CPH 2: Copenhagen 2.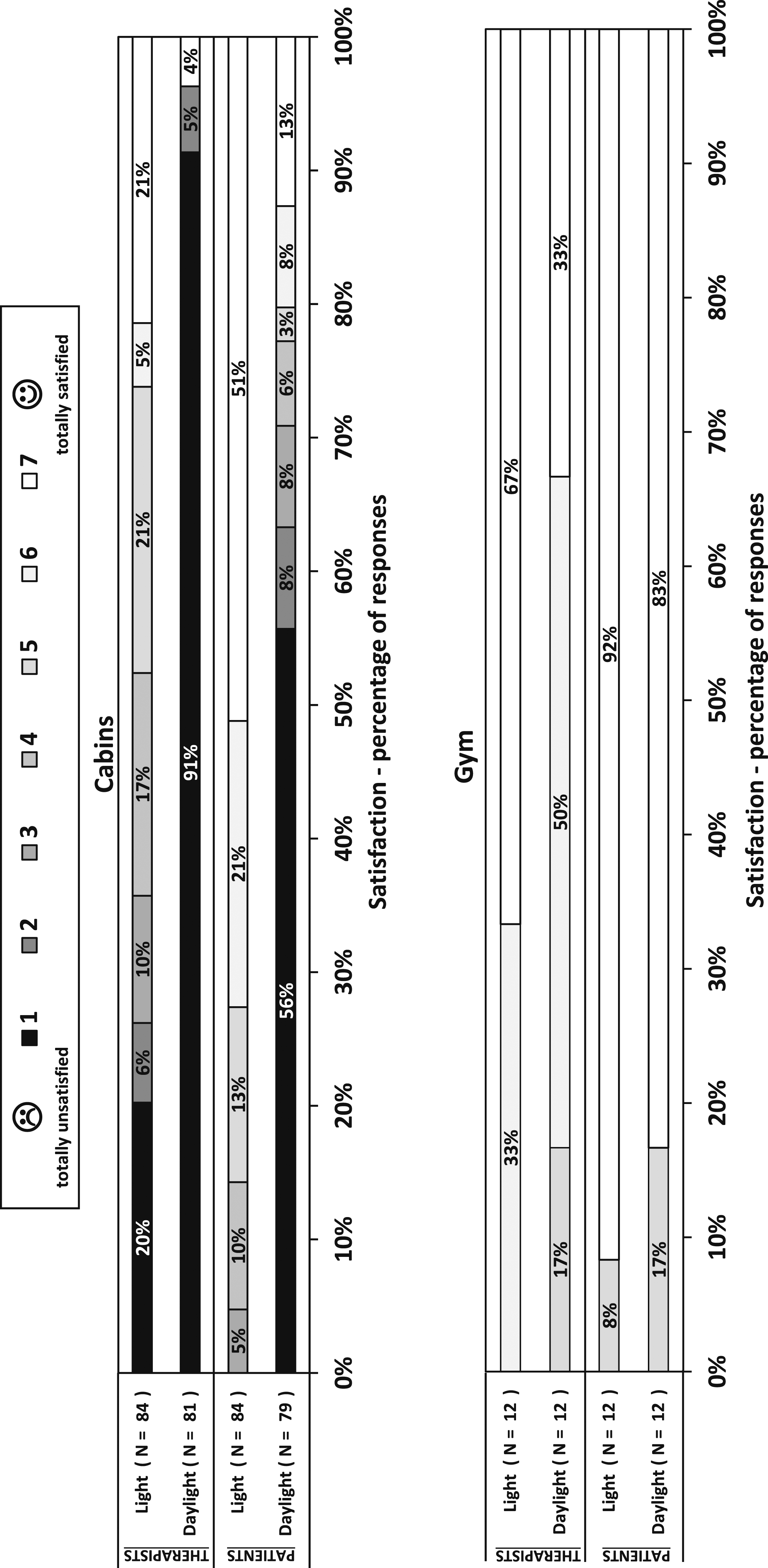
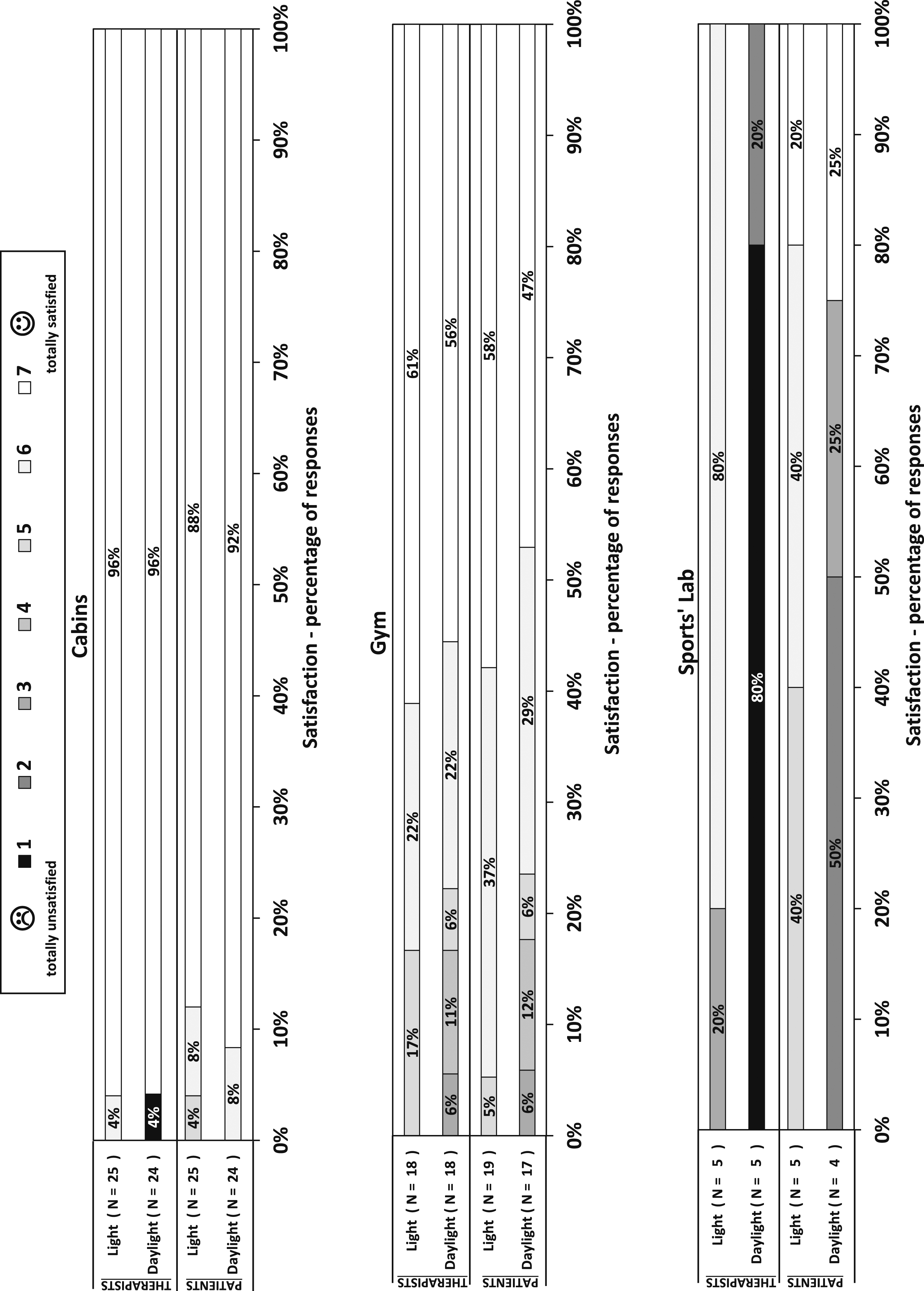
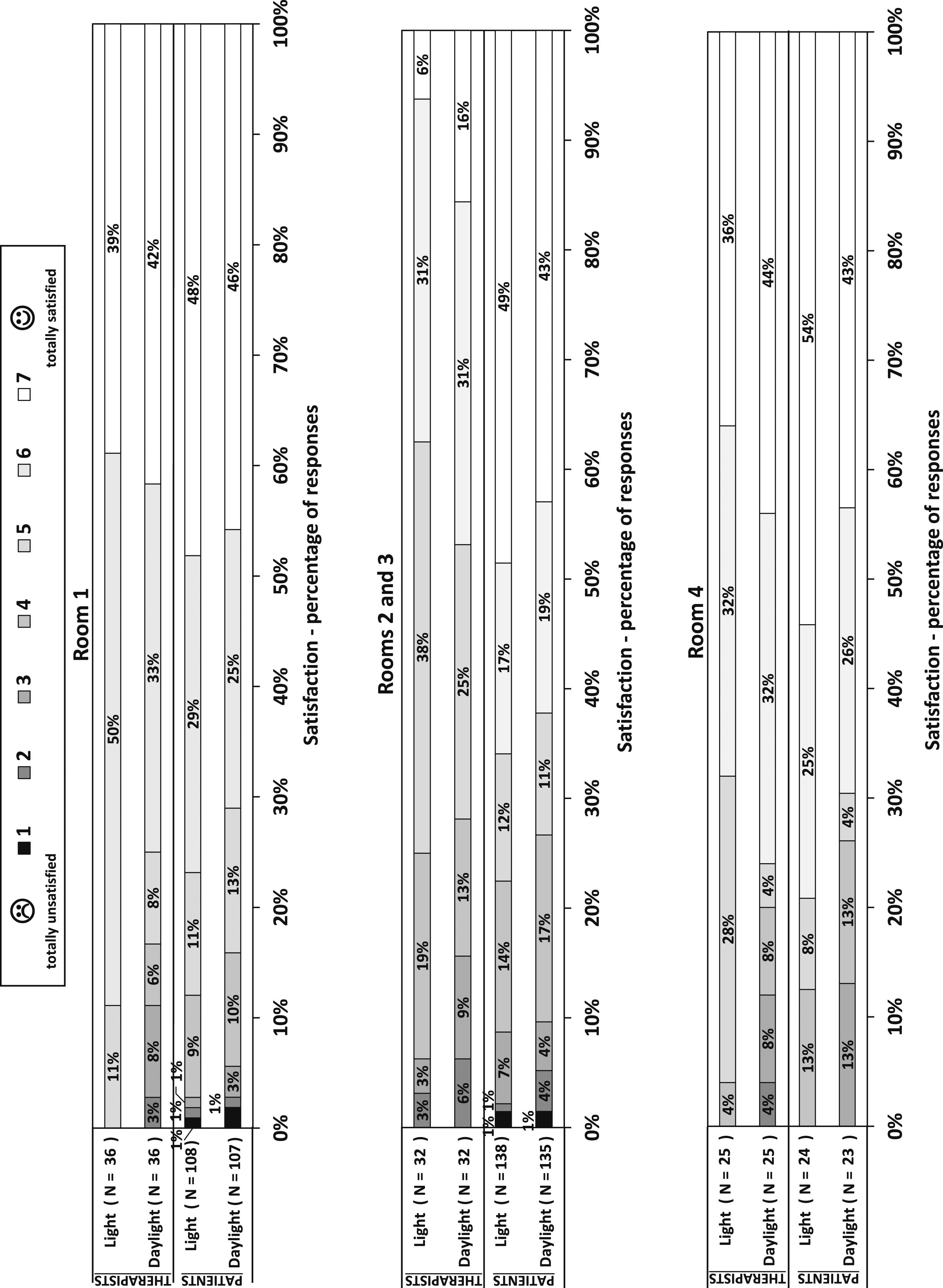
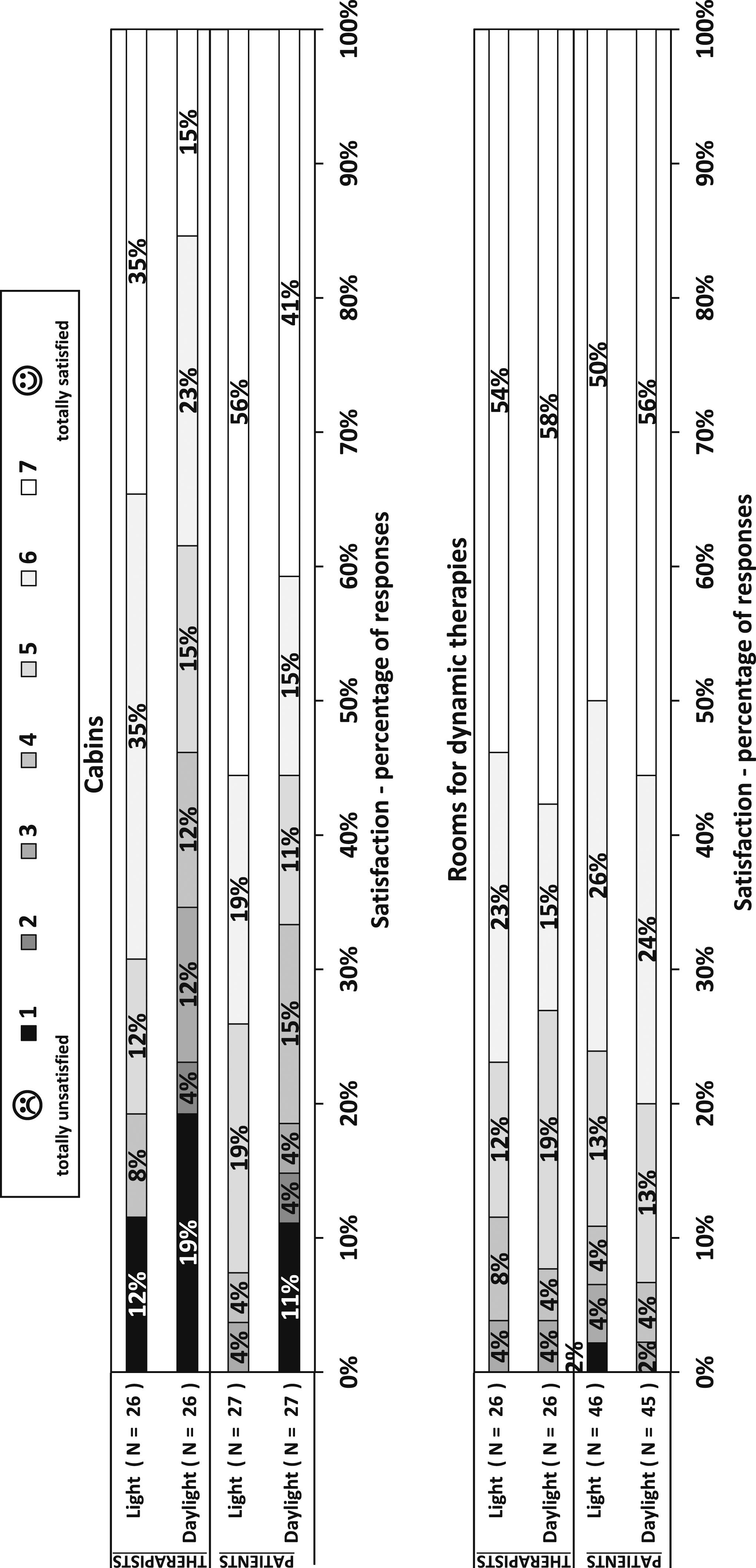
In the environments with no daylight access and artificial light only (cabins of Bolzano 1 and Sports’ Lab of Bolzano 2), the daylight satisfaction was the lowest. A remarkable percentage of occupants (therapists and patients in cabins of Bolzano 1 and only therapists in Sports’ Lab of Bolzano 2) also expressed a low light satisfaction (equal or below 4) in these rooms. Moreover, issues of ‘too high light’ were detected, probably due to the high illuminance, considerably exceeding the threshold of 300 lx. ‘Too low light’ was also reported in the cabins of Bolzano 1 due to the use of a desk light with the general light switched off by some therapists in order to avoid the too high illumination due to ceiling lamps (Section 3.1). Also, in rooms with issues in exploiting daylight due to low fenestration area, permanent use of shadings or orientation (Rooms 2, 3 and 4 of Copenhagen 1 and cabins of Copenhagen 2), considerable percentages of respondents with limited satisfaction (equal or below 4) were present. In rooms where measured values (Table 3 and tables in Supplementary Appendix 2, available as supplementary file) indicated an illuminance under the 300 lx threshold with only artificial lighting (Rooms 2, 3 and 4 of Copenhagen 1 and dynamic therapy rooms of Copenhagen 2), ‘too low light’ was indicated by a considerable number of occupants, especially therapists. This also happened in cabins of Copenhagen 2 due to the insufficient light when only the smaller lighting group (group 2) was on (Section 3.1). The issue of too low light was accompanied by limited light satisfaction in some cases (cabins of Bolzano 1, Rooms 2 and 3 of Copenhagen 1 and cabins of