
Abstract
Vulnerability is frequently conceptualized as a group attribute, with all members of that group automatically receiving additional safeguards, including denial of access. There has, however, been a move to recognize more nuanced, context-driven concepts of vulnerability. In the research setting, this has taken the form of a taxonomy that identifies eight types of vulnerability (cognitive, juridic, deferential, social, medical, situational, allocational, and infrastructural) that can lead a potential research subject to make choices against their own best interests. In the consumer context, vulnerability is conceptualized as a lack of control arising from the interaction of personal states, personal characteristics, and external conditions that hinder marketplace navigation. This study examines both the research and consumer conceptualizations of vulnerability for candidates for uterus transplantation (UTx)—a procedure that is transitioning out of the context of clinical trials, and into a consumer marketplace. It identifies the potential for most types of vulnerability defined in the research taxonomy, as well as the strategies, such as a psychosocial evaluation during the screening process, that can be carried forward from UTx clinical trial protocols to manage these vulnerabilities. Likewise, the consumer-driven model for vulnerability indicates similar risks for UTx as have been identified for in vitro fertilization: specifically, a willingness among women with low chances of success to repeatedly incur physical, financial, and emotional risks in the pursuit of pregnancy, and the need to support a sense of control through managing expectations and validating decisions about appropriate treatment endpoints.
Introduction
Vulnerability is frequently considered to be a characteristic that applies at a group level, with the additional safeguards or resources automatically applied to all group members and denied to nongroup members. For example, in the context of research involving human subjects, the groups identified as vulnerable or requiring enhanced protection for participation in research in the Code of Federal Regulations are: Pregnant women, human fetuses, and neonates; children; and prisoners. 1 Such sweeping categorization into “vulnerable” and “not vulnerable” runs both the risk of restricting access or participation for all those deemed vulnerable and the risk of failing to adequately protect individuals whose vulnerabilities are missed. In research studies, there is the opportunity for nuance to be addressed through institutional review board oversight, but as a practical matter, this requires standards for identifying and responding to vulnerability in a systematic, context-specific manner. 2 To do this, a taxonomy for vulnerability has been developed to identify vulnerable characteristics in research subjects, 2 and then applied to analogous contexts in medicine—for example, living organ donation3–5—where there are similar concerns to research about individuals taking on personal risk where most or all of the benefit will accrue to someone else. This taxonomy has not yet been applied to the systematic analysis of potential vulnerability characteristics in patients seeking interventions in which they will carry all (or most) of both the risks and benefits. This may be because, for much of medical care, these evaluations are based on medical necessity to preserve or prolong life, further guided by professional codes of ethics containing such exhortations as to “regard responsibility to the patient as paramount.” 6 Nonetheless, there are contexts within healthcare, such as cosmetic surgery 7 and fertility medicine 8 in which patients are willing, or even eager, to take on physical, emotional, and financial risks that seem disproportionate to the benefit, or likelihood of benefit, to be gained, making it appropriate to consider and address potential vulnerabilities.
This raises the question of how those potential vulnerabilities should be assessed. One option is to apply the taxonomy of vulnerability in research, 2 similar to its application to vulnerability analyses for living organ donors.3–5 A second is to consider the patient as a consumer and apply the definitions and models of consumer vulnerability that have been developed. 9
Uterus transplantation (UTx) is an evolving area of reproductive medicine for which the ethics have been vigorously debated in terms of autonomy, beneficence, nonmaleficence, and justice, 10 but for which a systematic taxonomy-based analysis of vulnerability characteristics has not been examined. Vulnerability has been analysed for living uterus donors, 5 but not yet for the candidates or recipients of UTx. Moreover, the concept of consumer-related vulnerability has not been explored in UTx. Here, we apply both the taxonomy of vulnerability developed for research settings 2 and adapted for organ donors,3–5 and a consumer-driven model of vulnerability 9 that has previously been applied to women seeking in vitro fertilization (IVF) services 11 to examine the situation from the perspective of women seeking to undergo UTx.
Applying the taxonomy of vulnerability in research to UTx recipients
Vulnerability is defined in the Declaration of Helsinki as “an increased likelihood of being wronged or of incurring additional harm,” 12 with the Council for International Organizations of Medical Sciences expanding on this to note that “persons are vulnerable because they are relatively (or absolutely) incapable of protecting their own interests” or “because some feature of the circumstances (temporary or permanent) in which they live makes it less likely that others will be vigilant about, or sensitive to, their interests.” 13
In the context of research, the primary vulnerabilities are those that call into question the efficacy of the individual's consent to participate, as this consent is what makes the normally impermissible experimentation on, or investigation of, a research subject permissible. 2 Similarly, in living organ donation, the primary question is whether donors can provide fully informed and voluntary consent to the otherwise impermissible removal of their organ for someone else's benefit.3–5 Informed consent is similarly critical to the permissibility of therapeutic interventions, since perception of risks and benefits is subjective, and the principle of respect for autonomy recognizes the right to choose which of these to accept and pursue. Vulnerabilities that threaten the validity of the consent process are a key component in the context of clinical treatment. In the case of treatments that occur over time, or in multiple steps, as is the case for UTx, it is important to consider that vulnerabilities may change over the course of treatment or be present only in certain steps, requiring anticipation and preparation for later vulnerabilities, where possible, as well as ongoing assessment and flexibility to address unanticipated vulnerabilities that arise.
