
Abstract
This article explores how the type of consent given for organ donation should affect the judgement of a patient's overall benefit with regards to donation of their organs and the pre-mortem interventions required to facilitate this. The findings of a qualitative study of the views of 10 healthcare professionals, combined with a philosophical analysis inform the conclusion that how consent to organ donation is given is a reliable indicator only of the strength of evidence about views on donation and subsequent willingness to undergo pre-mortem interventions. It is not an indicator of the strength of actual desire to donate. Clinical management of living patients prior to donation after circulatory death must therefore respect the values, wishes and beliefs of the potential donation after circulatory death donor. Our participants, however, suggested that the information currently provided is sufficient to authorise donation and that this consent, however provided, was sufficient to proceed with pre-mortem interventions. Respect for autonomy underpinned this ‘all or nothing’ approach. Although the legal requirements for donation authorisation and the protection of patients without capacity are clear, practice and policy regarding consent in donation after circulatory death may be based on donation following brainstem death where the patient is already dead when the family is approached. Custom and practice in donation after circulatory death may need to be revised to protect the interests of the dying potential donor.
Background
Donation after circulatory death (DCD) in the UK has increased from 61 cases in 2002–2003 to 507 in 2012–2013. 1 DCD may be less familiar to the lay public than donation after brainstem death (DBD), and raises ethical and technical issues that may not be foreseen by potential donors. In controlled DCD, the possibility of organ donation should be considered only after the decision that continuing life-sustaining interventions is no longer in the patient's best interests. 2 Maximising the chances of successful DCD donation and transplantation can, however, require invasive pre-mortem interventions, such as blood tests, bronchoscopies and insertion of a central line. 3 These can seem incompatible with the prior decision to limit intervention; an apparent ‘moral mismatch’. 4
The interests of unconscious patients in England, Wales and Northern Ireland are protected by the Mental Capacity Act, 2005 (MCA). 5 Such interests are determined with reference to known wishes and any beliefs, feelings or values that relate to the decision in question. Relevant Scottish legislation 6 considers whether treatment ‘benefits’ a patients, determined with reference to present and past known wishes. In line with existing GMC and UK Donation Ethics Committee (UKDEC) guidance,7,8 we will use the term ‘overall benefit’ to refer to the treatment that is most appropriate to a patient without capacity, so that our discussion is applicable to legislation throughout the UK. When patients who are unconscious with no hope of recovery have previously indicated a wish to donate their organs after death, it may serve their overall benefit to become an organ donor. UKDEC state that where donation is ‘consistent with the patient's wishes, values and beliefs, consideration of donation should become an integral part of that patient's care in their last days and hours’ 9 provided that it does not undermine other interests such as avoiding burdensome invasive medical procedures, having a particular sort of death, and avoiding unwelcome burdens and harms for their loved ones. Healthcare professionals (HCPs) have, therefore, to determine (1) whether DCD is a realistic possibility, which is a clinical judgement and will not be discussed further here, (2) whether consent to donation has or can be secured and then (3) whether the pre-mortem interventions required for maximising the chances of successful donation and transplantation are consistent with providing overall benefit to the patient.