Copenhagen 2). Despite the similar low daylight access, less dissatisfied occupants were found in rooms for dynamic therapy of Copenhagen 2 with respect to the cabins; this is probably due to the higher mental focus and lighting quality necessary to perform static therapies. The cabins of Copenhagen 2 also showed some issues of ‘too high light’ when group 1 or both groups of lights were on, with illuminance values considerably above 300 lx (Section 3.1). The ‘too low light’ issue was not observed in the gym of Bolzano 1, as the low artificial lighting was balanced by the considerable amount of daylight (WFR of 0.67, with no use of shadings due to the presence of an opacified glass) during therapy times. Surprisingly, 24% of patients in rooms without windows were highly satisfied (satisfaction ≥5) with daylight; this aspect will be explored in Section 3.6. Many therapists reported glare and flash blindness in cabins of Bolzano 1. In these rooms, therapists sit or stand next to the bed, not directly watching the lamps. Moreover, the type of luminaires (ceiling recessed) do not scatter much light in the environment. For these reasons, the nuisance from glare and flash blindness was probably due to the high contrast between illuminance on the task areas and in the surroundings (see Figure 1(a), left and central). Glare was often reported in Rooms 2 and 3 of Copenhagen 1: Room 2 has three large windows facing West-South-West, from which direct light could disturb occupants during the activities (Table 2 and Figure 1(c), central). Moreover, as the low UO with natural light shows (Section 3.1), there was a high contrast between areas close to and far from the windows in this room. Despite some peaks in the measured illuminance, high light and daylight satisfaction were generally observed in rooms with high fenestration areas and massive