
Abstract
This article discusses what kinds of organisational and change processes take place when shifting to customer-oriented service concept, here called ‘third generation services’. Our interest lies in the learning process that produces the development of services in cities and regions in new ways and how to develop services in practice so that the customer is at the centre. Our article is a comparative study with special focus on reforms implemented in social and health care services. The material consists of case studies from cities and regions in several different countries, including Barcelona, Glasgow and Melbourne. The material has been gathered from service development projects in which the aim has been a shift over to services with the customer in the centre.
Introduction
In many countries, one of the most significant trends of change concerning the public sector has involved services and their conceptual basis (Hartley & Skletcher, 2008). This has been described as transfer from a production-oriented to a service-oriented approach (Osborne, 2009). It has not been just a question of developing the services, but in a wider sense of how, for example, cities and regions organise their operations with respect to civil society.
There are several underlying reasons for the changes in services. These include straitened economic circumstances, which have forced changes and technological progress that has offered novel ways to realise services. Needs and expectations of the citizens’ and the users’ of services have changed. The users have, for instance, higher levels of education and they demand personal service (Pasquier & Villeneuve, 2012). This has also created a new kind of operating environment for a learning and intelligent city (Anttiroiko, Valkama, & Bailey, 2013). The question is no longer what the service users – such as pupils and their parents – can learn from the city, but also what the city can learn from them, or how the city can utilise intelligent solutions to create conditions for personal learning among the service users.
Research literature has analysed the reform of services particularly as an ideological change (Bovaird & Löffler, 2012; Osborne, 2009; Pestoff, 2006). A novel concept of the customer has also been seen as a source of change (Jung, 2010). One possible starting point is that services are developed, above all, on the basis of observed problems occurring in service production (Laitinen, Aulton, Stenvall, & Kinder, 2015; Ostrom, 1973), and that this process of change can also be consciously implemented (Gulati, 2009).
The public sector has favoured zero tolerance to mistakes and avoidance of failures. This indicates a gap between daily routines, and new knowledge creation and its absence in modern public organisations. People who are focused on demonstrating competence are less likely interested in learning new skills, but repeat doing tasks where failure is unlikely and where they have succeeded before.
We have identified a paradigm shift in services. The key factors of the current generation of services are to enhance innovativeness, knowledge sharing, cooperation and iterative learning. These imply a concern with the knowledge and competencies of all stakeholders, how well organisation is led, how it is learning, how it adopts strategies, and how it interacts and mutually encourages and facilitates.
Three generations of service science
In our view, service thinking can be divided into three generations that can be analysed and defined using the framework presented by Risto Harisalo (cf. Laitinen, Harisalo, & Stenvall, 2013, p. 51). The differences between these generations lie not only in their concepts of the nature of services, but also in the ways the service system should be developed and what kind of learning processes their reform contains.
The first generation of service science concentrated primarily on single public services and service sectors. The objective was to understand the laws governing certain services, such as design services or health care and social services. Services were organised identifying the customers’ needs, but largely with a production-oriented approach. From the perspective of the public sector, the first generation services included the view that each service constitutes an independent unit or sector that must be examined from its internal conditions and circumstances. Each sector has its own professionally trained staff. Professionalism is strong in many public service sectors. A central feature of the first generation service science is hierarchy. Services are organised with production-oriented top-down approach. Professional, legislative, conditions define how services are produced and for whom. The laws governing services are also context-dependent, and the operating logic is of a one service sector – such as health care services – that cannot be transplanted to another sector.
