
Abstract
The procedures for structuring clinical ethics case reflections in a childhood cancer care setting are presented, including an eight-step model. Four notable characteristics of the procedures are: members of the inter-professional health care team, not external experts, taking a leading role in the reflections; patients or relatives not being directly involved; the model explicitly addressing values and moral principles instead of focussing exclusively on the interests of involved parties; using a case-based (inductive) rather than principle-based (deductive) method. By discusing the advantages and disadvantages of the proposed procedures, our paper aims to contribute to the literature on models and procedures for ethical analysis that can be used in clinical settings. It is suggested that our proposed procedures have some advantageous features when it comes to promoting health care staff’s learning to structure their thinking about ethical issues.
Introduction
When a child is seriously ill, the whole family is affected, and pediatric cancer care often entails difficult ethical problems. 1 Ethical problems are often derived from value conflicts regarding what is the right thing to do in the clinical context. 2 Value conflicts can occur within and between individuals. They might, for instance, arise from differences related to cultural and religious beliefs. 3 Inter-professional conflicts are common in relation to ethical problems and it has been observed that parents and staff in pediatric care may have conflicting views on what is best for the child. 4 In pediatric oncology, ethical problems include continuation or termination of the curative intended treatment, how to inform those concerned about the development of the disease and how to handle parents’ requests in the light of the patient’s interests.3,5,6
Clinical ethics case reflections
One way to deal with ethical problems in health care is through clinical ethics case reflections. Such reflections may serve different ends, including handling concrete ethical problems in care, providing arguments for decision-making and providing training in ethical awareness, competence and argumentation.7–9 Ethics case reflections in the team can provide health care staff with tools for ethical analysis, a base to collaborate as a team, greater inter-professional understanding, and a common intention with the care.10,11 Research has shown that when health care staff are given the opportunity to participate in ethics case reflections, their ethical awareness and competence increase. 8
There are several models for ethical analysis of clinical cases, including case-based models such as the Norwegian model for case reflection, 12 the dilemma method,8,13,14 and different principle-based models.15–17 Principle-based models are deductive in the sense that they specify beforehand what moral principles and values to apply to the case, while case-based models are inductive; that is, case-based models focus on the values and moral principles that are found to be relevant in the case. 15 Although there are similarities between the different case-based models, the context and the organization of clinical ethics case reflections vary widely between and within countries.18–22
The context and the organization differ regarding the legal status of the decisions made, whether or not patients or relatives are included in the reflection, and whether external consultants or members of the health care team take the leading role in the reflection and decision-making.18–22 There are also considerable differences between countries regarding the extent to which clinical ethics case reflections are established in the health care system.
In Norway, for instance, clinical ethics committees are established at all hospital trusts using a six-step model for reflection on individual patient cases 12 while neither ethics committees nor ethics consultation practices are established nationwide in Sweden. There are initiatives in Sweden to establish ethics committees in many county councils, and work continues to identify appropriate tasks for these committees. Clinical ethics case reflections are as yet not among the top priorities. However, there are initiatives at individual hospitals, and in a few of them, clinical ethics case reflections are fairly well established.
Clinical ethics case reflections at the Karolinska University Hospital
The Karolinska model for ethical analysis.
However, there is still a potential for further improvement of the Karolinska model because (1) it focuses heavily on individuals interests and (2) it is deductive regarding how values and moral principles are introduced in the case reflections. The procedures for the clinical ethics case reflections that will be proposed in this paper constitute a development and modification of the Karolinska model. We will describe our proposed procedures as well as the underlying rationale.
Objectives
The central aims for this paper were to describe the procedures, including a model, for clinical ethics case reflections and to discuss pros and cons of the presented procedures.
Procedures for ethics case reflections
In this article, we present the details of how the clinical ethics case reflections are to be carried out. Experiences described derive from the authors. The first author has previous experiences from participating in clinical ethics case reflections, and the second and last authors have experiences as participants as well as facilitators.
