
Abstract
Objective
The objective of this article is to provide an ethical analysis of a high-risk, advanced treatment case where the patient received transcatheter aortic valve insertion (TAVI), for aortic valve stenosis. Particular emphasis will be placed upon the significance of evidence and the implications for priority setting.
Method
One paradigmatic case involving a TAVI patient from a large university hospital in Norway is described and analysed. The method used was ethical case analysis modified after Kymlicka by Miljeteig et al. Perioperative mortality risk was estimated using the Euroscore risk-logarithm and the Society of Thoracic Surgeons’ risk model, STS. These predict the risk of operative mortality and morbidity associated with adult cardiac surgery. GRADE, the Grading of Recommendations Assessment, Development and Evaluation, was used to evaluate the evidence.
Results
In the case analysis, we found that it would be ethically justifiable not to recommend TAVI treatment for this patient. Although the patient had a severe condition in need of treatment, the expected improvement was marginal, the quality of evidence was low and the opportunity costs for other patients and society were higher than usually deemed appropriate.
Conclusions
Decision-making in the absence of high quality evidence from randomized trials is a complex process involving difficult ethical judgments. Novel high-risk devices often enter the European market with limited clinical evidence. Transparency and improved clinical evaluation are required so patient safety is not jeopardized. We argue that implementation of high risk, high cost interventions should be better regulated at a national level.
Background
All clinical decisions imply priority setting and therefore indirectly affect other patients and other patient groups. The use of expensive, innovative health technologies has an affect on individual patients as well as on other patient groups competing for the same resources.
Transcatheter aortic valve insertion (TAVI) is a relatively new technique involving the implantation of an artificial aortic valve – a high-risk device – into a narrowed aortic valve without the need to stop the heart. 1 It serves as a treatment alternative for severe aortic stenosis (AS). The quality of the evidence for this treatment has been subject to controversy amongst researchers and physicians. 2
AS is the most common valve disease of the heart and the fourth most common heart disease in Norway. AS has a prevalence of 18% 3 with severe AS in 2% of 75 year olds and 6% of 85 year olds, 4 with an increasing incidence with advancing age. Patients with untreated, severe AS have a poor prognosis, with a 50% mortality rate in 2 years. 1 As life expectancy increases in Norway, we expect an increasing demand for treatment of severe AS. The current treatment options for severe symptomatic AS are surgical aortic valve replacement (SAVR), pharmacological treatment or TAVI.
In 2008, the Norwegian Council for Quality Improvement and Priority Setting in Health Care assessed the evidence of outcomes of TAVI in Norway. 5 They concluded in their report that TAVI should be considered as experimental treatment and should not be offered in Norway other than in clinical trials. Nevertheless the treatment was offered as an established treatment option at several hospitals and funded over the regular budget.
There are several studies analysing the evidence for treating older patients with advanced high-cost and high-risk treatment.1,6 However, we found no studies that considered the ethics of selecting patients for such procedures, given the resource limitation and the scarcity of evidence on outcomes for the very old.
This article aims to explore the process of implementing TAVI in Norway and to uncover, through ethical analysis, the quandaries of decision-making and the implications for priority setting when deciding to implement a high-cost, high-risk treatment.
Method
Ethical case analysis.
Illustrative case report
A 79-year-old woman presented with breathlessness. Her previous medical history included hypertension, mitral insufficiency and pulmonary hypertension. She was a widow living by herself and received no help from the public sector. She had three children and seven grandchildren who gave her great pleasure. She stated that her life had been a good one and that she wished to live longer to see her family grow up.
An echocardiogram showed severe AS, left ventricular hypertrophy, mitral regurgitation and pulmonary hypertension. She was considered inoperable for conventional aortic replacement surgery because of the high risk. She did not have anatomical limitations for surgery.
Perioperative mortality risk (the risk of dying under the operation, or during the first 28 days) can be estimated using the Euroscore risk-logarithm and the Society of Thoracic Surgeons’ risk model, STS.9,10 These predict the risk of operative mortality and morbidity associated with adult cardiac surgery on the basis of patient clinical characteristics:
– Euroscore: Mortality: 21.3% – STS score: – Mortality: 23% – Mortality or morbidity: 76% (A composite endpoint defined as any of the outcomes: mortality, stroke, renal failure, prolonged ventilation, deep sternal wound infection or reoperation).