In relation to (2), registration on the organ donor register (ODR) (where people can express their willingness to donate their organs) gives some indication of a patient's prior wishes in relation to donation. Indeed, registration amounts to an authorisation to remove organs for the purposes of donation under the Human Tissue Act. 10 In the case of absent registration, family and friends can authorise donation, but the Act places no obligation on them to make a decision (either for or against donation) that reflects the wishes of the patient, save where the patient is known to have objected. Discussion of whether or not this amounts to a coherent position, including revisiting well-trodden arguments in favour of opt-out or even mandatory systems,11–13 is beyond the scope of this article. Wales has recently transitioned to an opt out system (and other devolved Governments may follow), but the current law throughout the rest of the UK is that organ donation should only go ahead if there is no indication that the potential donor would have objected to this and appropriate authorisation has been secured. 10
In relation to (3) the Organ Donation Taskforce argued that registration per se does not meet the standard of informed consent usually required in medicine and may not, therefore, justify the necessary pre-mortem interventions required for effective transplantation. 14 The patient, whilst clearly expressing a wish to be a donor, might not have anticipated what donation entails and therefore in lieu of evidence to the contrary, it cannot necessarily be assumed that willingness to donate equates to a consent to everything that will make donation possible before death has occurred. Additional information about the strength of the desire to donate can be gained from family and friends. It may be reasonable to assume, absent evidence to the contrary, that the stronger the desire the more likely it is that interventions that make donation possible would have been acceptable to the patient. 15 Evidence of prior knowledge of what donation might entail could also be helpful. Where there is no direct knowledge of the patient's wishes, a judgement about overall benefit will need to be made in conjunction with family and friends, who can provide knowledge of whether the potential burdens of pre-mortem interventions can be justified in the light of the patient's values, feelings and beliefs. The UK Code of Practice 16 suggests that interventions should only be performed for the benefit of the patient and not solely to preserve organs. Accordingly, clinicians have to be confident that donation is of overall benefit to the patient to the extent that interventions prior to death are beneficial to the patient in terms of bringing about this benefit. 17
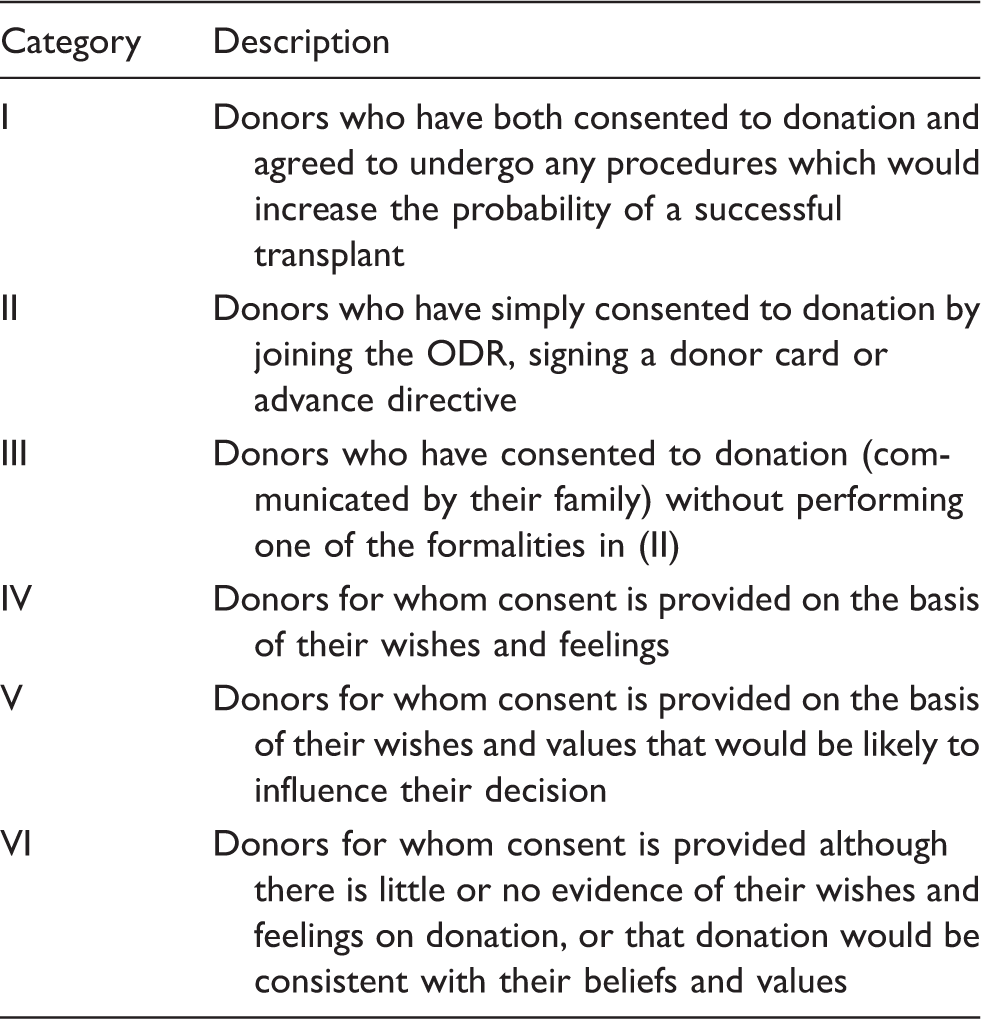
Hierarchy of consent in organ donation (UKDEC, p. 17).
