
Abstract
Ethical clinical practice requires cultural competency. In the United States, Hispanics report stronger attitudinal barriers to drug abuse treatment than any other racial/ethnic group. Hispanics report feeling that drug abuse treatment providers do not understand their unique cultural needs and are unfamiliar with their experiences of discrimination and immigration. Using this case study to explore broader ethical and policy issues, this study investigates the extent to which US universities train counselors to address the culturally specific needs of Hispanic patients and how this is reflected in practice in Los Angeles County. Based on a content analysis of the required courses, syllabi, and course descriptions at 30 universities related to culture/race/racism/ethnicity/diversity at the undergraduate and graduate levels on the addiction therapist track, and thematic analysis of eight in-depth interviews with counselors working in outpatient rehabilitation centers in Los Angeles, I argue that cultural competency education for drug abuse counselors is too surface level and infrequent to adequately prepare students for a career in addiction counseling for Hispanic clients. Significant changes must be made to how cultural diversity is valued and prioritized in the field of psychology to provide better care for Hispanic people with a substance use disorder and fulfill the moral obligation to eliminate this health disparity. Although this study focuses on counselors in Los Angeles, these findings are relevant for professionals and healthcare systems across the United States and beyond who seek to provide equitable and effective care for Hispanic patients.
Keywords
Introduction
The need for cultural competency is increasingly recognized within clinical ethics. As a case study, this article focuses on the needs of the Hispanic population in the United States in relation to drug abuse treatment. As of 2020, there are approximately 62.1 million Hispanic/Latino a people in the United States, just over 19% of the total population. 1 With 15% of families living at or below the poverty level, 2 facing immigration stress, and discrimination, Latinos are a particularly vulnerable group for addiction and substance use disorders (SUD). 3 In fact, the 2018 National Survey on Drug Use and Health (NSDUH) from the Substance Abuse and Mental Health Services Administration (SAMHSA) estimates that 1.1 million Hispanic youth engaged in illicit drug abuse that year. 4 Over 17% of Hispanic adults suffer from mental illness, which is linked to increased drug abuse. Because the current opioid and fentanyl crisis in California disproportionately affects Latinos, with fentanyl-related deaths doubling among Latinos in the past year, effective SUD treatment for Latinos is more important than ever. 5 Alarmingly, only 3–7% of Latinos with a substance use disorder seek treatment from a specialty facility, at about half the rate as their white counterparts. 6 Various studies show that Latinos are the least likely to use specialty SUD treatment programs compared to other racial/ethnic groups. 7 This has led to recent efforts in research to identify and resolve barriers to seeking SUD treatment among Latinos.
Apart from the extensively researched socioeconomic and linguistic barriers, Latinos also report attitudinal barriers to specialty drug abuse treatment more than any other racial/ethnic group. 5 These include cultural barriers such as machismo, familismo, personalismo, fatalismo, and social stigma, concepts that will be discussed herein. 6 Latinos also report feeling that drug abuse treatment providers do not understand their unique cultural needs and are unfamiliar with their experiences of discrimination and immigration. 7 This assumption that counselors do not understand Hispanic cultural issues is a major attitudinal barrier to seeking treatment.
Existing literature on Hispanic cultural barriers to SUD treatment point to enhancing cultural competency among counselors to improve treatment engagement and outcomes. 8 While much of the existing literature stresses the importance of addressing Hispanic patients’ b cultural concerns in treatment, there is no research on how practitioners are trained in cultural competency/sensitivity. The purpose of this study is to fill this gap and identify areas of strength, weakness, and potential for improvement.
Analyzing how counselors are prepared to handle Hispanic cultural factors in drug abuse treatment is important because it can identify a potential health inequity and help improve treatment outcomes by encouraging more targeted, culturally sensitive treatment. This study focuses on substance abuse rehabilitation centers in Los Angeles County because of its large Hispanic population (49.1% Hispanic/Latino compared to 18.9% nationally). 9 The guiding research questions are: (i) to what extent does the training in US universities prepare counselors for the culturally specific needs of Hispanic patients with an SUD and (ii) how is this reflected in practice in Los Angeles county? Based on a content analysis of the required courses, syllabi, and course descriptions at 30 universities related to culture/race/racism/ethnicity/diversity at the undergraduate and graduate level on the addiction therapist track, and thematic analysis of eight in-depth interviews with counselors working in outpatient rehabilitation centers in Los Angeles, I argue that cultural competency education for drug abuse counselors is too surface level and infrequent to adequately prepare students for a career in addiction counseling for Hispanic clients. Significant changes must be made to how cultural diversity is valued and prioritized in the field of Psychology to provide better care for Hispanic people with a substance use disorder and fulfill the moral obligation to eliminate this health disparity.
Background on risk factors for addiction: Migration, acculturation, and discrimination
Key studies on the intersection of migration, health, and addiction explain why Latinos are a particularly vulnerable group to addiction and substance use disorders. Factors including unemployment, limited access to education, living in disadvantaged communities, family conflict, and racial and income discrimination are common stressors that contribute to depression and anxiety disorders. 10 One 2011 ethnographic study assessing drug use among Latino migrant laborers observed that many migrants use alcohol and drugs to cope with strenuous working conditions and long-term separation from their families. 11 Prevalence rates of drug use among Latino migrant laborers are as high as 80% for binge-drinking, 39% for alcohol dependence, and 25% for methamphetamine or cocaine use. 12 Hispanic immigrants are also vulnerable to ataques de nervios or “nerve attacks” that stem from stressful life experiences, family crises, the disruption of migration, losses, and abandonment. 13
Adverse Childhood Experiences (ACEs) also play a significant role in substance use disorders among Latinos. Childhood adversity is a well-established risk factor for substance abuse and other mental health issues during adolescence and adulthood. Latinos face significantly more ACEs than their white counterparts, stemming from poverty, discrimination, and immigration-related traumas. 14 After controlling for cultural variables including ethnic identity and acculturation, ACEs are uniquely associated with higher substance abuse among Latino youth. 15
Acculturation is also a significant risk factor for substance use disorders among Latinos in the United States, especially among adolescents and young adults. Acculturation—the assimilation to a dominant culture and loss of the heritage culture––is directly related to drug use: Hispanic adolescents higher in acculturation are more likely to use drugs than those more in touch with their family's culture. 16 This supports the “acculturation gap hypothesis,” the idea that Hispanic parents and children assimilate at different rates; such discrepancies create family conflict that leads to difficulties in children's psychological adjustment, anxiety, and depression. 17
Studies on acculturation gaps among Mexican-American adolescents observed that acculturation dissonance was associated with delinquent behavior, alcohol, and tobacco use. 18 These findings are consistent with several nationally representative surveys of over 1200 Mexican-American immigrants in the United States from 2001 to 2003: Mexican-born immigrants were at a lower risk for drug disorders than US-born Mexican-Americans, who exhibited higher levels of acculturation. 19 Likewise, a 2019 nationally representative survey of 641 adult Latinos from 6 regional groups established cultural resilience as a protective factor for depression and substance abuse. 20 Overall, research indicates that Latinos are more likely to develop a substance use disorder if they do not maintain a strong connection with their culture. Therefore, addressing Latino patients’ connection to their culture could boost SUD treatment efficacy.
Another significant risk factor for substance abuse among Latinos is discrimination. Repeated experiences with discrimination cause emotional distress, reduce productive coping mechanisms, and increase the attractiveness of substance use. 21 Many studies show the relationship between discrimination and tobacco, alcohol, and illicit substance use. In one study of Latino ninth graders who self-reported varying amounts of perceived discrimination and substance use behavior, perceived discrimination was associated with lifetime smoking, marijuana use, alcohol use, binge-drinking, and other inhalants. 22 Similarly, an analysis of the National Epidemiological Survey on Alcohol and Related Conditions examined the association between discrimination and substance use disorders. This study of 6,294 Latino respondents identified an association between discrimination and increased drug use, though more pronounced among men than women. 23 This disparity may be due to greater cultural acceptability among men to use substances to cope with stress; women were found more likely to rely on social support and food to cope with stress. 23 Overall, this relationship indicates that SUD treatment efficacy would benefit from helping Latino patients cope with feelings of discrimination as part of the therapy.
