
Abstract
The administration of pro re nata medications is the responsibility of the nurse. However, ethical uncertainties often happen due to the inability of incapacitated patients to collaborate with the nurse in the process of decision making for pro re nata medication administration. There is a lack of integrative knowledge and insufficient understanding regarding ethical considerations surrounding the administration of pro re nata medications to incapacitated patients. Therefore, they have been discussed in this paper and practical strategies to avoid unethical practices have been suggested. The complicated caring situation surrounding the administration of pro re nata medications is intertwined with ethical issues affecting the consideration of the patient's wishes and interventions that override them. The patient's right of autonomy and treatment refusal, surrogacy role, paternalism, and coercion are the main ethos of ethical pro re nata medication administration. Education and training can help nurses avoid legal and ethical issues in pro re nata medicines management and improve the quality and safety of healthcare. Empirical research is needed to improve our understanding of this phenomenon in the multidisciplinary environment of medicines management.
Introduction
A medication error is defined as ‘an avoidable adverse effect of healthcare, whether or not it is obvious or harmful to the patient something incorrectly done through ignorance or inadvertence; a mistake, e.g. miscalculation, judgment, speech, writing, action, or a failure to complete a planned action as intended, or the use of an incorrect plan of action to achieve a given aim’ (p. 6013). 1 Medication administration error is a high-risk situation during medicines management and with a median of 8.0% is the primary cause of medication harm. It is characterised by errors in the timing, omitted, and wrong doses of medication in various healthcare conditions and age groups.2,3 A multicentre study in 38 hospitals in the UK on the prevalence, nature, and predictors of medication administration omissions using the MedsST tool indicated that medication administration omission was frequent and was influenced by the number of administered medications to patients. 4 Therefore, the safety of medication administration is one of the most important initiatives for the improvement of patient safety in the healthcare system. The World Health Organization (WHO) has estimated that the global cost of medication errors would be 42 billion USD annually 5 and the Third Global Patient Safety Challenge on ‘Medication without harm’ has discussed issues and strategies to reduce harm associated with the medication process in high-risk healthcare situations.5,6
The application of multidisciplinary and collaborative strategies by physicians, pharmacists and nurses can enhance the safety of medicines management. 7 In this respect, the administration of medications is the primary role of nurses with an undeniable impact on patient safety.8,9 Nurses are trained and authorised to prepare medications, calculate doses, administer and monitor medications’ side effects and adverse drug reactions.10–12 Safe administration of medications requires nurses to use their theoretical knowledge and clinical skills during the medication process.13,14 The ‘rights of medication administration’ as patient, drug, route, dose, time, documentation and reason have been recognised as traditionally important tools in the hands of nurses to ensure the safety of medication administration. 15
Pro re nata medication administration by the nurse
‘Pro re nata’ (PRN) medication administration is a main responsibility of nurses and has been described as the administration of medications based on the patient's immediate need instead of administration at predetermined times.16,17 After the prescription of PRN medications by the physician, the nurse makes a collaborative decision with participation of the patient regarding medication administration.17,18 PRN medicines management has been recognised by international healthcare associations as an appropriate method for the management of physical and psychological suffering among patients with acute and chronic healthcare conditions.19–21
