
Abstract
We do not know how much clinical physicians carrying out clinical trials in oncology and haematology struggle with ethical concerns. To our knowledge, no empirical research exists on these questions in a Nordic context. Therefore, this study aims to learn what kinds of ethical challenges physicians in Sweden, Denmark and Finland (n = 29) face when caring for patients in clinical trials; and what strategies, if any, they have developed to deal with them. The main findings were that clinical cancer trials pose ethical challenges related to autonomy issues, unreasonable hope for benefits and the therapeutic misconception. Nevertheless, some physicians expressed that struggling with such challenges was not of great concern. This conveys a culture of hope where health care professionals and patients uphold hope and mutually support belief in clinical trials. This culture being implicit, physicians need opportunities to deliberately reflect over the characteristics that should constitute this culture.
Introduction
Almost all clinical cancer centres carry out clinical trials. Care and research are there closely intertwined, even though the dominant paradigm of research ethics has made a sharp distinction between the two
1
(cf. HHS
2
). This can be viewed as problematic: Research ethics is characterized by a basic incoherence: on the one hand, clinical research is seen as ethically distinct from medical care; on the contrary, the obligations of investigators, especially in clinical trials, are thought to be grounded in the ethics of the physician-patient relationship.
3
(cf. Katz
4
)
Clinicians frequently face ethical situations or dilemmas.6,7 By definition, an ethical dilemma involves the need to choose from among two or more morally preferable options or between equally unacceptable courses of action, where one choice prevents selection of the other. 8 As ethical challenges are not always appropriately described as dilemmas, it might instead be preferable to speak of ethical challenges or issues. Ethical challenges can arise because of conflicting roles, each role connected with professional ideals, aspirations and norms, which might conflict in certain situations. There is thus a change of focus, from the rational conflicts involved with ethical dilemmas, to the lived conflicts resulting from particularistic and role-based circumstances in lived experience. Sometimes challenges arise because of physicians simultaneously having several different roles that make conflicting demands upon them. They can simultaneously function as clinically responsible practitioner and researcher, as well as having complementary roles such as the administratively and economically responsible, or being a collaborator with other staff categories. In their various roles, different moral, organizational or professional expectations and ideals might be present. 9 For example, while clinical work often is based on an ethics of care, research is ultimately based on the value of knowledge: ‘If there is one overriding ethic in research, it is to learn and to tell the truth’. 10
We do not know much about if, and if so, how physicians carrying out clinical trials struggle with ethical concerns. To this end, we need to investigate experiences of physicians recruiting patients to clinical cancer trials and dealing with the sometimes-disparate frameworks of care and research. No previous empirical research has addressed these questions in a Nordic context, to our knowledge.
This study aims to find the kinds of ethical issues and challenges physicians face and experience when they include and care for patients in clinical trials; and what strategies, if any, they have developed to deal with these ethical challenges.
Methods
This study used a descriptive design and explorative qualitative approach. 11 An exploratory–descriptive design is suitable as this design describes a largely unknown phenomenon in a Nordic setting from the perspective of the participants. The design is in line with the aim, to develop a rich understanding of physicians’ challenges and experiences when including and caring for patients in clinical trials. In this way, lived experiences of physicians have been sought and analysed.
Settings and participants
The inclusion criteria were to work at a cancer clinic and to be involved in clinical trials at that clinic. Initially, the division heads at each Nordic university hospital, located in large urban cities, were asked for permission to perform the interviews. The intention was to recruit the same number and types of clinics in every country. After approaching the department heads, we eventually got access to two clinical research units in Sweden, one in Denmark and two in Finland (from two different hospitals). However, we did not succeed in recruiting any clinics from Norway in the timespan available.