Cultural barriers to SUD treatment
Even when controlling for factors such as income, health insurance, and English proficiency, Latinos seek SUD treatment less than any other ethnic group in the United States, and at about half the rate of their white counterparts.6,7 Latinos report more attitudinal barriers to treatment than any other group. Compared to their Black and White counterparts, Latinos were significantly more likely to report cultural barriers, including the provider's lack of experience with immigration and discrimination; Latinos felt that their healthcare provider would not be able to understand or relate to their unique needs and experiences with culture, immigration, and discrimination. 7 This expectation was in turn associated with low treatment efficacy. Factors such as stigma and lack of social and family support were major concerns among Latinos. Other studies have found that Latinos are more likely than other ethnic groups to distrust the medical community due to “past experiences of discriminatory treatment or ineffective care, as well as cultural stigmas and attitudes towards psychiatric disorders and mental health services.” 6 Various studies have identified other major cultural barriers to treatment engagement and efficacy. These include familismo, family hierarchy, machismo and marianismo, personalismo, and fatalismo. Many researchers have stressed the importance of acknowledging cultural and social contexts in treatment such as stigma, immigration, and discrimination to increase treatment efficacy.
Moreover, Latinos are primarily Catholic, which greatly impacts their experiences of guilt and shame in their life experiences, such as identifying as LGBTQ. Many Latinos may develop a substance use disorder to cope with intense guilt and internalized homophobia. 24 Because guilt is so ingrained in Catholicism, the work of the counselor must be sensitive to the patient's relationship with religion.
The Hispanic value of Familismo—the moral responsibility to place the family's needs above individualistic needs—is one of the most important factors in treatment engagement and efficacy. If a treatment process begins without the consideration of the nuclear or extended family, the therapy most often results in failure. 6 Latino families typically deal with issues privately, as seeking treatment is seen as a sign of a failing family. 7 Latino family hierarchies are also a significant cultural factor in SUD treatment: Machismo—or the belief that a man's wife and children should submit to him—is associated with excessive alcohol consumption, and Marianismo—the expectation that Latina women submit to their husbands—is the primary predictor of depression among Latina women.6,23 Another factor practitioners should incorporate in treatment is fatalismo, or the strong belief among some Latinos that their problems are determined by destiny rather than free will. 6 The incorporation of these cultural factors into SUD treatment is proven to boost treatment engagement and efficacy.
Cultural competency training in SUD treatment
Cultural competency is the understanding and incorporation of cultural factors that influence addiction and treatment. 25 The existing literature on the importance of cultural competency in treatment outcomes highlights the need for comprehensive cultural competency training among mental health practitioners. Culturally competent counselors that use and understand patients’ cultural backgrounds, immigration, and acculturation experiences in treatment have higher success rates: cultural competence is associated with improved communication, therapeutic alliance, and higher patient satisfaction. A 2017 meta-analysis review on youth 12 to 20 years of age in the United States and Canada suggests that culturally sensitive treatments offer promise as an effective way to address substance use among racial/ethnic minority youth. 26 Culturally enhanced care is associated with a higher likelihood of program completion and fewer depressive symptoms. 27 These findings underscore the need for comprehensive cultural competency training as part of the clinical licensure requirements for SUD practitioners.
The quality of training is just as important as its presence. Studies have shown that shorter, didactic courses on cultural competency are ineffective at changing implicit bias, negative attitudes, or discriminatory behaviors toward minority patients. 28 Training is also often uneven; one study of cultural competency training in medical school only showed learning in some areas and not in others. 29 Much of the existing research on cultural competency training in mental health treatment is from before the year 2000. Interest in minority cultural and health issues has grown substantially since then. There is currently no research on the state of cultural training and education for SUD counselors. This study aims to fill this gap by analyzing the syllabi and descriptions of courses relating to multiculturalism, race, and diversity on the track to becoming a licensed practitioner and by interviewing substance abuse counselors on their experiences regarding cultural sensitivity in training and in practice.
Research design and methods
This study explores how the training in US universities prepares counselors for the unique cultural concerns of Hispanic patients with an SUD and how this translates to practice in Los Angeles County. A thorough analysis of how counselors are equipped to handle Hispanic cultural concerns in SUD treatment is important because it may help Latinos make more informed decisions and improve treatment outcomes. Moreover, the findings could reveal a critical health disparity and open a broader discussion of the moral obligation to ensure people of all racial and ethnic backgrounds receive equitable care.
This study aims to achieve this goal through a content analysis of the psychology curricula regarding cultural sensitivity, diversity, race/racism, and Hispanic cultures at the graduate and undergraduate levels, and thematic analysis of qualitative semistructured in-depth interviews with outpatient drug abuse treatment providers in Los Angeles. This multifaceted approach provides insight into the prevalence and quality of cultural psychology training in higher education, as well as how individual therapists address Hispanic cultural concerns in practice.
Curriculum content analysis
The curriculum content analysis assesses the prevalence and quality of cultural sensitivity training throughout the educational track of becoming a drug abuse therapist. Traditionally, a master's degree in clinical psychology or an equivalent degree is required for addiction therapy. However, the ongoing opioid crisis in California resulted in a rapid expansion of substance abuse treatment centers. In order to staff the new rehabilitation centers, California expanded its licensure system to include therapists with both undergraduate and graduate degrees. 30 Therefore, this curriculum analysis examines the Clinical Psychology graduate and Psychology undergraduate curricula to account for the most common paths in higher education leading to a career in addiction counseling. Although this study's scope focuses on SUD treatment in Los Angeles County, the curriculum content analysis was not limited to universities in LA County or California because students do not necessarily find employment in the same region as their university. The universities whose curricula were analyzed in this study were the top 15 universities for Clinical Psychology and undergraduate Psychology, ranked by the number of degrees awarded in 2020. This was done to represent the most common experiences in higher education for a future clinical psychologist, as these programs have the highest number of graduates. The university data for these psychology programs were acquired through the Integrated Postsecondary Education Data System from the National Center for Education Statistics.
First, I examined the required courses at each university relating to cultural psychology, psychology of race and racism, and diversity, and the syllabus for each relevant course. I then emailed professors and program faculty for course syllabi. Follow-up emails were sent after 4 weeks of no response. In the cases where obtaining a syllabus for a course was not possible, I analyzed the course description available on the program website in a separate category as the syllabi. The course descriptions were analyzed separately from the syllabi because course descriptions are significantly less thorough than syllabi, and therefore cannot be compared. Only required courses were considered for this study in order to generalize the findings for the overall student experience. This establishes the baseline where all counselors are in relation to their learning experience in cultural sensitivity and provides insight into what higher education prioritizes in a diverse education. If no courses on culture/diversity were offered, I included a Social Psychology course in the content analysis. Although Social Psychology courses do not typically focus on culture, rather on social influences and group interactions, I included them in the content analysis to account for any class that could foster discussions of culture, race, and diversity. Additionally, most undergraduate students in US universities are required to take a diversity and inclusion course as part of their general education requirement (GER). In order to more thoroughly represent psychology students’ experience with diversity and multiculturalism in education, I also analyzed two Diversity in America course syllabi. I used the University of Southern California and Rutgers University's syllabi because those were the only ones that were publicly available online.
Based on both the literature review and an iterative coding process of the syllabi and course descriptions, 18 themes have been identified as the most important cultural factors in drug abuse treatment for Latinos: race/racism, culture/ethnicity, prejudice/discrimination, racial inequality, training students to become culturally sensitive psychologists, individual experiences of culture, awareness of cultural differences, the impact of power and oppression, Hispanic/Latino groups, immigration, cultural competency/sensitivity, cultural barriers in seeking treatment, cultural factors in diagnosis and treatment, stigma, acculturation, familismo, family hierarchy (including machismo and marianismo), and religion/spirituality. These themes were predetermined to reflect the cultural factors described in the literature review. Two additional themes were coded for after reading the syllabi that were not included in the original list of predetermined themes; these are “individual experiences of culture” and “awareness of cultural differences.” Those themes kept emerging throughout the syllabi in the Clinical Psychology programs and were included because they are more specific than the general “culture/ethnicity” theme. Because these themes were identified while conducting the Clinical Psychology syllabi content analysis, I went back to the Undergraduate Psychology syllabi content analysis and scored the syllabi for the two new themes.
