
Abstract
Background
Pediatric critical care physician attitudes about withdrawal of ventricular assist devices (VAD) and extracorporeal membrane oxygenation (ECMO) in cases of medical futility are poorly defined. Our aim was to define current attitudes regarding the withdrawal of these devices.
Methods
IRB-approved, cross-sectional observational survey conducted among pediatric critical care attending physicians and fellow physicians in the United States between 2016 and 2017. Data was collected anonymously and statistically analyzed.
Results
A total of 158 physicians responded with 67% being attending physicians. Compared to a VAD, a higher percentage had taken care of a patient on ECMO where the device was turned off because care was believed to be futile (99% vs. 84%), including currently (95% vs. 57%). Nearly all reported that it can be ethically permissible to withdraw support from a patient with a VAD and on ECMO (97% vs. 99%), but varied opinions existed as to who should ultimately make this decision if the patient/their family disagrees. More respondents agreed that a patient/their family should agree to withdrawal of VAD or ECMO support prior to initiation if futility is later determined (60% vs. 58%) and that protocols should be created for VAD and ECMO withdrawal (77% vs. 76%).
Conclusion
Most pediatric critical care physicians felt that it can be ethically permissible to withdraw VAD and ECMO support. Our study indicates that pediatric VAD and ECMO withdrawal protocols are desired, but further investigation is needed to determine how to best design protocols that would incorporate multiple stakeholders.
Keywords
Introduction
A ventricular assist device (VAD) and extracorporeal membrane oxygenation (ECMO) are medical devices utilized in both the pediatric intensive care unit (ICU) and the pediatric cardiothoracic ICU. ECMO use was first described in a pediatric patient in 1976. 1 VAD use in pediatric patients has been described since the early 1990s. 2
While both ECMO and VADs are distinct devices with different indications and uses, they do share some common roles. One of the primary roles of ECMO and a VAD is to provide mechanical circulatory support for critically ill pediatric patients, especially in cases of cardiac failure.2,3
ECMO can also be used in cases of severe pulmonary failure in addition to heart failure where a patient’s risk of death despite conventional therapy is high.4,5 One of the first uses of ECMO was as a support tool for newborns with severe respiratory failure.6–8 Additionally, ECMO has been established as a support modality for pediatric patients with acute respiratory distress syndrome by the Pediatric Acute Lung Injury Consensus Conference. 9
VADs can be used as a bridge to transplantation in patients with congenital heart disease and end-stage heart failure as well as a bridge to recovery.10,11 VADs have also been used as destination therapy or long-term support and treatment for adult patients with end-stage heart failure. 11 The use of a VAD is much rarer than the use of ECMO.
There are contraindications to both ECMO and VADs, and decisions to move forward with these modalities initially involves a risk-benefit analysis on the part of the clinician. Contraindications to VADs typically include irreversible end-organ function as well as active systemic infection. 11 Relative contraindications to ECMO according to the Extracorporeal Life Support Organization (ELSO) typically include conditions incompatible with life, pre-existing conditions which may affect quality of life (including neurological status, malignancy and risk of bleeding), patient age and patient size. 5
Both devices have a typical length of use that distinguishes them from other medical technologies that may be used over several years, like dialysis and mechanical ventilation. ECMO has been shown to have a high rate of complications, including bleeding and thrombosis, with increased mortality after two weeks of use.5,12 VADs have been described for both short-term use as well as long-term use with complications including bleeding, thrombosis, infection and neurologic dysfunction.10,11
Outcomes for both ECMO and VADs have been described in the literature. VADs have overall been reported to have favorable outcomes with recent data showing that for pediatric patients supported by VADs, 79% underwent heart transplant, and 14% died.11,13 Pediatric survival to discharge and/or transplantation after ECMO has been recently reported to be between 42% and 58%, with extracorporeal cardiopulmonary resuscitation (ECPR) cases having the lowest survival rate and pulmonary cases having the highest survival rate. 14 Survival rates to discharge and/or transfer after ECMO for neonatal cases have recently been reported to be between 41% to 73%, with ECPR cases having the lowest survival rate and pulmonary cases having the highest survival rate. 14
During the course of a pediatric patient’s illness and outside a family’s request for withdrawal, withdrawal of these devices will typically occur due to three reasons. The first is that the patient improves or receives a heart and/or lung transplantation and no longer requires mechanical circulatory support. The second is that the patient expires while on support by predefined brain death criteria. In these two instances, there are clear reasons for discontinuation of ECMO or VAD support. The third is when medical futility has been determined. While there are many definitions and interpretations, medical futility can be defined as any clinical scenario where based on current medical literature the medical team can conclude that any further treatments, apart from comfort care, will not reasonably lead to a restoration of quality of life that would be acceptable to the patient or their family. 15
