
Abstract
Background
Universal standards for bioethics, including the tenet of informed consent, should be upheld in the setting of humanitarian medical missions. The obstacles to obtaining informed consent in the global health setting have been thoroughly discussed in the literature, but no studies have investigated these issues from the patient’s perspective. We sought to understand the patient’s experience of the consent process during a four-week surgical mission to Haiti.
Methods
All patients selected for surgery during a mission to Hinche, Haiti, were invited to participate in a survey assessing communication between them and their physicians, their understanding of the surgical procedure, and their desire for information during the consent process. Complete data were collected from 55 patients.
Results
Understanding a basic explanation of surgery and the associated risks was important to 98% of Haitian surgical patients, and 96% reported the desire for extensive risk communication. All patients felt that they should demonstrate their understanding of the surgery by signing a consent form before undergoing surgery. No demographic factors correlated with patient desire for additional information regarding surgical risk.
Conclusions
Our results highlight several areas needing improvement in the consent process during surgical missions, including deliberate and consistent use of a consent process as well as more extensive risk communication. Our survey demonstrates that the process of obtaining informed consent for surgery is important to Haitian patients in the setting of short-term surgical missions and suggests that continued efforts to improve our methods are necessary.
Introduction
Short-term surgical missions face multiple obstacles when educating patients about the procedures they will be performing. These include respecting cultural norms for patient consent, crossing language barriers, and educating patients who may have only a primary education. Frequently, teams display paternalistic attitudes regarding consent—patients are informed of only bare-bones information under the belief that patients are either not sophisticated enough to understand the presented risks, or that patients in developing countries merely want the chance to get better without regard to potential untoward outcomes.1,2
The various cultural and infrastructure obstacles to obtaining informed consent in the global health setting have been extensively discussed in the literature. These barriers can take the form of inadequate communication between provider and patient, provider assumptions regarding patient desire for risk communication, insufficient patient health literacy, excessive patient or provider motivation to perform a procedure, limited time to develop a relationship between patient and provider, and various cultural barriers to having an open discussion of either the procedure or the prognosis.2–4 The perspectives on the informed consent process of patients living in developing countries have not been thoroughly investigated.
Our team sought to understand the patient’s experience of giving consent in short-term surgical missions during a four-week mission to Haiti. Our primary objective was to understand the amount of information Haitian patients wished to be provided during the consent process. We also wanted to identify whether patients felt significant communication and cultural barriers exist in the informed consent process between themselves and their American surgical team.
Materials and methods
A 28-question survey (Appendix 1) was designed to assess patient attitudes regarding informed consent during a four-week surgical mission in the Central Plateau of Haiti. The Emory University Institutional Review Board (IRB) reviewed the study design and determined that it met criteria for exemption from full review in accordance with policy from the United States Health and Human Services Department Office for Human Research Protections. No IRB exists at Hôpital Sainte Thérèse.
One hundred and fifty-two patients presented as potential candidates for surgery. All patients were screened for medical and surgical suitability. Patients who required surgeries other than the ones the team could perform were provided referral information. Patients who had comorbidities that needed additional medical management to optimize their health prior to surgery were provided initial treatment by the team and received referrals for continuing management. Following this screening process, 61 patients were considered appropriate surgical candidates.
Subsequent to this selection process, patients were then provided informed consent for the surgical procedure through a two-step process. Consent forms included basic explanations of surgery, general anesthesia, and neuraxial anesthesia, as well as the associated risks and benefits. These forms were written at a Flesch-Kincaid second-grade reading level and translated into Haitian Creole by a native-language speaker who is also a health-care worker. To ensure that patients were not excluded based on literacy (United Nations Children’s Fund reports a literacy rate of 49% in Haiti), all patients were shown videos of a Haitian nurse reading the consent forms applicable to their surgery. Surgery and anesthesia providers were available to explain and answer any questions. Certified medical interpreters were present throughout to facilitate communication between providers and patients. Once the consent videos were viewed and all questions were answered to the patient’s satisfaction, the patient signed the consent form.
All patients who were selected for surgery were invited to participate in the survey on the day of surgery. In the case of pediatric patients, the parent or guardian was invited to participate. Patients were informed that their participation in our survey would not change their care and that they may discontinue participation in the survey at any time for any reason before the survey was administered. The survey was provided in Creole using an interactive iPad survey application (QuickTapSurvey; TabbleDabble Inc., Toronto, Canada). Certified interpreters were present to assist in reading and administering the survey to all patients. Neither patient identity nor other identifying information was obtained. Demographic data including age, gender, and education level were collected. The remaining questions were intended to assess patient attitudes towards informed consent, perceptions related to risk communication, and patient comfort level with interacting with medical providers. To minimize bias, survey results were not reviewed until all surveys had been completed.