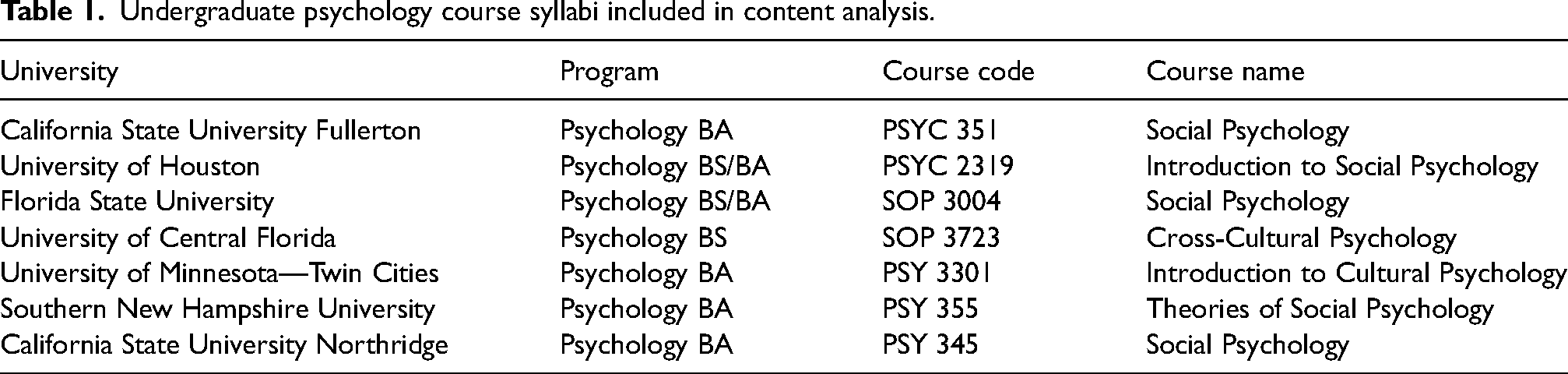
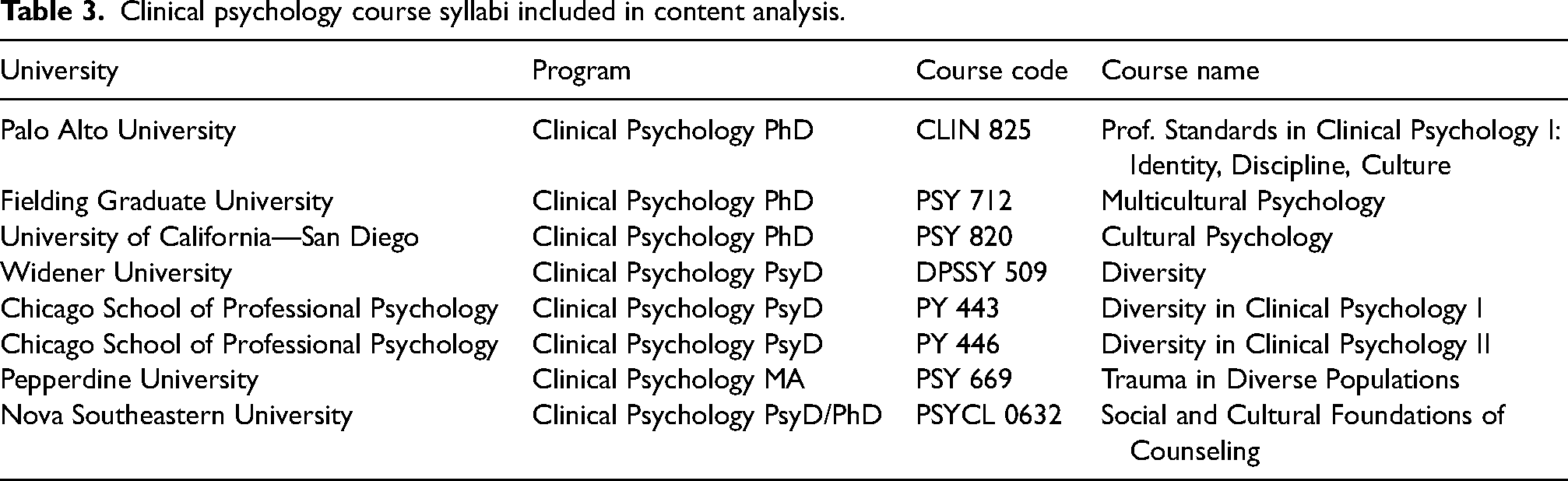
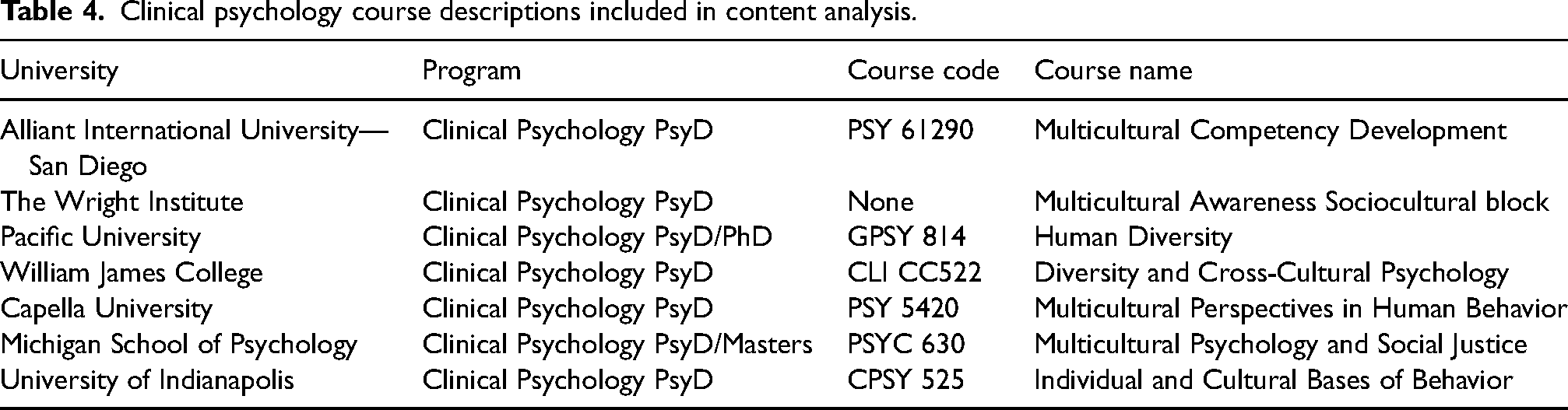
Overall, 24 courses were analyzed (17 course syllabi and 7 course descriptions). Seven of the syllabi were for Undergraduate Psychology, eight syllabi and seven course descriptions were for Clinical Psychology, and the last two syllabi were the GER Diversity courses. The courses included in the content analysis are shown in Tables 1–4.
Undergraduate psychology course syllabi included in content analysis.
GER diversity course syllabi included in content analysis.
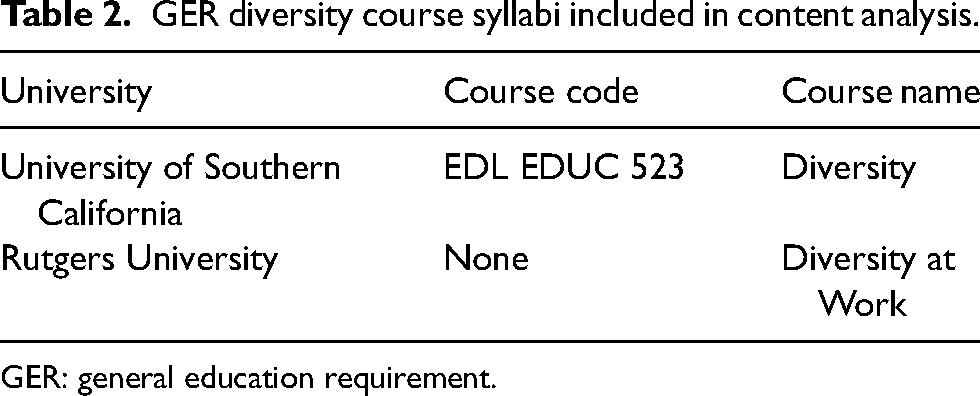
GER: general education requirement.
