
Abstract
The dominant rule of economic evaluation within health care posits that resources are distributed in order to maximize health benefit. There are instances, however, where the public has demonstrated that they do not prefer such an allocation scheme, particularly in the context of life-saving interventions.
Objectives
Deviations from preferences of maximizing health benefit have important implications on both financial and distributive levels. This study sought to specify the circumstances in which respondent preferences are inconsistent with maximizing health benefit.
Methods
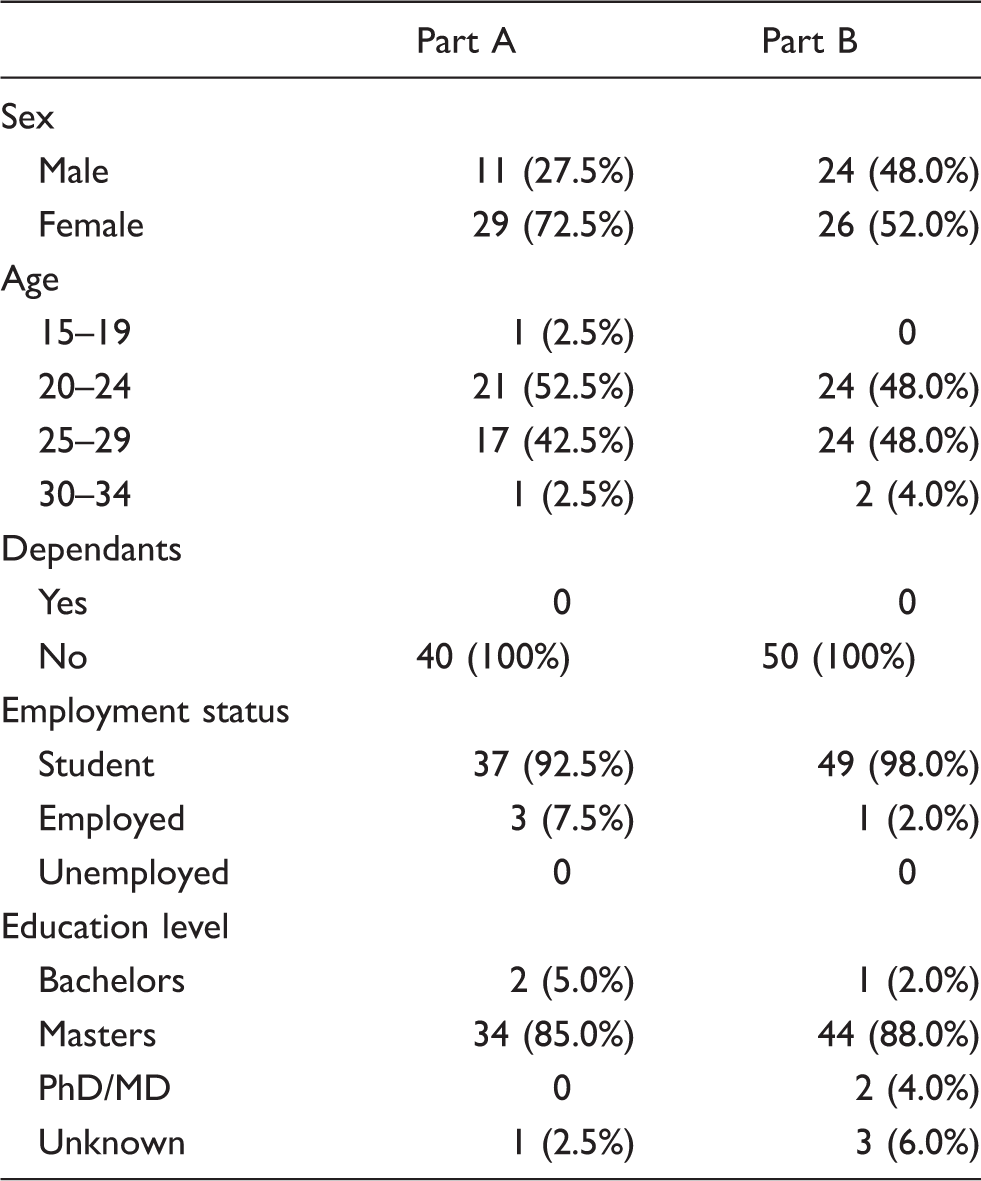
Ninety respondents recruited from the London School of Economics and Political Science completed a questionnaire comprised of a series of paired profiles involving various combinations of life-saving or quality-of-life enhancing interventions.
Results
The results indicate that saving a life holds value beyond that captured by traditional health benefit measurement and that the value of saving a life is not consistent across ages. More specifically, the value of saving a life was age-dependent and markedly attenuated for older-age patients.
Conclusions
Many respondents were willing to overlook maximizing health benefit in order to rescue a life in immediate peril, and showed a diminished sense of moral imperative to rescue older-age patients. In light of difficulties related to the implementation of larger-scale policies incorporating Rule of Rescue concerns, the most realistic approaches will likely involve adopting smaller-scale policies that address issues such as do not resuscitate (DNRs) and living wills. Potential policy solutions such as age or monetary thresholds for life-saving interventions may be favoured in a research context; however, their overall social feasibility is questionable.