Prescription and administration of PRN medications have become the main part of medicines management in various healthcare settings. For instance, 90% of patients with mental and psychiatric health conditions and 20–86% of residents in nursing homes are prescribed at least one PRN medication.22–24 The exact number of medication errors due to PRN medication administration has not been reported in the international literature. PRN medication errors are characterised by not mentioning the reason behind medication administration and ambiguities in steps taken to manage the administration process, as well as to monitor their effects and side effects after administration.25,26 Coercion in the administration, 27 and over-administration of PRN medications, when medication is not the first choice for treatment18,28 are quite common. Inappropriate use of PRN medications is associated with polypharmacy and longer stays in nursing homes with a median of 2.1 years. 29
The safety of medicines management is intertwined with ethical nursing practice.30,31 Nurses are professionally obliged to administer medications in a manner that is consistent with ethical codes for practice as ‘do the good and right thing for patients’, prevent harm, and evaluate the probable outcomes of medication administration interventions.32–34 Insufficient knowledge of ethical considerations influencing all types of medication administration including PRN medications has become the source of moral distress in nurses, 35 their burn-out and job turnover. 36
Decision making for care by incapacitated patients
Temporary or permanent physical and psychological incapacity during each person's life is common. Over one billion people, that is about 15% of the world population, live with some form of disability and incapacity and an increasing trend is captured in this figure. 37 Incapacitated patients often suffer from severe mental or physical conditions to the extent that they have no sufficient understanding required for making or communicating responsible healthcare decisions.38,39 With the capacity to make decisions, the patient should have the ability to understand the meaning of the information provided by healthcare staff, can connect them to their healthcare situation, use the information to decide, and communicate their choice and preferences regarding therapeutic measures.40,41
Incapacitated patients can be older people and mentally ill that have been described as highly vulnerable patients in the healthcare literature. 42 They sometimes have no friends or family to make medical decisions as default surrogates. 43
According to the Convention on the Rights of Persons with Disabilities by the United Nations, patients with any sort of disability and incapacity have the right to benefit from appropriate decisions made on their lives. 44 Making appropriate decisions with regard to healthcare and therapeutic measures influence the patient's wellbeing. If the patient has no capacity to make decisions, family members and healthcare providers can be authorised to make decisions on their behalf. 45
Decision making for incapacitated patients who cannot make decisions for themselves is considered a common concern for healthcare providers and is often intertwined with ethical issues, 46 given that the patient's informed consent is a prerequisite for all types of healthcare interventions. Nevertheless, interventions that are in the interest of such incapacitated patients and when the interventions are accompanied with a minimum risk and burden are exempt from this rule. 47 Having no capacity to decide imposes high levels of care burden on healthcare providers especially when medications are prescribed and administered, and in case that patient refuses to undertake healthcare procedures.48–50 This situation is also accompanied by various ethical complexities affecting the society and healthcare staff individually.51,52
PRN medicines management for incapacitated patients
PRN medicines management generally is the process of creating a mutual understanding and the feeling of responsibility between the nurse and the patient in order to choose the most effective medication with the lowest possibility of side effects and adverse drug reactions.14,17 However, the requirements for making bilateral decisions by the nurse and the patient may not be achieved given the patient's incapacity to understand and actively take part in the medication process as a member of the healthcare team.53–55 This situation creates barriers to ethical decision making by clinical nurses and can be the ground for the development of ethical dilemmas.
Given the lack of integrative knowledge and insufficient understanding of ethical challenges surrounding the administration of PRN medications to incapacitated patients, the question is: How nurses can avoid unethical practice in PRN medicines management for these patients?