Clinical psychology course syllabi included in content analysis.
Clinical psychology course descriptions included in content analysis.
A content analysis was used to determine how much culturally sensitive topics emerged throughout the syllabi and course descriptions. Each syllabus and course description was scored based on whether a theme was present, such as a mention in the description, learning objectives, topics covered, and required readings. A higher score means that the student was more exposed to these topics, which could mean that the student is more prepared to counsel Hispanic clients. The course descriptions were analyzed in a separate category from the course syllabi, as the course descriptions only provide a general description of the course content, and therefore expectedly score lower in the content analysis.
Additionally, it is important to note that the course descriptions may not accurately reflect what the students actually learn in a course. Learning outcomes are influenced by faculty training, assigned readings, and assignments. Though not sufficiently extensive to derive a complete picture of learning objectives, the course descriptions provide a valuable insight into what general topics and objectives are prioritized the most in the course. The course descriptions were analyzed with the same method as the course syllabi, acknowledging that they would score much lower in the content analysis. For example, the course description at Alliant University San Diego stated that “participants will improve their multicultural competencies as psychologists” as part of the course. This was coded under both the “cultural competency/sensitivity” and the “training students to become culturally sensitive psychologists” categories.
Interviews
The second part of the method was thematic analysis of eight qualitative interviews with counselors at outpatient rehabilitation centers in Los Angeles County. A thematic analysis was chosen as the method because of its ability to identify and organize patterns within the interviews. 31 The rehabilitation centers were identified using publicly available data from the Substance Abuse and Mental Health Services Administration. Only centers that offered services in both English and Spanish were considered to ensure the clinic had a significant Hispanic demographic. Centers that only offered DUI/Driving school were not considered because of their focus on safety and driving rather than behavior therapy. Out of 158 outpatient rehabilitation centers in Los Angeles County, 75 centers were identified as candidates for interviews. Thirty-one individual centers were contacted because they had a publicly available email address. Various centers were part of larger organizations, so I reached out to the parent organization rather than each center individually. Follow-up emails were sent after 3 weeks of no response.
Ultimately, eight interviews were conducted. Participants signed an informed consent form prior to each interview. All interviews were conducted through Zoom and lasted approximately 20 to 30 min. Participants were asked about their experiences working with Hispanic clients, and the unique challenges they face. The interview questions can be found in Appendix A. With the written consent of each interviewee, I recorded and transcribed each interview. After the interviews were complete, I read through the interview transcripts and identified recurring patterns and themes. I coded the data with a focus on cultural sensitivity, and determined which themes were visited more than the others. Participants have been assigned pseudonyms to preserve anonymity. The pseudonyms assigned match the participants’ gender and cultural background. The full demographic and educational background for each interviewee can be found in Appendix B. All procedures and interview questions were approved by the Cambridge Center for International Research Ethics Review Board (# CCIR-ERB-0125) Granted September 30, 2022.
Results
Curriculum content analysis
Undergraduate Psychology
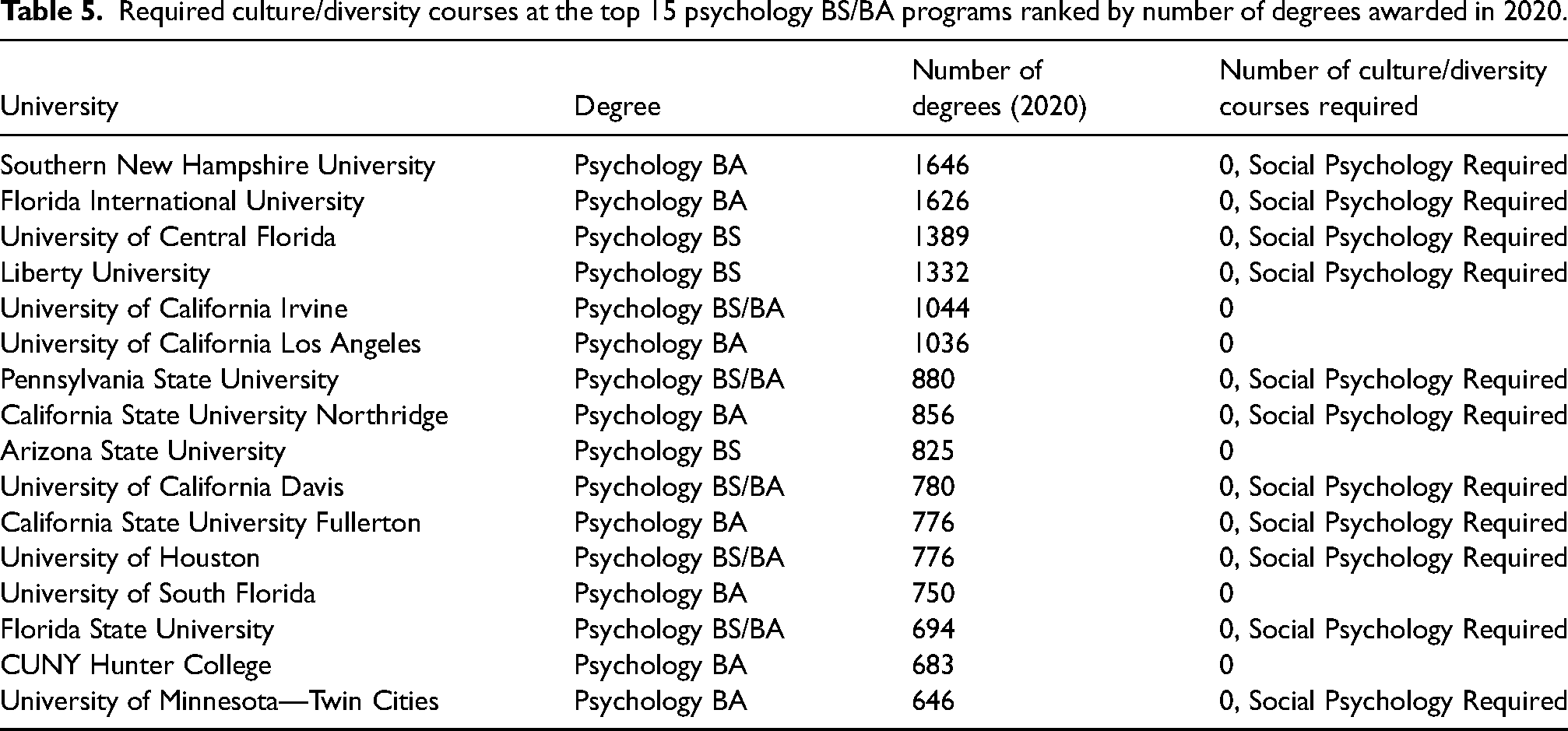
Out of the top 15 universities with the most degrees awarded for a Bachelor of Arts or Bachelor of Science in Psychology, none required a course on the psychology of culture, race/racism, or diversity. The required courses for these universities are shown in Table 5. Ten out of the 15 programs required a Social Psychology course. While none of these universities required a cultural course, many offered one as an elective. Notably, the University of California Davis is the only university to offer an extensive list of Latino/Chicano Psychology electives.
Required culture/diversity courses at the top 15 psychology BS/BA programs ranked by number of degrees awarded in 2020.