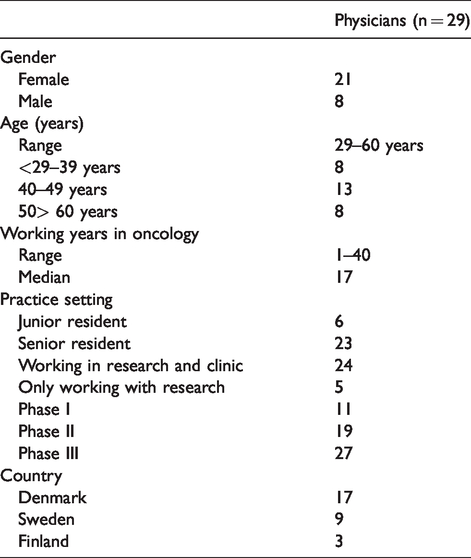
The interviews were performed by all the authors except MM and SE. In total, 29 in-depth interviews were carried out with physicians from the Nordic clinics. Of these, two-thirds of the sample was female. The participants were at different stages of their careers (from junior resident with one year of experience to a senior with 40 years). About two-thirds were senior residents. Thirty-eight per cent had familiarity with phase I trials, 59% with phase II and 93% with phase III, so there was a good spread of experience in different phases of research. Sample characteristics are presented in Table 1.
Participants’ characteristics.
Data collection
The interview guide was semi-structured, informed by previous research, and covered known ethical issues of concern to physicians. By being largely open, it created lot of opportunities for the physicians to bring forth their own experiences, concerns and thoughts. We first compiled, discussed and wrote the interview guide in English, so that we could agree on the content and wordings. Translation into each national language ensued, in order for us to carry out the interviews in each native language. This process seemed to ensure both coherency and facilitate feasibility. The guide started with a broad question: ‘What does it mean for you to work with care and research?’. The guide had three sections: (1) experiences when recruiting, (2) ethical dilemmas and issues and (3) potential strategies. After each question, when necessary, follow-up questions were asked of the form: ‘Can you tell me more; When, why and how?’.
A pilot study with three health care professionals was performed and to refine the interview questions we did several minor revisions. The interviews took place at the clinic or outside the hospital according to the subject’s wishes and needs. They were about an hour long, audiotaped and transcribed verbatim in the local language.
Data analysis
A qualitative, inductive content analysis was used, 12 as we had little former knowledge about this issue in a Nordic context. The inductive analysis was performed in three stages: preparation, organizing and reporting. In the first stage, TEG and SE prepared and independently coded the first six Swedish interviews. In the second stage, the study group met in a workshop and decided on which codes to use. A first draft of possible themes was identified in the same six interviews. Next, all the Swedish and Danish interview transcripts were read repeatedly, and codified by SE. The Finnish analysis was done by AH and MP according to the initially codes formulated in the workshop; the quotes considered were translated into English to facilitate further processing by the whole group. Then, TEG and SE analysed the whole data set and considered categories to organize the content (using ATLAS.ti 8). We revised the categories in several steps, using Skype and frequent email exchanges, until the findings found broad consensus. When analysing and sorting the codes into categories, we could notice consistent and overarching themes in the data. Eventually, the content of the interviews was summarized into themes.
Results
The results describe the physicians’ experiences of ethics in clinical research according to three dominant themes: (1) research in support of clinical work, (2) the culture of hope and (3) lacking strategies. Three categories were identified regarding the culture of hope: (i) challenge of autonomy, (ii) unrealistic hope and therapeutic misconception (TM) and (iii) avoiding the talk. The quotes’ provenance is indicated by S for Swedish, D for Danish and F for Finnish interviewees (numbers do not correspond to the order of interviews to ensure further anonymity).
Research in support of clinical work
When asked if they experience tensions or conflicts of interest being both clinician and researcher, many mentioned that they see the roles as associated: ‘These are two sides of the same coin’ (D6). The research was looked upon as a necessary, integrated part of cancer care and as a condition for being able to offer patients cutting-edge treatments. Research is a natural constituent of an academic cancer centre’s daily work and benefits the patients: We do work with studies all the time; as clinicians. It is part of being a physician at an academic hospital so then you aren’t a researcher. You are just a clinician doing studies. Then you do not ponder ethical issues so much, someone else did that, you just do your part. (S1) We then get access to drugs we never would have had otherwise. And that is good for the patient, so we do it. It is a win-win situation for the patient who gets something and the drug companies who learns something. And so we do the in-between work, so to speak. And we are happy to do it, for the patient’s sake. (S3) …it is alright to say that this is a study, it is voluntary to participate, all the things you are expected to say and do say; but there is a difference between saying that and then say ‘You can also decline’. That can be said in an appropriate way, you can put more or less emphasis on it. (D16) For example, in a study where you receive three months treatment instead of six months standard treatment, you need as a physician to be very sure that this is least as good before participating. However, every time you inform a patient for such a study, it feels problematic, because the patient often asks the difficult questions: Are you sure that this is just as good? And so on… Then you cannot say … I mean, if you are sure, you wouldn’t do the study, that's the problem. All research aiming to reduce treatment intensity is thus ethically problematic by definition. (S4)
The culture of hope
The ethical challenges brought up most by the physicians were the challenge of autonomy, unrealistic hope, TM and the pull to avoid difficult discussions with the fatally ill patients.
