
Abstract
Introduction
Compulsory care is controversial, since respect for the patient’s autonomy is a standard requirement in health care. Many psychiatrists have experienced that patients with borderline personality syndrome sometimes demand compulsory care for themselves in order not to exert self-harm—like Ulysses contracts. The aim of this study was to examine the possible existence and extent of borderline personality syndrome-patient demands for Ulysses contracts regarding compulsory care in acute psychiatry, and how external influences and demands could affect the caregivers’ decisions about compulsory care.
Method
An anonymous questionnaire, with three questions with fixed answers, was distributed to 42 licensed medical doctors on call at the psychiatric emergency unit in the city of Stockholm. Thirty-three questionnaires were answered, giving a response rate of 79%.
Results
Ninety-four percent of the respondents recognized the phenomenon of borderline personality syndrome patients requesting compulsory care, 21% stated that this request had affected their clinical decision, and 55% had used compulsory care for other reasons than the patient’s best interest.
Discussion
The results indicate that compulsory care is sometimes given in the form of Ulysses contracts for borderline personality syndrome patients. Also, compulsory care is sometimes used for other reasons than the borderline personality syndrome patient’s best interest. Psychological mechanisms affect the decisions of both patients and caregivers. More research should be done concerning to whom, why, and with what consequences compulsory care is prescribed.
Keywords
Introduction
Compulsory care is a controversial form of health care, which is intended to be used with caution and as an exception to voluntary care, since respect for the patient’s autonomy should be the standard procedure. In Sweden, the legal ground for using compulsory care is when a patient (1) suffers from a “severe psychiatric disorder,” (2) is considered to be in indispensable need of psychiatric in-ward care, and (3) refuses such care (or is considered not having decision-making capacity). The definition of “severe psychiatric disorder” is somewhat vague but includes primarily psychotic or close-to-psychotic disturbances. 1 According to the legislation, the patient’s best interest and need for care is to be of main importance for the decision to prescribe compulsory care.
However, in clinical practice, one group of patients that frequently is subject to compulsory care is patients with borderline personality syndrome (BPS).2,3 BPS is a term for a set of debilitating personality characteristics with onset in young adult age. These personality traits include a chronic pattern of emotional instability, instability in interpersonal relations, separation anxiety, feeling of inner emptiness, switching sense of identity, difficulty handling anger, impulsiveness, suicidal ideation and self-harm, and transient dissociative symptoms. 4 The diagnosis BPS in itself is not considered to be a “severe psychiatric disorder,” even though the addition of an impulsive breakthrough of psychotic character, such as moments with severe dissociative symptoms, can be defined as such. 1
The most common reasons for hospitalization of patients with BPS are suicide attempts, self-harm, and suicidal communication.5,6 Suicidal behavior in BPS is common, often commanding the attention of others, and can be a way for the patient of handling strong distress and anxiety. 7 There is an increased suicide risk for patients with BPS. 8 However, there is no evidence that hospitalization reduces the suicide risk for BPS patients. 7 Also, hospital care for patients with BPS is questioned as hospitalization, at least when longer than a few days, does not seem to benefit this group of patients and sometimes even seems to aggravate the problem with regressive and self-destructive behaviour.7,9 As the NICE guidelines 10 point out: “It may be appropriate to consider admission for patients with a diagnosis of borderline personality disorder following a suicide attempt, but the assessing clinician should consider that such a response might inadvertently increase the risk in the longer term by decreasing the patient’s capacity to manage their own risk,” and “… despite frequent use of inpatient admissions in the management and treatment of people with borderline personality disorder, the effectiveness of admission as an intervention is uncertain.”
In clinical practice, some psychiatrists seem to have experienced that patients with BPS sometimes demand (explicitly or indirectly) compulsory hospitalization for themselves in order not to self-harm—like Ulysses contracts—but there is no research available concerning this. Like Ulysses afraid to be lured by the sirens, these patients feel they cannot trust themselves and are prepared to give up their freedom for a limited time in order to protect themselves. For example, BPS patients sometimes come to psychiatric emergency units and display a help-seeking behavior and pronounce suicidal intentions, but at the same time, they communicate, directly or indirectly, that voluntary care is not an option for them staying at the hospital since they cannot trust themselves. There have also been reports of clinicians using compulsory care and prolonged hospitalization for this group of patients as a way to avoid conflicts or criticism. 11 The aim of this study was to examine the existence and extent of BPS-patient demand for Ulysses contracts regarding compulsory care in acute psychiatry, and how external influences and demands affect the caregivers’ decisions about compulsory care. We want to incept a discussion concerning these phenomena, since they are challenging from a clinical, ethical, and juridical point of view.