On the basis of this risk assessment, the patient was not considered eligible for ordinary cardiac valve surgery
Analysis
Statement of the problem and alternative actions
Would it be ethically justifiable not to recommend transcatheter aortic valve insertion to this patient?
What is the evidence concerning the outcomes of the different alternatives?
To date there have been two randomized controlled trials investigating TAVI: the PARTNER trial (cohort A and B) and the STACCATO trial.11–13 The STACCATO trial was stopped early because of an increase in adverse events, including increased risk of major stroke and severe paravalvular leakage in elderly patients eligible for surgery. 12 PARTNER cohort A included high-risk patients randomized to TAVI or surgical treatment. PARTNER cohort B included patients considered inoperable randomized to TAVI or non-surgical treatment.
In 2012, the Norwegian Knowledge Centre for the Health Services updated their initial assessment of the evidence and possible cost of TAVI from 2008. 14 Using the GRADE methodology, they have rated the quality of evidence of the PARTNER studies. In 2011, the Belgian Health Care Knowledge Centre performed a critical analysis of the PARTNER study. They also did a health economic study of TAVI based on the PARTNER results and cost figures from Belgium. 15 They carried out a subgroup analysis of all-cause mortality in medically and anatomically inoperable patients. This analysis showed that the results of TAVI were better in the anatomically inoperable patients, 27.9% vs. 17.0% mortality reduction.
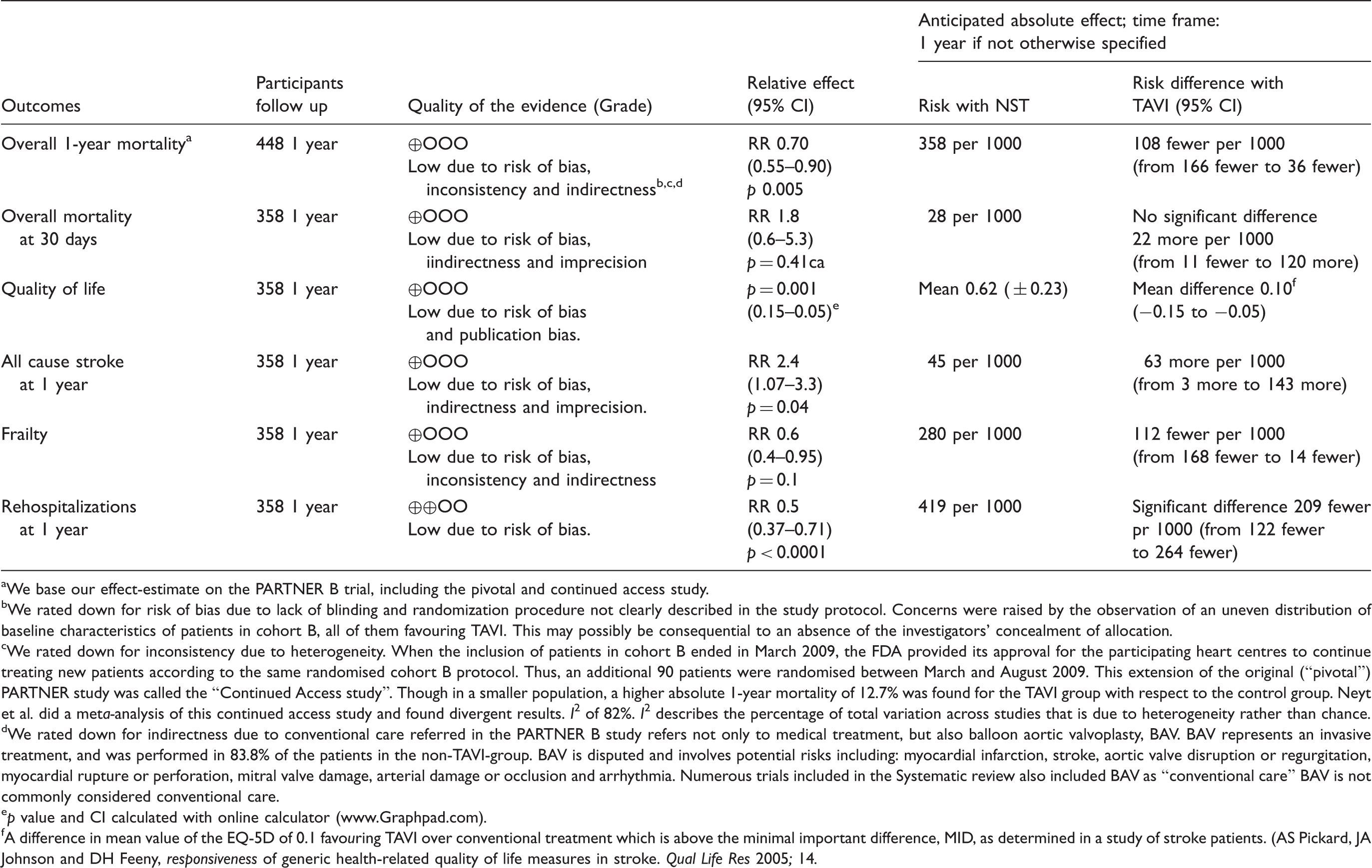
We base our effect-estimate on the PARTNER B trial, including the pivotal and continued access study.