daylight exploitation (gym of Bolzano 1, cabins and gym of Bolzano 2 and Room 1 of Copenhagen 1). The small number of occupants complaining about glare or flash blindness indicated a proper use of shadings in cabins of Bolzano 2 and Room 1 of Copenhagen 1. This routine, together with dark weather conditions often present in winter months, is the reason why some occupants indicated lower light and daylight satisfaction and ‘too low light’ as an issue in Room 1 of Copenhagen 1. On the other hand, the presence of 17% of therapists and 18% of patients with a daylight satisfaction equal to 3 or 4 in the gym of Bolzano 2 might be due either to the lack of natural light availability in the areas of the room farther from the daylight sources or the too direct sunlight close to them (Section 3.1).
3.5 Relationship between light and daylight satisfaction and illuminance level
In the cabins of Bolzano 1 and Room 1 of Copenhagen 1, it was possible to correlate the light and daylight satisfaction with the specific level of illuminance in these rooms at the time of responding. The following values (maximum, minimum and average) were calculated in the cabins of Bolzano 1 from the point-in-time measurements in order to estimate the illuminance at times of answering (see Section 2.4): 1. 788–975 lx (average: 873 lx) with 3 luminaires (answers before 23/11/2018); 2. 559–712 lx (average: 623 lx) with 2 luminaires (answers after 23/11/2018 and before the week of 08–14/04/2019); 3. 303–380 lx (average: 342 lx) with 1 luminaire (answers after the week of 08–14/04/2019); 4. 33–45 lx (average: 38 lx) with desk light (answers at all the times when the subjects indicated that the main recessed luminaires were off).
In Copenhagen 1, illuminance levels extracted from the long-term measurements were used.