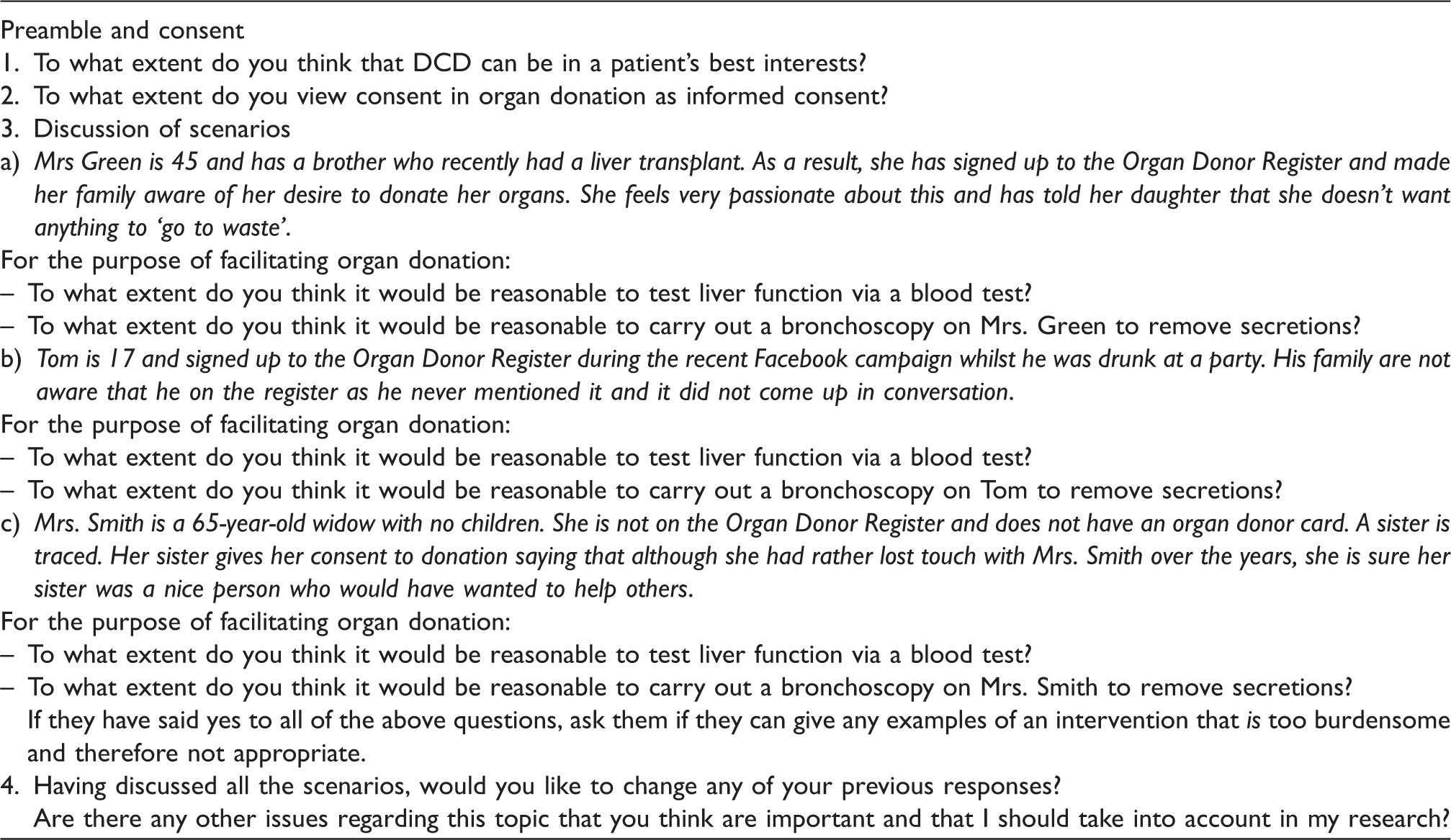
Topic guide.
Methods
As this is an area in which there is no existing literature, making it likely that new ideas and theories would emerge, face-to-face interviews were undertaken to allow for in-depth descriptions of complex phenomena. 20 The interviews were semi-structured to provide consistency, whilst also allowing participants to raise relevant issues important to them. The topic guide (Table 2) provided uniformity, structure and anticipated general key issues identified by a pilot interview conducted prior to the 10 interviews through which data were collected.
