
Abstract
Background
Regulations on research ethics in France have evolved considerably over the past four years: the implementation of the Jardé law and of the General Data Protection Regulations have changed the landscape of research ethics for research involving or not involving human persons. In a context of creation of an Institutional Review Board at the University of Bordeaux, France, we sought to explore research ethics practices and perceptions in the medical community of our University Hospital.
Methods
A short questionnaire was sent to all physicians of the University Hospital of Bordeaux. The questionnaire included closed questions and main topics were: physicians’ education in research ethics, ethics practices concerning researches non implying human persons, and physicians’ perceptions about current regulations.
Results
86 questionnaires were sent back (response rate: 24.2%). If a majority of physicians have validated Good Clinical Practices (GCPs) trainings (76%), there was a low rate of specific training on fundamental references in research ethics and a high proportion of responders do not consider themselves as educated in research ethics after completion of GCPs (56%). Regulations on research ethics have many implications on medical research, especially by inducing changes in protocols in order to alleviate ethical requirements (57%). Malpractices were acknowledged like false mention of positive opinion from an ethics committee (21%). If If a majority of responders considers regulations as a positive answer to research ethics, a large majority considers it as a constraint and a complexification of research process. For 58%, regulations in research ethics are perceived as a hindrance for research initiatives.
Conclusion
Because of their impact on research process, regulations seem to constitute a scarecrow for physicians. Lack of training, bad representations and questionable practices (or even malpractices) highlight the need to improve education and to propose concrete guidance for medical researchers.
Introduction
Regulations on research ethics in France have significantly changed over the past four years. Since November 2016, Jardé law governing “researches involving the human person” (RIHP) has been applied. RIHPs are defined as “researches carried out on healthy or sick volunteers aiming to develop biological or medical knowledge”. 1 All prospective studies (interventional and non-interventional ones) are concerned by this law which makes imperative to submit RIHPs’ protocols to a Committee for the Protection of Persons (CPP: French equivalent of independent ethics committees). CPPs give their approvals on the basis of a both scientific and ethical analysis. With Jardé law, the spectrum of researches requiring the approval of a CPP has been widened, all the more since non-interventional prospective studies are considered as RIHPs.
Researches considered “not involving human persons” (RNIHPs) do not need to be submitted to a CPP. RNIHPs are researches in Humanities, but in most cases, they consist in retrospective studies based on secondary uses of care data (they constitute the majority of medical theses). However, the general data protection regulation (GDPR) has also modified the concrete practices for RNIHPs. Indeed, information and non-opposition of patients concerning the collection and use of their data have become imperative. 2 In addition, approval by an Institutional Review Board (IRB) becomes almost systematic before acceptance for publication. There are currently no clear recommendations or regulations for these IRBs in France, so these procedures and analysis frameworks can be very heterogeneous. 3 For example, in the University Hospital of Bordeaux, France, ethical approvals are currently given by the local Ethics Committee (which is not a genuine IRB).
We are currently working on the creation of a support structure for researchers in research ethics. Its mission will be to offer training in research ethics and to provide ethical approval for RNIHPs through an IRB. We aim to create a unique and transversal structure for the University Hospital but also for all departments of the Universities of Bordeaux, France.
In this context, we conducted a survey among physicians of the University Hospital of Bordeaux in order to explore education, general practices and perceptions in research ethics in the medical community.
Methods
A questionnaire with closed questions (with binary answers: Yes/No) was used for data collect. The amount of questions was limited as much as possible in order to optimize the response rate.
A first version of the questionnaire was created by a panel of 10 health professionals or researchers (3 pharmacists, two physicians, two nurses, one research coordinator and one health anthropologist). All have expertise in research conduct or research ethics and belong to the Ethics Committee of the University Hospital of Bordeaux.
Three topics were identified to constitute this survey about research ethics: education, concrete practices and perceptions about research ethics. Those topics were chosen according to the experience of our Ethics Committee (on the basis of the most frequent questions from physicians of our institution but also of our experience in ethical approval for RNIHPs). They also correspond to the functional role of our forthcoming research ethics support structure.