Collected data were analyzed using Student’s t test, and statistical significance was accepted with a P value of less than .05 (JMP, Version 10.0; SAS Institute Inc., Cary, North Carolina).
Results
Survey responses
Over the course of two weeks, 61 procedures were performed. Of the 61 patients who underwent surgery, we obtained complete survey results from 55 patients (Figure 1).
Study flowchart.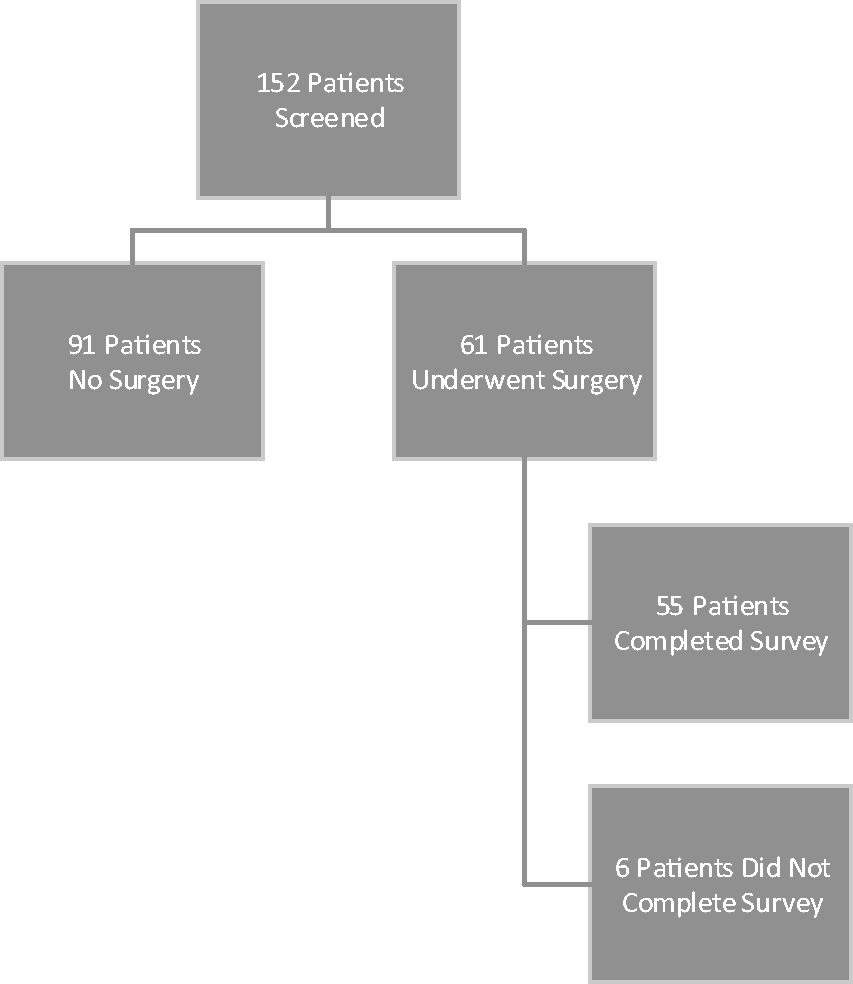
Patient population
Patient demographics.