We rated down for risk of bias due to lack of blinding and randomization procedure not clearly described in the study protocol. Concerns were raised by the observation of an uneven distribution of baseline characteristics of patients in cohort B, all of them favouring TAVI. This may possibly be consequential to an absence of the investigators’ concealment of allocation.
We rated down for inconsistency due to heterogeneity. When the inclusion of patients in cohort B ended in March 2009, the FDA provided its approval for the participating heart centres to continue treating new patients according to the same randomised cohort B protocol. Thus, an additional 90 patients were randomised between March and August 2009. This extension of the original (“pivotal”) PARTNER study was called the “Continued Access study”. Though in a smaller population, a higher absolute 1-year mortality of 12.7% was found for the TAVI group with respect to the control group. Neyt et al. did a meta-analysis of this continued access study and found divergent results. I2 of 82%. I2 describes the percentage of total variation across studies that is due to heterogeneity rather than chance.
We rated down for indirectness due to conventional care referred in the PARTNER B study refers not only to medical treatment, but also balloon aortic valvoplasty, BAV. BAV represents an invasive treatment, and was performed in 83.8% of the patients in the non-TAVI-group. BAV is disputed and involves potential risks including: myocardial infarction, stroke, aortic valve disruption or regurgitation, myocardial rupture or perforation, mitral valve damage, arterial damage or occlusion and arrhythmia. Numerous trials included in the Systematic review also included BAV as “conventional care” BAV is not commonly considered conventional care.
p value and CI calculated with online calculator (www.Graphpad.com).
A difference in mean value of the EQ-5D of 0.1 favouring TAVI over conventional treatment which is above the minimal important difference, MID, as determined in a study of stroke patients. (AS Pickard, JA Johnson and DH Feeny, responsiveness of generic health-related quality of life measures in stroke. Qual Life Res 2005; 14.
All three of these analyses rated the quality of evidence as low, mostly because of the risk of bias, inconsistency and indirectness. This reflects low confidence in the effect-estimates for patient-important outcomes. In addition, the PARTNER trial has been criticized for its low methodological quality and unethical conduct of science.2,15,18
Effect and cost-effectiveness of TAVI-based Belgian health technology report.
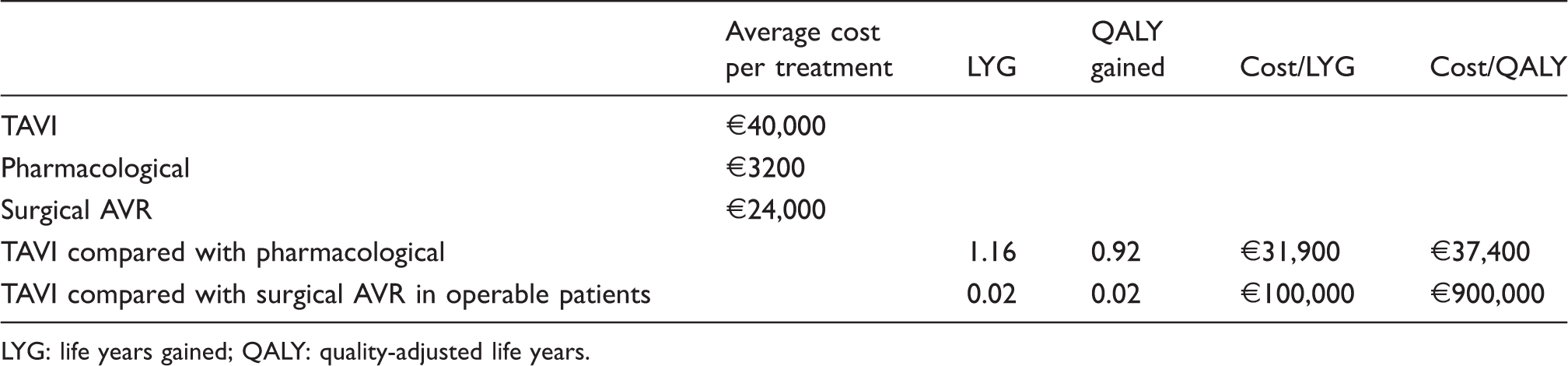
LYG: life years gained; QALY: quality-adjusted life years.