The comparisons between illuminance and light satisfaction in the two rooms are shown in Figures 7 and 8, in terms of percentages of respondents giving different satisfaction levels for each illuminance interval in the rooms when the evaluations were given. In Room 1 (with windows) of Copenhagen 1, illuminance and daylight satisfaction were also compared (Figure 9). As it can be observed, when only artificial light was available (cabins of Bolzano 1), the lowest satisfaction levels were seen at the highest illuminance intervals, and the highest satisfaction was at about 300 lx. The different perception of the two groups of occupants is also further underlined since the levels of dissatisfaction among patients were not so low as among therapists, and less marked differences in their satisfaction among the illuminance levels were noticeable. Different observations can be made for the case with natural light available (Room 1 of Copenhagen 1): (1) With respect to cabins of Bolzano 1, higher satisfaction levels were present among therapists, and (2) the lowest satisfaction levels were expressed when a lower illuminance was present. This second point is true for both light and daylight satisfaction for the patient group and for daylight satisfaction for the therapist group. Comparison between the measured illuminance and the light satisfaction in cabins of Bolzano 1. On the y-axis, the percentages of answerers expressing different levels of satisfaction for different intervals of illuminance Comparison between the measured illuminance and the light satisfaction in Room 1 of Copenhagen 1. On the y-axis, the percentages of answerers expressing different levels of satisfaction for different intervals of illuminance Comparison between the measured illuminance and the daylight satisfaction in Room 1 of Copenhagen 1. On the y-axis, the percentages of answerers expressing different levels of satisfaction for different intervals of illuminance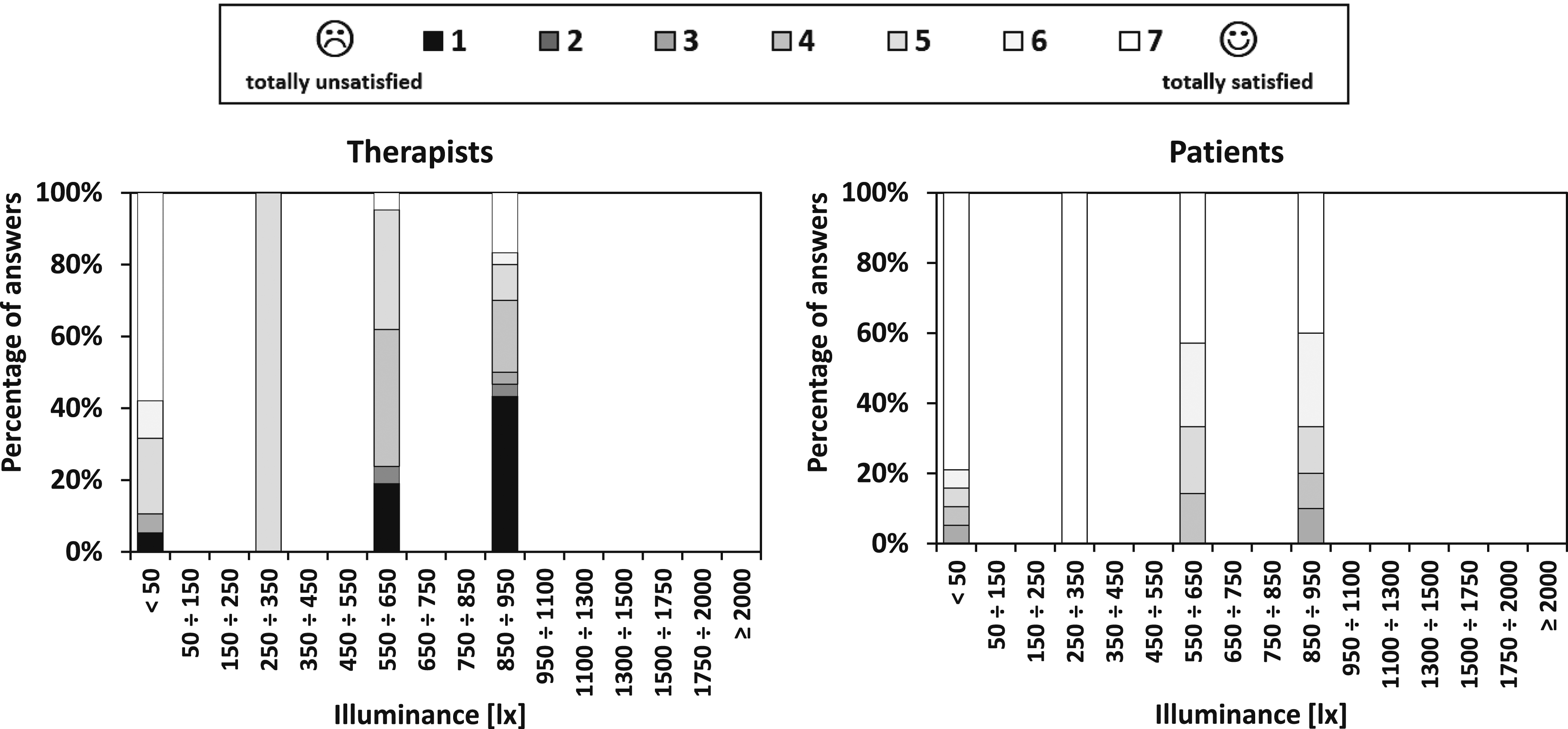