Keywords
In healthcare, as in virtually every public sector, resources are limited and must therefore be rationed. It is a matter of fact that there are insufficient resources (specifically, funds available) to provide optimal treatment to every individual. 1 If demand for healthcare exceeds the supply of resources (namely, the funds available), then methods by which available resources are distributed must be determined. This involves prioritizing what programs or interventions are funded and who (which patients) are eligible beneficiaries. 2
Currently, several health systems use the quality-adjusted life-year (QALY) in economic evaluations whereby efficiency is attained by reaching ‘greatest health gain per amount spent.’ The QALY is a composite measure of health benefit, incorporating both quantity (life-years gained) and quality (health-related quality-of-life) from treatment, enabling comparisons of health care programs with different types of outcomes from various domains within health care.3,4 When paired with the cost of the intervention, the resulting cost per QALY ratio can provide guidance on the economic efficiency of respective interventions. Within the discipline of health economics it is generally understood that given a restricted budget, it is best to strive to maximize overall health gains, the reasoning underlying QALY maximization strategies (i.e. the greatest health gain – number of QALYs – at the lowest cost).
The absence of concerns of equity in the current ‘efficiency-focused’ QALY methodology has provoked widespread philosophical debate as to how resources may best be distributed. Although some argue that allocating an equal weight to QALYs regardless of individual characteristics of the recipient achieves a form of equity through ‘distributive neutrality’, 5 alternative arguments to QALY maximization have been presented that more actively address equity concerns alongside those of efficiency.
Alan Williams’ ‘fair innings’ argument, for example, holds that each individual is allocated some ‘normal span of health’ (usually denoted as three score and 10 years) with those who exceed this expectation ‘living on borrowed time’ (119) and those who fail to do so having been ‘cheated.’ 6 Williams 7 extended his argument by proposing that equity weights could be assigned to compensate for socioeconomic status and disability whereas Johannesson 8 thought fair innings should be defined in a manner that would be specific to an age/sex subgroup. Another prominent argument, by Harris, 9 proposes that each individual should have an equal claim on available resources. Harris argues that each life should be valued equally and that considerations of prognosis or ability to benefit from treatment are irrelevant, that it is ‘lives that are valuable and not life-years.’9,10 Alternatively, methods of resource allocation may also align with measures of societal importance (often considered in terms of productivity, reflective of disability adjusted life-year, DALY, age-weights), allocating more importance to a year of life lived by a young or middle-aged adult than to that of a child or an elderly person. 11
‘The Rule of Rescue Paradigm’
Of particular concern, and the primary focus of this study, is the QALY's inability to distinguish between quality-of-life improving treatments and those that are life-saving.
In what could be considered the scheme most contrasting with QALY maximization, the ‘Rule of Rescue’ (so termed by Jonsen 12 ) stipulates that individuals whose lives are in immediate peril should have priority over all other needs. The rule starkly violates QALY maximization, in that the opportunity cost of options foregone is either not considered or, alternatively, life-saving is considered to offer value beyond that captured by current measures of health benefit. 13 Jonsen 12 articulates the essence of the Rule of Rescue in describing, ‘… we reach a conclusion contrary to the utilitarian principle: We benefit a few at cost to many’ (174).
Within the health care context, the Rule of Rescue involves providing life-saving treatments or procedures even when it means denying these resources to others (e.g. those who would benefit from quality-of-life improvements). It is relevant, for example, to the provision of extremely costly, life-saving drugs to patients suffering from rare ‘orphan’ conditions. Given recent advancements in health technology and interventions, particularly those that are targeted at life-extension, the merit of Rule of Rescue is likely to become increasingly debated.
The reasoning behind the imperative that individuals feel to rescue those at immediate risk of dying has been discussed largely within philosophical boundaries. Many academics and philosophers13–15 reference deontological arguments overriding those of utilitarian or quasi-utilitarian nature that are often reflected in existing policy (i.e. QALY maximization) and the focus of decision-makers seeking to get the best ‘value for money.’ 16
The current study
Much of the literature discusses the Rule of Rescue in reference to highly publicized cases where it is argued that exceptionality of occurrence and victim identifiability play significant roles in why such cases are allocated scarce resources. In this study, however, the Rule of Rescue is defined as the more general imperative to save lives in immediate peril.
While a range of studies17,18 have investigated public preferences when respondents must allocate life-saving treatment to one of two individuals (what could be viewed as a modified ‘test’ of the Rule of Rescue) or choose between improving the quality-of-life of one patient over another, the literature exploring preferences for the Rule of Rescue as defined in this study is limited (i.e. whether respondents are willing to prioritize life-saving over quality-of-life improvements). Further, few studies have examined the trade-offs involved in the Rule of Rescue at a ‘micro-level’19,20 as the majority of the research comparing life-saving versus quality-of-life enhancing interventions applies a ‘person trade-off’ technique.21–23 Micro-level decisions may elicit different thought processes (e.g. considerations of equity and access) than decisions between groups of patients. 20
The purpose of this study was to build on existing findings related to the Rule of Rescue, and investigate whether or not preferences for life-saving over quality-of-life enhancing interventions apply consistently across all age groups.