Are there guidelines or legal acts that regulate the issue at hand?
Clinical guidelines
The following American and European guidelines are often applied in Norway.
American guidelines state: TAVI is recommended in patients with a predicted survival of 12 months, and who have a prohibitive surgical risk as defined by an estimated 50% or greater risk of mortality or irreversible morbidity at 30 days.
19
(abbreviated)
European guidelines state Based on current data, TAVI is recommended in patients with severe symptomatic AS who are, according to the ‘heart team’, considered unsuitable for conventional surgery or an individualized decision of high-risk patients who are still candidates for surgery.
1
(abbreviated)
However, neither of these guidelines adhere to established standards for trustworthy guidelines20,21 and are therefore not considered of high enough quality for use in the context of our patient. The guidelines do not provide sufficient evidence to demonstrate that the benefits outweigh the risks, nor is the evidence of a sufficiently high standard to justify the strong recommendations.
Moreover, we know our patient is inoperable for medical reasons, which places her in the subgroup with a poorer outcome. The decision about whether or not a patient is operable can partly rest on objective tests like Euroscore and STS, but will always partly rely on clinical judgments and individual risk assessment.
In the 2012 update of the 2008 assessment of the evidence of outcomes of TAVI treatment in Norway, The Norwegian Knowledge Centre for the Health Services conclude TAVI can provide increased quality of life and survival to selected inoperable patients with severe AS. For operable patients there is no health gain shown with TAVI. There is great uncertainty about which patients have an expected benefit of TAVI and whether the treatment is cost-effective
14
Legal aspects
In Norway, the patient has a right to necessary specialized health care according to the Patients’ Rights Act and national guidelines for priority setting, when,
The patient has a condition with reduced prognosis related to life expectancy or quality of life if health care is delayed, and The patient has an expected benefit from the health care, and There is a reasonable relationship between the costs and the effectiveness of the treatment. There is good evidence concerning outcomes and cost-effectiveness.
The first criterion concerns severity. In the process of developing these criteria there was an agreement that the severity of a condition should be balanced against the benefit criterion and that severity should not be used as an independent criterion.
Concerning the other criteria, the low quality evidence suggests there is an expected benefit of treatment when considering 1-year mortality, re-hospitalizations, need for renal replacement therapy, frailty and quality of life. These benefits come at the cost of a higher 30-day mortality and higher incidence of major stroke (Table 2). The cost per QALY is approximately €37,400.
In summary, applying the national guidelines for priority setting to our case patient shows that she has a condition considered to be severe, but that the benefit is probably small, the cost substantial and the quality of evidence low. Thus treating our patient with TAVI is not in accordance with the Patients’ Rights Act of Norway.
Who are the affected parties?
The next step in the ethical analysis is to identify the affected parties. We identify the following to be the most important: the patient, the next of kin, other patients in the hospital, other patient groups, doctors, nurses, other hospital personnel, the hospital (publicly financed in Norway), society at large and the medical technology industry.
What are the benefits and burdens for the affected parties under the alternative options?
Table 1 shows the benefits and burdens for the treatment alternatives of TAVI versus non-surgical treatment. The trade-off for the patient is the increased chance of survival of 13% after one year if treated with TAVI, weighed against the increased risk of a stroke at one year of 6.1% or the increased risk of 30-day mortality of 2.2%. Some may consider the investigations routinely performed before TAVI treatment a burden. These investigations include cardiac catheterization, echocardiography, trans-oesophagus echocardiography, CT, spirometry and assessment by an oral surgeon. If not treated with TAVI, patients may experience the burden of not being given a chance, and the burden of the knowledge of having a somewhat shorter life expectancy.