3.6 Satisfaction differences between user groups and light conditions
Results showing the differences between the satisfaction of therapists and patients and the dependences between light and daylight satisfaction of each category of occupants are reported in Table 5. The data from the gym of Bolzano 1 and Sports’ Lab of Bolzano 2 were not used in the analysis due to too few observations.
Values suggest a high difference between ratings of therapists and patients (Test 1) for the cabins of Bolzano 1. In the same case, also remarkable differences between light satisfaction and daylight satisfaction (Test 2) were found, in both the cases of therapists and patients. In this environment, both tests gave p-values lower than .01; moreover, effect size analyses, and median differences mostly confirmed the remarkable differences between the two samples of therapists and patients in terms of both light satisfaction (δ = −0.550 and ΔM = 3.0) and daylight satisfaction (δ = −0.349 and ΔM = 0.0) and the remarkable differences in terms of satisfaction with light and daylight for both therapists (δ = 0.699 and ΔM = 3.0) and patients (δ = 0.723 and ΔM = 6.0). Similar results were found for the cabins of Copenhagen 2: Test 1 revealed association of satisfaction with the type of occupant in terms of daylight satisfaction (δ = −0.277 and ΔM = 1.0); Test 2 suggested significant differences between light and daylight satisfaction of therapists (p-value < .01, δ = 0.355 and ΔM = 1.0) and patients (p-value = .022, δ = 0.267 and ΔM = 1.0). Association of satisfaction ratings with occupants’ type (Test 1) were also found in Rooms 2 and 3 of Copenhagen 1, both in terms of light (p-value < .01, δ = −0.400 and ΔM = 1.0) and daylight satisfaction (p-value = .012, δ = −0.275 and ΔM = 1.0).