The challenge of autonomy and informed consent
A critical ethical challenge identified concerned patient autonomy. Most of the physicians said that explaining clinical trials to patients is very demanding. A majority was concerned about how much information patients really do understand. Even physicians sometimes have difficulties with understanding the trial protocols, they believed: These likelihood things are like UFO things for most people. People don’t understand relative and absolute benefit or harm, or difference between them. You must explain in words of one syllable. (F3) We also [physicians] have difficulties in understanding exactly how they work, and why they are not working, i.e. dose escalation studies; doctors hardly understand the point of them, so patients just can’t. (D1)
Many interviewees found the written information about the study of little help to patients. The information is too long, complicated and include excessive facts about side effects: ‘And that I find annoying, there is like some sort of barrier; you seemingly just can’t distribute patient information which can be easily understood, not looking like a telephone directory’ (D11). When asked if they believe that the patients read the written information provided, many physicians were unsure. Great help with these difficulties from the nurses were often emphasized; they could be relied on to elaborate and deepen study understanding when physicians felt a bit unsure. ‘I think our nurses are very good at talking with relatives. The clinical trial unit has great skills; they genuinely look to the individual patients and make sure they are well informed’ (D7).
Another major concern was that patients often want to enrol in all kinds of research to obtain cutting-edge drugs not part of conventional therapy (such as immunotherapy): ‘You can get patients to sign up for anything’ (D8). Phase I trials were mentioned by most physicians as the major ethical challenge: When one is to include patients in a phase-I-study investigating a drug, well, the purpose of a phase-1-study is to investigate toxicity. You are not interested in efficacy; you just want to check that the very drug does not kill the patients. Patients usually enrol because they want something, like a straw. (S1) To me, they seem much more interested in hearing about studies involving treatment. Studies without any extra pain, side effects, medicines, somehow being exposed to something, scans for example, they are not that interested in, I believe. They prefer to focus on that for which they came. (D17) The press and the internet is where they often find out all sorts of things, which still is in development, but where much knowledge is disseminated underway. And then, as they learn about it, they can’t understand why this treatment isn’t publicly available. (D8) Then this person says to me, “you make sure he gets in the right arm”. So he tried to push us into … influencing the result of randomization, which we cannot do. I mean, he does not understand this, but we can’t do it. But it came to a huge conflict with this son when I said I couldn’t do it so “take it or leave it”. (S3)
Unrealistic hope and TM
Unrealistic hope and/or the TM were mentioned in all interviews, particularly encountered in phase I trials. This can be a challenge: ‘[A] patient can have hope, but you must be realistic. You cannot cheat patients’ (F2). When asked if patients often have unrealistic hope, one respondent said: ‘Yes, they always have. That is part of the game. However, unfortunately, the sickest patients are worst in this respect’ (S4). Another said: ‘[A] large portion of patients think they will be cured from the incurable disease’ (F3). When asked if they believe that patients in end of life will participate in all kind of trials related to hope, one physician answered: ‘I believe that if you were to ask all fatally ill cancer patients, a truly substantial part would say that they want to participate precisely because of that hope…’ (D14).