Benefits and burdens for other affected parties also need to be considered. Increasing treatment with TAVI at a cardiology department results in other patients’ having to wait longer for their investigations. This affects most patients in the department. For example, it will increase the waiting time for cardiac catheterization and complicate the logistics of the acute revascularization in non-ST elevation myocardial infarction (NSTEMI) patients, a treatment in which the beneficial effect is well documented. 22 Often TAVI patients are admitted to the medical intensive care unit (ICU) after the procedure. This also represents a potential burden for other patient groups. The ability to offer most patients well-documented treatment is considered a societal benefit. Funding poorly documented and possibly futile treatment over the regular budget could reduce access to health services for other patient groups.
Contributing to the development of a promising new treatment option is often meaningful for clinicians. Treating a severely ill patient successfully is in itself rewarding. The skill of implanting valves using catheters will possibly benefit future patients. It can therefore be seen as a benefit for both physicians and patients. However, studies show that clinicians can find it distressing when older patients are prioritized above younger patients who may have a greater potential benefit of treatment. 23
The medical technology industry has substantial economic benefits from selling their devices.
Are substantial interests in conflict?
The conflict of legitimate interests between the individual patient and the healthcare system
The patient has a legitimate interest in a prolonged life with a better quality of life. Our patient wanted to live longer so she could take part in her grandchildren’s lives. If TAVI was withheld contrary to the patient`s wish, this would be a conflict of interest between the patient and the health system.
The conflict of interest between other patients and the individual patient
Treating our patient with TAVI will leave fewer resources for other patients. By prioritising costly treatments for older patients with a low expected outcome, other patient groups with a potentially higher expected benefit would receive less.
The conflict of interest between the medical device industry and patients/clinicians/researchers
Edwards Lifesciences sponsored the PARTNER trial. The co-principal investigator received $6.9 mil from Edwards Lifesciences when it purchased Percutaneous Valve Technologies, the heart valve company he founded. The deal reportedly also included the chance for the co-principal investigator to earn an additional $1.5 million if the product achieved certain milestones, one of which related to the number of patients successfully treated. 24
The interests of patients and the interest of the medical technology industry may be conflicting. Industry’s main goal is high revenue. In recent years, sponsoring companies have become intimately involved in all aspects of research on their products. They often design the studies, perform the analysis, write the papers, and decide whether, when, and in what form to publish the results. 25 When integrity in medical science or practice is impugned or threatened – such as by the influence of industry – patients, clinicians and researchers are all at risk of harm, and public trust in research is jeopardized. 26
The conflict of interest between cardiologists and patients
Cardiologists find it meaningful and important to contribute to the development of new promising treatment alternatives. This can cause a conflict of interest if the treatment is offered as an established treatment modality and the patient is inadequately informed about the expected benefit, risk and the quality of evidence.
The conflict of interest between society and the healthcare system
We believe that citizens of our society are interested in a fair distribution of resources within the healthcare system. Offering a treatment with high cost, high risk and a potentially small benefit for older patients may not be in accordance with what most consider a fair distribution of resources. The decision to offer such treatment also results in reduced resources for non-health societal welfare benefits.
Are fundamental principles in conflict?
The principles of biomedical ethics of Beauchamp and Childress provide a basic analytical framework for reflecting on moral issues within biomedicine. 27 The four principles that form the core of modern bioethical discussion are beneficence, non-maleficence, autonomy and justice.
Where there is a lack of good evidence, it is difficult to analyse whether the fundamental principles of beneficence and non-maleficence are in conflict. One needs to assess the evidence of the relevant outcomes and then weigh the desirable and undesirable effects for the individual patient in question. When making the decision to treat our patient with TAVI it should be a prerequisite that it would be beneficial for the patient. This analysis shows clearly that the basis for such an assumption is uncertain because of the low methodological quality of the PARTNER trial and a possible overestimation of the clinical effect of TAVI.
In a healthcare setting, the principle of autonomy often translates into the principle of informed consent. Patients need to make judgments consistent with their personal values. This presupposes that they understand the potential outcomes and are able to communicate their wishes. When the evidence is of poor quality, informing patients adequately becomes a challenge. We do not know whether our patient was informed about the level of evidence concerning all the relevant outcomes or if she was informed that the treatment was investigational. There is no formal requirement of documenting such information in Norway.