Between the original taxonomy of vulnerability for research participants published in 2001 2 and a version published 2 years later focusing on pediatric research subjects, 14 eight discrete vulnerability traits have been identified, and all have been included in the analyses of vulnerability in living organ donors.3–5
Cognitive or capacitational vulnerability hinges on whether the potential UTx candidate has the capacity to deliberate about undergoing the process. Characteristics associated with cognitive/capacitational vulnerability include immaturity of age, intellectual disabilities, and mental illness. 15 In considering capacity to consent for UTx, it needs to be kept in mind that the goal of the clinical procedure as currently practiced is not only a technically successful organ transplant but also pregnancy and childbirth; additionally, a graft hysterectomy will ultimately be required. Consent to such reproductive choices is set to a high bar. The widespread exceptions for rape to laws banning abortions, as well as more recent legislations such as the 2021 California law making nonconsensual removal of a condom during intercourse a civil offence 16 and inclusion of unwanted pregnancy resulting from sexual assault among the aggravating factors considered in many states, 17 recognize the importance of consent to impregnation. Court decisions that have weighed one gamete donor's objection to the use of remaining frozen embryos over the other donor's desire to use them 18 likewise recognize the importance of consent to the related concept of genetic parenthood. At the other end of the reproductive cycle's decision-making, the history of forced sterilization of those with intellectual disabilities under the influence of the eugenics movement and through to the second half of the twentieth century 19 has led to recognition of a “heavy presumption against sterilization of an individual incapable of informed consent.” 20
There are essentially two strategies for dealing with capacitational vulnerability in any context that requires decision-making: selection criteria that bar participation by anyone who does not have the necessary capacity, or using surrogate decision-makers. Which strategy makes most sense to employ depends very much on the context, and examples of each being used in relation to the reproductive decision-making required over the course of the UTx process exist. Age-based selection criteria that avoid the issues associated with having participants considered too young to legally provide informed consent have been applied at the threshold of entry into UTx clinical trials (e.g., the selection criteria for the clinical trial of UTx in the United Kingdom includes a minimum age of 24 years 21 ) and are now being applied by transplant centers offering UTx outside the context of clinical trials (e.g., the UTx program at Baylor University Medical Center lists an age range of 18–45 years among the eligibility criteria for potential recipients 22 ). The selection criteria approach makes sense where the bar to access it creates as a trade-off for the protection from capacitional vulnerability it provides will not cause substantial harm. Establishing minimum age-eligibility criteria for access to an elective procedure like UTx is a good example of such a situation. Another scenario in which the bright-line approach of selection criteria to address capacitational vulnerability applies is when the balance of risks to benefits of a procedure makes the individual's own judgment so essential that the use of a surrogate decision-maker is inadequate. The decision to become a living uterus donor has been identified as one of these, given the risk to the donor and lack of medical urgency for the recipient. 5
The surrogate decision-maker approach, in contrast, is well-suited to situations in which there is a need for case-by-case determinations of capacity and related adjustment to the patient's role in decision-making (e.g., the use of supported decision-making 23 ), rather than the complete bar to access that selection criteria can create, and to time-urgent situations in which there is no opportunity for time or some intervention (such as treatment for a psychiatric illness) to cure the lack of capacity. A recent review of the literature examining reproductive decision-making in women with severe psychiatric illness (e.g., schizophrenia) 24 provides examples into how lack of capacity has been dealt with for several of the reproductive decisions that may be encountered during the UTx process (from transplant, through IVF, pregnancy, and cesarean delivery, to graft hysterectomy). These are worth considering because, while the screening processes that were developed for UTx clinical trials 25 and are now being applied where UTx is offered as a clinical procedure 26 can ensure that UTx recipients do not have any substantial capacitational vulnerabilities at the point of entry on the UTx pathway, it is a multiyear process, involving multiple surgeries and, where successful, one or more pregnancies. In other words, the potential for the recipient to lose capacity (e.g., if they suffered a stroke, or sustained a traumatic brain injury during a car accident) at some point in the process when one or more critical reproductive decisions still needed to be made, is a risk that should be considered and planned for. The most common reproductive decision points included in the review of the literature related to termination of pregnancy, and timing and method of delivery. 24 In some cases where capacity was lacking, it was able to be restored in time for the patient to make their own reproductive decision. 24 In most other cases, specified or unspecified relatives acted as surrogate decision-makers. 24 The exceptions were one case of psychotic denial of pregnancy, in which the decision-maker was the legal system applying the patient's substituted judgment (she was asked what she would want to do if she were pregnant),24,27 and one case in which it is not clear whether or not the patient lacked capacity, but the decision to follow her request for induction of labor was based primarily on the consulting psychiatrists’ recommendation to induce for worsening maternal psychiatric status combined with the obstetrics team's judgment that, as she was full term, the physical risks of induction were low.24,28 No cases reporting decision-making for IVF where the patient lacked capacity were identified in this review—which is consistent with it being a nonlifesaving, nonurgent procedure with significant ramifications for multiple parties. It is, however, worth noting that exceptions can occur: there is at least one reported case of IVF being performed in Israel for a patient who lacked capacity due to immaturity of age: a married, Israeli 16-year-old with polycystic ovarian syndrome for whom other fertility treatments had proved unsuccessful underwent IVF—with the decision to proceed factoring in the lack of any law restricting treatment under the age of majority; the combination of the patient's consent with that of her 23-year-old husband's; the specific cultural context of Arab–Israeli society in which not only is fertility highly valued but a young married couple is dependent on the wider family for income and residence; and the wide availability of and public funding for fertility treatment in Israel. 29 The physicians concluded in their case report “As long as the right of the physician to abstain from providing fertility treatment is not regulated, the role of the physician is reduced to discussing the issues with the young patient and her guardian.” 29 As such, it is not inconceivable that similarly placed physicians in a UTx program might feel compelled to employ a surrogate decision maker (rather than applying a minimum eligible age selection criterion) to provide informed consent if approached by a minor with absolute uterine factor infertility (AUFI) in a similar social situation seeking access to UTx.