Many interviewees stated that patients truly believe that in research patients’ best interests are promoted and that patients therefore have difficulties to distinguish clinical research from standard treatment: ‘They believe that if the clinic offers a new treatment, it is because we suppose it’s better’ (D16). This, as several physicians pointed out, was not only an issue among the patients but also for health care personnel: We do believe there is a straw to reach for as long as we include patients in studies; this might, by all means be unrealistic, but in such cases, also the clinical judgment is that there must be a chance; otherwise, the patient would not be included in the study. (S9)
Avoid the talk
Breaking bad news was highlighted as a complex and challenging task which sometimes were avoided: ‘…as long as I haven’t spoken; it’s not there’ (D1). As participation and hope was seen as a patient strategy to keep going through hard times, it became a reason for physicians to not deliver bad news to patients, trying to be supportive. All agreed that maintaining hope is an important and vital task for health care professionals, and for some of the physicians the easiest thing to do was giving end of life patients a straw to clutch: ‘…it is better just to say ‘let’s try this’ (D1). …initially one tries to avoid being unrealistic but one doesn’t present patients with a worst-case scenario… “we’ll see how this works”, and then: “But will not all get cured?” Then one has to answer that no, you won’t. But it might go well for a long time and then…one has to downplay it so that…deep inside they all know they are dying of cancer, they know that, so they want me to say: “this new treatment will cure you!”. I do not say that but often rather that we’ll see how it goes…and hopefully it does go in the right direction. (S3)
Lacking strategies
Many physicians said they lack forums for addressing ethical questions and that there is no clear strategy for dealing with ethical challenges. On the other hand, most physicians insisted that their clinic displays acceptance of and openness to ethical questions and discussions. When asked why they then do not explicitly discuss ethical issues, one explanation was: ‘I just don’t believe we think we have ethical dilemmas at all. So it is usually just not brought up’ (D1). Others said it was related to poor time resources or logistical hindrances: ‘We have few discussions about ethical dilemmas. We have a shortage of time, and therefore we don’t have time for such meetings. It’s a logistical hindrance in daily basis’ (S6). Another said: ‘[We talk] less and less because the time we have together is decreasing’ (D5). Time pressure was mentioned in almost all interviews as an essential barrier for addressing ethical challenges. Still, the self-image was of doctors having the individual craft and will to decide the best way to solve the problem. As one stated: …we do talk about it, but as with many doctors, we are very autonomous people, that is, we do what we believe is best. Therefore, just because some others think this or that, well, there is no guarantee that the assigned physician or the one at the bedside chooses to comply. (D7) Yes, I probably discuss those [ethical issues] more with nurses than with my physician colleagues. I do not want to generalize, but nurses has a keener eye … and it is good that some has that perspective, as physicians might be more concerned with treatment issues … My experience is that nurses sooner will put an end to some treatment or so, or not include [patients] … while we doctors want to treat and maybe, sorry if this sounds a bit harsh, can see things from a greater perspective. That it is good for medicine, not just the individual person. (D14) I do a lot of rationalizing. Actually I might have considered a few cases being wrongly handled, but most often I think that this was the option available; we couldn’t do otherwise. You tend to become desensitized. This does not have to be a bad thing; you should be diligent but not too sad. It is for the patient and the next-of-kin to be sad; the physician should be rational. (S8) But there are exclusion criteria in the trials that make [some patients] unfit to be included when unethical, as, I believe those who have designed the study have thought about which groups are badly suited for it, which then is nicely and clearly expressed in exclusion criteria. That goes so well together with how unethical it would be to include the group in a trial. (D2)
Discussion: The culture of hope
A common outlook was the close relationship between research and care. The respective goals of these activities were not perceived to be in opposition; on the contrary, the overriding idea was that they coincide. Strikingly, many physicians downplayed the importance of ethical problems related to their daily research work. We will look at the major ethical challenges identified, before discussing how many findings indicate the presence of a ‘culture of hope’, where potential ethical challenges might often go unnoticed (Figure 1).