Organization
At the pediatric oncology centre, clinical ethics case reflections can be initiated by any staff member who experiences an ethical problem in a case by contacting a consultant nurse. The cases should be prospective. The consultant nurse will send a brief summary of the case to the first and second authors who will review the case to confirm that it is an ethical problem rather than an organizational, professional or psychological/emotional problem. The consultant nurse will then discusses the problem briefly with the physician responsible for the relevant diagnostic group.
Before the clinical ethics case reflection begins, the team of physicians at the centre will hold a meeting about the case to clarify the medical facts. This is in order to prevent time in the clinical ethics case reflection being spent on medical issues only. Reasons for postponing clinical ethics case reflections may be that a second opinion or a crucial test result is pending. The consultant nurse is responsible for arranging the meeting in cooperation with the first author, and the meeting will take place in a small conference room or other convenient facility at the hospital and lasts approximately 1 to 1½ hours.
If circumstances permit, the appointed facilitator for the reflections will be given a brief summary of the case – a sentence or two – by e-mail beforehand (such as ‘The reflection concerns a three-year-old girl with a brain tumour, whose parents disagree about her treatment.’). The first author will introduce the meeting by briefly explaining how it will be conducted, making time for the introduction of the participants and for setting the rules of the meeting, such as time limits and confidentiality. When the clinical ethics case reflection is completed, documentation of what has been discussed will be entered by one of the team members into the patient’s medical record.
Participants
Participants will be the inter-professional team of health care staff involved directly in the care of the patient concerned – mainly physicians and nursing staff – but there can also be other professionals such as psychologists or social workers. Health care staff from other units involved in the case, such as staff from the unit for advanced home care of children, will also be invited to participate. All in all, the number of participating health care staff will vary between 4 and 10 to promote good interactions.26,27 There will be no permanent teams participating in the ethics case reflections, but rather different compositions of team members each time.
Finally, there will be a facilitator for the reflection meeting. This may be a professional ethicist or a health care professional with previous experience of facilitating clinical ethics case reflections in organized form. Patients or parents will, however, not participate; reasons for this will be discussed below.
The role of the facilitator
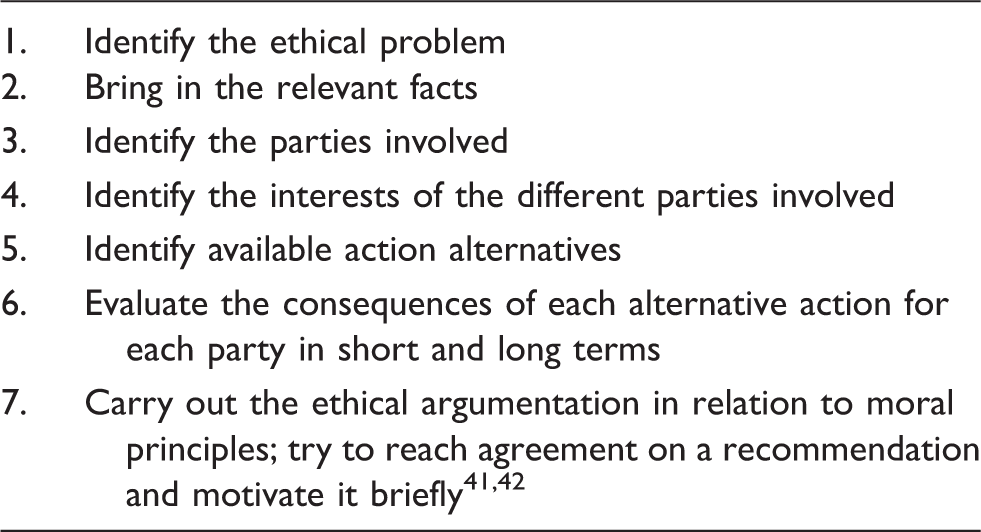
Modified version of the ‘Karolinska model for ethical analysis’.