When cases become medically futile, there are no consensus guidelines that exist to assist in the withdrawal of these devices. In this scenario, disagreement among the medical team and the patient or their family may occur regarding who should ultimately make this decision to discontinue ECMO or VAD support. Stopping ECMO in cases of futility has been suggested in ELSO’s guidelines for ECMO cases. 5
There have been several studies evaluating both ECMO and VAD withdrawal. Studies examining the ethics of VAD withdrawal have found that withdrawal of VAD support can be ethically permissible but also ethically challenging.16,17 Recent publications regarding VAD withdrawal highlight the absence, complexities and need for comprehensive guideline development.18,19 One study has also shown that withdrawal of ECMO support can also be a difficult decision, especially for families and parents to accept. 20
Despite these potential risks and challenges of ECMO and VAD support, both medical devices also have seen an increase in the amount of use since their implementation. There have been more than 55,000 reported pediatric cases of ECMO since 1990. 21 In addition, at a recent meeting of the International Society of Heart and Lung Transplantation it was reported that as of June 2016 there have been a total of 171 pediatric VAD implantations at 29 centers around the world, with 65% of those being implanted in the last two years. 22
Based on our experience, withdrawal of mechanical circulatory support in a case of medical futility can become ethically challenging when there is disagreement between the medical team and the patient/their family. This is due to the fact that withdrawal of these devices would very likely lead to the cardiac death of the patient. With increasingly medically complex patients in the pediatric critical care medicine population, these ethical issues will continue to persist and likely increase in number in the future.14,21–26 For these reasons, the development of consensus guidelines to help pediatric critical care physicians in these difficult ethical situations may be useful as an adjunct to clinical expertise. To our knowledge, however, these attitudes have yet to be described.
The aim of this descriptive study was to define the current attitudes regarding the withdrawal of VAD and ECMO support among pediatric critical care physicians in cases of medical futility. The ultimate goal of this study is to aid in the creation of future practice guidelines for clinicians. We hypothesized that withdrawal of a VAD would be seen as ethically different than ECMO withdrawal. We also hypothesized that protocols for VAD and ECMO withdrawal are rare but desired.
Methods
This study was approved by the UCLA Institutional Review Board. A waiver of informed consent was obtained. A 23-question online survey was created to examine the current attitudes of pediatric critical care attending and fellow physicians in the United States (Appendix 1). The same questions were asked for VADs as well as ECMO. Experience with VADs and ECMO was assessed along with current practice exposure. Questions were also asked about protocols for withdrawal of VAD and ECMO support.
This multicenter study was conducted in the United States between 2016–2017. The online survey was distributed through a variety of sources including a pediatric critical care website (www.PedSCCM.org), pediatric critical care fellowship program directors, an email list and a newsletter. In the United States, pediatric ECMO and VAD patients may be cared for by critical care physicians with varied training and experience. Furthermore, ECMO and VAD patients may not be physically confined to a cardiac ICU. To ensure a broad sampling of opinion, our survey was not targeted to nor did it distinguish between critical care physicians working in cardiac ICUs. Anonymous data was collected for statistical analysis using SurveyMonkey (San Mateo, CA).
Survey results were statistically analyzed. Kappa coefficients were used to interpret degree of agreement between opinions, with a value close to 1 representing close agreement. Fisher’s exact test was utilized to determine whether or not there was a significant association between responses. Results were interpreted with the statistical significance in relation to the clinical setting, with P < 0.05 being considered statistically significant.
Results
A total of 158 physicians responded to the survey. Given that we employed survey advertising in a newsletter as well as through a website, we cannot calculate the total number of invited participants and, therefore, a response rate. Attending physicians comprised 66% (105) of the respondents, with fellow physicians comprising the remaining 34% (53). Attending physicians had a range of years of experience with 30.2% (32) with less than 5 years of experience, 27.4% (29) with 5–10 years of experience, 13.2% (14) with 11–15 years of experience and 29.2% (31) with 16 or more years of experience. Our respondents were distributed throughout the country: Northeast 25% (40), Midwest 32% (50), West 30% (47) and South 13% (21).
Most respondents had taken care of and currently take care of both ECMO and VAD patients. Compared to a VAD, a higher percentage of physicians had taken care of an ECMO patient at some point in their career (99% (157) vs. 84% (133)). In addition, a higher percentage of physicians currently take care of ECMO patients compared to VAD patients (95% (150) vs. 57% (90)).