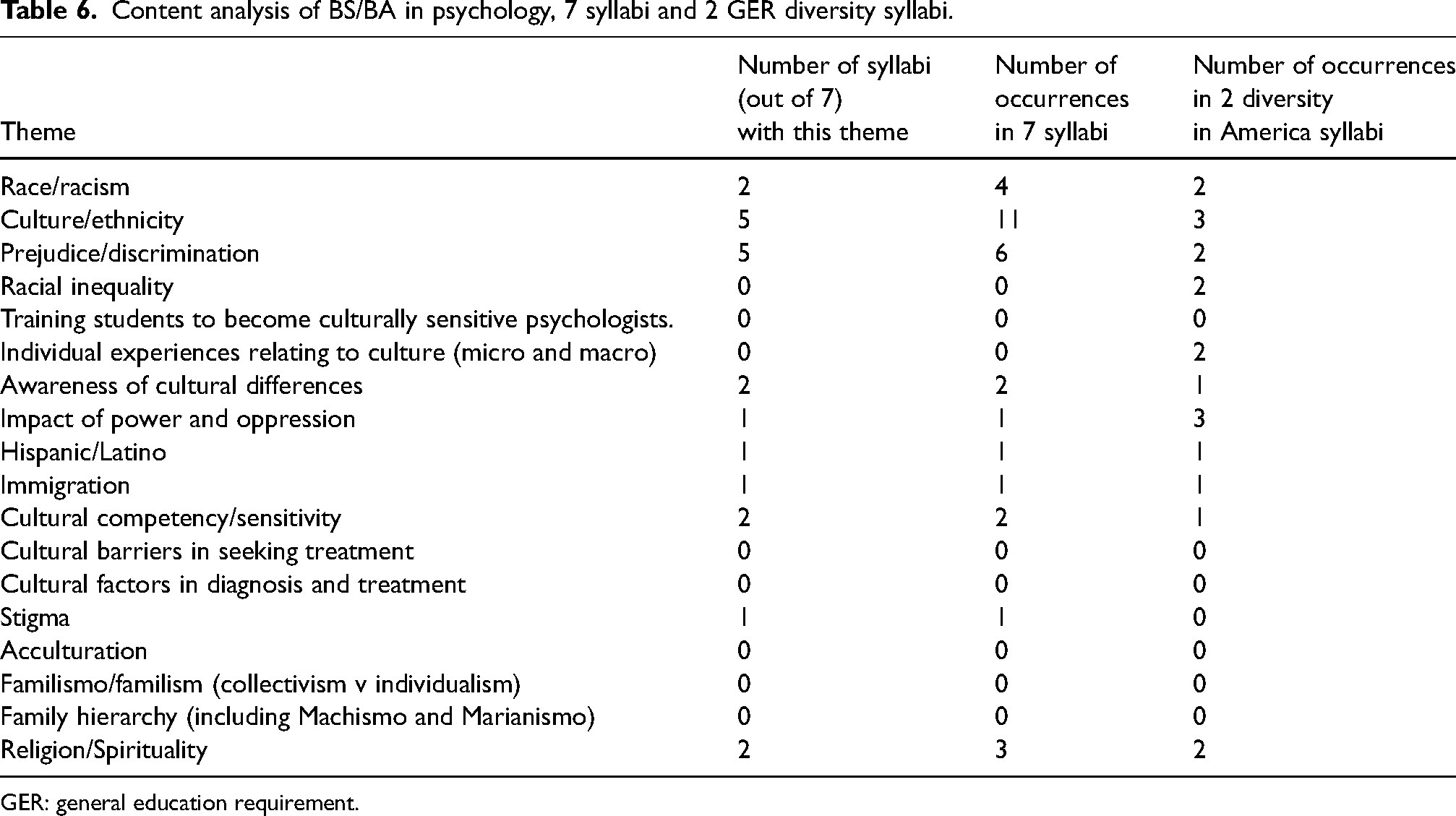
The content analysis for the required Social Psychology courses and the Diversity in America GER syllabi is shown in Table 6. Overall, none of the themes were represented in all seven syllabi.
Content analysis of BS/BA in psychology, 7 syllabi and 2 GER diversity syllabi.
GER: general education requirement.
The most represented themes throughout the syllabi were “Culture/Ethnicity,” occurring 11 times in 5 out of 7 syllabi, and “Prejudice/Discrimination,” occurring 6 times in 5 out of 11 syllabi. However, one of the courses uses prejudice and discrimination to describe “liking others,” and another course dedicates only 2 days out of the entire semester to discuss prejudice and discrimination, which could suggest an oversimplification of the complex phenomena that shape discrimination. In the two Diversity in America general education courses, “Culture/Ethnicity” was the most prevalent theme, with three occurrences. Although 11 out of 18 themes were represented across both syllabi, none were used in a psychological context, rather in general discussions of workplace diversity and social justice.
Graduate Clinical Psychology
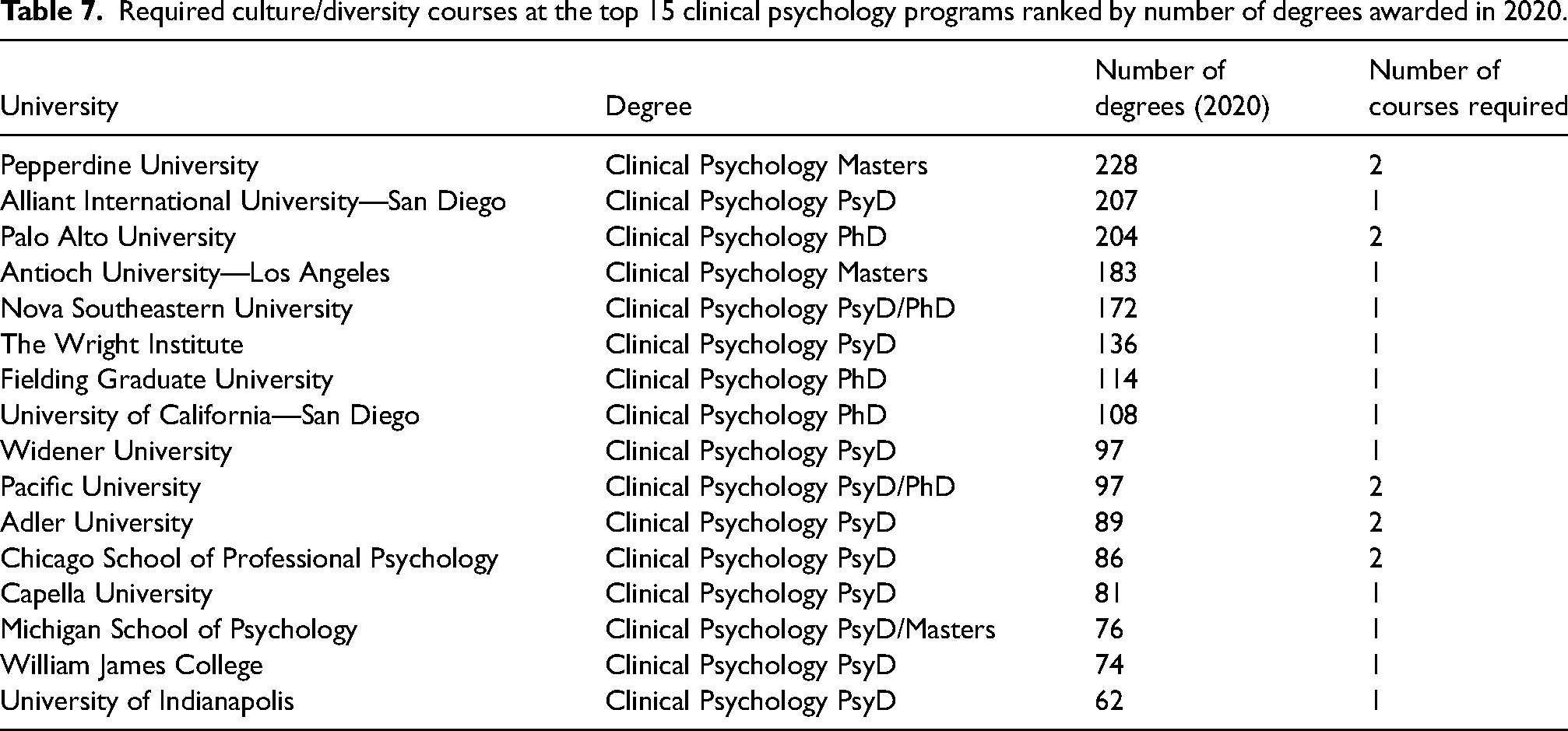
Out of the top 15 universities with the highest number of graduate degrees awarded in Clinical Psychology, 14 out of 15 required at least one course on the psychology of culture, race/racism, or diversity. Five programs required two courses. Antioch University, the only one to not require a multicultural psychology course, offers a Socio-Cultural Perspectives course as part of the Addiction Specialization track in the Clinical Psychology degree. The required courses for each program are shown in Table 7.