Ethics of administration of PRN medications to incapacitated patients
The nurse is obliged to play the role of the patient's advocate and put the patient's individual preferences and wishes at the centre for making the decision to administer PRN medications. However, in some situations, the healthcare professional's wishes override those of the patients to benefit the patient and prevent harm. The ethical problem is raised in the preservation of the right to accept or refuse receiving medications given the patient's right of autonomy. Respect for the patient's autonomy requires to recognise his/her right to decide about own treatment and to refuse receiving treatment in case that the patient understands the action and is not forced to comply with the action.56–58
Complying with the patient's wishes
Some patients such as nonverbal trauma patients or those with severe mental and cognitive impairments may have no or very limited decision-making capacity. Therefore, they may be unable to understand the reason for PRN medication administration and collaborate in the related process. Therefore, being the patient's representative or taking the surrogacy role to predict therapeutic needs for such incapacitated patients is needed. A suggested solution is the involvement of patients’ families for the prediction of their preferences during periods of incapacity and to receive treatments that comply with their own needs and wishes.59,60 Family members are appropriate sources to find the most suitable treatment and care modality, 61 because they can better guess the patient's preferences in similar circumstances and how their needs can be met. 62 Family members also can play the role of the patient's surrogate and the essential partner for making decisions on the patient's behalf and can share the responsibility of decision making with nurses. This approach to decision making can prevent moral and emotional distress in clinical nurses and enhance trust and consensus between healthcare professionals and family members. 63
Making decisions to perform any sort of medical interventions including the administration of PRN medications to incapacitated patients who have no family members to take the surrogate role is also complicated and is filled with ambiguities. 64 Therefore, obtaining consent to start the medical procedure for these patients is intertwined with ethical issues and the patient's right problem. 43 If it is not resolved by the healthcare team, an ethical dilemma may occur given its impact on the patient's care outcome. 65 As if it is not a perfect solution, the use of clinical guidelines and a three-step approach of the physician, ethics committee, and guardian have been suggested. 64 The essential legislative core for all European member states to guarantee the protection of human rights regarding biology, medicine and healthcare is the ‘Convention for the Protection of Human Rights and Dignity of the Human Being about the Application of Biology and Medicine’ 66 and its additional protocol. 67 This legislative document recommended that ‘Where, according to law, an adult does not have the capacity to consent to an intervention because of a mental disability, a disease or for similar reasons, the intervention may only be carried out with the authorisation of his or her representative or an authority or a person or body provided for by law’. 66
Nevertheless, ethical issues remain unresolved even if healthcare professionals including the nurse take the surrogate role as they need to identify to which extent therapeutic interventions for patient care can be performed. 68 The nurse is obliged to collect all types of data from the patient including verbal and nonverbal clues as well as consider vital signs and symptoms to find how he/she can meet the patients’ physical and psychological needs before making the decision on the administration of PRN medications. 69 The patient's behaviours should be observed and interpreted to decide about the need to the involuntary administration of PRN medications to incapacitated patients. However, this could be a challenge to go beyond reported symptoms and understand their meanings in order to provide individualised care. 70 In this respect, the nurse's personal attitudes, beliefs and knowledge regarding symptoms and behavioural clues indicating the need for medication can influence his/her decision to administer medications to a great extent. 71
Overriding the patients’ wishes
A source of moral concerns is to take a paternalistic role and coerce the patient to take PRN medications while the agitated patient is unwilling to cooperate and resist taking medications.72–74 Beauchamp and Childress 56 define paternalism as ‘the intentional overriding of one person's known preferences or actions by another person, where the person who overrides justifies the action by the goal of benefitting or avoiding harm to the person whose preferences or actions are overridden’ (p. 178). 56 Paternalism is the sharp end of professional beneficence 75 and has been suggested to be considered when the patient is severely incapacitated and when treatment is in the patient's best interest 76 However, it is contradictory to the value of autonomy and is a source of tension between restraint and freedom, even if it may accompany by good intentions in patient care. 77 The nurse's effort to pursue the patient's autonomy as an end state reflects the value given by him/her to paternalism. He/she may act paternalistically based on the assumption that his/her actions may allow the patient to have a more autonomous life in the future. 78
It is noted that even if physical force is not applied by the nurse, the persuasion of patients to take medications limits the patient's autonomy. 79 In such situations, the use of informal coercion as an ‘unpleasant good’ can be considered if it is one part of the nurse's job description, despite inducing negative feelings in the patient and discomfort in the nurse.80–82 Although it may create a feeling of safety in the patient, it is also associated with some negative consequences including the feeling of fear and disempowerment in the nurse. The nurse has the responsibility to protect the human rights of patients, and he/she should be aware of situations in which informal coercion is used and what its potential adverse psychological effects can be on therapeutic relationships.76,83
As a matter of self-determination, disabled and incapacitated patients may decline invasive procedures for medication administration compared to less invasive ones such as the oral route. 84 Therefore, there are some clinical situations in which covert medication administration has been suggested for those incapacitated patients who refuse taking medications but indicate a high risk of self-harm. 85 Nevertheless, complex clinical and ethical issues appear when covert medication administration is used, 86 as it can damage the relationship between the patient and the family member, with the nurse.