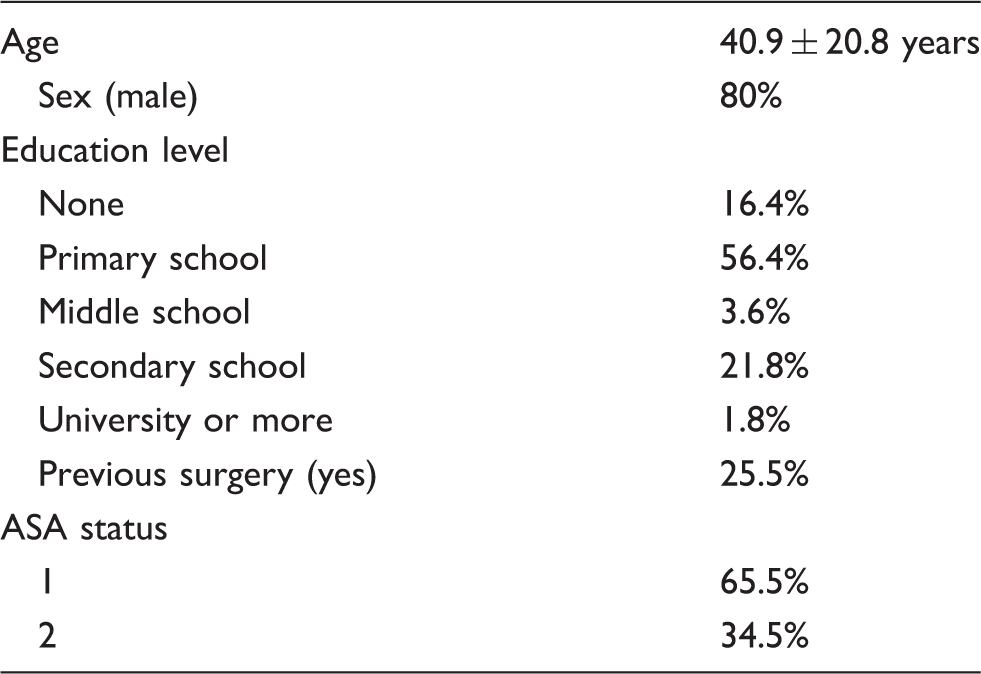
Due to the nature of surgeries performed, primarily hernia repair and prostatectomy, most patients (80%) were male. Twenty-five percent had previously undergone surgery. Most patients (73%) had completed primary school or less. All patients had an American society of anesthesiologists (ASA) physical status classification of one or two.
Attitudes toward informed consent and risk communication
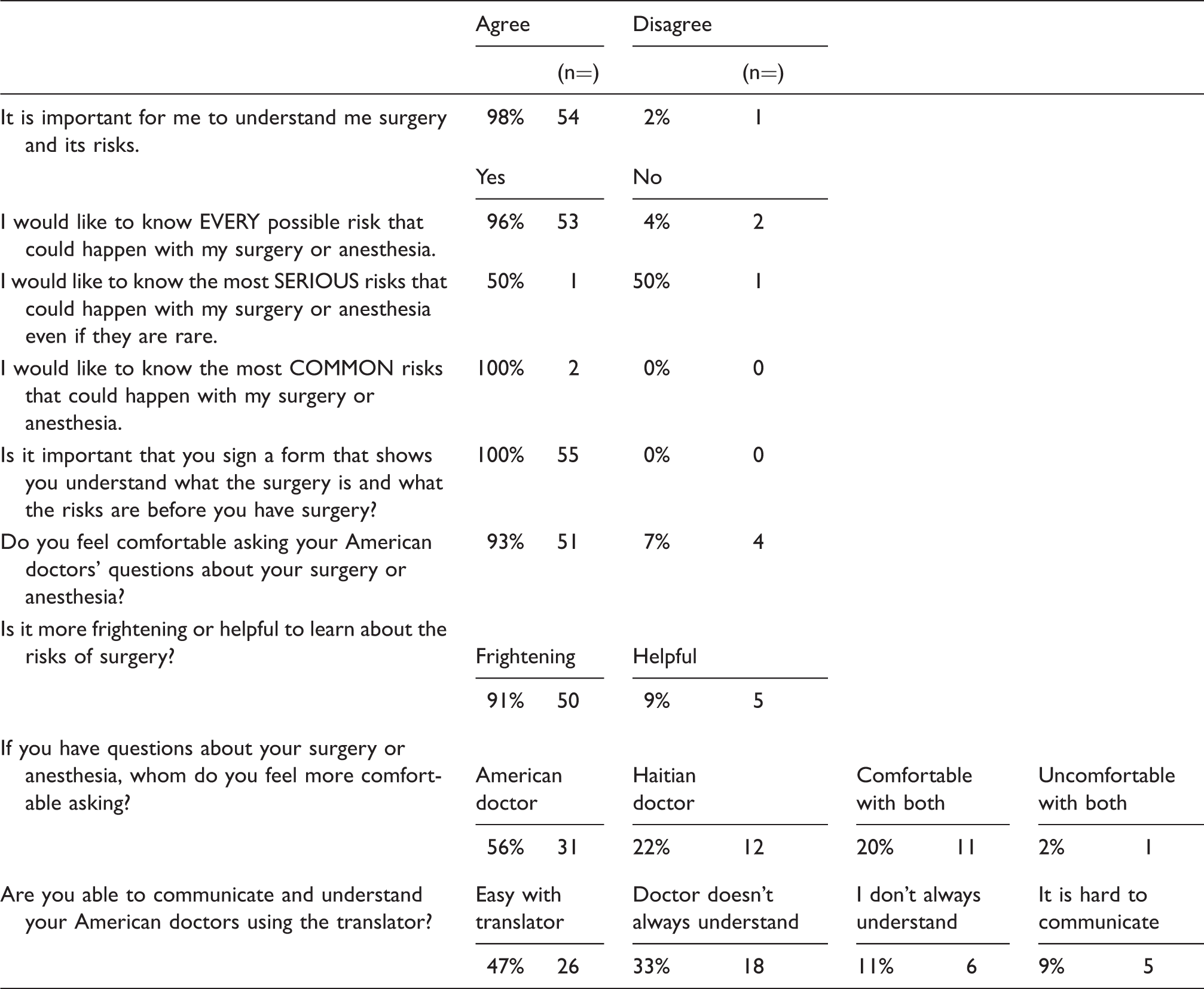
Responses to survey questions.