More physicians had cared for a patient on ECMO than a VAD where the device was turned off because care was believed to be futile (93% vs. 35%, P < 0.0001). When asked if it can ever be ethically permissible to withdraw support from a patient with a VAD or on ECMO, nearly all of the respondents agreed (VAD 97%, ECMO 98%, P = 0.38). More respondents agreed that a patient or their family should agree to potential withdrawal of VAD or ECMO support prior to initiation if futility is later determined (VAD 58%, ECMO 56%, P = 0.39).
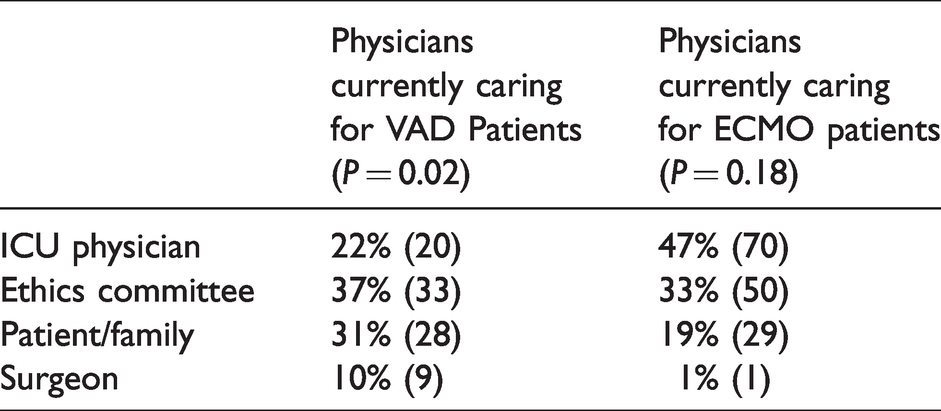
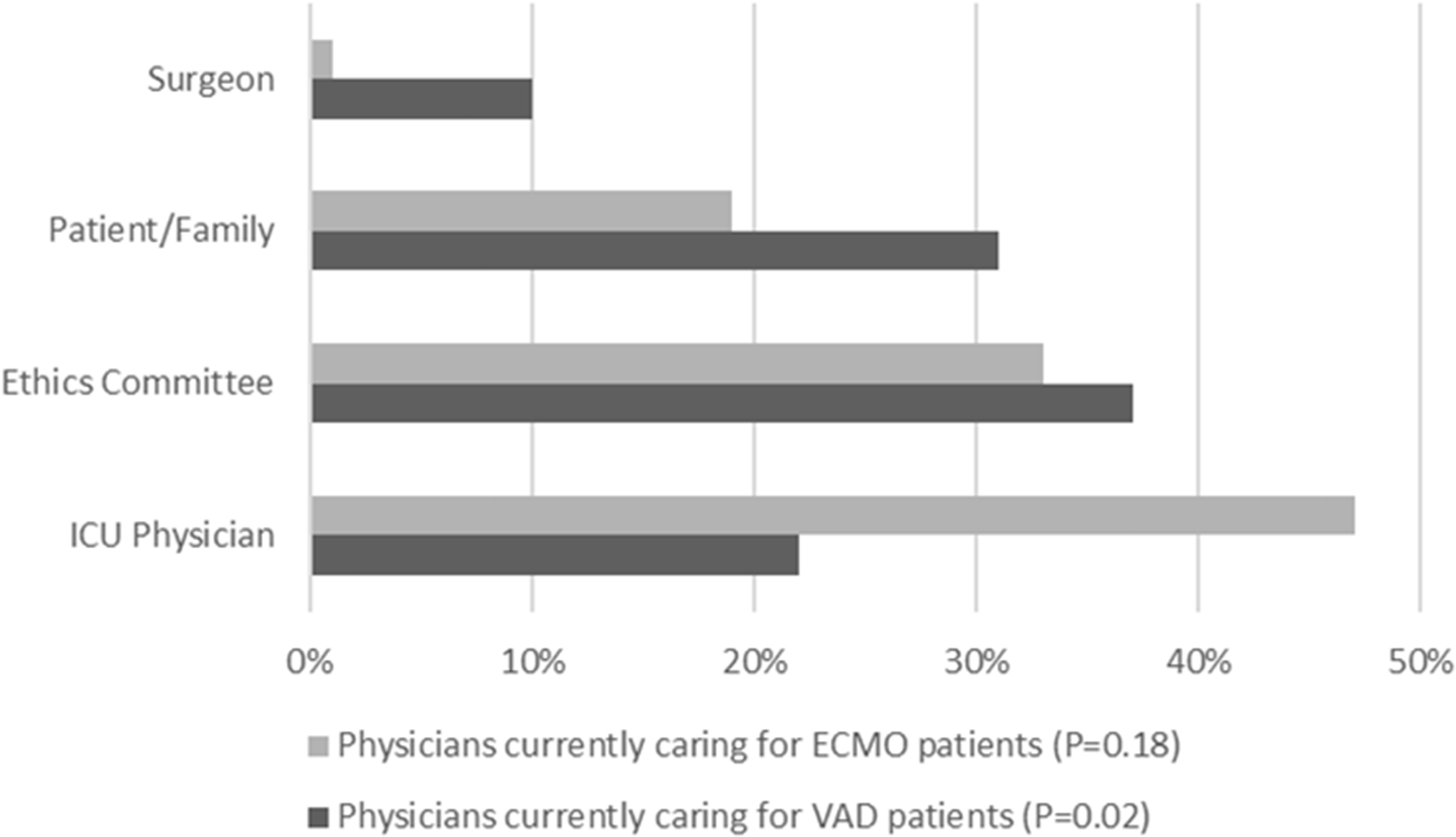
If a patient or their family disagrees with the removal of a VAD or ECMO in a case of medical futility, varied responses were seen when clinicians were asked who among the patient/family, the ICU physician, the surgeon or an ethics committee should ultimately make the decision to terminate support (Table 1). There was a significant difference among physicians who are currently taking care of VAD patients as to who should make the decision to terminate support in cases of futility (P = 0.02). There was no significant difference among physicians who are currently taking care of ECMO patients as to who should make the decision to terminate support in cases of futility (P = 0.18) (Figure 1).