Patients have the right to refuse medications unless there is a court order obligating them to take the medication or in emergency situations and only for a limited duration. This is a change from previous practices in which those patients who have been involuntarily hospitalised does not have decision-making capacity and are considered unable to refuse any kind of medication. In this difficult ethical situation, the nurse should face the problem of balancing their own level of control over decision making with the preferences of incapacitated patients. 87 Therefore, the nurse has the responsibility to assess the situation objectively and document the medication process to avoid forthcoming legal and ethical issues.81,88
An argument in favour of paternalism emphasises the utilitarian principle in which decisions for the administration of PRN medications may be taken because of the control of patients’ behaviour to benefit other people than the patient him/herself. Roberts 89 affirms that in case of illnesses leading to severe incapacity, paternalism will be exercised by the means of interventions aiming at the alleviation of human suffering for those afflicted with that illness. From an opposing perspective, the negative consequences of forced and involuntary administration of medication may include further detachment from therapeutic measures that can lead to a violent outbreak requiring the use of restraints and seclusion90,91 to gain control over the patient's threatening behaviours.
How the nurse responds to an ethical situation is influenced by his/her understanding of the illness. If mental illness is considered a ‘bodily disease’, medications will be seen as beneficial for avoiding human suffering. On the other hand, if the mental illness is understood as a deviation from the culture's values and norms, a paternalistic medical intervention becomes a political act rather than a caring one. 89