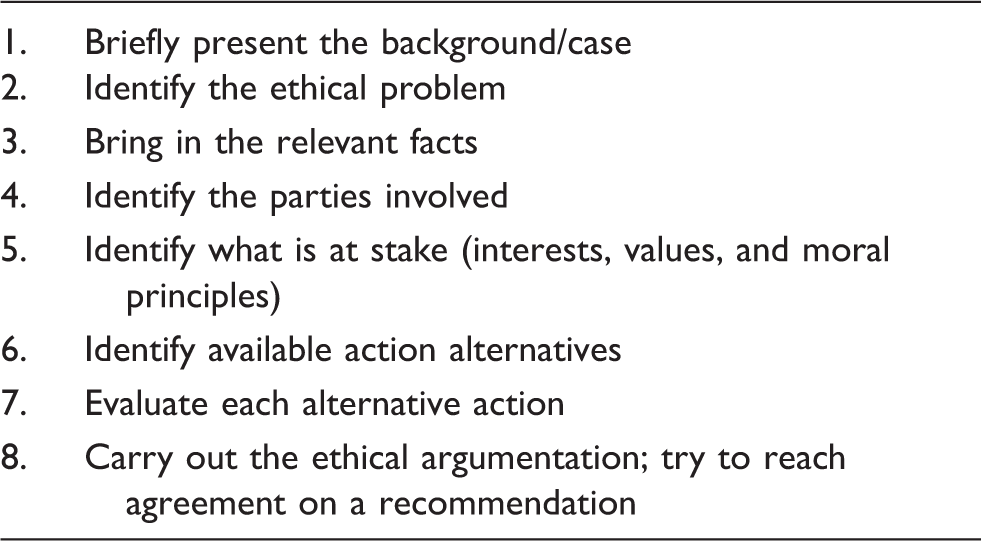
The modified version of the ‘Karolinska model for ethical analysis’
The different steps of the model for clinical ethics case reflections are presented below.
Step 1: Present the background/case in brief
The facilitator asks for a brief presentation of the case to be discussed. This is normally done by one of the physicians, although others might add certain details. The background should include age and medical condition of the patient and a short description of the present situation.
Step 2: Identify the ethical problem
Participants are asked to specify the ethical problem that is to be discussed. This may take time to settle or be resolved quickly. There may often be more than one ethical problem involved, but participants are asked to choose the one most urgent or important. Regardless, the initial specification may get revised later in the reflection process. The problem is preferably formulated as a question starting with ‘Should I/we…’.
Step 3: Bring in the relevant facts
In this step, participants are asked to fill in the picture by bringing in additional facts that are relevant to the case. First, medical facts are presented, including any uncertainties that are relevant to the case. Then other facts, such as legal, cultural, religious/existential or psychosocial aspects, are presented if perceived to be relevant.
Step 4: Identify the parties involved
The stakeholders are identified at this stage. Who else, apart from the patient and his/her parents or guardians, are directly involved or could be affected by the decision? This could include siblings, grandparents, other relatives, health care staff, other patients and health care staff at other units, for example, if care at an intensive care unit could be needed as a result of the decision. Even if the patient and the family are the most important parties, it is also essential to identify other stakeholders.
Step 5: Identify what is at stake (interests, values, and moral principles)
When the stakeholders are identified, it is time to identify the relevant personal interests, values and moral principles. A guiding question could be: What is important and what does that mean in this case? Other questions include: What do the stakeholders want? What does the patient need? What values and moral principles are relevant to the case? The different aspects may not be equally important, but at this point any aspect that seems at least somewhat important should be identified and brought into the open.