Percentages of those respondents currently caring for VAD or ECMO patients who believe the ICU physician, an ethics committee, the patient/their family or the surgeon should make the decision to terminate support in cases of medical futility when the patient or their family disagrees with removal.
Percentages of those respondents currently caring for VAD or ECMO patients who believe the ICU physician, an ethics committee, the patient/their family or the surgeon should make the decision to terminate support in cases of medical futility when the patient or their family disagrees with removal.
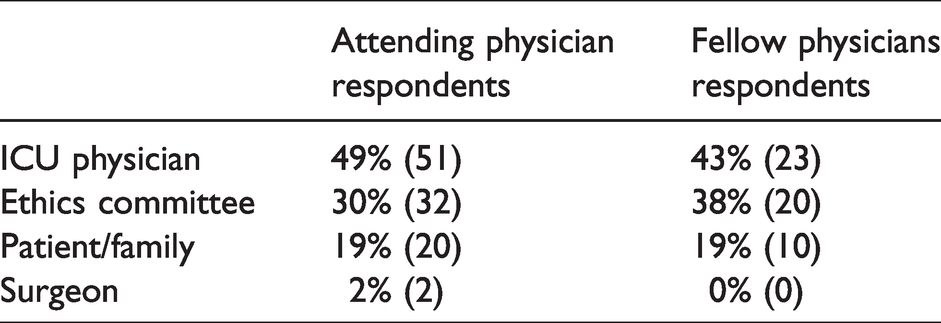
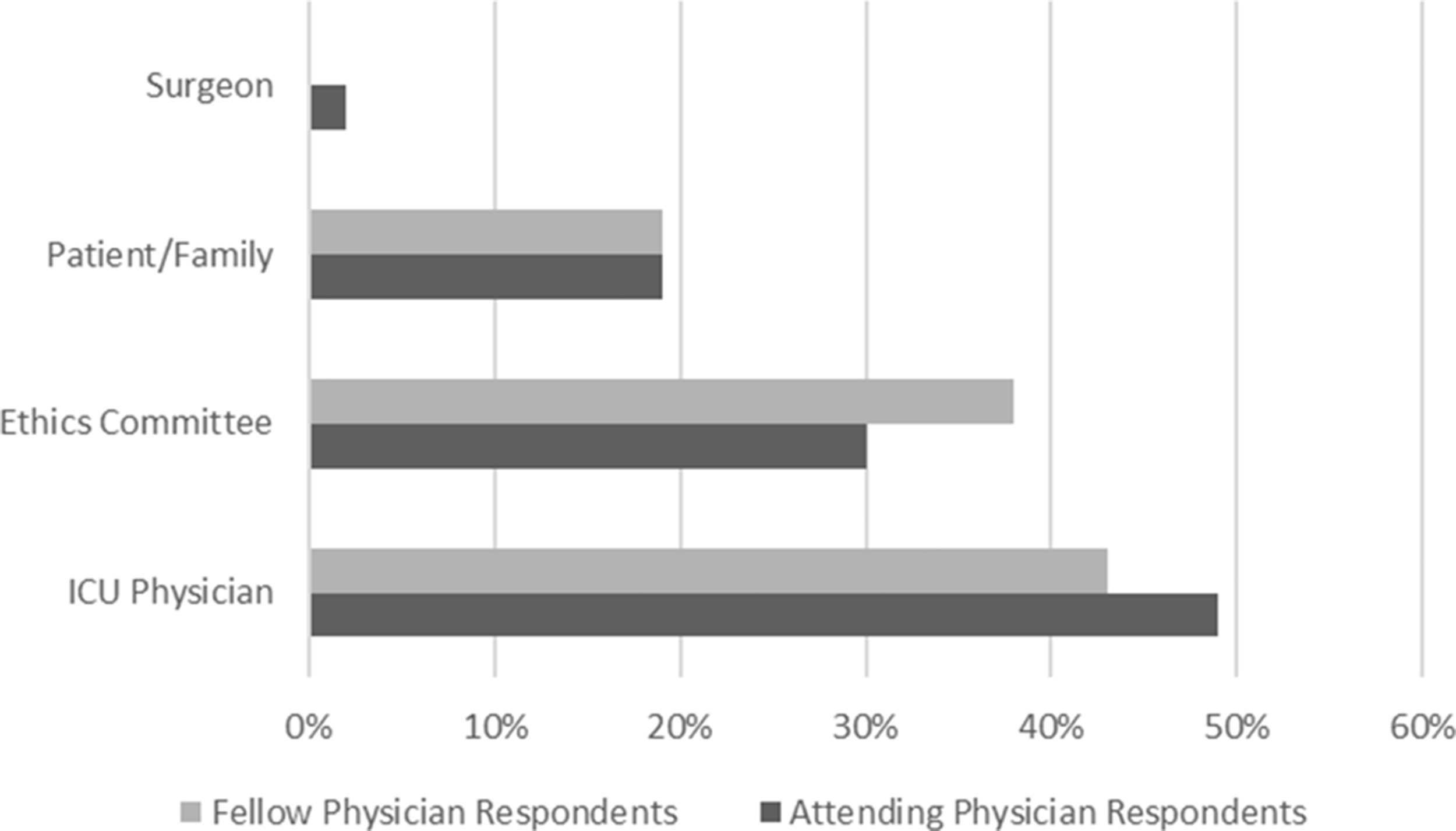
Differences between attending and fellow physicians were also examined. In cases where ECMO would be removed in cases of medical futility, more respondents felt that the ICU physician and/or the ethics committee (attending 79%, fellow 81%) should make the ultimate decision to terminate support versus the patient/family (attending 19%, fellow 19%) or the surgeon (attending 2%, fellow 0%) (P = 0.71) (Table 2) (Figure 2).
Percentages of attending and fellow physicians who believe the ICU physician, an ethics committee, the patient/their family or the surgeon should make the decision to terminate ECMO support in cases of medical futility when the patient or their family disagrees with removal.
Percentages of attending and fellow physicians who believe the ICU physician, an ethics committee, the patient/their family or the surgeon should make the decision to terminate ECMO support in cases of medical futility when the patient or their family disagrees with removal.
In cases where a VAD would be removed in cases of medical futility, more respondents felt that the ICU physician and/or the ethics committee (attending 65%, fellow 69%) should make the ultimate decision to terminate support versus the patient/family (attending 26%, fellow 28%) or the surgeon (attending 9%, fellow 4%) (P = 0.56) (Table 3) (Figure 3).
Percentages of attending and fellow physicians who believe the ICU physician, an ethics committee, the patient/their family or the surgeon should make the decision to terminate VAD support in cases of medical futility when the patient or their family disagrees with removal.