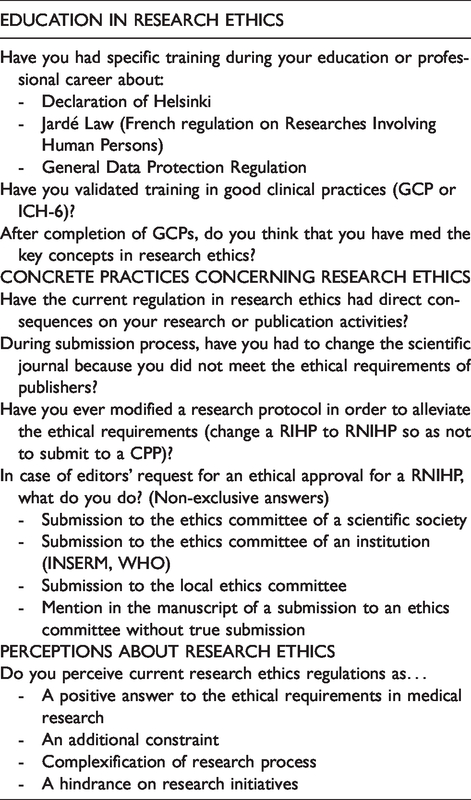
The first part explored physicians’ specific education in research ethics, their validation of Good Clinical Practices (GCP) and their perception of GCPs’ relevance in terms of research ethics education. The second section focused on concrete practices in research ethics for RNIHPs which constitute a major part of studies carried out at a hospital and which do not need a primary validation from a CPP. It was about exploring the frequency of research changes directly due to research ethics regulation and what institution was convoked by physicians in case of request for an ethical approval for a RNIHP. Finally, a last section focused on physicians’ perception of research ethics according four submitted proposals.
This first version of the questionnaire was presented to a group of 8 physicians (all working at the radiation oncology department of the University Hospital of Bordeaux). This meeting permitted to check the readability and the intelligibility of the questionnaire. This test phase has especially modified the chosen formulation of the proposals concerning perceptions on research ethics. It appeared that negative proposals were uneasy to evaluate so that affirmative proposals were privileged, so finally three of the four proposals appeared as negative opinions about research ethics. In addition, the distinction between the terms “complexification”, “constraint” and “hindrance” was necessary and well understood. These choices of formulation were finally validated by the research team. Collected data are summarized in Table 1.
Questionnaires’ content (binary answers: YES/NO).
The questionnaire was sent to the professional email address of all physicians belonging to medical, surgical, and biomedical services of the University Hospital of Bordeaux. Participants sent back their questionnaires by email. Questionnaires remained anonymous, so that after collection, no identifying information remained on questionnaires (a separated table of answerers was used to avoid double answers). Only a descriptive analysis was done. This study was approved by the Ethics Committee of the University Hospital of Bordeaux (N° GP - CE 2020 – 12).
Results and discussion
Three hundred and fifty four questionnaires were sent and 86 answers were received (response rate of 24.2%). Results are summarized in Table 2.
Summary of results.