Step 6: Identify available action alternatives
Against the backdrop of the previous reflection, what are the preliminarily reasonable, viable and available action alternatives? Since the basic action-related ethical question is ‘What should I/we do?’, the core practical dichotomy regarding alternative actions in health care is ‘Should we or should we not … [e.g. terminate curative treatment and switch to palliative care]?’ Creativity is encouraged to find alternative solutions, since the more obvious main alternatives can often be divided into different alternative ways of executing them; for instance, if the preferred alternative is to tell the patient about the latest developments of the disease, it requires a careful consideration on why, what and how. 28
Step 7: Evaluate each alternative action
The next step is to evaluate the identified alternatives and specify the pros and cons of each alternative in the light of medical and other facts as well as relevant values and moral principles.
Step 8: Ethical argumentation; trying to reach agreement on a recommendation
At the last step, there is explicit ethical argumentation for and against specific alternatives, with the purpose of identifying an alternative that the inter-professional health care team can agree upon as the preferable choice, after having considered and properly evaluated the relevant aspects of the case. In the reflection, the participants are encouraged to be specific; if they, for instance, argue in favour of one action referring to respect for the patient, then the facilitator might ask them to clarify what they want to see with respect in regard to the patient, for example the right to decide or the right to privacy.
These reflections might, for instance, involve weighing the patient’s or relatives’ present preferences against the long-term health and well-being of the patient. Or, if the patient has only slim chances of survival, weighing continued treatment with only a faint hope of success against higher quality of life at the end of life but with no hope of recovery. At other times, respect for the child’s growing autonomy might stand against the parents’ wish that certain information is withheld from the child. This is a delicate situation since it is important not only to respect patient autonomy but also to maintain a good relationship with the parents. An action-oriented conclusion of such a reflection might, for example, be: we should discuss with the parents once again about what we could tell the patient in an, for them, appropriate way. We should also inform them about the consequences of withholding the information from the patient. It would be wrong to pretend to the patient that the situation is very different from what it is, but it is also important to keep a good relationship with the parents. If disagreement remains at the end of the reflection, the meeting concludes that no consensus could be reached and participants agree to disagree.
It should be noted that these clinical ethics case reflections have no formal authority – it is still the physicians responsible for the treatment who have the formal and legal responsibility to make the decisions. The case reflections may nevertheless play an advisory role, not least since one or more treating physicians are always among the participants, but also since many different aspects have been brought up and reflected on.
Comparison with the Karolinska model
Before discussing the pros and cons of the presented model for clinical ethics case reflections, we will clarify how our version relates to the Karolinska model, from which it originates, and give our arguments for the modifications made.
First, in our model, it is spelled out that the reflection starts with a short presentation of the case – this step is not explicitly included in the Karolinska model (Table1). We also made changes to the formulations of three other points: steps 4, 6 and 7 (see tables).
Step 4 of the Karolinska model – ‘Identify the interests of the different parties involved’ – might make it seem as if the problem is only about individual interests and not about ethical issues. It has been explained to us that the reason for putting it this way, although philosophically inadequate, was to stress the importance of paying proper attention to the individuals concerned in the specific case (patients, relatives, etc.) and their wants, hopes and desires as a means to counter any paternalistic tendencies. Furthermore, ‘interests of the different parties’ can arguably be interpreted widely enough to cover also, for instance, justice. Also, health care staff might find it challenging to answer questions about values and moral principles since they may not have training in ethics. However, by asking a question of what is important and at stake in the case, the most important values and principles could be discovered in the words of health care staff rather than in the words of ethicists. We therefore changed the step to ‘Identify what is at stake in terms of interests, values, and moral principles’, mainly because we want it to explicitly state that this step includes identifying values and principles that are relevant in the case. This also makes explicit that our model is inductive regarding its use of values and principles. Furthermore, the chosen wording throws some light on the next step (Step 5), ‘Identify available action alternatives’. The idea here is not to identify any possible alternative, but those worth considering in the following reflection.