Broadly speaking, the nonurgent, nonlifesaving nature of UTx, coupled with the substantial long-term consequences for multiple parties of the parenthood it is intended to achieve, capacity to consent should be a requirement for initiating the UTx process. Uterus transplantation programs can ensure candidates’ capacity through psychosocial screening that considers age, health literacy, and mental and emotional well-being. Establishing minimum age criteria will be the most efficient means of avoiding capacity issues related to immaturity for most UTx programs. This approach has been followed by some jurisdictions regulating surrogacy: for example, requiring that all parties to the gestational agreement be at least 21 years old. 30 However, as the case of IVF use in an Israeli adolescent demonstrates, 29 there may be specific contexts, such as a UTx program located in a jurisdiction that the physicians do not feel protects their right to refuse fertility treatment, 29 in which case-by-case determinations factoring in additional criteria are applied.
In addition to considering the potential UTx candidate's immediate capacity to consent to beginning the UTx process, including a psychosocial evaluation that incorporates a comprehensive clinical interview as well as standardized mental health measures in the screening process25,26,31 offers the opportunity to consider the potential loss of capacity in the course of treatment, and have candidates identify surrogate decision-makers and consider providing written records regarding their preferences for the reproductive decisions that can be anticipated over the course of the UTx process.
Juridic vulnerability addresses situations in which the patient is liable to the formal legal authority of a third party who has an independent interest in the treatment or its outcome. 2 Examples include prisoners (subject to the authority of their warders), military enlistees (subject to their officers), children (subject to their parents), and, in some countries, adult women (subject to the male head of household—typically a husband or father 32 ). 2 Unlike the research context in which the taxonomy of vulnerability was developed (where, historically, there were financial or tactical incentives for prisons and military units to host research studies33,34) or the organ donation context (where the possibility of a reduced prison sentence may arise 35 ) it is an unlikely scenario in which those in authority in a prison or the military would have anything to gain from forcing or coercing female prisoners or soldiers to undergo UTx. In contrast, there are incentives in these settings (cost savings, no disruptions to routine related to the time/resources required for fertility treatments, prenatal care, or maternity leave) to exercise authority to prevent women from accessing UTx—or to fail to exercise authority to ensure access to immunosuppressants 36 in the case of a woman who had already undergone UTx at the point of incarceration—that need to be considered as part of the discussion about equitable access to UTx.
The use of parental authority to obtain UTx may need to be considered in societies in which fertility is considered an intrinsic part of a woman's value, and parents may see UTx as an opportunity to increase the prospect for or value within a marriage 37 for a minor daughter with AUFI. Likewise, for UTx candidates in countries where husbands or male relatives have legal authority over women's reproductive decisions, 38 the final decisions at each step in the UTx process may not rest with the patient, and UTx programs in such countries will have to develop their consent processes for that context. In the case of UTx candidates from such countries traveling to UTx programs located in countries without male guardianship requirements, the UTx program is likely to regard the situation as one of deferential vulnerability (outlined below), since local laws will require the patient's own consent.