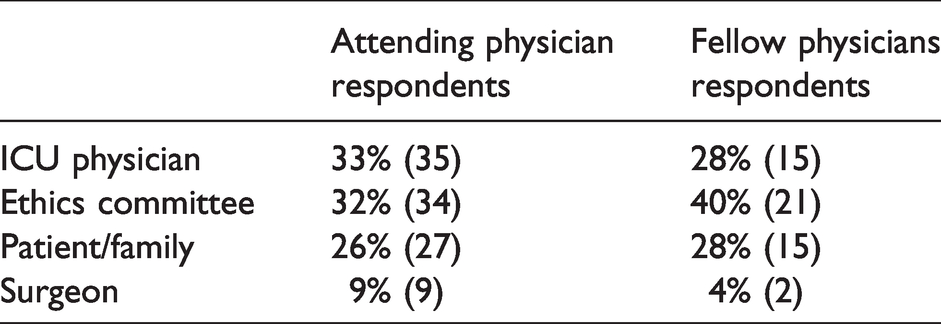
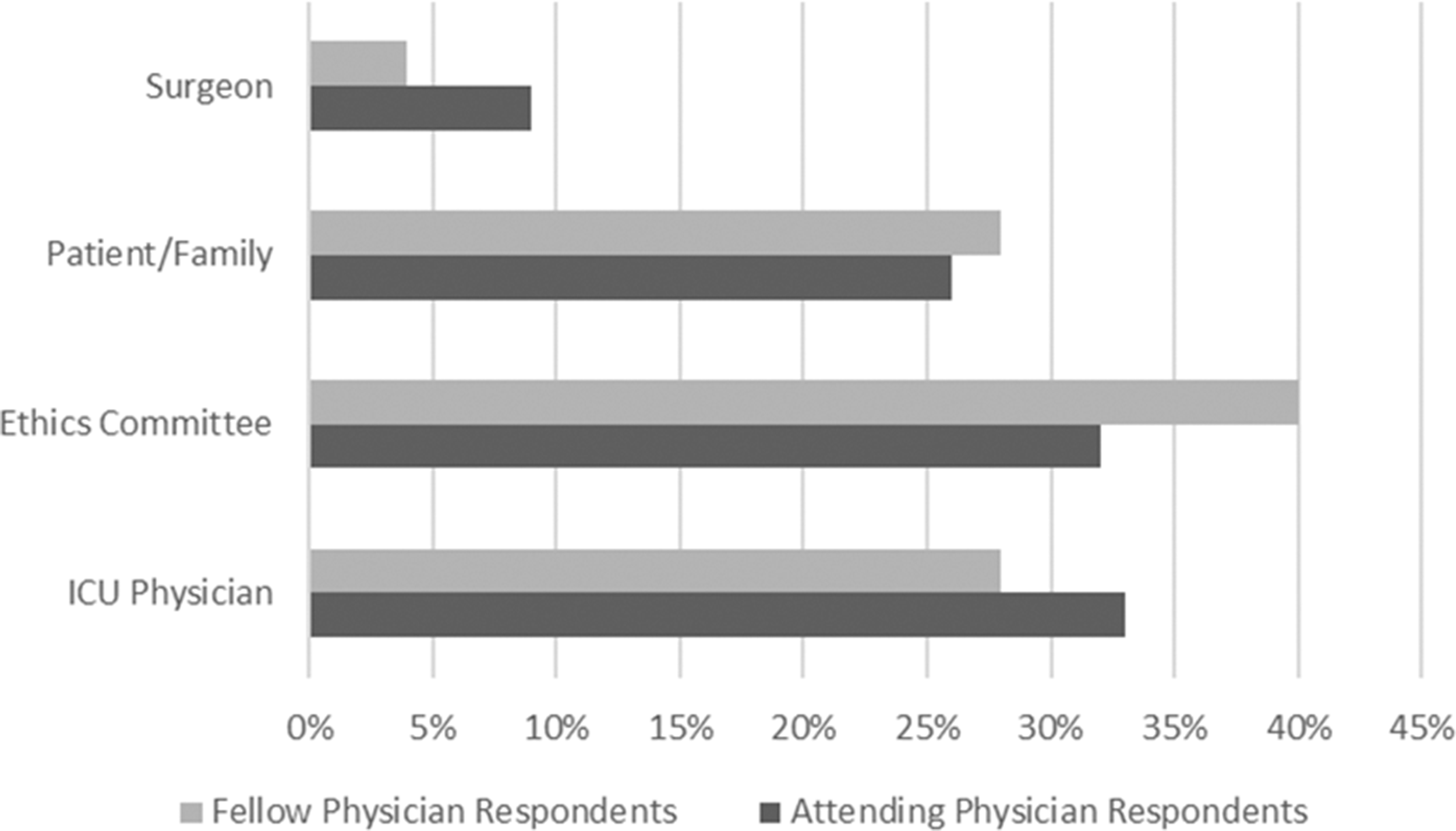
Percentages of attending and fellow physicians who believe the ICU physician, an ethics committee, the patient/their family or the surgeon should make the decision to terminate VAD support in cases of medical futility when the patient or their family disagrees with removal.
More respondents reported that a patient and/or their family should have to agree to withdrawal of ECMO prior to initiation if medical care is later found to be futile (attending 55%, fellow 62%, P = 0.4). A similar percentage agreed that a patient or their family should agree to potential withdrawal of VAD support prior to initiation if futility is later determined (attending 62%, fellow 57%, P = 0.52). More respondents reported that there should be protocols for withdrawal of ECMO (attending 72%, fellow 83%, P = 0.14) and VADs (attending 75%, fellow 81%, P = 0.4).