Given public preferences for allocating life-saving resources to the relatively younger patients present in the current literature,24,25 it is possible that life-years have different ‘value’ at different ages. As a result, in the current study it is hypothesized that preferences for the Rule of Rescue may be less apparent at older ages than middle and younger ages.
Methods
Overall study design
Questionnaires were completed during a face-to-face interview with the author. A between-subjects design was selected to allow the Rule of Rescue to be assessed in isolated age-groups (Part A) prior to evaluating it in varying age-groups (Part B). Although already established in the literature (that is, that life-saving holds inherent value beyond health benefit), Part A allowed for observation as to whether preferences varied depending on the age of the individual to whom the intervention was to be allocated. Furthermore, it was thought that rather than respondents answering a large number of questions in regard to both intra- and inter-generational trade-offs, a between-subjects design with a limited number of questions would minimize participant fatigue.
In both Part A and Part B, respondents were presented with pairs of health profiles, each profile explained to be representative of ‘lifetime health patterns’ of a typical patient of the population (disease/condition-specific) they represent. Respondents were asked to assume that they are the health policy-maker and that there are sufficient available health care resources to treat only one patient in each pair. The profiles were described in words, and then depicted diagrammatically side-by-side. Respondents were asked to select only one of the two patients to allocate a health intervention (and were also given the option to indicate indifference). In order to gain further insight into preferences, qualitative reasons behind their decisions were elicited by asking respondents to explain their choices for each pair.
Respondents' reasons for their preferences were coded according to an a priori coding template that included: QALY maximization, life-year maximization, quality-of-life maximization, life-year equalization, the fair innings argument, the Rule of Rescue, equal access, productivity, suffer minimization, cost minimization or no reason/unclear. Only one reason, which was determined to be the main reason for the respondents’ choice, was coded. Answers were coded as ‘Unclear/No Response’ when they had not indicated any reasons.