Required culture/diversity courses at the top 15 clinical psychology programs ranked by number of degrees awarded in 2020.
The content analysis for the required Clinical Psychology courses is shown in Table 8.
Content analysis of clinical psychology, eight syllabi and seven course descriptions.
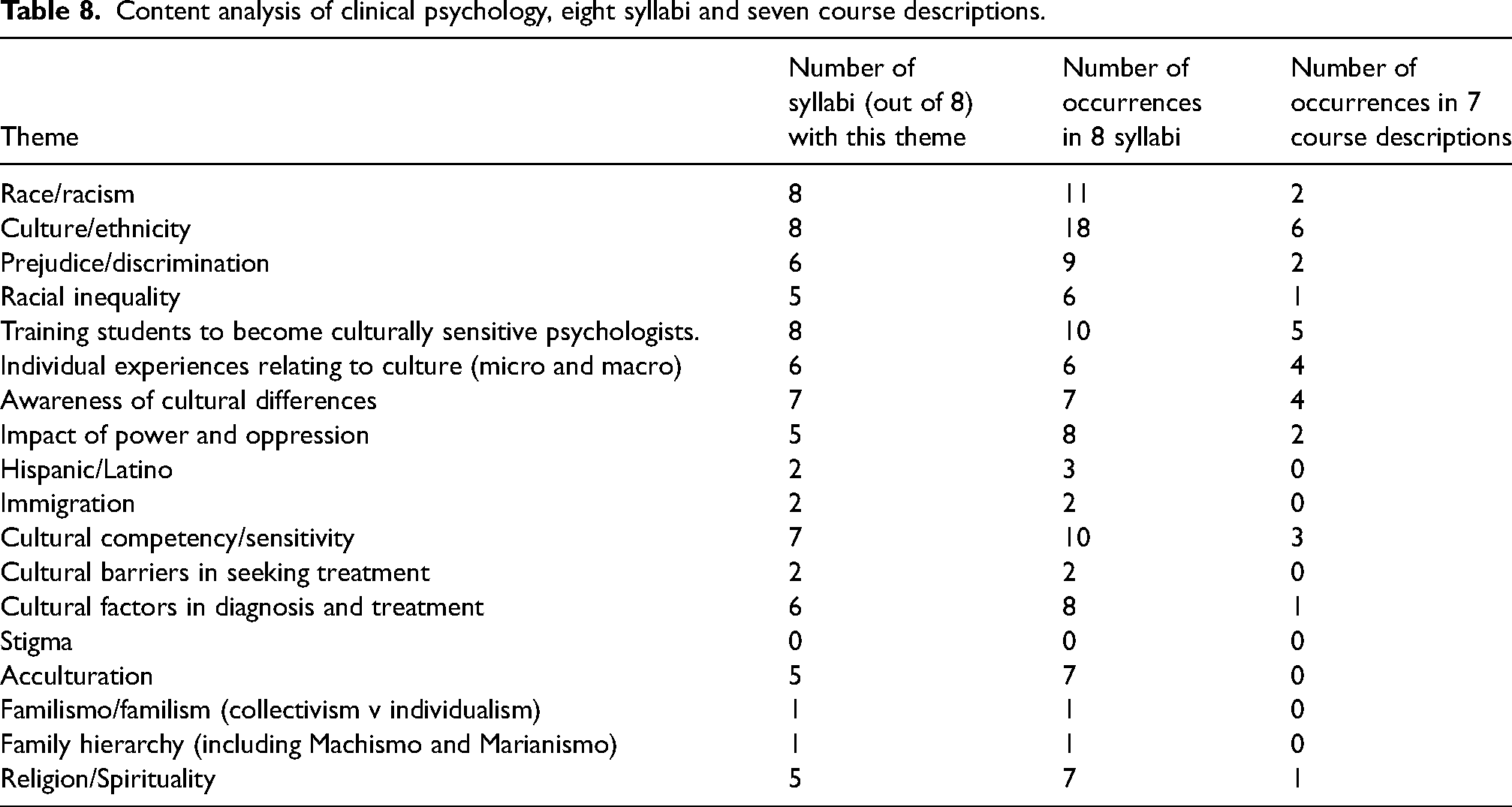
As previously mentioned in the methods section, I obtained eight syllabi and seven course descriptions. Every theme except “Stigma” was represented at least once. “Culture/Ethnicity” was the most represented theme, occurring at least once in every syllabus and course description. “Training students to become culturally sensitive psychologists” was the next most represented throughout the courses. Only two out of eight syllabi addressed Hispanic issues in counseling. Mentions of specific cultural issues (familisimo, family hierarchy, stigma) and cultural barriers were rare throughout the syllabi and course descriptions: familismo and family hierarchy appeared once across all courses. Cultural barriers appeared twice, and stigma was not mentioned at all. The themes “Religion/Spirituality” and “Acculturation” occurred more frequently, appearing in five out of eight syllabi.
Therapist interviews
While the content analysis of the course syllabi and descriptions were helpful in determining the extent of cultural competency education in US university programs on the addiction therapist track, the therapist interviews offer insight on how this education is reflected in practice. Every counselor interviewed said they had patients of all racial/ethnic groups, including Latinos. The participants identified various institutional issues such as language barriers and legal status, as well as cultural issues in treatment, such as overcoming stigma, rejection from the family, and internalized racism. The participants also indicated varying amounts and quality of cultural training. Most reported few if any courses with general discussions of culture and race. The interviewees were not all graduates from the universities included in this study. Marcos Santos, Larry Wilson, and Marvin Stevens were all graduates of universities with a syllabus in this study. Andrew Liu studied at Antioch University, which is one of the universities identified in the top 15 Clinical Psychology programs ranked by the number of graduates in 2020, but does not have a syllabus or course description in this study. The educational background of each counselor can be found in Appendix B.
Institutional issues—language barriers and legal status
Four out of eight participants identified language barriers as a significant issue in counseling for their Hispanic patients. According to Marcos Santos, most centers “don’t have enough Spanish-speaking staff and interpreters.” Natalia Choi adds that there are “not enough translated materials,” for patients to refer to. The shortage of Spanish-speaking counselors and translated materials is well documented as a major barrier to providing bilingual drug abuse treatment, 32 and this deficiency is directly related to worsened treatment outcomes for Hispanic immigrants. 33 Pete Otto describes that one way that the language barrier affects counseling is when “undocumented parents speak little-to-no English, their children are placed into a parentified role of acting as a translator.” This shift in power toward the child damages the parents’ authority and family functioning and hinders the development of a therapeutic relationship between the counselor and the client. 16 Documentation and legal status also emerged in three out of eight interviews as a significant issue in counseling. According to Santos, “his center would never turn anyone away [for being undocumented], but many other centers would.” Larry Wilson describes a “having to hide mentality” among undocumented patients that lead to internalizing behaviors and an inability to fully open up to counselors.
Hispanic cultural factors in treatment
Familismo, stigma, religious guilt, and internalized racism came up as major issues in counseling throughout the interviews. According to Andrew Liu, the “fear of disapproval and rejection from older family members” and “how much control [a patient's] families have in their lives” often exacerbates patients’ mental conditions. Kai Taylor adds that “patients experience difficulty being assertive and setting boundaries with their family.” Similarly, Otto describes that “external and internal stigma are the biggest cultural concern. You can’t talk about what's going on in the family. What happens in the family stays within the family.” Marvin Stevens elaborates on this, stating that “there is pressure from family… to present like they have it all together. It doesn’t leave space for [family members] to process their emotions.” Liu also notes that religious guilt, being LGBTQ, and the fear of rejection by a patient's family lead to internalized feelings of “you’re going to hell, you’re a bad person,” and “anger, frustration, deteriorated self-esteem, hopelessness, suicidal ideation, and self-harm.”