The phrasing of step 6 in the Karolinska model – ‘Evaluate the consequences of each alternative action for each party in short and long terms’ – was also modified since it was unfortunate in more than one way. As with step 4, it may sound as if the focus should be exclusively on to what extent individuals get their personal interests, including wishes, satisfied. It may be the case that not all wishes are morally relevant. It may also be the case that other things, apart from individual interests, matter. Also, putting the evaluation exclusively in terms of consequences is inadvisable since it might be taken to imply that only consequentialistic considerations matter. Models for clinical ethics case reflections should not include that kind of restrictions.
Step 7 of the Karolinska model – ‘Carry out the ethical argumentation in relation to moral principles; try to reach agreement on a recommendation and motivate it briefly’ – has been modified by the deletion of the reference to moral principles, in order not to invite the reading that we recommend a principle-based approach. On the contrary, we believe that a case-based model is more appropriate in the clinical context, since it focusses on the values and principles that are identified as relevant in the specific case discussed. A principle-based approach, on the other hand, may hinder participants from feeling free to bring up aspects of the case that they find important but that do not clearly fit with the pre-established principles.
We have also decided that the steps of our modified model should not be strictly applied. They are meant to support the clinical ethics case reflection by providing a structure, but flexibility is allowed in order to facilitate constructive dialogue. The basic idea, after all, in this and many other models for ethics deliberation, is to get a decent picture of the case, those involved, what is at stake, and how that relates to the alternatives at hand. For instance, new facts can be brought up as they become relevant, some action alternatives may be identified and evaluated jointly instead of separately, and the meeting may, even quite late in the reflection, return to the question of what the ethical problem to be solved is.
In summary, the essential differences between the Karolinska model and our modified model are that our model is explicit about (1) focussing on relevant values and moral principles rather than merely individuals’ interests and (2) being inductive (case-based) regarding how values and moral principles are introduced in the case reflections.
Discussion
The decisional status of the ethics case reflection
In Sweden, decisions made in clinical ethics case reflections do not have legal status. However, if the patient-responsible physician and nurse are included in the reflections, their decisions can be based on the conclusions drawn. Even if a full consensus cannot be reached, a common understanding of the issue and a plan of action can be established at the end of the reflection. In a previous study that evaluated ethics case reflections without the aim of leading to consensus or a recommendation, the nurses were very frustrated about the lack of solutions to the problems produced in the reflection. 11
Patients and relatives
One potential disadvantage with the way we will organize clinical ethics case reflections relates to the fact that the reflections take place without the patient or his/her parents being present. Parents and other relatives might be worried that decisions are taken over their heads at these reflections even if they are informed that the clinical ethics reflections are only advisory. Another potential disadvantage is that if the question of what the patient or parents believe or want is raised, then they are not there to inform the meeting in their own words – this leaves the participants at the meeting to, at best, make an insightful guess if the specific topic has never been discussed directly with the patient or the parents. Even if the health care team members will do their best to present the views of the patient and the parents at the meeting, what they tell will be filtered through their own perceptions and understanding. This means that these views might come out differently if the patient or parents would get the opportunity to express them directly at the meeting.
Quite a lot has been written about the pros and cons of patients or relatives participating in clinical ethics case reflections. One frequently mentioned advantage is that the patients’ participation could provide additional facts about their own well-being, experiences, beliefs, hopes and wishes, thereby reducing the risk that their interests will not be sufficiently considered.19,21,29 Participating patients or relatives may also be able to identify ethical problems and arguments that the health care team has failed to recognize.30,31 Participation may also have an educational value. 18 The literature, thus, suggests that the participation of the patient and/or the parents could improve the reflection.19,21,29
There is, however, also an awareness of the difficulties, such as stress suffered by patients and relatives to participate, but also that the patient’s views and wishes (or those of the relatives) could be given too much consideration when there is direct personal interaction during clinical ethics case reflections.18,21,31
There are also practical circumstances that speak against including patients or parents. First, some staff members have been reported to feel uneasy and uncertain when patients participate.33 In Norway, where the patient and/or the public are sometimes represented, the ethics case reflection is performed in the established committees rather than in the health care team.34 To include patients or parents in ethics case reflections performed in the health care team, with varying levels of experience and training in ethics case reflections, is something completely different.