Prior to beginning the main questions, respondents were asked to complete a practice question and to verbally confirm whether they understood the task. Figure 1 shows the practice question presented in Part A – the main questions follow the same structure. In order to minimize interviewer bias, respondents were then required to answer the main questions without asking any further questions. For both Part A and Part B, the sequence of questions was randomized using a random number table, and participants were able to review and change previous answers while completing the task. Three filler questions (in Part A and Part B, respectively) were included in the study in an attempt to minimize the respondents' recall of their answers to the main questions. The filler questions were also framed as prioritizations in order to draw the respondents' attention away from the fact that the focus was on inter- or intragenerational prioritizations.
An intragenerational priority-setting question.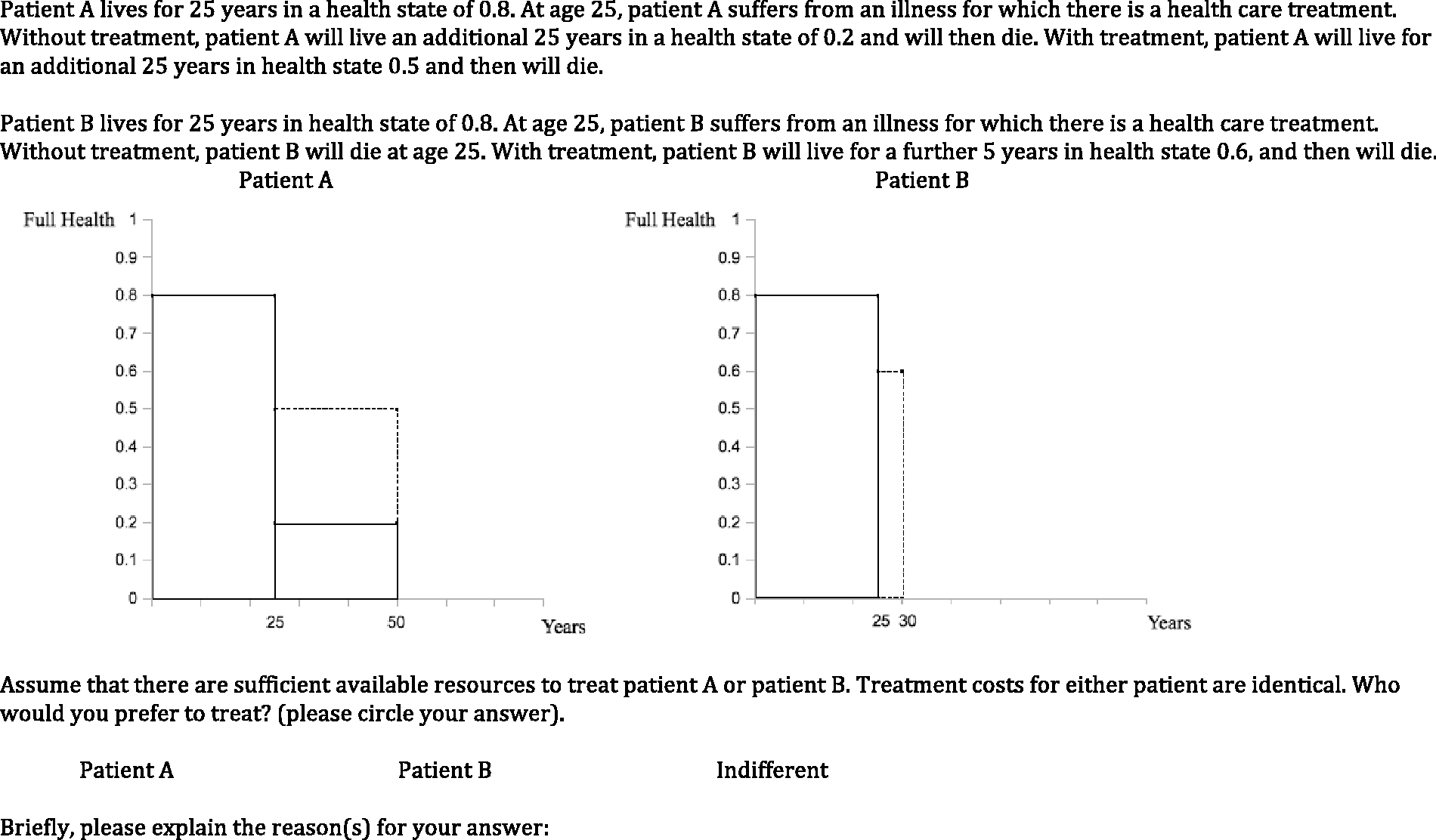
Profile construction
Profiles for both Part A and Part B were constructed such that in each question respondents would be choosing between allocating resources to a quality-of-life enhancing intervention (generating more QALYs) or to a life-saving intervention, yielding fewer QALYs. Profiles were constructed such that the x-axis extended to 80 years (the average combined male/female life expectancy as stipulated by the Office for National Statistics, 26 79.6 (80) years). Characteristics of the health states and the health condition itself were not specified.
The same initial health state values were given for the two profiles being compared. This meant that some lines of reasoning, such as Williams’ fair innings argument, could be of less significance, as respondents would be more concerned with factors such as post-treatment health and/or patient age. Also respondents would not be influenced by Harris’ ‘double-jeopardy’ argument, specifically that those who have already experienced a misfortune should not receive less priority