The principle of justice implies a fair distribution of resources. This is a core challenge in priority setting. We can define priority setting as the ranking of interventions with respect to obtaining resources for implementation. 28 When the physicians made the decision to treat our patient they indirectly rank some other interventions lower. A fair distribution of resources depends on the theoretical basis of how one should set priorities fairly. This requires methods for comparing risk and benefits for different patients and patient groups. The assessment of these theories and methods goes beyond the scope of this paper.
Discussion
We claim it would be ethically justifiable not to recommend TAVI for this patient.
The patient has a right to know when there is a low quality of evidence about a treatment and should be informed when treatment is considered to be experimental. An expected average net benefit must be balanced against the substantial risk of mortality and morbidity. The cost of this marginal benefit is high for our patient. On the basis of current evidence, and considering efficient use of limited resources, it appears that these resources could have been spent more wisely elsewhere. There is no adequate mechanism to ensure fair resource allocation between different disciplines in medicine.
In the EU, all that is required to get an approval for a medical device is a simple CE mark.
Dissatisfaction with EU device approval and post-market evaluation systems is increasing and has been debated in recent years.29–32 Contrary to what physicians and users may assume, the pre-market clinical evaluation of high-risk medical devices in Europe is not comparable to the evaluation of pharmaceuticals in terms of safety and efficacy. The uncertainty of effects and adverse effects poses an unreasonable risk for patients. Priority setting aspects of the European approach for high-risk devices have not been widely discussed in the literature.
New health technologies have the potential to improve healthcare and health systems. On the other hand, we have seen examples of new, highly specialized treatments implemented with little or no clinical evidence, and then proving to be ineffective or dangerous. For example, rotational atherectomy for coronary artery disease, 33 or laser therapy for coronary heart disease. 34
We support the conclusion of the Belgian Health Technology Assessment (HTA) 15 that on the basis of current evidence TAVI should be limited to patients who are inoperable for anatomical reasons only and, within this subgroup, only for those patients where the benefits clearly outweigh the burdens. On the basis of data from Belgium, we estimate that the number of patients in need of TAVI in Norway would be 13–15 per year. The actual number of TAVI treatments in Norway in 2012 was approximately 200 patients. 14
The recommendations in the various guidelines seem to lack a transparent link to the underlying evidence base and they do not seem to represent the results of a systematic and critical appraisal of that evidence. Recommendations in both the American and European guidelines are possibly broader than what is supported by the evidence.
We have used only one patient case to illustrate the ethical dilemma patients and doctors face in cases of this type. Although we cannot generalize our conclusion on the basis of this case alone, the evidence base we used to assess this case is representative for many inoperable AS patients in need of valve replacement. The evidence was so weak that we were led to question whether the recommendations for medically inoperable patients, with high risks and old age, were acceptable at all. We have only examined the implementation of TAVI. Nevertheless our reflections are partly applicable to the implementation of other new health technologies. The method used is systematic, impartial and considers the perspective of all stakeholders. We hope the transparency of the method is sufficient to set forth our principal concerns and promote further discussion amongst clinicians and policymakers.
Conclusion
Ethically justifiable decisions about implementing new costly treatments should be based on appropriate procedures and widely agreed principles of evidence-informed priority setting. Ideally the decision procedure should grade the quality of evidence of the relevant outcomes, balance desirable and undesirable effects, and consider whether the intervention represents a wise use of resources. This should be regulated at national and regional levels to safeguard the individual patient, to ensure better and fairer allocation of common resources and to support physicians in individual priority-setting decisions.
Footnotes
Authors’ note
Concerning informed consent: The patient in the article is a paradigmatic case, based on several patients we have seen in our Heart Department. The patient is unidentifiable for any readers or patients. No information concerning the patients is stored. In the process of writing the article, the Data Protection Officer at our hospital was contacted concerning informed consent. The Data Protection officer is the local authority who controls that research is in accordance with the Norwegian Personal Data Act and the Health Data Filling system. Due to the fact that the patient is composed on the basis of several patients, serving as a paradigmatic case, and the fact that the patient is not identifiable in any way, the Data Protection Officer determined that there was no need for an informed consent.
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.