Second, to do so would require two meetings rather than one, since it seems necessary for one of the meetings to be with health care personnel only, so they can speak freely about medical and other aspects of the case.35,36 Otherwise, there is the risk that some of the information will not come up in the reflection or will be expressed in an overly considered and sensitive way. 33 Ethical problems often include aspects of communication and information 37 and questions like what to say to the patient/parents and how to say it cannot be handled in a forum open to patients/parents. Furthermore, if there are two meetings, then the risk reoccurs that parents or relatives might be worried that decisions are taken over their heads, at the first meeting.
Third, it is often difficult to find time for the reflections when those in the health care team who are particularly engaged can participate. Finding time for two meetings (or a longer time-slot if placed directly after each other) within a short space of time will be even more difficult. It may also be the case that there is a narrow time frame because of the patient’s deteriorating health condition. It has also been argued that if patients/relatives participate in clinical ethics case reflection meetings, then a follow-up may be needed to avoid negative reactions. 18 This would further increase the practical difficulties.
However, the counter-arguments regarding the need for two meetings are circumstantial rather than principal in nature. If it is practicable to create time within a relevant time-frame to arrange two meetings, and if someone in the health care team can talk to the patient/parents afterwards, it can add value and lead to a better foundation for decision-making if the patient/parents participate. Whether practicable or not is a matter of resources. Considering this and the arguments above, we have decided not to include patients or parents in the reflections.
Decision-makers or facilitators?
The literature on clinical ethics case reflections shows that there are many different practices.18–22 One important dividing line goes between, on one hand, reflections in the sense that ethics consultants or ethics committees gather information, analyse alternatives and decide on a well-reasoned recommendation and, on the other hand, reflections where one or several consultants serve as facilitators to reflections mainly held by members of the health care team. It is worth underlining that in our clinical ethics case reflections, the members of the health care team in question will do the actual presentation, analysis and argumentation regarding the case, aided by the facilitator.
In the light of the potential for health care personnel to improve their ability to identify, analyse and deal with clinical ethical issues, the latter approach is clearly preferable in our view. This is so because the health care team is not only presented with a recommended solution and a summary of the reasons for doing so, but also gets the opportunity to follow the line of reasoning from the beginning to the end. Furthermore, each member of the health care team gets the opportunity to take part in shaping the argumentation process. There is, thus, a greater chance of learning from this procedure than from alternatives where the reasoning takes place elsewhere. However, we cannot exclude the possibility that two facilitators would be better than one in cases where one facilitator guides the reflection, while the other observes, takes notes and ensures that no important aspects are left out.
Except from ethics training, the facilitator would benefit from skills such as responsiveness, proper communication and structure, to be able to aid the ethics case reflection, according to our experience. In cases where health care professionals have strong conflicting views, the role of the facilitator becomes more important and also more difficult. Then it becomes particularly important to shift the attention from the participants’ strongly held positions to the arguments for the different alternatives, while trying to make sure that everyone is, and feels, included in the reflection.
Inter-professional interaction
The group composition is important for ethics case reflections. It has been argued that there should be a balance between homogeneity and heterogeneity in the group in order to get an atmosphere of sharing while promoting dynamic group interaction. 38 If pre-existing health care teams participate in ethics case reflections, this could be useful for the group interaction because the group composition is familiar and the group therefore might feel more secure. 39 However, pre-existing power structures can be a challenge. Some research indicates that an open and constructive reflection is facilitated by having heterogeneous non-pre-existing groups. 40 Health care is a hierarchical environment. The physician has the decision-making role, and therefore a great medical and legal responsibility for the patient’s health. Thus, there is a risk that the opinions of physicians are given more attention by the other participants in the ethics case reflections, and that nursing staff are afraid to raise their voices. In a previous study, the presence of managers was found to cause an imbalance in the power structure and uncertainty in the groups. 2
It will be the job of the facilitator to try to counter any tendencies to use power instead of arguments, with the help of the participants, based on the implicit agreement that an important point of having the ethics case reflections at all is to openly test the arguments that can be made for the alternative actions. Misuse of power in reflections can be countered by recognizing attempts to win the discussion without genuine arguments and requiring that participants spell out their arguments. Similarly, dismissals of arguments must not be accepted without proper counter-arguments.