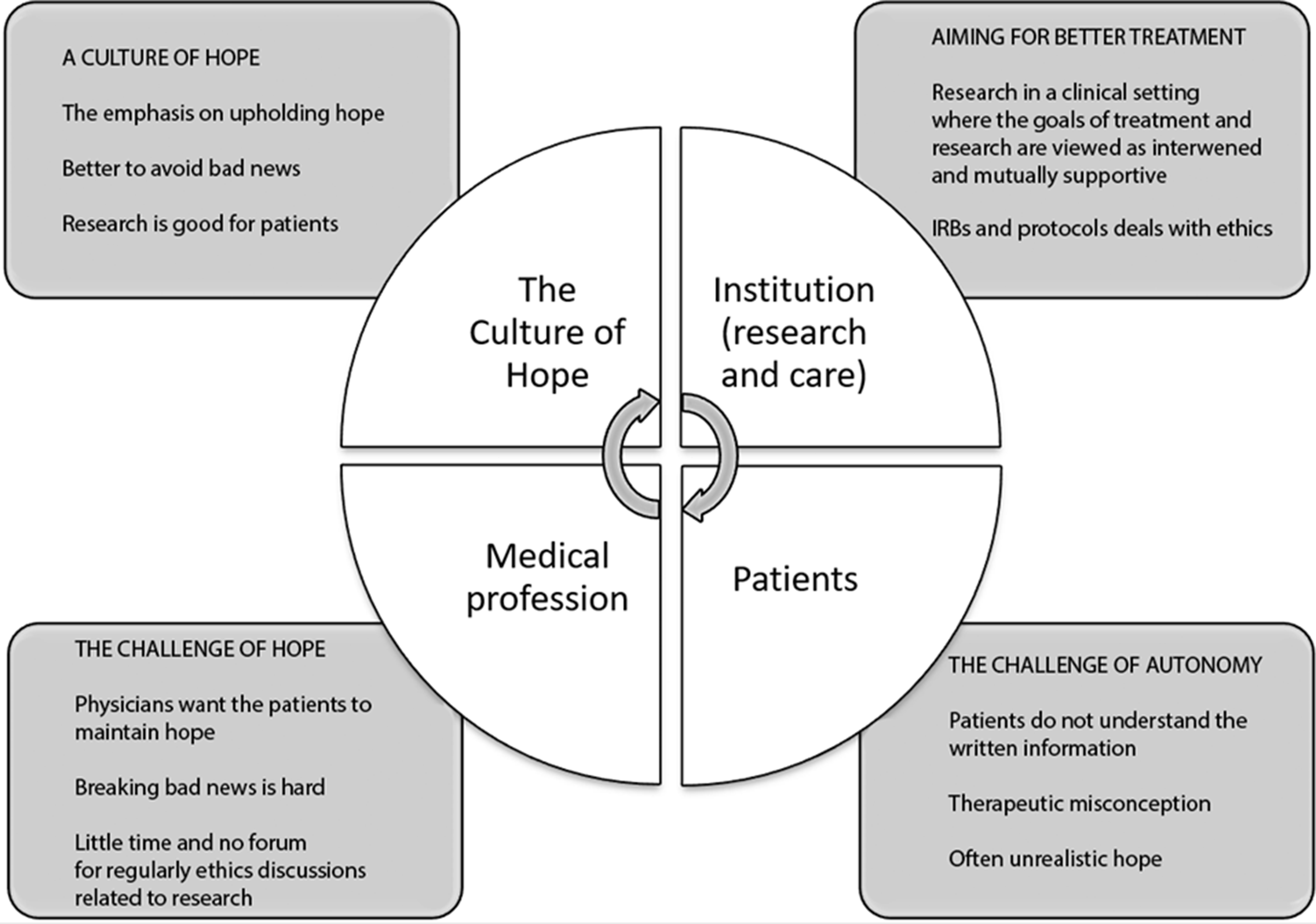
The circle of hope.