An additional aspect of juridic vulnerability needs to be considered for the pregnancy phase of the UTx process: access to abortion. While there is no formal legal authority restricting UTx, the inability to access abortion in high-risk pregnancies may deter patients from seeking UTx in certain countries (or certain states within the United States), or force recipients to relocate to an area inexperienced with UTx if an abortion is being considered. This is particularly relevant in the case of abortion bans that lack clear exceptions for risk to the health or life of the mother.39,40
Deferential vulnerability refers to patterns of behavior that may mask an unwillingness to participate. 2 In the case of living uterus donors, risk of deferential vulnerability has been identified in the case of related, particularly maternal, donors, who may want to please their family or “make up” for their daughter's infertility. 5 In the case of UTx recipients, the existence of UTx as a treatment for AUFI opens women with AUFI up to the pressures, or even abuses, from their families to “continue the family line” that has been recognized in women for whom IVF and other forms of assisted reproductive technology (ART) have offered potential solutions to their or their partner's infertility. 41
Deferential vulnerability might be most expected in the context of a couple from a traditional patriarchal society in which the husband (or his family) has the majority of the reproductive decision-making power.42,43 If the UTx program is not located within a community in which those are the norms, consultation with physicians, psychologists, and/or religious leaders from the relevant society may be helpful in ensuring a culturally competent screening and/or informed consent process that meets the needs of the patient and her family, and the healthcare team. The potential for deferential vulnerability should not, however, be ignored for potential UTx candidates from any cultural background, as individual characteristics or situations—such as power dynamics within a marriage, with a recent U.S. study finding that women with low situational power during marital conflict (and particularly those holding traditional gender role beliefs) tend to resort to submission 44 —can create similar risks for deferential vulnerability. Uterus transplantation programs can guard against this by including an assessment of relationship quality between the couple/among the candidate's family as part of the psychological evaluation portion of the candidate screening process. 31
Social vulnerability refers to individuals who are in groups whose rights and interests have been socially disvalued.3,45 The National Bioethics Advisory Commission includes both economic vulnerability and the stereotyping and discrimination that members of such groups are subject to as aspects contributing to their vulnerability. 45 Others have expressed it in terms of “these individuals may be vulnerable because they are less valued and the risks they experience are considered less important and less in need of remediation than the same risk experienced by a more valued member of society.” 46 In the context of research, involving members of socially vulnerable groups in research planning/design and oversight is the suggested strategy to guard against the discrimination or exploitation that might otherwise occur. 45 Similar considerations have been raised in the context of vulnerability among living organ donors—for example, that a family seeking a living donor might look first to its nonwage earning members, as their contributions to the family resources may be less visible and valued. 3
The majority of women who have undergone UTx to date in the United States do not fit the typical conception of “socially vulnerable” groups: they have been predominantly white, with above-average household income and levels of education. 25 The lack of access for lower income women, and those belonging to racial or ethnic minorities, needs to be addressed, as for other fertility treatments, through insurance coverage and other reimbursement policies that lower financial barriers,47,48 and through culturally competent education about and recruitment into clinical trials to produce a representative evidence-base regarding safety and effectiveness.
However, beyond traditional social vulnerability access concerns for UTx, contextual social vulnerability related to the stigma and stress experienced by women living with infertility49–51 must be considered. The attitudes that disvalue the social contributions of women with infertility have been internalized by many, who report feelings of inadequacy related to their inability to get pregnant, embarrassment about infertility, and feeling that family and friends look down on them. 49 Women's sense of childbearing responsibility has led them to pursue fertility treatments despite awareness of the risks to themselves—and to continue treatment even as the physical, emotional, and financial risks escalate with repeated failures and treatment intensification. 8 This tendency has been exacerbated in some cases through questionable practices by some assisted reproductive technology providers, exaggerating the claims of benefit from “add on” procedures, not providing age-specific estimates of likelihood of success, and basing marketing on poor-quality, ill-defined research. 41 Continuing treatment despite substantial risk and in the face of poor probability of success is also encouraged through online forums in which the “persistent patient” narrative—the woman who exhaustively researches treatment options, and undergoes multiple treatment cycles (enduring the related multiple failures), and ultimately achieves the success of pregnancy—is privileged and equated with deserving a child, encouraging women to feel that pursuing more therapy is the right approach.52,53 Even more concerningly, discussions about barriers to persistence—for example, lack of financial or social resources to pursue multiple rounds of treatment—in these forums are silenced or deliberately misunderstood to reappropriate the thread back to the preferred narrative.52,53 The historical lack of treatment for AUFI may have protected women with this condition from some of the pressures to pursue treatment regardless of risks. However, as the availability and success of UTx increase, the potential for similar pressures can be seen in research reports that have found candidates/potential candidates for UTx willing to make substantial financial investments, tolerate significant personal risk (ranking the risks to self below any risks to resultant children in importance), and to prioritize psychosocial risks—such as not falling pregnant or carrying to term after UTx—over physical risks associated with the procedure.54–56 Additionally, UTx candidates have previously reported social pressure to adopt 57 ; given the persistent stigma around adoption being a “second best” or less authentic option for parenthood, 58 the availability of UTx as an option that enables not only a genetic relationship to the child but a gestational one, may redirect the pressure towards UTx.
The psychosocial evaluation conducted at the beginning of the UTx process can help identify and address social vulnerability during initial decision-making about UTx candidacy but will have limited ability to counter those that may emerge over the course of the process, particularly for women who do not have early success with the graft or embryo transfer procedures, and want to keep trying beyond the limits of recipient graft time or number of pregnancies initially agreed upon in the UTx protocol. Decisions about second pregnancies and timing of graft hysterectomy have already been found to be emotionally charged and to require support from the UTx team psychologist, 59 and UTx programs should anticipate offering, or building into UTx protocols, ongoing psychological evaluation and support for UTx recipients.