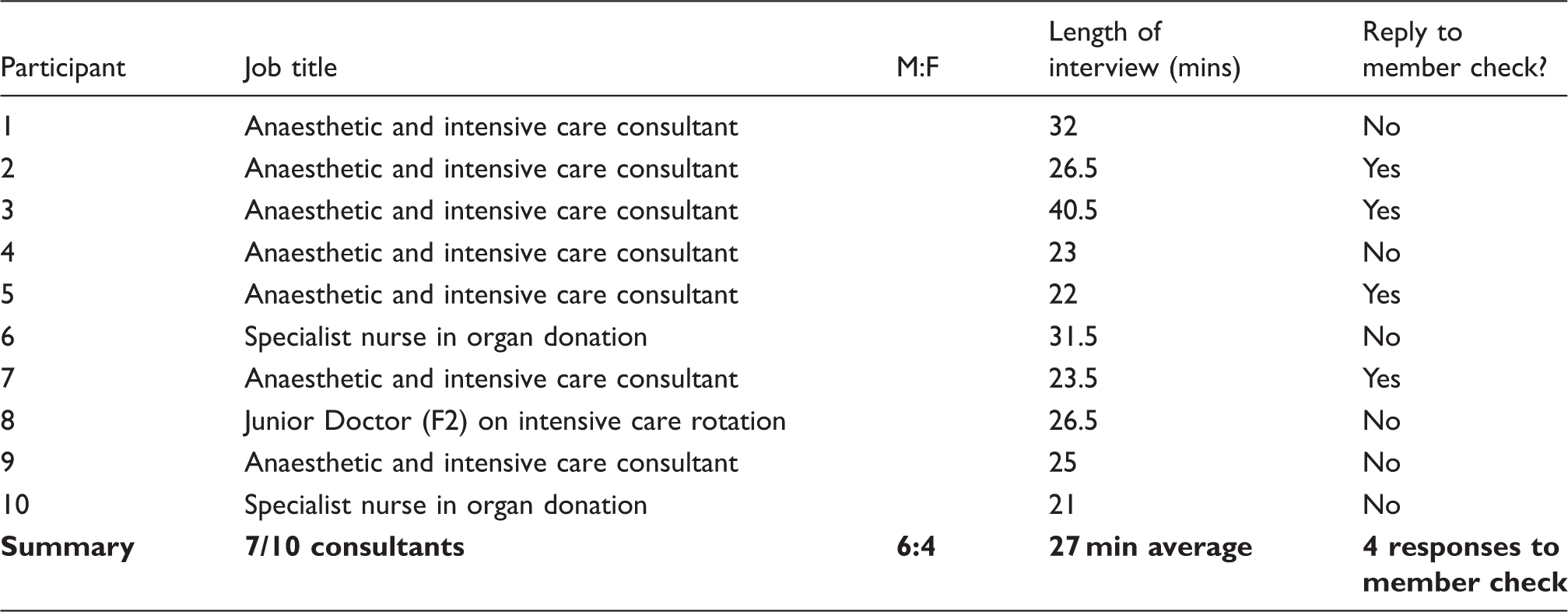
Participant characteristics and interviews.
Permission for the study was gained from the Trust R&D following favourable review by the BMedSc Population Sciences and Humanities Internal Ethics Review Committee at the University of Birmingham.
The data was initially coded against a predetermined framework to target areas of interest identified from an initial philosophical analysis of the ethical issues involved. These included best interests, consideration of the interests of others and views about consent. A separate code termed ‘new issues’ was allocated to any ideas or lines of argument that had not been foreseen. Analytic memos were used to increase familiarity with the data and begin the analytical process. 22 Focused Coding 23 was used for the second coding cycle. This enabled the development of major categories and themes through the search for the most frequent and salient initial codes.
A short report of the interpretation of each participant's views was emailed back to the participant as a form of member validation, 24 which allowed them to check/correct the researcher's interpretation and add any additional comments. Those who replied (n = 4) agreed with the researcher's interpretation. Once these stages were completed by Gathani, Draper independently checked the coding and the two researchers discussed the analysis and came to an agreement about the interpretation.