Ethical dilemmas resulting from moral doubt or uncertainty, i.e. the need to choose among two or more morally acceptable options or between equally unacceptable ones, were not mentioned often. Most ethical challenges were related to autonomy, an unreasonable hope for benefits or the TM (particularly in phase I trials), findings in line with other studies. 13 Physicians were concerned over patient ability to understand the aim and scope of trials, especially phase I trials, as many patients are willing to participate in anything that offer a glimpse of hope. They do not show much interest in studies without the potential to benefit them. This makes informing patients difficult, and the physicians often seemed to experience a moral duty to respect autonomy and make sure patients decide whether to participate from a proper understanding of the study. But regardless of whether you inform about a study that a patient can frame in terms of hope or about a study lacking that quality, the information will not be just neutrally received. The understanding of the information is rather heavily shaped by patient interests, which many physicians in the study seemed well aware of. Such a willingness to participate in experimental research is previously well documented, as well as poor understanding of trial purpose.14–17
Unrealistic hope was a prominent ethical issue reported. The physicians felt concerned both with patients losing touch with what was going on, and with their own part in creating or sustaining unrealistic expectations on possible benefit from trials. One possible explanation for unrealistic hope stems from patients not understanding the difference between care and research and then mistakenly believing that research aims primarily for their benefit (the TM). Factors facilitating such unrealistic hope include having the research carried out by one’s own physician, 18 which was commonly occurring among the physicians in our study. Joffe and Weeks 19 have shown that not only patients but also physicians and investigators might share such misconceptions of clinical trials. 20 This is further discussed by McDougall et al., 21 who suggest a new concept, therapeutic appropriation (TA). TA occurs, they state, when ‘patients, or clinicians, actively reframe research participation as an opportunity to enhance patients’ clinical care, while simultaneously acknowledging the generalised research aims’. Then they do not mistakenly conceptualize research as care, but are seizing an opportunity to find hope in something they know is research. This strikes us a valid interpretation also of our data.
Despite identifying these ethical challenges, most physicians stated that struggling with them was not a great concern. If they sometimes had some pressing ethical issues of this kind they might discuss them with nurses or in ad hoc meetings with colleagues, but in everyday work, such challenges were usually not brought to the fore. Looking at the results, several reasons may explain why these ethical issues are not given more attention.
First, there simply is no time to attend to ethical issues and no institutional systems in place to deal with them. 22 All the participants agreed on this, basically, and expressed that clinical work and study protocols are in strong focus. It is not surprising then that ethical issues are out of view. This phenomenon, called ‘ethical fading’, has previously been studied: when we focus on other aspects of a situation, this psychological process makes the ethical aspects of a decision disappear from view. 23 As the number and complexities of clinical guidelines typically are overwhelming for physicians, 24 striving for compliance with just those policies and guidelines will leave little room for thinking about research ethics.
Second, physicians supposed that any ethically difficult issues were already taken care of by those responsible (the PIs) for the study, by the physician who refers patients to the specific study and by the Ethical Review Board (IRB or ERB). Since the ERB had previously evaluated the ethics of the clinical trial protocol and its methods, and appropriate steps had been taken to protect the rights and welfare of patients, they were at ease with the protocol. Some mentioned explicitly that the inclusion and exclusion criteria could be of good help when dealing with ethical issues, such as unrealistic hope. In this way, the physicians relied on the ERBs and protocols to do the ethical work for them; so for e.g. when patients in an advanced stage of cancer are in poor clinical condition but still want to participate, making use of the exclusion criteria were thought to be an aid in protecting them from harm.
Third, most physicians were convinced that in general it is an advantage to participate in clinical trials. Physicians felt no moral conflict in endorsing enrolment as an important option, mostly because they were convinced that they met patient interests by offering access to the best available treatment. This positive outlook even extended to phase I trials for some of the physicians, but most of them pointed to indirect benefits in that setting, such as meeting patient wishes for more surveillance or contact. It is important to bear in mind, however, that most experimental drugs in phase I trial are not effective. 25 Also, there is often no substantial therapeutic difference between the standard treatment and the clinical trial drug.26,27 In this study, some physicians were convinced that research constitutes the best available treatment for patients, and when becoming uncertain whether it is so in a specific case, they acted as gatekeepers for patient enrolment, as a physician’s primary focus is the benefit and interests of the individual patient. This finding is consistent with the literature. In the study of Joffe and Weeks, 19 U.S. oncologists (n = 547) were asked to state the aim of clinical trials and to specify why they asked patients to participate. Most of them said that clinical trials aim to collect generalizable knowledge for future research; still, many also claimed that a principal purpose is to benefit them. Some oncologists viewed trial participation as a state-of-the-art therapy. This shows that there is a lack of consensus among physicians ‘working with care and research about the nature of the relationship between research and treatment in clinical trials’. 27
The end result is a culture of hope where health care professionals and patients perpetually reinforce their common belief in clinical trials and their hope for something that might be somewhat helpful in a dreadful situation. Whether such TA is a good thing or not is not for us to say. The involved do certainly not embrace this process consciously, but it is a result of several factors, reflecting deep and common human traits and dispositions. What is troubling is the very fact that this culture is not the result of weighing moral aspects of the culture. Is it better to have hope than having to realize that the end is near? Is being truthful more important than being compassionate for a doctor? Is doing what you want in the final days more valuable than being ‘a fighter to the end’? Some such questions are deeply personal, some are professional rather, while some belong on a societal level, but if they fade from view they cannot be thought over at all.