in the receipt of future interventions despite their capacity to yield fewer QALYs according to efficiency calculus. Respondent recognition of the potential to adapt to a lower health state might also have influenced responses were initial health states to differ. Thus the same initial health states were chosen in order to confine respondent's potential considerations as well as to align with QALY maximization focus of post-treatment quality and length of life.
The samples
Respondent characteristics.
Part A: The quality-of-life/ life-saving trade-off (within age-groups)
Part A was conducted with the purpose of confirming existing results that life-saving has value beyond that of health benefit. Consequently, when presented with two patients of the same age, one requiring a life-saving intervention and another who would benefit in terms of quality-of-life, respondents would have a tendency to select the patient requiring life-saving when selecting for reasons related to the Rule of Rescue.
Part A: Summary of priority-setting questions and potential QALY gains.
Results – Part A
Quantitative results
Part A response frequencies.
Qualitative results
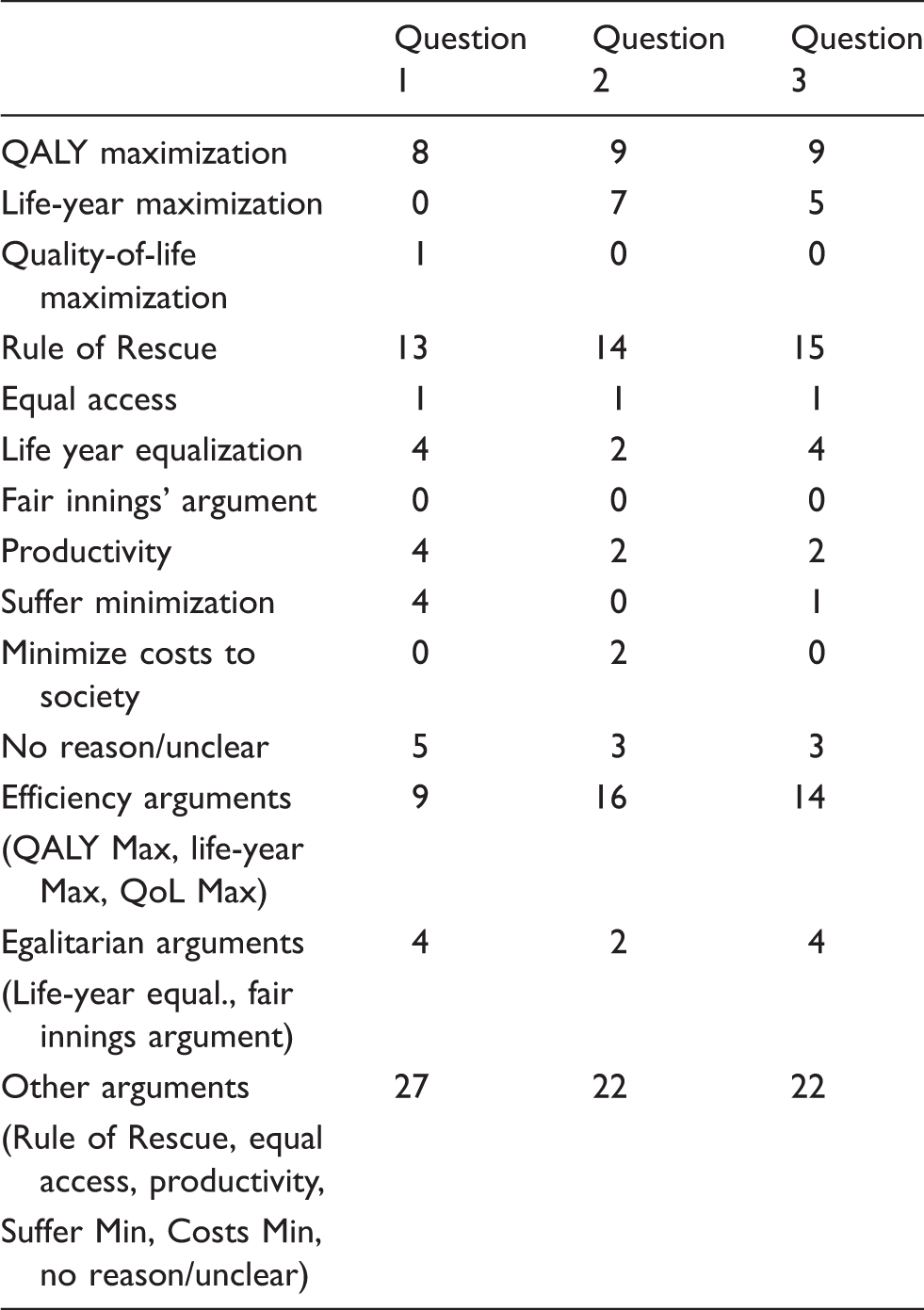
Part A: Qualitative responses for the priority-setting questions.
Part B: The quality-of-life/ life-saving trade-off (between age-groups)
Fifty respondents were presented with nine sets of paired health profiles comprised of six main questions and three ‘filler’ questions. In contrast to Part A, in Part B respondents were asked to prioritize between patients at different stages in the life-course (i.e. of different ages). Respondents were given paired health profiles and asked whether they preferred to increase quality-of-life or allocate resources to a life-saving intervention where the profiles depicted one individual at either ‘young age’, ‘middle age’ and ‘old age’ and another individual of a different age group. Patient A (greater QALY gain) was older than Patient B (life-saving) in Questions 1, 5 and 6 and younger than Patient B in Question 2, 3 and 4.
Results – Part B
Quantitative results
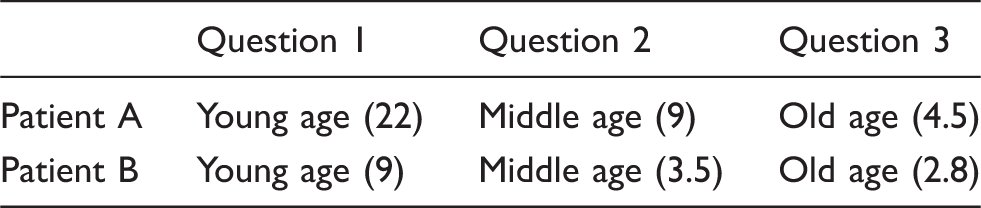
Part B: Summary of priority-setting questions and potential QALY gains.

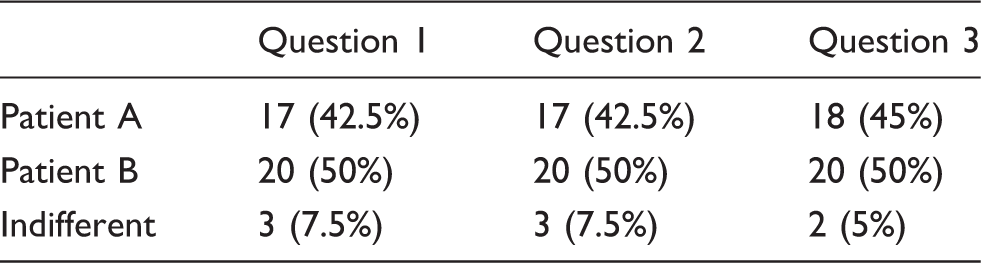
Part B response frequencies.