Test 1 showed significant differences in satisfaction ratings of therapists and patients in rooms with low or no daylight access or in rooms where lighting issues were present, resulting in lower satisfaction especially for therapists (Sections 3.1 and 3.4). This tendency underlines how access to natural light positively influences both light and daylight satisfaction. In cabins of Bolzano 1, natural light was absent. Nevertheless, 24% of patients indicated a daylight satisfaction higher than 4 (Figure 3). This did not happen among therapists (96% indicated less than 2) and might be due to reasons of adaptation since patients spend a relatively small amount of time in cabins, they are aware of the lack of daylight, but they do not see it as a problem. Additionally, it may be due to a larger reliability of therapists, who were more directly involved in the study since it regarded their workplace, probably paid more attention in reading the questionnaire, and properly answer the questions.
On the other hand, Test 2 suggested that both therapists and patients often expressed different levels of light and daylight satisfaction in environments with significatively low or no daylight access.
The considered interiors were very different from an architectonical point of view (fenestration area, shadings, daylight access, etc.). These statistical analyses showed that light satisfaction and daylight satisfaction were generally associated. The analyses identified rooms with light and daylight issues. Generally, these were associated with lower daylight satisfaction among all the occupants, while the light issues (e.g. a too high illuminance in cabins of Bolzano 1) resulted mainly in a lower light satisfaction among therapists. This was probably due to a more prolonged exposure to the lighting conditions. In contrast, patients' lighting experience before the therapy could have been very different depending on the case and situation.
3.7 Correlation between (day)light satisfaction and thermal, indoor air quality and acoustic satisfaction
Tables 6 and 7 show the correlation coefficients between light and daylight satisfaction of therapists and patients and their thermal, indoor air quality (IAQ) and acoustic satisfaction rating. The tables also indicate the p-values and the correlation levels.
Patients’ light and daylight satisfaction were found correlated with the thermal, IAQ and acoustic satisfaction in all the cases except when strong issues were present: 1. The daylight satisfaction in Bolzano 1 was very low due to the absence of natural light and did not correlate with any of the other indoor environmental aspects. 2. The light satisfaction in Bolzano 2 was not correlated with the acoustic satisfaction. In fact, patients’ satisfaction with acoustics was lower in this centre. This was due to the presence of echo in the rooms for dynamic therapies.
The results for therapists showed a different trend, with correlations only when strong issues were present: 1. In Bolzano 1, there were significant correlations between light satisfaction and all the other satisfaction dimensions (low levels of light satisfaction expressed by therapists in these rooms) between daylight and IAQ satisfactions and between daylight and acoustic satisfaction. 2. In Bolzano 2, there were significant correlations between light and acoustic satisfaction. 3. In Copenhagen 1, there were significant correlations between light and IAQ satisfaction (in this centre, a lower IAQ satisfaction was expressed by therapists, mainly due to bad smells).
Significant correlations were always positive, meaning that higher satisfaction with one parameter resulted in higher satisfaction with another. Even though it is difficult to determine strong causal-effect relationships with correlation analyses, results highlighted a possible different psychological reaction to discomfort by therapists and patients. For therapists, stronger dissatisfaction with an environmental parameter other than the visual might also affect the light and daylight satisfaction, and vice-versa. In fact, light and daylight satisfaction were generally not associated with the other domains when the environments were satisfactory. The presence of significant correlations when issues were present denotes the possibility of positive or negative psychological influences of a stimulus on the other ones. This is another evidence of the effect of the longer exposure that therapists have to the indoor environment in physiotherapy centres. As they stay in their working environment for a long time, a single unsatisfactory parameter can influence the perception of the other environmental stimuli. This is not true for patients, who seemed to be more focussed on the single environmental parameter, as correlations were not found when higher dissatisfaction with one aspect was present. Patients were generally more satisfied with the environments than therapists. A higher satisfaction rating was indicated with all the domains, which may be why they were generally correlated. Moreover, as also highlighted in Section 3.6, therapists were probably more reliable and objective in answering, differentiating the satisfaction answers among the various domains more. When an issue with a domain was present, patients’ satisfaction with that domain dropped, making it more independent of the other fields. Correlations were generally stronger for light satisfaction, indicating that daylight satisfaction was a more independent parameter for both employees and patients, probably being clearly identifiable by therapists and patients (i.e. presence of windows, windows dimensions, view from windows, etc.).