Method
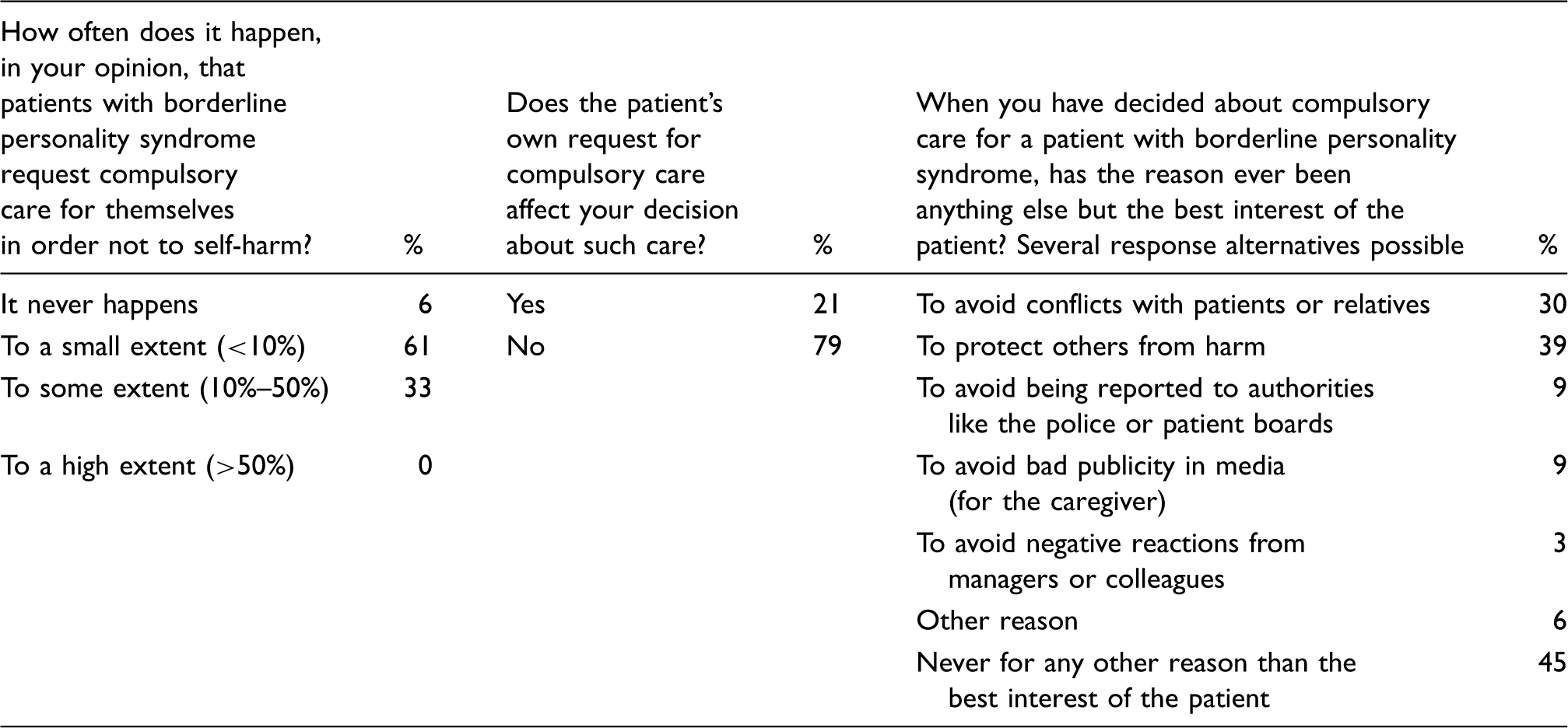
Overview of survey questions and responses.