Results
Four main themes were identified (1) donation reflects the consenting patient's overall benefit (2) non-maleficence, (3) types of consent and (4) the information provided for consent.
Participants' opinions regarding the necessary pre-mortem interventions required for DCD held across all three scenarios discussed in the interviews. The results therefore focus on participants' reasons for agreeing or disagreeing with such interventions as opposed to the differences between the scenarios.
Due to their location in an English hospital, participants tended to refer to ‘best interests’ rather than the ‘overall benefit’ referred to throughout this article. We take these terms to be broadly synonymous, so although quotations refer to ‘best interests’, we will continue to use ‘overall benefit’ in our discussion.
Donation reflects the consenting patient's overall benefit
The view held strongly by the majority of the participants was that DCD and the necessary pre-mortem interventions were of overall benefit to a consenting patient. Consent was regarded as an indication of a patient's wishes and it was of overall benefit for these wishes to be respected. P8: Generally, it's [organ donation] in a patient's best interests if they have wanted to donate their organs after death. P6: You need to respect all of her wishes and if she wants that to go ahead in this situation then we need to try and facilitate that. P1: We have a duty to the donor, to the recipient to make sure we're transplanting organs in optimum condition. P5: [T]he hospitals and the trust should do … everything possible to make these organs as optimal as possible in the recipient body.
Non-maleficence
Although it was felt that patients' wishes regarding organ donation should be respected, any procedure that caused the patient physical distress or went against the wishes of the family was considered wrong by all participants. Whilst it was universally agreed that the wishes of the patient should be regarded as decisive even if the family expressed conflicting wishes, none of the participants would go against the wishes of the family. Participants pointed out that pre-mortem interventions necessary for donation did not cause distress because the patients would be unconscious and sedated. P3: [T]he bottom line is always do no harm and you know, cause no distress for the family. P8: If they say they want to donate, and you don't do that, then you're sort of disrespecting their last wishes and you're doing harm by them. P7: I think we've got the right to dignity, as long as dignity is provided, I have no problems with additional tests on somebody who is dying. P1: You're doing what they want you to do, just get over it … it's interesting because it was the lay people on the ethics committee [that considered the issue of withdrawing treatment prior to DCD] that said ‘you what?’ They basically said, ‘you patronising so and so's. I want to donate my organs …. And you're gonna say that I can't donate my organs because you're too squeamish to pull my tube out?’ P4: Do we then get to the point where we then respect their wishes to donate so much that we should keep them alive until … a recipient becomes available? … [E]ven with a femoral line, you could well prang the artery. Are we then going to start giving blood transfusions? And resuscitate them?
Types of consent
Two participants said their practice was influenced by the strength of the desire to donate: interventions, such as a bronchoscopy, were only regarded as permissible if the patient had been especially passionate about organ donation. P3: In my practice I base this very much on how much consent or what this patient's feelings were. So I have some patients where I say I will do everything. P1: [I]t's a binary response isn't it … it's either right to proceed with donation or it's not. It's not a bit more right, sort of, so you do a bit more tests on that one. I think it's … an on/off thing isn't it?
Information provided for consent
Opinions were divided about whether consent for organ donation, specifically DCD, was sufficiently informed. Some participants thought that in normal medical practice, when one procedure may result in another, patients are usually told; this norm suggested that consent for DCD is not sufficiently informed because information about the procedure itself and/or the interventions that may need to precede it, is not provided by the current consenting system for organ donation. P9: I think that more information is needed about what happens, erm cos they're just agreeing to be an organ donor, without actually knowing what has to be done. And quite a lot of the procedures are quite invasive erm so I think it's important. P7: Well I think it's as informed as anything else. P2: [I]nformation is available … whether or not donors choose to use that information is a personal choice …. I do think it's true to say that many patients, many donors, choose not to know. P1: The notion of informed consent is that they know it's not informed. Intelligent people know that it's not informed and they accept that … they accept that as part of the contract of trust they have with you and I.
Limitations
This study was conducted in one transplant centre and only involved staff working in intensive care. Ten participants from the targeted ITU population were interviewed and it is possible that data saturation was not achieved. Consultants were overrepresented in the sample and junior doctors, registrars and nurses were under-represented. Consultants will, however, usually have ultimate responsibility for decisions regarding end-of-life care and so their views are likely to be the most influential in guiding practice. Data were not collected from potential donors or donor families, so further research involving these stakeholders may provide alternative perspectives and would be a useful addition to the discussion of this topic.