4. Conclusions
In this study, light and daylight quality was investigated in four different physiotherapy centres located in Bolzano (Northern Italy) and Copenhagen (Denmark). Detailed measurements in such environments are particularly challenging due to the activities performed and privacy issues. Surveys including illuminance measurements and questionnaires answered by therapists and patients in terms of light satisfaction, daylight satisfaction and lighting issues were used. The study led to the following conclusions: 1. As expected, the lowest satisfaction with daylight was found in rooms where the light source was only or mainly artificial. In these rooms, low daylight satisfaction was often accompanied by low light satisfaction, especially among therapists. On the contrary, when natural light was available, a tendency was observed to have higher light and daylight satisfaction, provided that glare risks were avoided by a proper shading use. 2. Rooms where an adequate illuminance over the threshold of 300 lx could not be provided by artificial and natural light, showed ‘too low light’ to be often reported by occupants as a source of discomfort. Moreover, in some cases, a lower light satisfaction was indicated in these environments. In the rooms where values of artificial illuminance considerably above the threshold of 300 lx (i.e. 500–900 lx) were measured, ‘too high light’ was often indicated as an issue by the occupants. Glare was detected with either direct sunlight from the windows or strong contrast between lighting on the task area and ambient lighting. 3. The comparison of questionnaire responses with long-term illuminance measurements showed that with high daylight availability, only higher levels of light satisfaction and daylight satisfaction were present with high levels of illuminance. On the other hand, when no daylight was available at all, a lower light satisfaction with illuminance considerably above 300 lx was likely, especially among therapists. This also underlines the positive influence of daylight access on both the light and daylight satisfaction of occupants. 4. In general, light and daylight satisfaction of patients was not associated with gender, age and self-evaluated health status but depended on the occupant type. Therapists reported significantly lower light and daylight satisfaction in rooms with low daylight availability or lighting issues; perhaps due to a longer exposure to the visual discomfort in their working environment. Moreover, light and daylight satisfaction of therapists and patients were generally correlated, except in rooms with a lack of daylight availability and in rooms where daylight satisfaction was lower. This underlines how the presence of natural light positively influenced both the light and the daylight perception. In rooms with no windows, it was observed that patients who were not dissatisfied with daylight were present. This suggests their higher adaptability to the conditions in the therapy rooms (they spend only a little time in these rooms; therefore, they do not perceive the lack of daylight as an issue). Additionally, it suggests possible higher reliability of therapists when reading and answering the questionnaire (i.e. they were more directly involved in a study regarding their workplace). 5. Patients’ light and daylight satisfaction ratings were always correlated with the other satisfaction domains (thermal, IAQ and acoustic), except when there was stronger dissatisfaction with one of the domains. Patients generally expressed a high satisfaction except when issues with a domain were present. Therapists’ light and daylight satisfactions showed an opposite trend, as they were never correlated with any other domains, except in the cases where an indoor environmental parameter was found unsatisfactory. Therapists were generally differentiating their answers on the different domains more, resulting in the absence of significant correlations in most cases. Nevertheless, employees stay in their working environments longer. The continuous exposure could make negative aspects of the environment psychologically influence the perception with other domains. Low satisfaction with light and daylight can negatively influence thermal, IAQ and acoustical satisfaction, and vice-versa.