Medical vulnerability considers the presence of a serious health-related condition in the intended recipient for which there is no other, or only less satisfactory, treatment. 3 The concern is that—where no other satisfactory options exist—medical exigency will lead patients to accept risks that would ordinarily be unacceptable. 45 Examples of conditions that create medical vulnerability are typically either imminently terminal (e.g., metastatic cancer) or significantly impede daily life (e.g., severe spinal cord injuries). 45 Infertility is recognized as a disease by such organizations as the World Health Organization, American Society for Reproductive Medicine, and American Medical Association, 60 and research conducted in women undergoing fertility treatment has determined that women frequently engage or persistent in treatment with low chances of success, in the face of substantial physical, emotional, and financial risks. 8 For women with AUFI, UTx offers the only path to parenthood that includes the experience of gestation. Uterus transplantation programs need to consider the medical vulnerability of potential candidates as they develop or update their eligibility criteria and screening process, balancing the need to respect the autonomy of women with AUFI willing to accept risks for the chance of pregnancy and parenthood against the ethical responsibility to avoid causing unacceptable harm. Additionally, as the evidence base accumulates to support it, UTx candidates should be given individualized estimates of the likelihood that UTx will result in pregnancy and a live birth for them, taking into account factors such as age and other health conditions that are known to influence success of IVF or other steps within the UTx process.
Situational vulnerability captures situations in which the medical exigency or other external factors impact the time allowed for adequate education and deliberation. 3 This should not be a significant source of vulnerability in UTx recipients as UTx is an elective procedure that does not treat a life-threatening or particularly time-dependent condition. While potential candidates approaching the upper age limits accepted for UTx may need to decide relatively quickly whether or not to pursue the option, the urgency would still be measured in weeks or months—providing adequate time for education and deliberation—rather than the minutes or hours in an emergency situation. For recipients using deceased donor uteri, decisions about whether to accept a specific organ may need to be made rapidly, but the opportunity to thoroughly explore, under little to no time constraint, with the transplant team what criteria might make a donor organ desirable or undesirable prior to any specific organ being offered, means there is little risk of situational vulnerability.
Allocational vulnerability focuses on the situation in which an individual's decision to consent is driven by a lack of subjectively important social goods that they believe will be provided as a consequence of participation or treatment. 3 In the case of living organ donation such social goods have been identified as including improved community social status or improved intrafamilial relationships, 3 and, in the specific case of related living uterus donors, obtaining grandmother status. 5 In the case of UTx recipients there are collateral benefits beyond the tangible outcomes of pregnancy and parenthood that may influence potential candidate's desire to undergo the procedure. It has previously been noted that women undergoing fertility treatments include the benefits of femininity and fertility among those that justify or outweigh the risks of physical harm associated with treatment. 56 This may be particularly influential for women with congenital AUFI: UTx clinical trial participants with congenital AUFI have described both the impact their infertility diagnosis had on their female identity and the impact UTx had on healing the related emotional scars through sharing the female experiences of menstruation and pregnancy.57,61,62 Similar social or psychological benefits have also been identified as a motivator for UTx in transgender women, should the procedure be expanded to this population. 63 The desire for experience of female identify and fertility and that for the experience of pregnancy and parenthood are likely to be entwined for many women seeking UTx. Given the temporary nature of at least some of the benefits around female identity 61 in contrast to the long-term consequences (impacting multiple people) of parenthood, it is important that the psychological evaluation conducted during the UTx screening process explore the relative weights of these motivations: where the former is particularly strong, allocational vulnerability may be a substantial risk, and counselling and other interventions around female identity may be needed before final decisions about whether to proceed with UTx are made. Similar considerations apply for decision-making around number of pregnancy attempts and timing of graft hysterectomy, which clinical trial experience has shown to be an emotionally charged process requiring support from a clinical psychologist. 59 In all these decisions the risks of retaining the graft (including kidney injury and increased risk for cancer related to prolonged use of immunosuppression, as well as the potential for graft rejection) have to be weighed against the desire to keep it, either for the purpose of continued attempts for pregnancy or related to aspects of female identity and experience.57,59
The final construct of vulnerability considered in the research taxonomy is infrastructural: Does the political, organizational, economic, and social context of the setting possess the integrity and resources needed to manage the relevant process and follow-up? 3 This vulnerability considers both institutional and individual support systems.
On the institutional side, infrastructure considerations are similar to the concept of ‘field strength’ of the institution described by Francis Moore in the context of ethical surgical innovation. 64 It covers the resources and facilities needed to provide the necessary care, including coping with any complications that may develop. For UTx programs in the US, the Organ Procurement and Transplant Network (OPTN) has established minimum criteria—primarily related to the qualifications of the primary transplant surgeon and the primary obstetrician-gynecologist. 65 Given the complex, multistep nature of UTx—and the potential vulnerabilities of candidates for it identified above—the necessary resources extend far beyond the OPTN criteria. Identified needs include multidisciplinary teams covering not only transplantation and obstetrics-gynecology but also urology, psychiatry/psychology, anesthesiology, pathology, infectious diseases, and intensive care, radiology, legal/risk/ethics, transgender care, and hospital leadership. 66 Clinical trial experience has also demonstrated the value of a careful screening process, including both clinical and psychosocial evaluations reviewed by a multidisciplinary selection committee to ensure safety and optimize recipient outcomes. 25 Other important infrastructure (shared with healthcare more generally) relates to that supporting decision-making for all possible candidates—such as access to translation services for those whose first language differs from that of the UTx program providers, and resources and strategies to address deficiencies in health literacy.