Discussion
Donation reflecting the overall benefit to patients
Participants did not draw a distinction between ‘best clinical interests’ and ‘overall benefit’ but clearly understood patients to have interests that extended beyond receiving optimal clinical care. A known wish to donate organs was regarded as having an interest in being a donor, including where this wish was reported by a family member or based on a patients known values, beliefs and feelings. This closely reflects the current guidance on how to interpret the MCA in the context of DCD, and it consistent with similar interpretations 17 including those outwith donation, 25 expressed elsewhere.
Establishing overall benefit in relation to DCD is, however, likely to be more complex than this. A minority of participants believed that pre-mortem interventions to facilitate organ donation should not compromise the experience of death for the patient or family, which highlights that a patient's interests in becoming a donor could be in conflict or intertwined with the interests of their family. As noted above, it may be reasonable to assume that, absent evidence to the contrary, a dying potential DCD donor would not consent to an intervention that would add disproportionately to distress experienced by family/friends; administering such an intervention would not then be justifiable with reference to their desire to donate. 6 This is not necessarily the case, however, and a patient could have valued donating organs over the interests of their family/friends. If this is the case, however, it is likely that this would be known to the family/friends, and the strength of feeling reported by them to the clinical team. Where this is not the case, it is not obvious where the balance should lie, especially where accounts of the patient's wishes are ambiguous or based on suppositions formed by applying more generally known values and beliefs. It should not, perhaps, be left to the family/friends alone to suggest that the patient may also have had an interest in safeguarding their interests but it may be difficult for clinicians to judge the extent to which DCD is adding to their distress in already difficult circumstances. Some of our participants did seem sensitive to the effect on the family but this was not clearly tied in our data to the interests that the patient might have in their well-being even though decisions under the MCA should not be motivated by consideration of anyone other than the patient.
Does an interest in donating organs imply that undergoing pre-mortem interventions to facilitate donation is of overall benefit?
Although the conflicting interests of others should not be considered relevant (in their own right) when assessing whether donation or treatment to facilitate donation should go ahead, the same is not true of a patient's own competing interests. A patient may have an interest in becoming a donor, but they may also have an interest in avoiding pain, invasive procedures and having their life shortened or extended by interventions. Some participants thought that patients who had consented to organ donation would want their organs to be donated in an optimal condition for successful transplantation even if this required further interventions, and they therefore felt that they had a duty to facilitate this. Although this may be a reasonable assumption in many cases, it is again not necessarily correct, and may disregard important competing interests. Taking a blood sample for tissue-typing purposes and thereby causing a small puncture wound would most likely be considered a minor countervailing consideration, and therefore be readily outweighed by a known wish to donate. In contrast, however, a test that required transfer to a different location with a significant risk of the patient dying whilst in transfer without relatives by their bedside could be a more significantly countervailing consideration, so much so that it could override any expressed wish to become an organ donor.
Whilst there is a considerable literature about how interventions prior to DCD can contribute to the transplantation of organs in their optimal condition,26,27 the views of those who have to interpret whether the wish to donate implies consent to undergo any or all procedures necessary to facilitate optimal transplantation have not been explored previously. It has been argued elsewhere that an interest in donating may reasonably also constitute an interest in the donated organs being transplanted successfully, but that this stops short of also implying that a donor has an interest in the condition of their organs being optimised. 25 This has implications for determining which pre-mortem interventions are permissible. Interventions to improve the chance of successful donation and transplantation may therefore have to be considered quite differently from interventions intended to bring about the best possible outcomes for the recipient.