Communication
Several questions were designed to assess patient comfort level and ease of communication with medical providers. Almost all patients reported feeling comfortable asking the American team questions about surgery or anesthesia. Most patients (56%) felt more comfortable asking questions of the visiting medical team as compared to their Haitian counterparts, and 20% reported feeling equally comfortable asking American or Haitian providers’ questions. Twenty-two percent of patients reported feeling more comfortable asking questions of Haitian medical providers.
Nearly half (26/55) of the patients felt that communicating with the American team using an interpreter was easy. One-fifth of the patients reported difficulty with either communicating their questions or understanding the answer given. One-third (n = 18) of patients felt that communicating with the American team using interpreters was very difficult overall.
Efficacy of informed consent
Nearly every patient felt that watching the consent video improved his or her understanding of what the surgery and anesthetic would entail. After having all questions answered, 54 patients stated that they knew what surgery they were to undergo and understood why the surgery was being done. While most patients (n = 45) reported knowing the risks of their surgery, when asked to identify these risks, approximately one in four patients (15/55) chose a sham answer.
Patient variables
Age, gender, and education level did not correlate with patient desire to have additional information regarding surgical risk. There was no statistically significant relationship between these demographic variables and patient comfort with medical providers, desire for extensive risk communication, or attitudes toward informed consent.
Discussion
The Universal Declaration on Bioethics and Human Rights requires that any therapeutic medical intervention is “to be carried out with the prior, free, and informed consent of the person concerned, based on adequate information.” 5 There is consensus among the medical community that universal standards for bioethics, including the tenet of informed consent, should be upheld in the setting of humanitarian medical missions. 6 In addition to its ethical role, obtaining consent is occasionally taught as a defense against malpractice rather than an opportunity to allow the patient a role in medical decision-making. 3
In contrast to the methods used in the United States, informed consent is often obtained differently during short-term medical missions.2,7 Patients who undergo surgery during surgical missions typically arrive to the hospital with their decision to undergo surgery already made. Often, a formal consent process is overlooked altogether. The wider acceptance of paternalism in medicine by both patients and providers in low-income countries, combined with the improbability of malpractice accusations in surgical missions, makes the existence of a formal consent process unlikely. 8 When the patient arrives at the hospital on the day of surgery, assent is often assumed. Accepting this “assent” in place of informed consent reflects our tendency to see paternalism and autonomy in a different light when we practice medicine in developing nations. Similar to evolving views involving research in pediatric patients, assent should not be equated with consent, and consent should be obtained in competent patients. 9
Vulnerable populations require special protection to be enrolled as research participants. 10 The patients we see during short-term surgical missions are particularly vulnerable based upon several factors. 11 First, poor health-care infrastructure and poverty decrease the available treatment options. Lower education levels and health literacy imply that patients will likely need a more thorough explanation if they are to understand their surgery and have appropriate expectations regarding outcomes and risk. Finally, patients undergoing surgical procedures are vulnerable once administered medications render them unable to refuse care or participate in intra-operative decisions. 1 These vulnerabilities oblige medical providers to be especially thoughtful when approaching the consent process with patients in short-term surgical missions.