On the individual support system side, some UTx trials have included a requirement that candidates be living with a partner in a stable relationship, while others state a preference for such a relationship—recognizing the “support needed for the complex, invasive and lengthy process involved”—but only require the UTx candidate to have a good support system to participate. 21 The suggested framework for preoperative psychological evaluation that has been developed based on UTx clinical trial experience 31 includes examining the recipient's social support network, how the recipient and her spouse/partner have managed strains in the past and the stability of their relationship. Given the strains that fertility treatment can put on marriage and other family relationships,49,50,52 as well as the emotionally demanding nature of decisions that must be made throughout the UTx process as milestones are met (or fail to be met), 59 and changes in financial situation related to both the costs of fertility treatment and any changes in employment related to its time demands,50,67 ongoing psychosocial monitoring and support may be needed throughout the process.
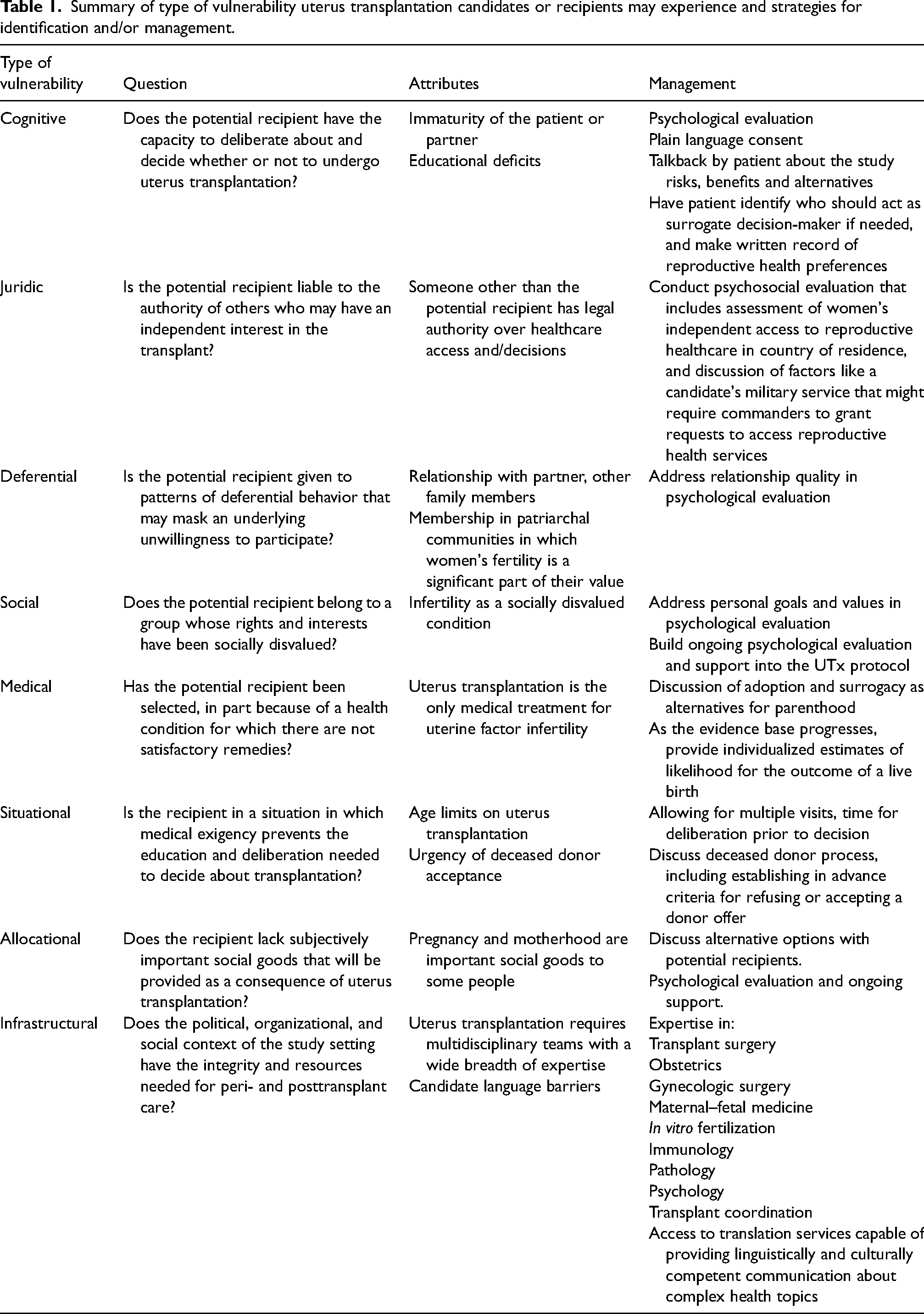
Table 1 summarizes the key questions and attributes of each type of vulnerability in the context of UTx candidates, as well as strategies implemented during the Dallas Uterus Transplant Study to mitigate or manage the different types of vulnerability candidates may experience. As none of these rely specifically on the research infrastructure, they can also be implemented in UTx programs offering the procedure outside the clinical trial context.