Participants unanimously supported avoiding all pain and distress to the patient, and this again accords with the current guidance on DCD. 1 Many participants, however, did not seem to consider that invasive, albeit fairly painless, interventions such as a blood test that delayed the withdrawal of life-sustaining treatment, as compromising the interest of the donor even though a prior judgement had been made that withdrawing life-sustaining treatment was of overall benefit to the patient. The most important interest was considered to be the facilitation of DCD, and consequently the primary negative outcome, other than causing physical distress and an undignified death, was preventing the procurement of organs in their optimal condition. This may reflect an assumption by the participants about how patients rank their interests. Those who would go ahead with the pre-mortem interventions regardless of the type of consent given focussed solely on the benefits of organ donation, perhaps an unsurprising outcome for those seeing the benefit of organ donation so often in their working lives. Interests in avoiding relatively unburdensome pre-mortem interventions were dismissed in favour of the idea that registering on the ODR or agreeing that donation was something a patient would have wanted was compatible with accepting the necessary measures to achieve donation. Only two participants expressed contrary views that recognised potentially conflicting interests in such situations and subsequently attempted to balance both sides before arriving at a decision regarding which interventions could be considered morally permissible, as recommended by recent UKDEC guidance. 8
Whilst it seems reasonable to assume that an interest in avoiding non-therapeutic interventions is outweighed by a very strong desire to be an organ donor where the burdens are unsubstantial, it is nonetheless important that this interest is not completely overlooked and efforts should be made to establish and weigh up/aggregate any potentially competing considerations in the build-up to donation in order to establish what is of overall benefit.
One participant felt that any intervention ‘interfering’ with the patient's death was wrong, but this position may go too far in the other direction. Competing interests such as the interest in avoiding invasive interventions should be considered relative to the desire to donate: to not do so has serious and ‘far-reaching ramifications in terms of conflicts of interest’. 28 Obstacles should not be placed in the way of donation by patients who would have agreed to the pre-mortem interventions necessitated by DCD, and barriers should be erected to protect those who would not agree to the unnecessary prolongation of their dying process. Our data suggest that by regarding consent as binary, staff may not be sufficiently sensitive to the different interests in play in DCD, as we will now discuss.
Consent to donation and consent for pre-mortem interventions
The acceptability of pre-mortem interventions hinges on a patient's interest in avoiding burdensome pre-mortem interventions relative to their interest in being an organ donor. As few patients are likely to have left specific instructions covering this eventuality for practical purposes their wishes are unknowable. We must therefore look primarily to wishes in relation to the latter to establish the acceptability of pre-mortem interventions. The topic guide was designed to highlight relevant differences in how consent/wishes about organ donation were established. However, only two participants considered how differences could impact upon the permissibility of pre-mortem interventions.
At first glance, the varying ways in which consent can be given, as described by the UKDEC hierarchy, may seem like a promising indicator of whether pre-mortem interventions are of overall benefit to a patient based on a sliding scale for the strength of evidence for a patient's wish to donate: ‘[t]he stronger the evidence of the patient's desire to become an organ donor, the greater the weight this should be given in assessing whether a particular intervention would be in the patient's best interests’. 6 If a patient has clearly recorded their wishes about donation by joining the ODR, it is tempting to assume that there is a strong case for pre-mortem interventions to facilitate donation. However, the weakness of this assumption is that whilst the strength of evidence may be affected by the way in which consent is given, this gives no clear evidence of a much more important consideration: the potential donor's strength of desire to donate. This would not be problematic if information provision prior to joining the ODR was sufficient to ensure that all registrants understood the possibility of pre-mortem interventions to facilitate DCD, but as will be discussed shortly, this is not the case.
Joining the ODR indicates a patient has a desire to donate, but it does not say anything about the lengths to which they would be willing to go for donation to be facilitated: the strength of their desire. Indeed it may be that once a potential donor is unconscious, the strength of her desire to donate can only be gauged by speaking to family members about her beliefs, feelings and values. In this respect, types of consent IV and V on the UKDEC list could be a better indication of desires with respect to DCD than II and III if the question of whether the patient's values and beliefs would suggest agreement to pre-mortem interventions is addressed directly with those who know that patient best. Yet, as we will now discuss, our participants did not necessarily agree that the detailed information that such a judgement would require is being, nor should be, disclosed at the time consent is sought.
Information provided for DCD
Although many participants did not consider pre-mortem interventions to be ethically problematic, the fact that potential DCD donors, and their families, may be relatively uninformed about the donation processes still raises ethical concerns.