From the perspective of research ethics, a demarcation between medicine and research has been widespread. This distinction was explicit in codes and regulations such as the Declaration of Helsinki and the Belmont Report, for example. In research there are partly different norms, meant to protect subjects from the kind of abuse that historically have shaped and provoked the emergence of research ethics. Therefore, in a way, a culture of hope situated in a care setting clashes with some of the traditional principles of research ethics that is built upon such a distinction. This has possible consequences for the conduct, review and regulation of clinical trials. This is not least so when it comes to addressing the issue of how to present the information to the patients. 28 Detailed regulations for trials exist under the supervision of ethical committees or institutional review boards, while a culture of hope might to a larger extent leaving many issues to professional discretion and judgment. True, in some countries, the existence of clinical, hospital or institutional ethics committees might present an opportunity for ethical deliberation beyond professional self-governance, but they are not that established in the Nordic countries. At the same time, there is in the practice of medicine often no sharp separation between practicing medicine and conducting research nowadays and many stakeholders argue for new ways of integrating the two. For example, a Learning Healthcare System is defined by the Institute of Medicine as a system in which ‘science, informatics, incentives, and culture are aligned for continuous improvement and innovation, with best practices seamlessly embedded in the delivery process and new knowledge captured as an integral by-product of the delivery experience’. 28 In this line of thought, a culture of hope might still be preferable to one where people for ethical reasons must be deprived of their own human impulses and motivations – not least as research collaboration between science and society should be based on a common understanding and commitment to shared goals and values. 29 The issues found here are highly complex, where patients and physicians have a variety of motivations and emotions affecting choices and attitudes, which means there are no easy answers.
In conclusion, the present system or culture needs to become visible to those working in it and be openly discussed. Ethics training with a focus on normative education and visible formal systems may only be partially effective. These issues also include various hidden, informal, systematic factors of communication, surveillance and sanctioning mechanisms that together make up an organizational climate or ethical infrastructure. 30 There is a need to provide many more opportunities for physicians to come together for reflection and conversation around these issues – an infrastructure that facilitates and promotes ethical reflection. 31 Ethical challenges should not be allowed to fade away from sight, but be put high on the agenda for a future where care and research become even more closely knit and a likely place where we put our trust and hope for a future.
Strength and limitations of study
The current study adds to previous work by investigating the views and experiences of physicians in three different clinical cancer settings within the Nordic countries. The key strength of this study is the large sample size; physicians had a significant variety of both short and long experience of clinical trials, in addition to having experiences from all three trial phases. However, these findings have some limitations. Although the sample size was large, the small sample size in each country means it is not possible to draw conclusions on any differences between the countries. It is up to the reader to determine to what extent the results are transferable to settings outside that which was studied here. 32 Nevertheless, the findings from Sweden, Denmark and Finland are not unique to this context and are therefore likely to be representative of other clinical trials setting outside the Northern countries.
Acknowledgements
The authors acknowledge and thank all research participants who supported and facilitated this research. We are also thankful to Merja Pirinen (MP) who helped out with the Finnish interviews.
Ethical considerations
This study followed each country’s regulatory demands. According to Swedish, Danish and Finnish law on research involving humans, no ethical approval is required for this kind of non-interventional study which does not involve risks or the processing of sensitive personal data. 33 Approval to perform interviews was obtained from the department head of each hospital. The study followed the requirements of the Declaration of Helsinki, 34 in that participants were informed about the study, the handling of personal data, and how confidentiality would be kept in the management of material and in publishing and presenting results (§§ 24–26). Written informed consent was obtained at the start of the interviews. All identifiers were removed from transcripts before being distributed to the research network.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.