More respondents reported that withdrawal of a VAD is the same as withdrawal of ECMO (attending 59%, fellow 57%, P = 0.77). When asked if it can ever be ethically permissible to withdraw support from a patient with a VAD or ECMO, nearly all respondents agreed for a VAD (attending 96%, fellow 98%, P = 0.66) and for ECMO (attending 99%, fellow 98%, P = 1).
Lastly, more respondents agreed that protocols should be made for VAD and ECMO withdrawal (77% and 75%, kappa coefficient 0.86). Very few centers reported having protocols in place for VAD or ECMO withdrawal (3.2% vs. 14.6%). There was no clear consensus on whether the withdrawal of support from a patient with a VAD was the same as a patient on ECMO, with 58% of respondents reporting that withdrawal of support from both devices was the same.
Discussion
With greater use of ECMO and VAD support in the growing medically complex pediatric critical care population, critical care physicians are increasingly faced with cases of medical futility.12,15 In these situations, when there is disagreement among the medical team and the patient or their family, the decision to terminate ECMO and VAD support can become ethically challenging.16–18
To our knowledge, there are no consensus guidelines or evaluations of current attitudes among the pediatric critical care physician community regarding who should make the decision to terminate ECMO or VAD support in cases of medical futility. This study is the first to characterize current attitudes among pediatric critical care physicians and trainees across the United States.
Our study highlights that most of the surveyed attending and fellow physicians felt it can be ethically permissible to withdraw ECMO and VAD support in cases of medical futility. This agreement is an important first step in the process of developing consensus guidelines for the withdrawal of support. Additionally, our survey results indicate that protocols for withdrawal are desired but are rare in current practice. We speculate that the development of withdrawal protocols may increase as the number of complex pediatric critical care patients and familiarity with ECMO and VAD technology grows. Our study highlights, however, the need for such protocols given that there were varied responses about who should ultimately make the decision to terminate ECMO and/or VAD support in cases of medical futility. These findings can help shape protocol development by ensuring all clinical stakeholders, including critical care physicians, surgeons, cardiologists, perfusionists, nurses, nurse practitioners, chaplains, child life specialists, family volunteers and ethicists, as well as physical and occupational therapists, participate in their formation.
Our survey results also indicate that ECMO and VAD patients are viewed differently when futility is determined. Only 58% of respondents viewed the withdrawal of a VAD to be the same as the withdrawal of ECMO. We speculate this may be related to several clinical differences between ECMO and VAD patients observed in everyday clinical practice. For example, ECMO patients are generally less mobile and are unable to leave the hospital while on ECMO support, while VAD patients have the potential to be more mobile and even leave the ICU with a VAD in place. VAD patients may, therefore, be less sedated, more interactive and more participatory in their care and recovery. We speculate that these characteristics likely lead to the formation of stronger emotional bonds between healthcare providers and VAD patients. Healthcare providers are more likely to connect with these pediatric patients on a more personal level – observing their personalities, preferences and emotions. This humanistic element likely influences a healthcare provider’s ethical perception of the two support modalities. ECMO patients are more likely to be sedated and possibly medically paralyzed given the typical emergency nature of ECMO. This could lead to the perception that ECMO patients are sicker than VAD patients, perhaps leading to the attitude that ECMO withdrawal is more acceptable. Further examination of this speculation would require additional focused study.
When debate exists over withdrawal of support in cases of medical futility, physicians tended to respond that the ICU physician or an ethics committee should make the ultimate determination. In addition, fellow and attending physicians did not statistically differ in their responses to survey questions. While the reason for this is unclear, we speculate this could be due to several factors. First, the attending and fellow physicians questioned were likely from similar institutions where teaching regarding care of these patients would be modeled and discussed by attending physicians. Additionally, there is a smaller cohort of physicians across the country taking care of patients on ECMO and VAD support versus those who are not. With collaboration and conferences, ideas regarding management are likely to be shared and, therefore, be similar among physicians caring for this patient population in their current practice.
We did not examine United States case law, if such exists, pertaining to ECMO and VAD withdrawal, as this was beyond the scope of this study and our expertise. Although an ethics committee may support a provider’s decision to terminate ECMO or VAD support for an individual patient, we speculate that a court could impose an injunction at the request of the family, thereby preventing, at least temporarily, such a withdrawal. Additional options could include offering the family a second opinion from another ECMO or VAD center as well as transferring care to another center if one was willing to accept the patient.