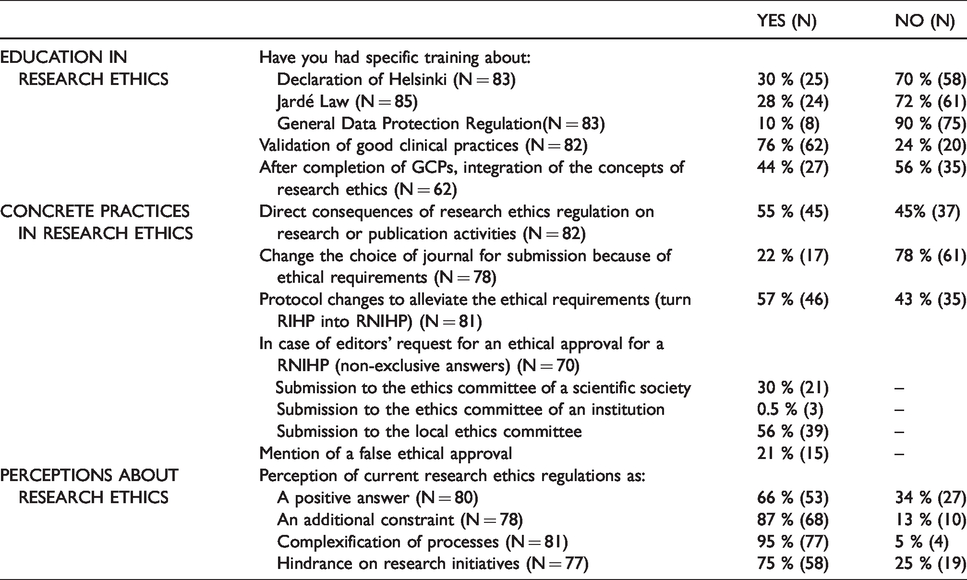
Concerning physicians’ training in research ethics, the survey showed that a minority of doctors have already followed specific training on one of the three most relevant regulations in research ethics (Declaration of Helsinki, Jardé Law or GDPR) while specific training courses along with practical guidance for researchers have showed concrete impacts on research activity. 4 On the contrary, a majority of them (76%) have validated a GCPs training as investigators. GCPs are identified as the minimal training that physicians must validate in order to consider researchers as sufficiently trained in research ethics to be investigators. 5 The frequent requirement from sponsors or IRBs for GCPs validations explains this high rate. However, among trained physicians, only 44% consider that they have integrated the key concepts of research ethics after GCPs completion. For a majority of physicians, a gap seems to exist between their representation about being educated and their genuine feeling of being educated in research ethics with GCPs. The high heterogeneity of the media of GCPs trainings (from classic course to e-learning with final online questionnaires for validation) may bias these results. If the content of knowledges that GCPs must provide to investigators is well described, their relevance has already been discussed in the literature. 6 Another explanation for this gap is that GCPs are more about procedures and practices in accordance with ethical principles than a genuine teaching in research ethics which should consist in integration of values and of their complexity. However GCPs are not perceived as a specific education in research in most cases, strengthening the need of research ethics training for physicians.
The second part of this survey on research ethics practices demonstrates the concrete impact of regulation: 55% of physicians report direct consequences on their research activities. For about a quarter of responders, ethical requirements have required changing the scientific journal to which scientific articles were submitted. Ethical requirement is still not mandatory for all scientific journals even for RIHP, so that ethically-non-validated researches may still be published.7–9
More questioning is that a majority of physicians acknowledge they already have modified research protocols in order to ease ethical requirements (57%). Review of protocols by a Research Ethics Committee constitutes a gold standard of research ethics. 10 However the caution and depth of the ethical analysis are proportionate to the nature of researches so that non interventional studies require less deep analysis than interventional ones. This seems logical since the levels of risks and constraints are different according to study designs. Thus, there is no mandatory prior validation from an IRB for retrospective studies in France. 1 Our results tend to show that this gradation of ethical review according to type of research is fully integrated from the design phase of the research, to the point that it can even condition the design. In these cases, ethical review is seen as an obstacle which is better to avoid in order to set up research anyway. One could fear that research ethics plays the role of a scarecrow for physicians, inducing an increase of “ethically-easy” but less relevant works (this result is closely linked to the perception of research ethics as a complexification or a constraint according to our study).