The various obstacles for medical providers obtaining informed consent in the global health setting have been extensively discussed in the literature, but the patient’s perspective has not been thoroughly investigated. We analyzed the results of surveys completed by 55 patients during a short-term surgical mission to Hinche, Haiti. The vast majority (98%) of our patients desired understanding of their surgery and its associated risks; they also preferred a formal informed consent process to demonstrate this understanding. While the consent form may be important, it is likely that the process it represents is what patients find crucial. 12 Despite a lower level of health literacy, patients desired extensive risk communication, with 90.9% reporting that learning the risks of surgery was more helpful than frightening. In Haiti, providers should ensure that patients fully understand what surgery will entail, including postoperative care and recovery, and are deliberately invited to give consent.
The new multi-step consent process, which included the use of video, was well received by patients. Educational videos have several demonstrable patient benefits. Increased patient understanding has been demonstrated in Haitian patients who viewed an educational video. 13 Our team has demonstrated a decrease in wound infection attributed to increased compliance with postoperative wound care following implementation of a video. In this study, 98% of patients reported that the consent video helped them to understand what happens during surgery and anesthesia. Additionally, the video allowed for more efficient use of medical interpreters, which is one of our most limited resources. Using a video to explain information both standardized the message received by patients as well as allowed increased utilization of interpreters in other hospital areas, including the operating room and clinics.
Informed consent is an imperfect process even in the most optimal settings. Many studies have demonstrated that patients’ ability to retain information given during the consent process is extremely poor.14–18 Providers face numerous obstacles in underdeveloped countries when obtaining informed consent and the effectiveness of the consent process we use remains unclear. While 27% of patients in our study selected sham answers when asked to identify risks of their procedures, this is no more than what has been reported in similar studies performed outside of the global health setting. Ellis et al. described that after verbal counseling by a clinician, 38% of patients in a study performed in Edinburgh, Scotland, could not recall their diagnosis. 19 One study evaluating postoperative aortic aneurysm repair patients in the United States found that 18% of patients would not have undergone surgery if they understood the challenges of the recovery process. 20 Studies conducted on informed consent in the United States and Europe have shown miscomprehension rates between 20 and 33%, and results from studies in developing countries have shown even less comprehension. Krosin et al. showed that 90% of patients in Mali misunderstood withdrawal criterion for participation in research.21–23 The literature asserts that patient recall of risk is consistently poor and highly variable. 24 However, studies have shown that this poor understanding does not necessarily correlate with patient dissatisfaction. In fact, patient satisfaction with the information provided has typically been shown to be high, despite poor retention.25–28 Thus, while effectiveness may be difficult to measure, our results highlight the importance of focusing future efforts on more extensive risk communication with Haitian patients.
We were unable to identify any demographic factor that correlated with a patient’s desire for greater understanding their surgery and its risks. Our sample size was too small to identify a relationship between any single demographic variable measured and comfort level with American providers or the ability to communicate using an interpreter. Our Haitian patients expressed a preference for extensive risk communication, and a formal process demonstrating their understanding regardless of their age, gender, or education level.
Of the four cardinal principles of medical ethics described by Childress and Beauchamp (beneficence, nonmaleficence, autonomy, and justice), autonomy is at the core of the moral imperative for informed consent. 29 As physicians, we are obligated to promote the respect for autonomous decisions of our patients, though not necessarily above all other principles. Autonomous decisions imply intention, and without appropriate disclosure from the physician and understanding by the patient, medical decisions cannot be intentional. For disclosure to be “appropriate,” cultural context is critical. That is, the values emphasized in the United States are not always prioritized similarly in other cultures. 30 For example, some Eastern cultures are more likely to prioritize community interests over those of the individual. Others have been reported to believe that discussing illness or death may cause it to happen. A preference for physician directive rather than being offered choices has been reported in some Pacific Islander groups. 31 These examples demonstrate that the “best” method of obtaining informed consent in short-term surgical missions could be different for nearly every culture. Thus, it is important to remember that the results we obtained from surveying Haitian patients are not representative of all patients in lower income countries.
Based on our study results, it is apparent that Haitian patients desire a more complete consent discussion by physicians participating in medical missions. Our recommendation to provide more extensive informed consent discussions with Haitian patients may not necessarily be extrapolated to all patients in developing countries, and providers are encouraged to identify methods of medical decision-making that emphasize the values and priorities of their specific patient population. As part of the larger goal to improve the patient experience when undergoing surgery in a global health context, further efforts are necessary to ensure ethically sound methods of obtaining culturally appropriate informed consent.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.