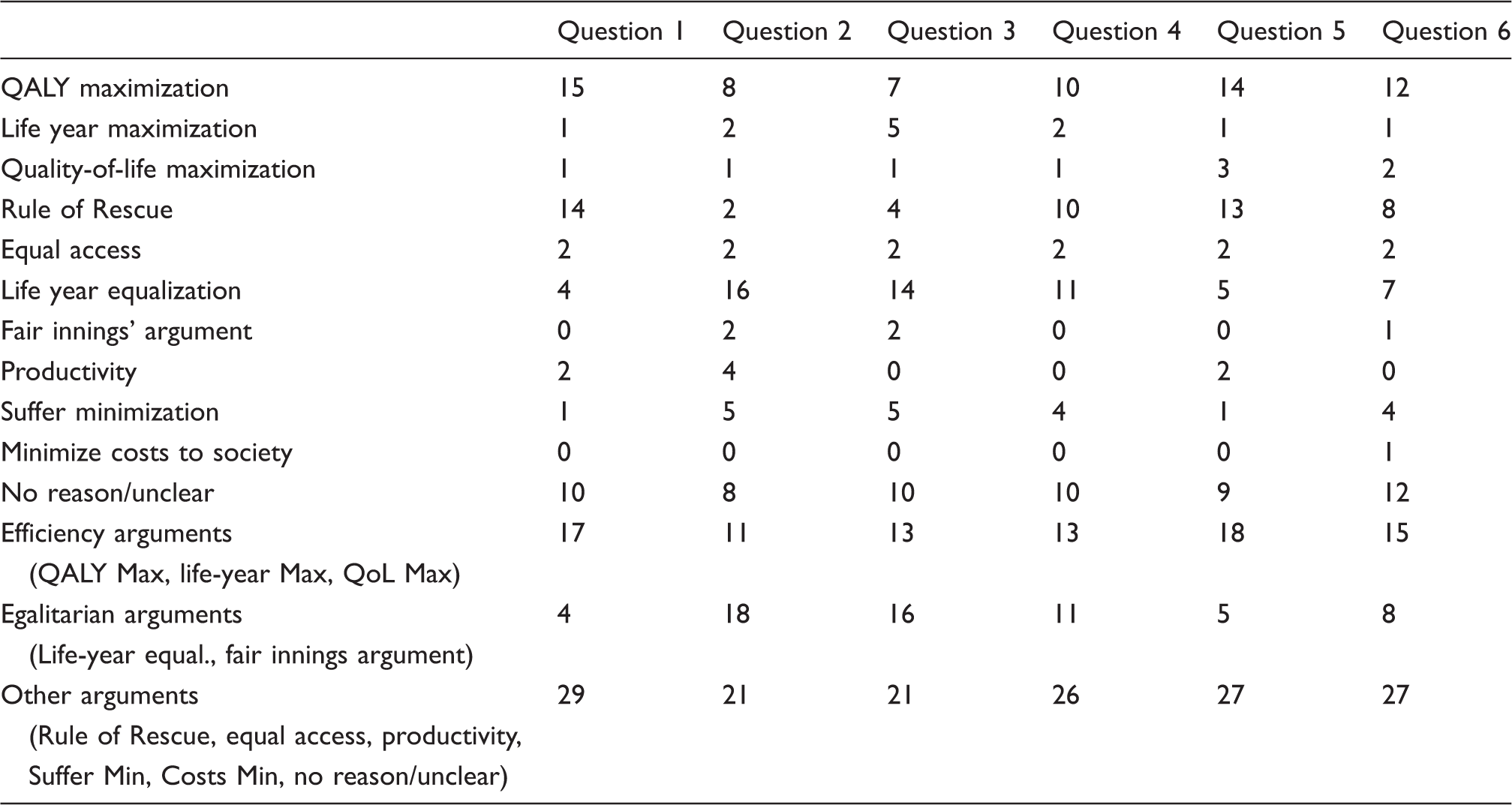
Part B: Qualitative responses for the priority-setting questions.
As in Part A, for a stronger test of the Rule of Rescue, Patient A profiles were constructed such that more post-treatment QALYs would be generated should they be allocated treatment. Profiles in Questions 1, 5 and 6 were designed with the largest QALY differentials between patients and Questions 2, 3 and 4 with smaller differences. It is therefore striking that Questions 1, 5 and 6 elicited the most equal allocation between patients.
Questions 2 and 3 show a strong bias against life-saving in old age in favour of improving quality-of-life in middle-age (Question 2) and younger age (Question 3). Although the QALY differential is not significant in either of these profile sets (1.5 QALYs in Question 2 and 3 QALYs in Question 3), both quality-of-life enhancing profiles extend for several decades (notably the 30's in Question 2 and 20's and 30's in Question 3), which are considered by most to be the years of one's life which are highly valued for reasons of productivity and self-realization. This may help explain the clear preference for allocation in favour of Patient A. Further, it may be that the older age of Patient B in Questions 2 and 3 is a factor in respondents' choices, although analysis of the qualitative responses is needed to support this hypothesis.
Question 4 demonstrates a slightly weaker preference pattern than do Questions 2 and 3. Reasons of productivity for the middle-aged patient and of suffering for the young-age patient may have influenced respondent choices; again, qualitative analysis is needed to support this conjecture.