In spite of potential difficulties with pre-existing power structures, we would like to argue for the involvement of inter-professional teams in clinical ethics case reflections. One reason for this is the importance of deep and relational knowledge about the case. The different members of the inter-professional team are important to get a full picture of the situation, since not only medial facts are important, but also social, cultural and psychological facts about the patient and his or her family. Previous research also indicates that an inter-professional dialogue is required in order to reach a sufficiently complete picture of the patient. 29
Another reason for involving inter-professional teams in clinical ethics case reflections is that such reflections can be useful as a learning process, increasing awareness of ethical problems and argumentation. In a previous study, where participants evaluated goals met during ethics case reflections, they gave high scores for goals related to knowledge of and insight in moral issues as well as goals such as to pay attention to reasons and arguments and to improve mutual understanding. 10 Research also shows that ethics case reflections in inter-professional teams improve communication. 8
Further research needed
More research is needed to evaluate procedures, models, and processes. A research project is presently planned to offer health care personnel clinical ethics case reflections on request at the pediatric oncology centre at Karolinska University Hospital in Stockholm. The project will study the group process of ethics case reflections, including the participants’ main concerns and how they deal with them. The reflections will involve health care staff and a facilitator.
Conclusions
This paper presents procedures for carrying out ethics case reflections in the clinical context. Such reflections may be carried out satisfactorily in many different ways. Yet some features may be more helpful than others. These are some central choices we have made and the reasons for making them:
Structured model: For experienced ethicists, a model adds little of value, but for participants learning to structure their thinking about ethical issues, this can be of considerable help. The one we suggest is clear and to the point.
Explicit focus on values and moral principles: This feature of our model stresses that ethics case reflections primarily are about identifying the best alternative action based on the arguments provided and not to negotiate the interests of different stakeholders.
Case-based approach: We believe that a case-based rather than principle-based approach is helpful in the clinical setting, since the principle-based approach may hinder participants from feeling free to bring up aspects that do not clearly fit with the pre-established principles, while case-based models focus on values and moral principles that are found to be relevant in the case at hand.
Inter-professional reflection: The facilitator of the reflections has the role of assisting the process and the dialogue. By leaving most of the reflection time, initiative and much of the analysis to the participants of the health care team, an established practice of clinical ethics case reflections on demand can provide a continuous opportunity for health care staff to improve their skills in ethical analysis on a practical level, while providing support for the structured handling of the individual ethics case.
Exclusion of patients/parents: There are good arguments both for and against including patients/parents in the reflections. Although providing a more reliable way of including the patient/parent perspective in the reflections, there is the risk of over-stressing the patient’s/parents’ preferences in the reflection. In our case it is greater likelihood, for practical reasons, of making the reflections take place if patients/parents are not included.
Footnotes
Acknowledgements
We want to thank the ethics committee at Karolinska University Hospital and the members of the research group ‘Childhood Cancer Health Care Research’ for valuable input and support.
Declaration of conflicting interests
The authors declare that there is no conflict of interest and confirm that the submitted material has not been submitted to or published in any other journal and is not under consideration by any other journal. All the authors have read and approved the manuscript and no one with a claim of authorship has been excluded. The authors take responsibility for the quality of the authorship.
Funding
This work was supported by the Swedish Cancer Foundation, [Grant number CAN 2009/912] and AFA Insurance, [Grant number 120019]. The study has been approved by the regional ethics committee in Stockholm.