Physicians reported their practices concerning the type of ethics committee they solicit in case of need for ethical analysis of RNIHP. In most cases, the local ethics committee was identified as the preferred structure, probably due to the proximity of our structure. Ethical reviews from learned societies were in second, their expertise in the field of research being a strong element of justification for this choice. More concerning is that 21% of physicians acknowledge they intentionally mention false ethical approvals (for 12/15 this practice was the only one reported). This result is in accordance with previous analysis of ethical approvals. 11 Many reasons can be assumed for explaining this type of misconduct among physicians: the absence of perception of risks for patients in RNIHPs or an appreciation of futility for such approvals concerning RNIHPs. However, this highlights an absence of perception of ethical issues concerning RNIHPs, in particular all ethical concerns regarding the collection and use of healthcare data. The possible lack of reactivity of IRBs must also be mentioned. In a general context of rush for publications, ethical approvals appear as time loss which is one of the main critics against IRBs. 12 This is why our local Ethics Committee proposes a maximal delay of 30 days to provide approvals, which seems more reactive than other existing structures. 13
Last topic was physicians’ perceptions about regulations on research ethics. If a majority considers current regulations as a positive answer to an imperative ethical framework, this does not seem effortless. Perceptions of constraint and complexification are overwhelming (respectively 87 and 95%). The changing landscape of research ethics may contribute to these findings. In recent years, national and European policies have extended the concerns about research ethics, imposing new frameworks to biomedical research (Jardé RGPD). The quasi systematic editors’ request for ethical approval (even for RNIPHs) has also strengthened the place of research ethics. Complexification of research process due to ethical review also stems from the lack of identified or clearly regulated structures for RNIHPs in France. Moreover, good practices in IRBs are not defined, so that ethical approvals are very heterogeneous. 14 Time consumption and bureaucratic work may be others reasons for those perceptions. 15
75% of responders consider current ethical regulation as a hindrance for research. Such a bad representation among physicians has already been reported in the literature. 16 This result is particularly concerning and enlightens a gap between research stakeholders and French ethical frameworks. Paul Ricoeur aptly described that moral standards can only work if moral agents identify them as legitimate. The feeling of being obliged to apply the standard arises from this recognition by the stakeholders. 17 This result shows that a lack of congruence seems to exist between current regulations and what researchers could identify as an adequate ethical framework. In this context, research ethics regulation might be a scarecrow for physicians, first because it lengthens research procedures, but also because it does not seem relevant according physicians’ perceptions.
Our study has many limitations. First, our survey has only been addressed to physicians in a single institution whereas other health professionals might be involved in research initiatives (as nurses, psychologists or dental surgeons). Our results concern only one professional community. Second, the response rate is quite low, leading to a limited amount of data.
The use of a questionnaire is also questionable. This was the first time such a sensitive topic was explored in our institution. As our study could reveal bad perceptions and even ethical misconduct, this anonymous way to collect data was privileged. Biases due to misinterpretation are possible with questionnaires. We tried to limit them, especially concerning the evaluation of physicians’ perceptions about research ethics. Even if no formalized cognitive pre testing was done, discussing the first version of the questionnaire with a group of physicians permitted to limit the interpretation bias. The most debated term was “hindrance” We intended to explore the possible appreciation of ethics regulation as an obstruction towards research, as it has already been discussed in the literature.18,19 This term was considered as the most adapted both by our research team and the panel of 8 physicians to which the first version of the questionnaire was submitted. Finally, the current work takes place in a singular context of the creation of a transdisciplinary institutional ethics committee. Such a context might influence results.
Further researches are necessary in order to better understand the underlying reasons of our results. We especially aim to explore what physicians identify as concrete ethical matters in biomedical research, and what they perceive as needs or appropriate processes in research ethics. The idea is to explore physicians’ proper definitions of research ethics principles and not only to ask them about the currently identified ones. We will proceed to new studies with semi-directive interviews and focus groups using empirical bioethics methodology in order to take simultaneously into account collected empirical data during research process but also the underlying normative questioning. 20 Symbiotic empirical bioethics seems the more adequate methodology, as it is found on a philosophically-neutral and stakeholders-centered approach to explore data but also to question or even build normative assumptions. 21 The final objective of our approach is to identify the means to rehabilitate research ethics and to promote it not only as a procedure to be respected but also as an authentic and adequate support corresponding to the needs and expectations of both physicians and society. 22
Conclusion
Our survey aimed to describe the training, practices and perceptions of physicians in research ethics in a French university hospital. The results fuel the need to reinforce specific training in research ethics and to create relevant and effective processes for research ethics practices. Strengthening training in research ethics on the basis of regulatory references but also on the basis of theoretical and historical contributions appears to be the first priority. 23 The main objective would be to give back to research ethics its real role within our institution: support for researchers aiming an ethical and valuable biomedical research, and not a scarecrow or a simple procedure perceived as an obstacle.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.