Qualitative results
Slightly more respondents selected on the basis of QALY maximization (Patient A) than the Rule of Rescue (Patient B) in questions 1, 5 and 6. Both quantitative and qualitative data from Questions 1, 5 and 6 and Part A appear to reflect an influence of the significant QALY differentials between the two patients. In these trade-offs it seems that the imperative to ‘save life’ was not deemed strong enough by some respondents given the large health benefit Patient A would receive.
In Questions 2, 3 and 4 there was an over-arching preference for life-year equalization to support respondents' selections (although 1 fewer respondents selected the Rule of Rescue than life-year equalization in Question 4). QALY maximization (and in Question 4, the Rule of Rescue) was the second most common reason.
Across all six questions in Part B, roughly one-fifth of the respondents gave no reason for their choice or their reason was deemed too unclear to categorize. Only two respondents explicitly stated reasons of equal access to resources regardless of possible benefit, in line with argument proposed by Harris. 9
General commentary
Upon completing the questionnaires, many respondents expressed that they had found it quite difficult to select between the patient profiles. Some level of difficulty is apparent in Part B where approximately one-fifth of respondents were unable to provide clear reasoning (or any reasoning at all) for their choices.
The results of the current study appear to support findings of other studies20,27,28 that have suggested respondents may adopt a variety of decision rules depending on the priority-setting context (i.e. which patients and which of their characteristics are being considered).
In priority-setting between patients of the same age, no clear preference for life-saving over improving quality-of-life was observed. However, despite the large differences in post-treatment QALYs in each profile pair, almost half of the respondents remained influenced by the imperative to ‘save life’ consistent with the Rule of Rescue. Preferences for life-saving according to the Rule of Rescue may have been even greater had the QALY differentials favoured the quality-of-life enhancing intervention less.
The Rule of Rescue was more prominently observed when comparing across patients of different ages. In contrast to results of a recent study by Shah et al. 29 who found age was not a factor in providing life-extending, end of life care, the imperative to save a life in immediate peril was largely absent in this study when the patient requiring the life-saving intervention was in ‘old age.’ The findings of the current study substantiate those of Brazier et al., 30 for example, who found that priority was often not allocated to individuals who were nearing the ‘natural end of their life’. The main reasons for the respondents opting not to select the older patient were based on arguments of life-year equalization and QALY maximization. Further, when respondents did select the older-age person as the beneficiary, it was primarily due to reasons against the younger or middle-aged person, as opposed to wanting to specifically save the life of the older-age person. As such, concerns for minimizing the suffering of Patient A and inability of Patient B to be productive were more frequently cited than Rule of Rescue-related reasons.
Understanding preferences for priority-setting was most challenging when a patient in middle-age could benefit in terms of quality-of-life and a younger patient's life was in peril. It is possible that there was an appeal to the participants to select Patient B since the age range of benefit captured that of virtually all respondents, however, greater clarification is required.
Note on profile construction and limitations
It is difficult, given the limitations of the current study to determine whether or not respondents have a defined preference for treatment of those in middle age over younger age (potentially in accordance with DALY/productivity perspectives) or younger age over middle age (consistent with the fair innings argument and/or life-year equalization).
A further difficulty lies within QALY methodology in that individuals with shorter life expectancies (e.g. older-age individuals) are unable to generate as many QALYs as those with longer life expectancies, ceteris paribus. When constructing profile sets in which Patient B was an older-age individual, it was difficult to allocate enough post-treatment QALYs to their profiles so as not to make the likelihood of selection of Patient A on the basis of health benefit glaring. In an attempt to compensate, in all six priority-setting questions, relatively low health states (all 0.2 except for Question 4 which was 0.3) were set for Patient A should they not receive treatment. This may have, however, encouraged some respondents to have an overriding concern for minimizing suffering of the younger individual.
Had Patient A and Patient B profile sets been constructed such that allocating resources to either one generated a more comparable number of post-treatment QALYs, it would be expected that respondents who had selected patient A on the basis of QALY maximization may have been persuaded by the emotional appeal of the Rule of Rescue imperative and that more respondents would have chosen to save Patient B's life.
Two other issues should be noted. First, since the characteristics of the health states were not specified in the health profiles, variation in how respondents interpreted the numerical values provided (i.e. the health state value ranging from 0 to 1) may have influenced prioritization decisions. Second, the respondent sample was a relatively homogenous group of young academics. This may affect the generalizability of the results. Winkelhage and Diederich, 31 however, note that studies on the influence of age and other respondent characteristics in empirical studies of health care prioritization have been inconclusive. Future research may seek to more clearly understand how respondent characteristics affect specific types of inter- and intragenerational prioritization preferences such as those elicited in this study.
Potential policy solutions to incorporating Rule of Rescue preferences
The preferences yielded in the current study support the findings of other studies that have shown that the public often does not choose to maximize health benefit when asked to prioritize between two patients, one of whom requires a life-saving intervention. Of particular importance in this study are the results that suggest the life-saving imperative posited by the Rule of Rescue becomes weaker as the person facing immediate peril gets older.