Results
The number of answered questionnaires was 33. On the actual month of the study (October 2015), there were 42 active licensed physicians on call at the psychiatric emergency unit, leaving a response rate of 79%. For an overview of the results, see Table 1. Some respondents commented on the third question that “protect others from harm” was equal to “best interest of the patient,” but in this survey, we have chosen to separate these two items since prevention of harm to others primarily focuses on community safety rather than patient safety. 12 In summary, 94% of the respondents recognized the phenomenon of BPS patients requesting compulsory care, 21% stated that this request had affected their clinical decision, and 55% had used compulsory care for other reasons than the patient’s best interest.
Discussion
Even though this survey was made on a very small sample in only one center, the results clearly indicate that BPS patients sometimes demand Ulysses contracts regarding compulsory care. It remains to investigate the generalizability of our results, but we have no indications that this center would have a higher prescription of compulsory care for BPS patients than other centers.
The reason for BPS patients to sometimes want Ulysses contracts could be found in the characteristics of the disorder itself, where active passivity, rapid changes in affections, impulsivity, and fear of being alone and of trusting oneself have been described by Linehan. 9 Many patients with BPS have acted on destructive impulses before, with negative results, and even though self-destructiveness can have a strong allurement as anxiety-reducer, the patients often know that if they “go too far” they might actually die or get seriously injured.5,7,13 Thus, it is not surprising that some patients fear the responsibility of voluntary care.
Ulysses contracts regarding compulsory care could be interpreted as illegal in cases when the patient is considered to have decision-making capacity. However, if the clinician predicts that the patient will become decision-incompetent in the near future, this presumed instability in decisional capacity could be interpreted as a form of decision-incompetence, which would make the use of compulsory care legal.
However, one could ask if the caregiver should give in to these patient-demanded compulsory hospitalizations, despite good intentions, and reinforce the patient’s dysfunctional coping-strategies—at least when it comes to longer periods of hospitalization. The destructive effects of hospitalization and reduction of autonomy for patients with BPS are described in the literature, with consequences like long lengths of stay, increasing self-destructiveness, and increasing behavior of regression and helplessness.7,9,14 This knowledge has affected the NICE guidelines:
10
People with borderline personality disorder often find it hard to cope at times of crisis, and may look to others to take responsibility for their needs. While service providers may feel under pressure to try to do this, this approach may inadvertently undermine a person’s limited capacity to care for themselves.
NICE recommends that patients considered for inpatient care are actively involved in the decision-making, also regarding length and purpose of admission, that there is a joint explicit understanding of the potential benefits and harms of admission, and that the caregiver ensures that when compulsory care is used, voluntariness is resumed as soon as feasible. 10 Still, compulsory hospitalization is common.2,15 So, even if the intentions of the patient and caregiver are good when using Ulysses contracts, the long-term consequences could be bad.
Results from this questionnaire indicate that only a minority of physicians let their decisions regarding compulsory care be affected by the patients’ demands. At the same time, a majority of the physicians in this survey admit that the fear of negative consequences for the caregiver and others than the patient has affected decisions about compulsory care. This phenomenon has also been described in other articles.11,16,17 Patients with BPS can express quite distressing self-destructive thoughts and behaviors, which can upset and trigger people in their environment to demand that the physician takes “stronger” action. Thus, prescribing compulsory care—even if it leads to negative long-term effects for the patient—could be a way for the physician to calm the patient’s relatives and other caregivers and reduce the physician’s own anguish concerning complaints and suicide risk. However, compulsory hospitalization has no proven suicide risk-reducing effect for patients with BPS symptomatology,5,7,18,19 and suicide risk assessment is difficult and should not in itself guide clinical decisions concerning compulsory care.12,20 This is probably known to most psychiatrists, since it is mentioned in national health care programs,10,20,21 but it could stand in conflict with society’s intuitive or traditional ways of coping with suicidality; i.e., the mistaken idea that increased monitoring and control of BPS patients would reduce suicide risk.
Conclusion
The results indicate that compulsory care is sometimes given in the form of Ulysses contracts for BPS patients and not always given in the best interest of the patient. Psychological mechanisms affect the decisions of both patients and caregivers and not always in a way that leads to the best long-term results.7,9,14,17 Since compulsory care admits detention and the overruling of autonomy, it is, and should be, an exceptional form of care under constant review. The results from this small study indicate that more research should be done concerning the generalizability of our results, and for whom, why, and with what consequences compulsory care is prescribed.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support from the Swedish Research Council and from the Swedish Research Council for Health, Working Life and Welfare is gratefully acknowledged (2014-4024).