Environments like physiotherapy centres are peculiar as diverse sets of occupants share them: therapists and patients, who perform different activities, have different age and health conditions, occupy different positions in the rooms and have different durations of exposure to the environments. The diversity in such populations influence the general comfort of the occupants. This work is a first step to understand lighting satisfaction in such facilities with diverse occupants and needs. It evidenced how visual satisfaction is an aspect to be taken into account in physiotherapy centres design. In particular, the presence of natural light is an element that is fundamental for the satisfaction of physiotherapy centres’ occupants. This is particularly true for physiotherapists. It is of primary importance to design the environments in order to ensure as much daylight as possible and, consequently, to ensure a proper regulation through shadings to avoid glare. A proper level of illuminance needs to be maintained since lack or excess of illuminance can cause discomfort. In this framework, further research studying the importance of the synergy of dimmers’ and shadings’ operations in physiotherapy centres could be provided. This study evidenced how the availability of daylight and maintenance of good levels of illuminance are essential, since they might also influence the other satisfaction aspects, such as thermal, indoor air quality and acoustic.
These conclusions, if integrated with other studies, can help to develop guidelines to better meet the lighting requirements of occupants of physiotherapy centres.
Supplemental Material
sj-pdf-1-lrt-10.1177_14771535211046521 – Supplemental Material for Lighting conditions in physiotherapy centres: A comparative field study
Supplemental Material, sj-pdf-1-lrt-10.1177_14771535211046521 for Lighting conditions in physiotherapy centres: A comparative field study by L Zaniboni, M Sarey Khanie, G Pernigotto, J Toftum, A Gasparella and BW Olesen in Lighting Research & Technology
Footnotes
Acknowledgements
The authors kindly thank the four physiotherapy centres’ staff and patients for actively collaborating to develop this research.
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship and/or publication of this paper.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the project ‘Klimahouse and Energy Production’ in the framework of the programmatic–financial agreement with the Autonomous Province of Bozen-Bolzano of Research Capacity Building.
Supplemental material
Supplemental material for this article is available online.
Appendix 1
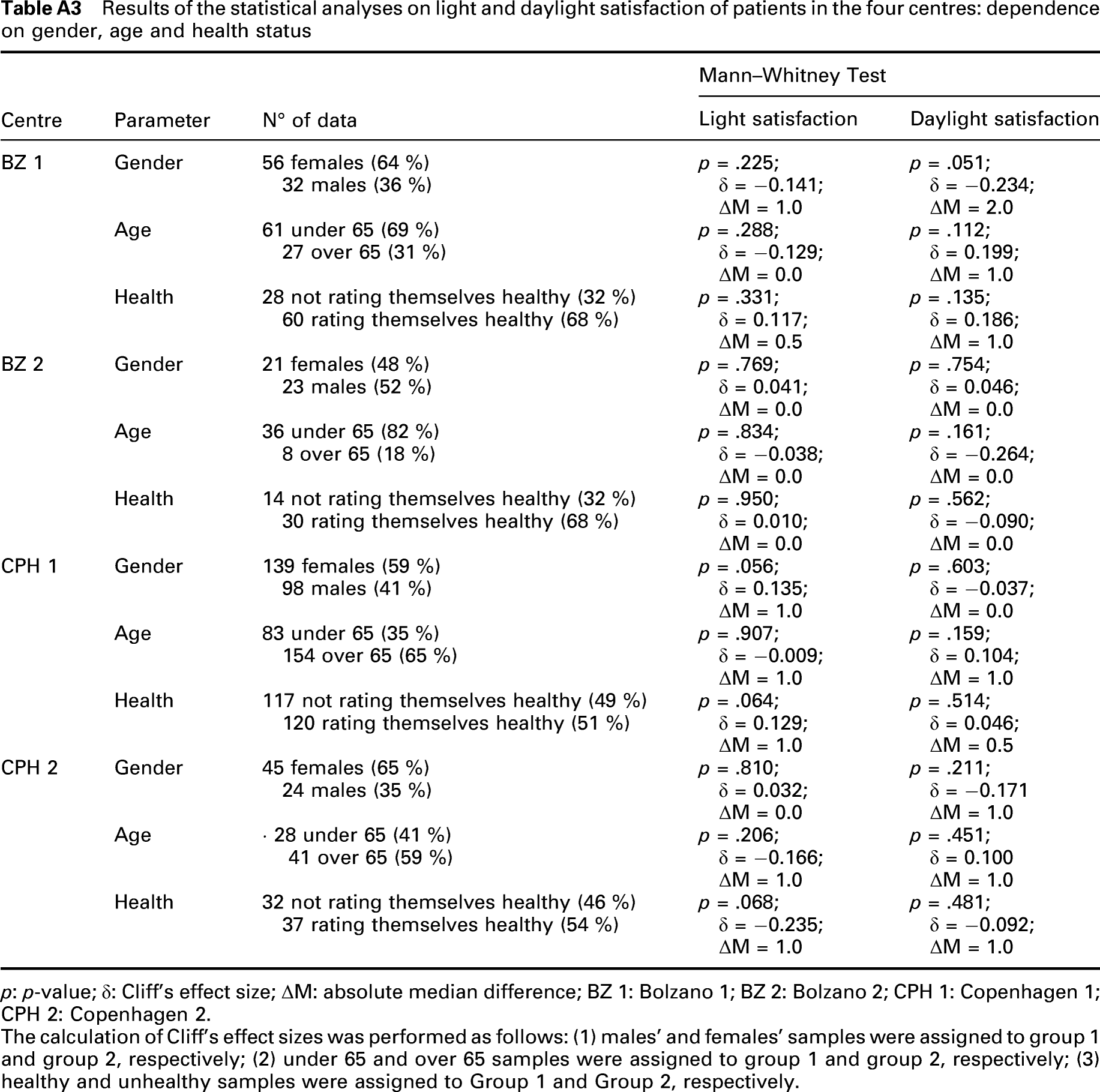
Results of the statistical analyses on light and daylight satisfaction of patients in the four centres: dependence on gender, age and health status
| Centre | Parameter | N° of data | Mann–Whitney Test | |
|---|---|---|---|---|
| Light satisfaction | Daylight satisfaction | |||
| BZ 1 | Gender | 56 females (64 %) 32 males (36 %) |
p = .225; δ = −0.141; ΔM = 1.0 |
p = .051; δ = −0.234; ΔM = 2.0 |
| Age | 61 under 65 (69 %) 27 over 65 (31 %) |
p = .288; δ = −0.129; ΔM = 0.0 |
p = .112; δ = 0.199; ΔM = 1.0 |
|
| Health | 28 not rating themselves healthy (32 %) 60 rating themselves healthy (68 %) |
p = .331; δ = 0.117; ΔM = 0.5 |
p = .135; δ = 0.186; ΔM = 1.0 |
|
| BZ 2 | Gender | 21 females (48 %) 23 males (52 %) |
p = .769; δ = 0.041; ΔM = 0.0 |
p = .754; δ = 0.046; ΔM = 0.0 |
| Age | 36 under 65 (82 %) 8 over 65 (18 %) |
p = .834; δ = −0.038; ΔM = 0.0 |
p = .161; δ = −0.264; ΔM = 0.0 |
|
| Health | 14 not rating themselves healthy (32 %) 30 rating themselves healthy (68 %) |
p = .950; δ = 0.010; ΔM = 0.0 |
p = .562; δ = −0.090; ΔM = 0.0 |
|
| CPH 1 | Gender | 139 females (59 %) 98 males (41 %) |
p = .056; δ = 0.135; ΔM = 1.0 |
p = .603; δ = −0.037; ΔM = 0.0 |
| Age | 83 under 65 (35 %) 154 over 65 (65 %) |
p = .907; δ = −0.009; ΔM = 1.0 |
p = .159; δ = 0.104; ΔM = 1.0 |
|
| Health | 117 not rating themselves healthy (49 %) 120 rating themselves healthy (51 %) |
p = .064; δ = 0.129; ΔM = 1.0 |
p = .514; δ = 0.046; ΔM = 0.5 |
|
| CPH 2 | Gender | 45 females (65 %) 24 males (35 %) |
p = .810; δ = 0.032; ΔM = 0.0 |
p = .211; δ = −0.171 ΔM = 1.0 |
| Age | · 28 under 65 (41 %) 41 over 65 (59 %) |
p = .206; δ = −0.166; ΔM = 1.0 |
p = .451; δ = 0.100 ΔM = 1.0 |
|
| Health | 32 not rating themselves healthy (46 %) 37 rating themselves healthy (54 %) |
p = .068; δ = −0.235; ΔM = 1.0 |
p = .481; δ = −0.092; ΔM = 1.0 |
|
p: p-value; δ: Cliff’s effect size; ΔM: absolute median difference; BZ 1: Bolzano 1; BZ 2: Bolzano 2; CPH 1: Copenhagen 1; CPH 2: Copenhagen 2.
The calculation of Cliff’s effect sizes was performed as follows: (1) males’ and females’ samples were assigned to group 1 and group 2, respectively; (2) under 65 and over 65 samples were assigned to group 1 and group 2, respectively; (3) healthy and unhealthy samples were assigned to Group 1 and Group 2, respectively.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.