Summary of type of vulnerability uterus transplantation candidates or recipients may experience and strategies for identification and/or management.
Applying a consumer-driven model of vulnerability to UTx candidates/recipients
While different models of consumer vulnerability have been developed according to source and purpose, they broadly capture the point that vulnerability is multidimensional, can be experienced by anyone, may be temporary, and arises from interactions between internal factors (individual biophysical and psychosocial characteristics, as well as individual states, such as grief, transition, or motivation) and external conditions (such as structural or societal problems that are beyond the individual's control), creating powerlessness or lack of personal control, and thus dependence on others to create fairness in the marketplace. 9 Consumers respond to experiences of vulnerability, and the lack of control inherent in those, with a variety of coping strategies, including cognitive, emotional, and behavioral strategies, and acts of “consumer resistance” to express their free agency; however, when circumstances become too overwhelming, they may develop learned helplessness, in which motivation, emotion, and cognitive processes are uncontrollable. 9 The types of coping strategies an individual uses, and their success in using them, affect how they view themselves and how they believe others perceive them—in turn influencing their experience of vulnerability in new or ongoing consumer interactions. 9
The experience of consumer vulnerability can also elicit market or policy responses with the potential to facilitate or impede consumers’ agency and control in future encounters, thus also feeding back into the experience of consumer vulnerability. 9
While data stemming from the nonclinical trial context are not yet available for UTx, the commercial model it is entering—in terms of health care coverage, access to care, and a clientele motivated to achieve parenthood through pregnancy—is likely to resemble that of other fertility treatments, such as IVF. As such, the application of the consumer vulnerability model to women undergoing IVF, which was done with specific focus on how fertility clinics might reduce the experience of vulnerability, 11 provides some insight regarding considerations likely to apply in UTx. Figure 1 presents Baker et al.'s 9 conceptual model of consumer vulnerability in the context of UTx candidates and recipients.
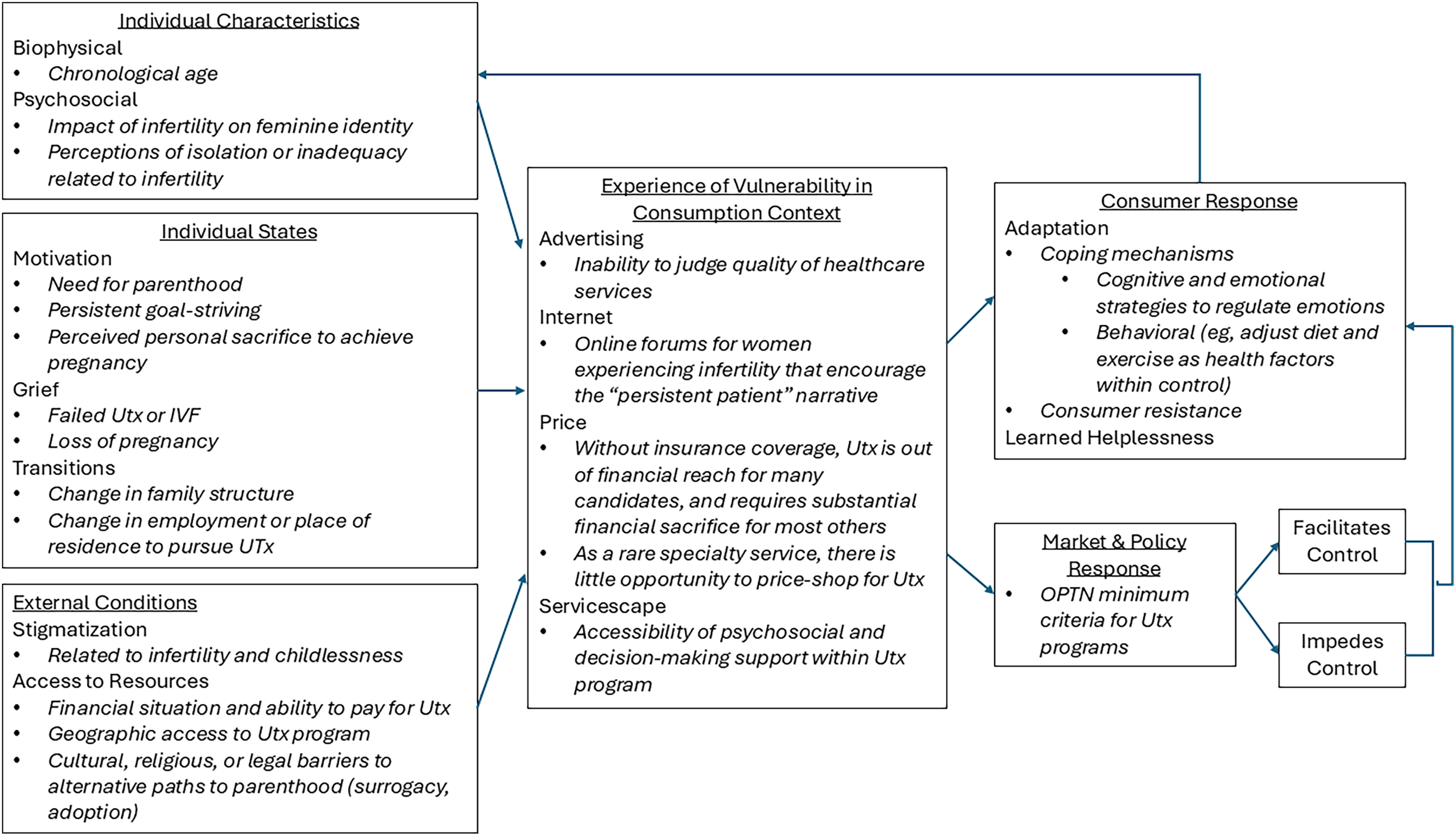
Consumer vulnerability model for uterus transplantation (UTx) candidates and recipients. Adapted from the Conceptual Model to Define Consumer Vulnerability published in Baker SM, Gentry JW, Rittenburg TL. Building Understanding of the Domain of Consumer Vulnerability. J Macromarket 2005;25:128–139. IVF: in vitro fertilization; OPTN: Organ Procurement and Transplantation Network; UTx: uterus transplantation.