Lastly, we also found that more respondents agreed that a patient or their family should agree to withdrawal of ECMO and/or VAD support prior to initiation if medical futility is later determined. This general consensus that patients or their families should have to agree to potential withdrawal of support at the onset of care with a VAD or ECMO highlights the anticipated ethical difficulty that clinicians, patients and their families may face during the course of treatment. Such a preemptive agreement strategy is, however, flawed and unenforceable as clinical thought is not enforceable. The findings would appear to point to the need for consensus guidelines with mechanisms included to deal with differences of opinion over time.
Our survey has a number of strengths. To our knowledge, we are the first to define current attitudes among a large cohort of pediatric critical care attending physicians and fellow physicians in the United States regarding the termination of ECMO and VAD support in cases of medical futility. Our survey was able to elucidate opinions from pediatric critical care attendings and trainees from across the United States and with varying levels of experience that will be useful for the creation of future studies as well as consensus guidelines.
There were limitations to our study. Given the relatively small number of pediatric critical care attending and fellow physicians widely dispersed across the United States, we sought numerous routes to reach as many potential participants as possible. We kept the survey anonymous to encourage participation. Given that we employed advertising in a newsletter as well as through a website, we cannot calculate the total number of invited participants. As a result, we recognize that the inability to determine the number of possible respondents in order to calculate a response rate is a significant limitation of our study. Additionally, as we used de-identified data, we could not group responses based on a respondent’s center, including whether the center had a pediatric cardiac ICU or whether the respondent was a cardiac critical care attending physician or practiced in a pediatric cardiac ICU. This may have provided more insight into different practices at different centers across the country, especially those who may be cardiac intensivists. The anonymous nature of our survey, however, likely helped to improve survey completion should a respondent, from an already small pediatric critical care and transplant community, be hesitant to complete the survey due to identifying their center and opining on a sensitive topic such as withdrawal of support. Furthermore, to help with determining whether our sample size was broad and representative of United States’ providers, we did characterize responses based on the region of the country the respondents were practicing in. We believe these results show that our cohort of respondents are representative of practicing pediatric critical care physicians throughout the United States. Since we analyzed physicians who may have participated in the selection of certain candidates for ECMO or VAD support in their practice, and ECMO and VAD support was likely not offered to all patients, these factors may have affected a respondent’s ethical views, and they may have been more invested in their patient’s care and outcome. Additionally, care possibilities and outcomes evolve over time and by hospital/region. Lastly, the multidisciplinary team required to care for these complex patients is large. We recognize that the opinion of other allied professions, such as nursing, perfusion, physical therapy, occupational therapy and child life, should be investigated. The absence of this analysis is a limitation of our study. Such a study, although beyond the scope of our aim, is nonetheless vital to investigating the full ethical landscape involved in the care of these patients.
Conclusion
From our data, we are able to conclude that while most pediatric critical care physicians felt that it can be ethically permissible to withdraw both ECMO and VAD support in cases of medical futility, varied opinions exist as to who should ultimately make this decision when the patient or their family disagrees with the medical team. Our study indicates that pediatric ECMO and VAD withdrawal protocols are desired but are rare, and further investigation is needed to determine how to best design guidelines that would incorporate multiple stakeholders. Given our experience in treating these patients in a large pediatric heart transplantation center, we recommend that these stakeholders include critical care physicians, surgeons, cardiologists, perfusionists, nurses, nurse practitioners, chaplains, child life specialists, family volunteers and ethicists, as well as physical and occupational therapists. Such a protocol would need to involve each of these stakeholders, as each member is vitally important to the multidisciplinary care of these complex patients. Future studies should be done to investigate the emotional aspect and the perspective of each of these stakeholders regarding withdrawal of ECMO or VAD support in cases of medical futility.
Supplemental Material
sj-pdf-1-cet-10.1177_14777509211001560 - Supplemental material for Opinions among pediatric critical care physicians regarding the ethics of withdrawal of ventricular assist devices and extracorporeal membrane oxygenation
Supplemental material, sj-pdf-1-cet-10.1177_14777509211001560 for Opinions among pediatric critical care physicians regarding the ethics of withdrawal of ventricular assist devices and extracorporeal membrane oxygenation by Antonia A Melas, Leanna L Huard, Rong Guo and Robert B Kelly in Clinical Ethics
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical considerations
This study was approved by the UCLA Institutional Review Board. A waiver of informed consent was obtained. Participation in the survey was voluntary.
Funding
The author(s) disclose receipt of the following financial support for their statistical analysis: NIH National Center for Advancing Translational Sciences – UCLA CTSI Grant Number ULITR001881.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.