There are numerous potential ways by which such preferences could be translated into a policy context. Given the multiple principles cited by respondents in the current study and similar context-dependent results witnessed elsewhere, perhaps the best solution would be to adopt a sort of multi-principle system, incorporating various decision rules. One possibility would be to incorporate both the fair innings argument and Rule of Rescue, such that life-saving interventions are restricted to those younger than a certain age. Alternatively, a monetary limit as to how much is spent on interventions after a patient reaches a certain age could be imposed. Another possible direction, similar to the ‘complete lives system’ that combines maximizing principles with other principles such as those that are needs-based. 32 Callahan 33 has suggested strict age cut-offs for scarce life-saving interventions, whereas Williams has suggested a system that allocates interventions based on individuals’ distance from a normal lifespan if left unaided (i.e. the fair innings argument).
Given the weaker imperative to save an older-age patient in the current study, potential policy solutions such as setting age or monetary thresholds for life-saving interventions could be proposed; however, their overall social feasibility is questionable. Currently, the most realistic solutions will likely involve adopting smaller-scale policies that address issues such as do not resuscitate (DNRs) and living wills. A decline in health service use has been witnessed as a result of promotion of their use, illustrating potential opportunities to free up existing resources for other purposes. Education and encouragement of physicians and family (for those who are unable to complete such directives themselves) is critical.
Establishing a procedural framework to guide clinicians in ‘rescue’ type situations should also be clearly specified to aid in difficult ‘bedside’ decisions that have to be made and to attenuate differences in implicit rationing by physicians. 34 Rulli and Millum 35 comment ‘the most difficult ethical dilemmas arise in non-ideal circumstances in which the potential rescuer faces substantial costs, but where her professional role does not provide clear guidance about incurring such costs.’ Orr and Wolff 36 suggest that a set of available resources for ‘rescues’ is determined a priori and that the clinician or organization should operate without exception within the boundaries of these resources.
Incorporating the Rule of Rescue into resource allocation: Existing policies
As such, at a policy level, a degree of vagueness remains both in terms of how the Rule of Rescue should be operationalized and once criteria have been established when they should be referred to. The National Institute for Health and Care Excellence (NICE) in the UK and the Australian Pharmaceutical Benefits Advisory Committee (PBAC) are two leading organizations that have undertaken to qualify and to set out policy directives aligned with the Rule of Rescue. Both organizations have operationalized the Rule of Rescue primarily in reference to situations of exceptionality, specifically to small groups of individuals (frequently suffering from rare, or ‘orphan’ conditions). 37
In 2006, NICE's Citizens Council (a representative sample of the public from England and Wales assembled to provide advice on social value judgments) deliberated on whether there is ‘a preference to save the life of people in imminent danger of dying instead of improving the life of other people whose lives are not in immediate danger’, or, alternatively, to save ‘the lives of many people in the future through disease prevention programmes.’ 38 The majority view was that NICE should take into account the Rule of Rescue, but only in ‘special circumstances’ determined based on criteria contained in a checklist of 11 items. The translation of the checklist into practical applications remains somewhat unclear.
More recently, NICE 39 set out advice on costly life-extending end-of-life treatments that proposed additional weight be allocated to QALYs if the intervention is: intended for treating a small patient population (i.e. less than 7000 new patients per year), these patients are not expected to live for more than two years and the intervention offers a reasonable increase in length of life (approximately 3 months) compared to current treatment. This guidance may be seen as a means of representing Rule of Rescue considerations through policy in an indirect manner.
The PBAC conceptualized the Rule of Rescue in a slightly different manner than NICE, focusing on orphan drug provision. The PBAC considers three conditions for its application: no available alternative treatment, severity of illness (severe and progressive conditions leading to premature death) and restriction of applicability to ‘orphan conditions.’ 15 The three criteria remain somewhat ambiguous in terms of their application.
In contrast, German constitutional right requires that statutory health insurance pays for non-standard medical interventions for patients with otherwise untreatable life-threatening conditions only if there is some evidence of ‘a not totally distant chance of healing or else a noticeably positive effect on the course of disease’ (BVerfGE 40 as in Schoene-Seifert 37 ). Essentially, there appear to be virtually non-existent limits to the provision of potentially life-saving treatment (the German Constitutional Court decision does not reference cost ceilings or a required threshold of evidence).
Conclusions
The current study offers unique insight into how age influences choice between two interventions varying in nature, an area which has largely been unexplored to date. It was observed that many respondents are willing to overlook ‘efficient’ distribution (QALY maximization) in order to rescue a life in immediate peril. In addition, the results indicate a diminished sense of moral imperative to rescue exists for older-age patients, with potentially important policy implications.
Numerous challenges, however, must be addressed in order for the Rule of Rescue to be effectively incorporated into a resource allocation strategy. Of the utmost important is specifically defining the Rule of Rescue within the particular policy context. Additional barriers such as validating existing health state elicitation models (essential in confirming individuals’ preferences are ‘true’) must also be resolved. Finally, upholding procedural justice – that is, criteria of transparent, fair, contestable decisions and decisions processes – will be imperative regardless of which allocation strategy is in place.
Footnotes
Funding
This research received no special grant from any funding agency in the public, commercial, or not-for-profit sectors.