Women seeking IVF may be motivated by a desire to fulfil a basic biological need of motherhood, as well as fitting perceived gender-role requirements, and complying with peer, social and family pressure to conceive a child. 68 Furthermore, women seeking infertility treatment may be experiencing feelings of anger, guilt, fear, sadness, and low self-esteem related to the diagnosis of infertility,49,69 contributing to feelings of loss of control over their reproductive health and the experience of vulnerability. 11 These internal factors can be compounded by the perceived stigma associated with both infertility and IVF treatment. 70 Certainly, greater desire or need for parenthood via IVF appears to make women seeking treatment more willing to accept additional risk—for example, any “new” or “add-on” IVF treatments despite unconfirmed efficacy, 71 indicating a hindered ability to effectively navigate the marketplace—that is, vulnerability. 11
Women experiencing vulnerability in their IVF consumer interactions respond with coping mechanisms—such as “persistent goal striving,” putting greater effort and determination into pursuing the desired goal of pregnancy, with associated increased personal sacrifice of other goals and priorities (e.g., career and finances). 11 In a study of 127 Australian women undergoing IVF, it was found that, while persistent goal striving reduced the experience of vulnerability by alleviating the perceived loss of control, the perceived personal sacrifice required to engage in this coping strategy increased the experience of vulnerability—outweighing the benefits for women with low chances of successful IVF. 11 As such, it was concluded that the actions IVF clinics can take to reduce women's experience of vulnerabilities depends on the woman's chance of success: for those with good probability of success, encouraging persistence in pursuing the goal of pregnancy is recommended to reduce vulnerabilities by reducing their perceived lack of control; in contrast, for women with a poor chance of success, managing expectations, rather than encouraging women to make additional personal sacrifices that increase their vulnerabilities in the face of continuing failure, is recommended. 11
As commercial availability of UTx continues to expand, the consumer vulnerability that has been demonstrated in IVF indicates that it will be important to empirically evaluate consumer vulnerability in UTx to inform policy responses that reduce rather than exacerbate vulnerabilities. The potential for persistent striving may need particular attention in the context of UTx, as the physical risks to the recipient—which include kidney injury and increased risk for cancer with prolonged immunosuppression, as well as graft rejection—are significant. 72 UTx clinical trial protocols have required graft hysterectomy at specific endpoints (e.g., after two live births or 5 years after transplant) to limit exposure to these risks, but nonetheless found that decisions about the timing of graft hysterectomy were emotionally challenging, requiring support from a clinical psychologist, and balancing preferences (or uncertainty) against medical risks of continued immunosuppression as well as those of an additional pregnancy. 59
Conclusion
Application of both the taxonomy of vulnerability developed for the research context and a consumer vulnerability model identify potential vulnerabilities throughout the process for women seeking UTx. These can largely be managed by requiring—as has been the case in UTx clinical trials—a psychosocial evaluation, in addition to a physical evaluation, to determine suitability as a UTx candidate, and using that evaluation to guide decisions about additional support (such as consultations with religious or cultural leaders to ensure culturally competent consent) or ongoing evaluations at critical points in the UTx process. As UTx moves out of the clinical trial context and potentially gains coverage under at least some health insurance policies or national health services, ensuring that provision is made for reimbursement for such evaluations and support will be critical. Given the reliance of UTx on IVF to achieve pregnancy, another important step UTx programs can take is to partner with IVF providers that have already implemented strategies to manage the vulnerabilities of women seeking IVF—such as providing age-specific probabilities of success, managing expectations for women with a poor chance of success, and only offering evidence-based “add-on” services—and to learn from these providers’ experience.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Data availability statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.