Paternalistic culture-bound preferences should not affect patient care. Each patient must be approached impartially addressing their needs, values and beliefs. Ethical principles and the requirement for best available care apply regardless of the ethnic, cultural and religious background, even if the patient is incapacitated. A summary of key ethical factors surrounding PRN medication administration to incapacitated patients has been presented in Figure 1.
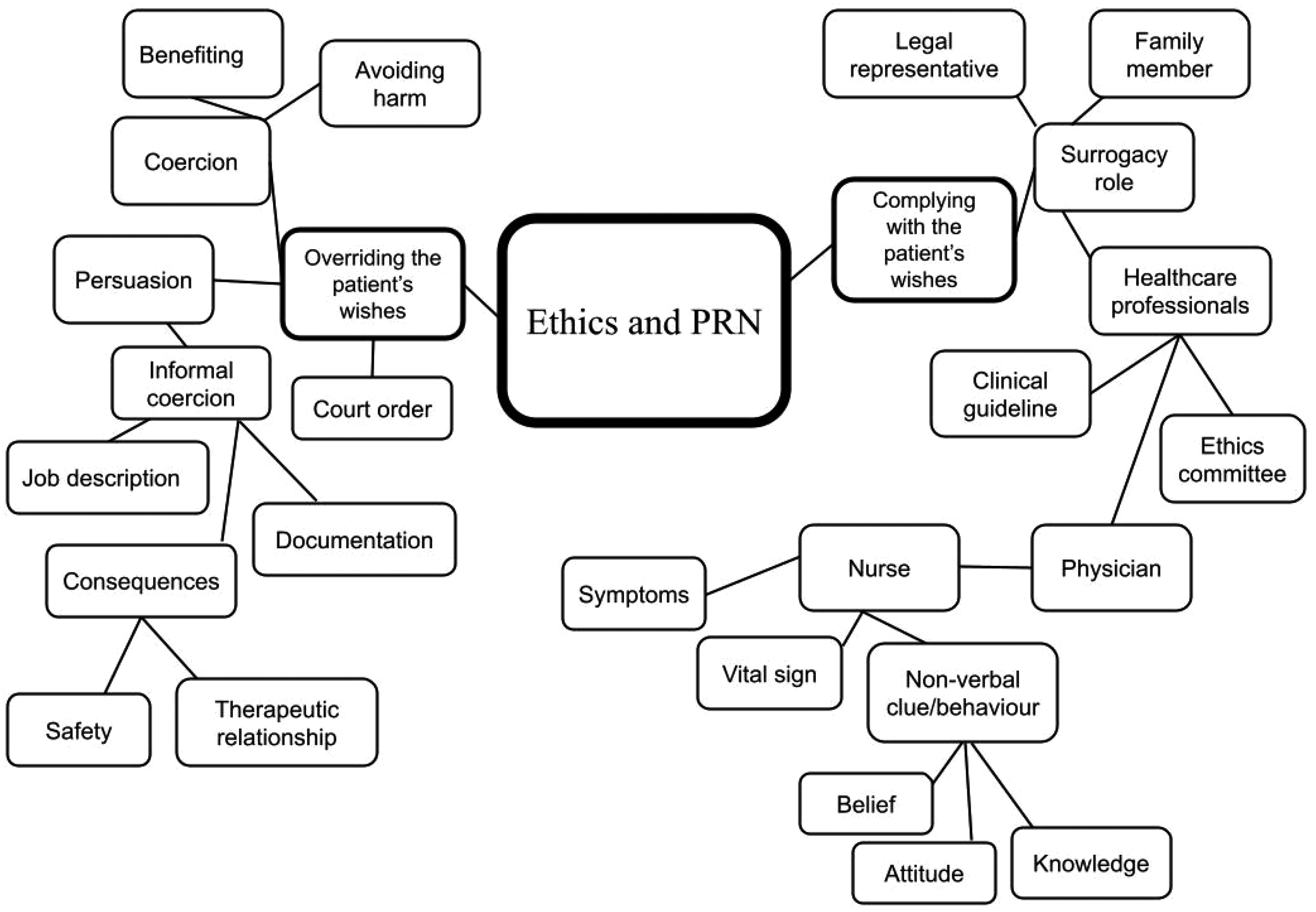
Ethical factors affecting pro re nata (PRN) medication administration to incapacitated patients.
Implications for clinical practice
Nurses have the required knowledge and clinical expertise to help with relieving physical and psychological suffering among patients, 92 and the administration of PRN medications allows nurses to become more actively involved in medicines management initiatives in the multidisciplinary environment of healthcare. 93 The requirement for the safe administration of PRN medications by nurses to incapacitated patients is to comply with regulatory, professional, ethical and legal frameworks that govern it to establish a caring environment in which the human rights, dignity, values, custom and spiritual beliefs of the patients are all respected. 94
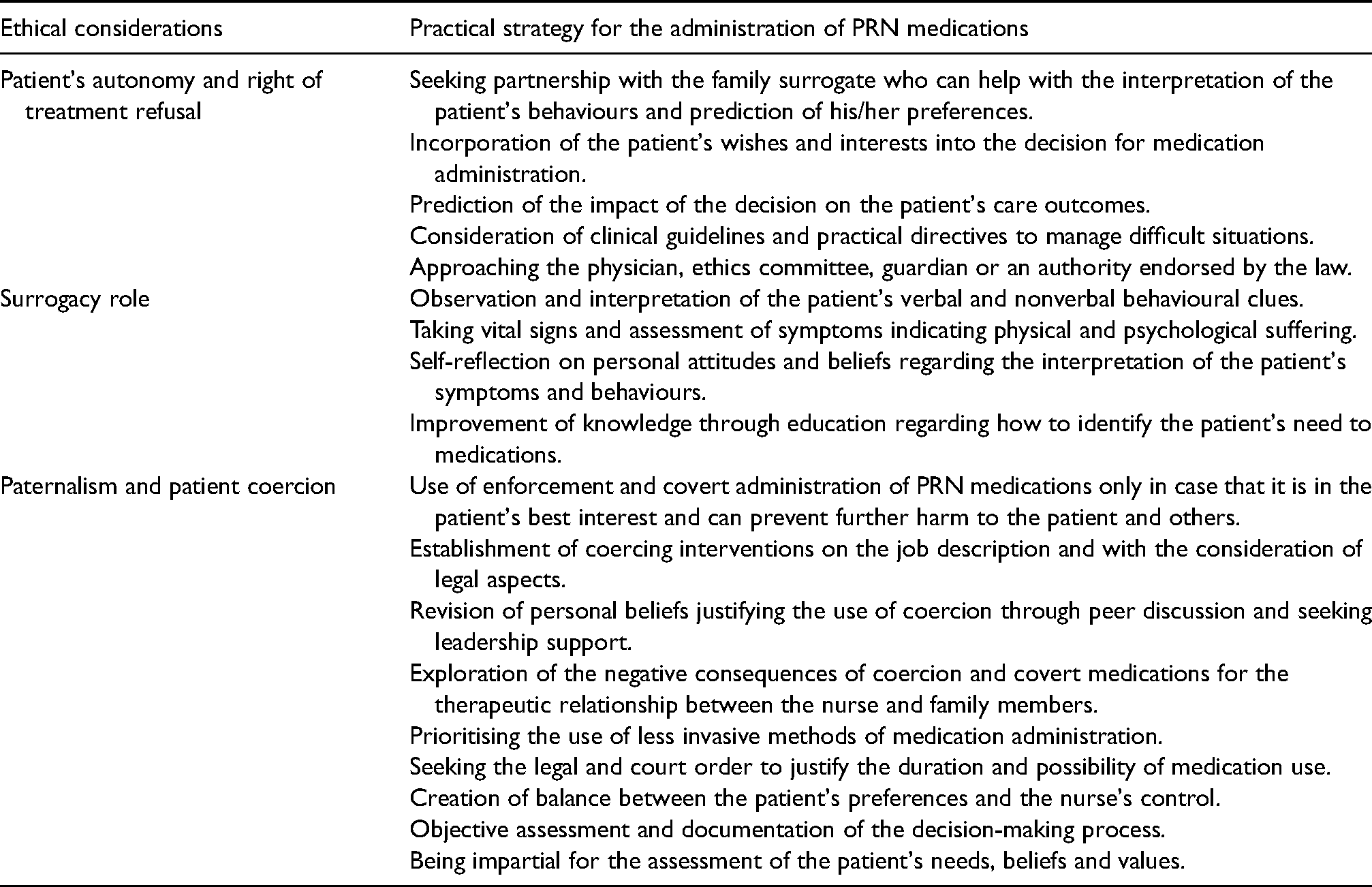
A summary of ethical considerations of the administration of PRN medications to incapacitated patients and clinical strategies to avoid unethical practice by the nurse has been presented (Table 1).
Pro re nata (PRN) medication administration to incapacitated patients and strategies to avoid unethical practice.
Conclusion
The administration of PRN medications to incapacitated patients creates a complicated caring situation for the nurse and is intertwined with ethical issues affecting the consideration of the patient's wishes and interventions that override them. The patient's right of autonomy and treatment refusal, surrogacy role, paternalism, and coercion are the main ethos of ethical PRN medication administration. Education and training can help nurses avoid legal and ethical issues in PRN medicines management and improve the quality and safety of healthcare.
The improvement of nurses’ knowledge and attitudes regarding the ethical considerations of PRN medication administration and their application to clinical practice requires discussion and reflection by nurses, multidisciplinary collaboration, and leadership support. Healthcare organisations can heed such an exchange of ideas by introducing supervision or more informal discussion rounds.
It is also suggested to incorporate these ethical aspects into clinical guidelines and directives for the safe administration of PRN medications to incapacitated patients. Also, extra efforts should be made by the nurse to evaluate the effectiveness of medication and the possibility of harm, as well as to detect the possible side effects of medications and adverse drug reactions, given the inability of incapacitated patients to report them.
Empirical research is needed to explore more the interconnection between the administration of PRN medications and ethics in the multidisciplinary environment. Also, there is a need to conduct experimental studies to investigate how the ethical aspects and principles of PRN medicines management can improve the quality and safety of healthcare.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.