Most participants seemed to assume that potential donors and their family/friends do not require any specific information regarding DCD and associated pre-mortem interventions. This would imply that they believe consent to organ donation amounts to tacit consent for whatever procedures are required to facilitate it. This position is potentially problematic, however, because the informational requirements of consent for DBD are different from the informational requirements of consent for interventions while alive.29,30 A person can join the ODR knowing little or nothing about organ donation or what it entails. There is no mechanism for checking understanding at the point of registration. This may be because DBD was, until recently, the most likely donation pathway. DCD, on the other hand, entails invasive medical procedures during life, and it may therefore be reasonable to anticipate a greater need for information to ensure valid consent for DCD.
Consider the following: if Mr X consents to Mr Y staying in his house whilst he is away but Mr Y loses his key, should we assume that Mr X has tacitly consented to Mr Y breaking down the door to gain access to the house? Probably not, as Mr Y did not foresee that Mr X would lose the key and that the only way to access the house would be to break down the door. Of course, Mr X could be asked whether he minds. If Mr Y is habitually careless, friends may even warn Mr X of the potential consequences of his generosity. Similarly, if a patient has consented to organ donation but is not aware of the pre-mortem interventions this may involve, she may not be said to have consented to all and any actions on her living body required to maximise the chances of a successful donation and transplant.
Some participants asserted that consent for DCD was equivalent to non-transplant decisions and patients were generally not fully informed unless they asked to be. Participants suggested that trust in the medical profession meant that patients did not require information detailing medical procedures. In the case of non-transplant procedures trust in doctors is not unreasonable given that they are professionally bound to exercise their expertise for their patients' therapeutic benefit.31,32 However, DCD and the interventions required to facilitate it are not of therapeutic benefit to the donor, but are instead justified with reference to broader overall benefit. The current system of consent and provision of information for organ donation means that overall benefit can be difficult to establish. Given the increasing shift from DBD to DCD the time may be ripe for providing more detailed information at the point of entry to the ODR. This would provide a clearer indication of the wishes of the potential donor who is on the register and may also have the effect of generally increasing awareness of what DCD entails so that when such issues are discussed ahead of the need to make a decision (as we are all being encouraged to do) family/friends will be better placed to provide insight in to how to strike a balance between the various interests in play in relation to pre-mortem interventions.
Conclusions
The pre-mortem interventions required to ensure that a DCD donation is successful can only be justified if they are considered of overall benefit to the patient. Our results suggest that those caring for potential DCD donors may be running together consent for organ donation with consent to pre-mortem interventions that may be necessary to facilitate donation. It is possible that their binary view of consent to donation as being either given or withheld is rooted in DBD. It may also be a pragmatic response: there is normally very little recorded evidence about a patient's wishes regarding pre-mortem interventions. To insist on clear evidence of prior potential donor consent to each and every pre-mortem procedure is probably setting the bar too high. Our data suggest, however, that some clinicians believe that neither patients nor family/friends want detailed information about the procedures necessary to facilitate DCD. A system that encourages them to choose how much information they want might prevent unwarranted assumptions being made on this score. Nonetheless, it remains the responsibility of clinicians not to provide interventions that are not of overall benefit to their patients. Where the interventions required are more burdensome, greater evidence may be needed of the strength – or likely strength – of the desire to donate. Given how little information is provided at the point of registration onto the ODR, few assumptions regarding a patient wishes can be deduced from one's presence as registered donor. As the demand for transplantation increases and fuels the on-going drive for increased numbers of donors, there is a risk that the emphasis is being placed on the legal authority to remove organs for the purposes of donation and insufficient weight is being given to ensuring quality of consent being given. Greater transparency about the impact that being an organ donor can have on the dying process when joining the ODR may make it easier to assess the strength of people's desire to donate, and therefore their willingness to undergo any necessary pre-mortem interventions. It may also help to have more precise options in terms of what people can register for. For example, people could opt to register only for DBD, for DCD with only minimally invasive and burdensome interventions or for DCD by any means required in order to facilitate organ donation. This suggestion reflects UKDEC's direction of travel. 15
There is obviously a balance to strike, however. Giving more options to people joining the ODR may cause confusion and wrongly deter people from becoming registered donors. Equally, however, more options may help to strike the balance between removing obstacles to willing donation and erecting barriers to protect those whose interests lie elsewhere.
Footnotes
Acknowledgements
The authors would like to acknowledge the help of Mr Simon Bramhall who helped with the recruitment of participants for the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.