Gender and family hierarchies also emerged as a cultural factor in treatment. According to John Black, “Especially among men, excessive alcohol use is seen as acceptable. It may be downplayed altogether.” Black's experiences with Hispanic men reflect the cultural value of Machismo. Machismo is characterized by physical strength, aggressiveness, and the ability to consume an excessive amount of alcohol without getting drunk. 6 This can be a significant barrier to seeking treatment for a substance use disorder, as Hispanic men may view treatment as showing weakness. Stevens, who specializes in the treatment of young men specifically describes Machismo as a serious cultural obstacle because it is difficult to get Hispanic men “into a vulnerable condition where they are willing to talk about things… and work on their health.”
Additionally, Wilson observes that Hispanic women may struggle with substance abuse due to an “exceptionally low self-worth” because they must “cower to their husbands,” reflecting the cultural value of Marianismo.
Liu also describes the effects of internalized racism on drug abuse among his Hispanic patients. His patients have experienced “normalized racism from such an early age that it is barely recognizable,” and have “gotten so used to microaggressions” that it leads to internalizing behaviors. The racism they experience becomes the “foundation of believing ‘I’m not good enough, I am an outsider.’” The suppression of these feelings and low self-worth is a major contributor to addiction and alcoholism. According to Liu, when “people don’t talk about their problems, [there is] an overwhelming desire for relief, making someone even more prone to alcoholism or substance abuse.”
Insufficient cultural competency training
When asked about their experiences with cultural sensitivity training and education, all eight participants indicated at least some formal education in multicultural counseling or cultural competency. Liu and Otto both talked about how culture was discussed all throughout their education, with no specific course. Liu states that “Social justice is a cornerstone of how [his university] approach[es] all education, and a lens that is used to look through at everything.” Otto states he “learned about the impact of faith on a person's worldly perspective” in his undergraduate degree, and “culture as a whole” in his master's degree. Like Liu and Otto, Choi states she had “no specific classes. A few classes sprinkled in discussions about diversity. [There were] some discussions about what to consider when working with particular groups.” Choi admits this education was “not very extensive… [there was] at most one lecture throughout the program.” Taylor also expresses dissatisfaction with how cultural competency and diversity was addressed throughout his education. He was “taught one course” that was “woefully insufficient, briefly went through different cultures and skipped a lot of things. It was one semester, very cookie cutter, rushed.” After graduate school, he had “only optional cultural courses.”
Most counselors said they have had some short workshops postgraduate school in cultural diversity. As Choi and Santos noted, every counselor needs to renew their license every 2 years and take 40 h of continuing education. This includes a multitude of topics, including HIV/AIDS and cultural diversity. According to Choi, these workshops are often “online self-paced videos and modules through a learning management platform, virtual webinars, and conferences.” Stevens elaborates on this idea, describing the courses as brief “videos you have to watch and a questionnaire you have to fill out.” He admits that the courses were not particularly memorable, and only focused on “ethics and understanding social contexts.”
Openness to cultural competency training
Two participants indicated that the effectiveness of cultural competency training is dependent on how willing the counselor is to engage with it. Liu states that “the Los Angeles bubble is more open-minded… I am sure that there are places where [cultural competency training] is excluded… The majority of clinicians are exposed to it, but not all are responsive to it.” Wilson echoes this idea. He states that they’ve all received training in inclusivity, but “some people don’t want to look at the struggles of being a minority.” According to Wilson, “Caucasians are less open to [cultural competency training] because it's too deep for them to deal with.” The importance of openness to discussions of cultural diversity is clear in Otto's interview. The conversation felt forced; when asked about whether he thought education in cultural diversity was important, he dismisses the question: “I think people forget that anything can be a culture… Gaming is a culture.” Liu and Wilson's point about openness to cultural sensitivity training is further illustrated in Santos's interview. When asked about his experience in cultural diversity education, Santos says, “we’re really being bombarded with these classes right now.” This reflects the attitudes of some counselors toward cultural sensitivity. Some see it as a burden and unnecessary.
Discussion
This study was conducted to determine the extent to which American universities prepare substance abuse counselors to address the unique cultural concerns of their Hispanic patients, and how this education is reflected in Los Angeles outpatient rehabilitation centers. The results of both the content analysis and the interviews indicate that cultural competency training for substance abuse counselors appears to be inadequate for addressing the specific needs and concerns of Hispanic clients. This is proven by the lack of exposure to Hispanic cultural issues in both undergraduate and graduate programs, as well as counselors’ descriptions of their education in cultural competency. Evidently, this presents a significant ethical issue, as counselors could potentially be underprepared to meet the needs of their Hispanic patients.
Cultural competency training is particularly weak at the undergraduate level. The discussions of race and culture in the samples found are too general and infrequent to adequately prepare students for a career in addiction counseling for diverse populations. The fact that none of the Psychology BA/BS programs in this study require a course on the psychology of culture, race/racism, or diversity is alarming because students may not have the necessary skills and knowledge to effectively work with Hispanic clients in their future careers as addiction counselors. Students that pursue a master's or doctoral degree in Clinical Psychology are likely better prepared than those with only a bachelor's degree in Psychology. Overall, the results of the Clinical Psychology content analysis make it clear that the objective of these courses is to train culturally competent psychologists. The themes “cultural competency/sensitivity” and “training students to become culturally sensitive psychologists” emerged in 100% of the syllabi and a majority of the descriptions (3/7 and 5/7 course descriptions, respectively). However, the lack of focus on specific factors (i.e. familismo, family hierarchy, stigma, and immigration) and distinct cultural groups within the syllabi raises serious ethical concerns about the effectiveness of the training in preparing psychologists to work with diverse client populations.
The results of the interviews confirm and expand on the results of the content analysis regarding the extent to which drug abuse counselors are trained in cultural competency for Hispanic clients. All eight participants said they had received significant variation in instruction in culture and diversity, which is reflected in the content analysis; there was significant variation in the number of cultural courses required for each set of psychology programs. Several counselors reported that issues related to language barriers, legal status, stigma, familism, racism, discrimination, gender, and being LGBTQ came up frequently in their professional experiences with Hispanic clients. However, as illustrated by the content analysis, these topics are noticeably lacking throughout the syllabi. This is another indication that the existing cultural competency education is inadequate for training culturally sensitive psychologists, as many of the real-world issues faced by Hispanic clients are either not mentioned or overly simplified in the universities’ curricula of this study.
The importance of cultural competence education for substance use counselors cannot be overstated. As society becomes increasingly diverse, it is imperative that counselors are equipped to understand and work with patients from different cultural backgrounds. The most crucial factor in a counselor's cultural competency education is the openness of the counselor to learning about the cultural and racial struggles of their patients. Simply offering cultural competency courses as an option is not enough—they must be made compulsory. At a minimum, undergraduate psychology programs must require cultural psychology courses instead of only offering them as electives. This way, all students will be exposed to some cultural issues they will encounter in their professional careers, rather than just the most interested students. While there is still much work to be done in improving the quality of cultural psychology courses, the first step is to ensure that students are exposed to issues of culture and diversity at all stages of their education.
From the course content analysis and interviews, it is clear that the curriculum in cultural competency education is too vague and surface level to adequately prepare students for a career in addiction counseling for Hispanic clients. In the syllabi, culture is used as a buzzword, referring to generalities such as “respect for diversity” without delving into the specific cultural considerations and experiences of Latinos or any other ethnic group. The generic, sweeping discussions of culture, race, and diversity in higher education may have led to cultural sensitivity not being taken seriously and addressed as a structural issue. This is evident in some counselors’ dismissive attitudes toward considerations of culture in treatment, particularly in Otto's remark that “anything can be a culture, gaming is a culture.” Lui and Wilson's commentary on the lack of receptiveness of many counselors towards these issues, and Santos's claim that counselors are “bombarded” with cultural diversity courses, highlight the low priority placed on cultural sensitivity among many substance abuse counselors. This lack of priority stems from the fact that cultural sensitivity is not a priority in higher education. Evidently, in order to address the wide variety in the amount and quality of cultural competency training and indifference among many substance abuse counselors, there is a need for comprehensive, mandatory cultural competency education that goes beyond generic discussions to the specific, cultural considerations that emerge in counseling.
Conclusion
Implications
This study on the extent of Hispanic cultural competency training in higher education for future drug abuse counselors has far-reaching implications for both the field of counseling and for Hispanic clients seeking treatment. The findings of the study can be used to guide university psychology programs in improving their curriculum regarding culture, race, and diversity. Universities can identify areas of improvement to ensure that their students are properly prepared to work with diverse populations. Furthermore, this study can help inform Hispanic clients about the state of cultural competency among drug abuse counselors in Los Angeles, which can help them make informed decisions when seeking treatment options. The findings of this study can be extrapolated beyond Los Angeles. If even in “sanctuary cities” like those in Los Angeles County, which trend toward improved mental healthcare for Latinos, the cultural competency training is not enough, it raises serious concerns about the state of cultural competency in substance abuse counseling nationwide. 34
The findings of this study highlight a critical health inequity toward a historically disenfranchised group and underscore our moral obligation to address it. It is a matter of ethical responsibility for the field of substance abuse counseling to cultivate a diverse and culturally competent workforce that can truly meet the needs of all clients. Without concrete action from education and healthcare systems, these findings will only continue to fuel the skepticism and mistrust toward substance abuse counselors that prevent Hispanic people from seeking care. Furthermore, these findings open a broader discussion of how clinicians may be underprepared to fully meet the needs of other racial and ethnic groups across the United States and beyond. Universities must prioritize a diverse, cultural education at all stages of a career in drug abuse counseling, from undergraduate education to professional development, and healthcare systems must implement policies that ensure that practitioners are well prepared to provide all patients with effective and equitable care.
Limitations
One limitation of this study is my sample size. Out of the 28 total required courses relating to multiculturalism and diversity identified in the 30 university programs with the highest number of graduates for Clinical Psychology and for Undergraduate Psychology, I obtained 17 course syllabi (including the two Diversity in America GER courses) and 7 course descriptions. Additionally, out of the 31 rehabilitation centers contacted, only 8 counselors reached out for an interview. A larger sample size would have increased the validity of the findings, as it would have allowed for more representative samples of the university programs and outpatient rehabilitation centers, and provided a more comprehensive understanding of the extent of cultural competency training for Hispanic patients.
The conclusions of this study are also limited by the study's delimitations. For the content analysis, this study considered bachelor's degrees in Psychology and master's or doctoral degrees in Clinical Psychology to account for the most common paths in higher education. However, this doesn’t include other common paths, such as a master's degree in Social Work or a master's degree in Marriage and Family Therapy.
Additionally, it is important to acknowledge the variation in the type of programs reviewed. Some are traditional schools, while others (specifically Liberty University, NOVA, and SNHU) are online. The standardized syllabi for the online programs may not fully reflect student learning outcomes because faculty do not have the freedom to modify the course content or determine what topics should be prioritized.
Areas for future study
This study highlights several areas for future study in the field of cultural competency for substance use counselors. Future research could expand the content analysis to include more universities and a greater variety of degrees such as a master's in Social Work. Another important area for future study is to analyze multiculturalism education in the licensing programs and licensing renewal programs. This would provide insight into the extent to which counselors are required to continue their education in cultural competency after graduation. It would also be valuable to expand the research beyond the open-minded “Los Angeles bubble” to see if the findings are consistent nationally. Further studies should also investigate clinical placements for the students in the programs analyzed in this study. Finally, because course descriptions and syllabi are meant to provide a general overview of a course, the exact characteristics of the courses in this study cannot be determined. There could be topics covered in a course that are not included in the syllabus or course description. Future studies could include participant observation in these courses, interviewing students who attend these courses, or conducting a survey with students to explore the content of these courses in depth.
Footnotes
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Data availability statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.
Notes
Appendix A
How did you decide to become a therapist? Would you be able to tell me a bit about your educational background?
a. University? b. Degree? c. License? Can you tell me about your work experience? What other centers have you worked at? Why did you arrive at this particular center? Do you have patients from diverse racial and ethnic backgrounds? Do you see a lot of Hispanic patients? What issues/concerns do you think are unique to your Hispanic patients?
What culture/race-related issues have come up during counseling for Hispanics? What kind of education/training did you receive on cultural sensitivity/diversity/race/racism?
Do you think it's important to have this kind of education?
If so, how would you design it? What would you add/remove? What changes would you make? Is there anything else you would like to add apart from what was discussed? Demographic: Gender, race, ethnicity
Appendix B: Interviewee Demographic Information and Education
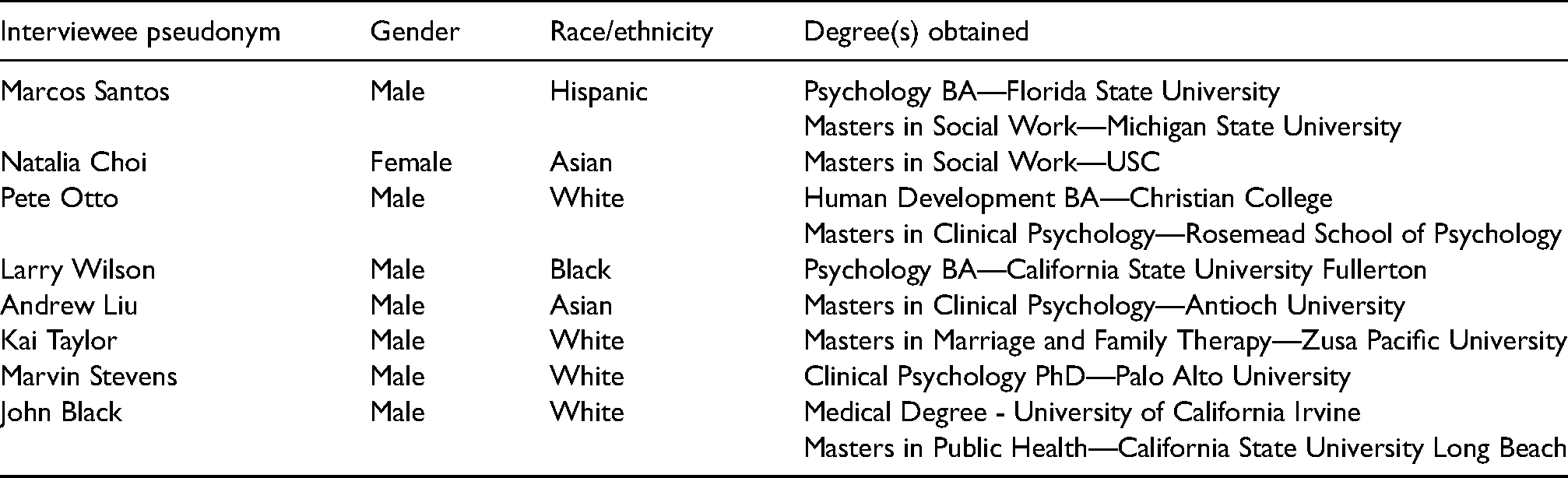
| Interviewee pseudonym | Gender | Race/ethnicity | Degree(s) obtained |
|---|---|---|---|
| Marcos Santos | Male | Hispanic | Psychology BA—Florida State University Masters in Social Work—Michigan State University |
| Natalia Choi | Female | Asian | Masters in Social Work—USC |
| Pete Otto | Male | White | Human Development BA—Christian College Masters in Clinical Psychology—Rosemead School of Psychology |
| Larry Wilson | Male | Black | Psychology BA—California State University Fullerton |
| Andrew Liu | Male | Asian | Masters in Clinical Psychology—Antioch University |
| Kai Taylor | Male | White | Masters in Marriage and Family Therapy—Zusa Pacific University |
| Marvin Stevens | Male | White | Clinical Psychology PhD—Palo Alto University |
| John Black | Male | White | Medical Degree - University of California Irvine Masters in Public Health—California State University Long Beach |