The second generation service science aimed at comprehensively organising and arranging services to solve the customer’s problems. This has meant the notion that sectorally organised service systems operate with too narrow views in solving the problems the customers have. This generation sees service models as solutions to the customers’ problems (e.g. Rummler & Branche, 1990). Often these solutions are even tailor-made to the customer. This means that in second generation services it is understood that there is a connection between products and services (Normann, 1995). Therefore, a service can, for instance, include consultation and a solution-based on technology. Similarly, second generation services emphasise operational integration. Customers are possibly provided with services as a process that is collaboratively produced by several groups of professionals. This directs the focus even in the information and skills necessary for integrated services. Operating across organisational borders acts as a central catalyst for learning (Kinder, 2000). The second generation service science forces a comprehensive approach to services, because several factors are simultaneously affecting the ability to produce services appropriately. Therefore, the organisation of the service system pays attention to issues such as structures, culture, processes and cooperation.
Services of the third generation are based on the view that services shall be organised according to open systemic thinking (Chesbrough, 2003; Prahalad & Ramaswamy, 2004). From this perspective, services are constantly developing, interactive processes, where reformation and learning are based on information, experience and in-process learning, regarding the realisation of services as well as the planning of service processes. In third generation services it is, thus, possible to apply the methods of learning by experience and learning by doing (Argyris, 1977; Kolb, 1984). Third generation services employ the concepts of co-production and co-creation. The former refers to services being implemented and their contents defined together with the customer (Bovaird, 2007; Needham, 2008; Pestoff & Brandsen, 2010). Co-creation, on the other hand, refers to planning the services together with the customers (Chathoth, Altinay, Harrington, Okumus, & Chan, 2013; Grönroos & Voima 2011; Vargo, Maglio, & Akaka, 2008). Technological solutions are also a part of third generation services (Kristensson, Matthing, & Johansson, 2008). The use of technology enables, for instance, the transfer of information, the involvement of customers in services, and the production of interactive information. An example of the technological applications is a reform in Finnish tax administration. Technology is utilised to produce personal tax proposals to citizens. The citizens participate in the production of this service by accepting the proposal or making the necessary amendments.
The conceptual understanding of services, the organisation and management of service systems, as well as development and learning, essentially depend on which generation of services we are talking about. In this article, we are especially interested in the shift to third generation services. Therefore, we are examining case studies of service development realised in different countries where one can observe some tendency to move towards third generation services.
Comparative study
The key idea of service science is to combine the factors that create and build service into a single entity, in which the service is a unifying factor. This means looking at customers, administrative structures, financial resources, technology and other such elements from the service perspective. Since work under the traditional method of review regards service as a derivative of these factors, it has been difficult to discern the significance of the unique dynamics of services. Service science is an attempt to direct attention to services and create a theory of services, related factors and the forces involved.
This article takes the reader through a discussion of how service integration is no longer a matter of the integration of structures and services; the new approach leads one at the same time to complex and varied questions pertaining to such issues as determinate sciences, background assumptions, the role of legislation and political control and specification of the good of the customer.
The material has been collected from the cities of Barcelona, Den Bosch, Glasgow, Melbourne, Toronto and Vancouver; the Greater London area; and the US state of Vermont. The target cities showcase varied successes and models for service integration, which contributed to the reason these environments were chosen for study. Furthermore, the target cities represent countries in which ‘new public management’ (NPM) is utilised, and they have faced many of the same challenges in social and health services that are currently being worked on in Finnish discussion (Blomgren & Sahlin, 2007; Lane, 2000, p. 3, 7, 14, 41–43, 134–138).
The choice of the target cities for this comparative study was affected by reform-oriented thinking with respect to their integrated social and health services, and related new service models. Our first criterion when selecting target cities and organisations therein was their service organisation being covered within the social and health administration sphere in the relevant location. The second criterion was that each site must have had programmes and measures aimed at integration of social and health services, and that they have been measured and evaluated. The third condition was that the interviewees represent the top levels of management and the most extensive expertise in social and health services.
In the cities mentioned above, numerous people were interviewed, both individually and in teams; in all, there were 100 informants. Each personal interview lasted an hour, while the group interviews took 90 minutes each. The interviews were conducted in a semi-structured manner. All site visits and interviews were conducted between May and August 2012. In each city, the interviewees represented two distinct groups of professionals, the senior management of social and health services and, secondly, leading experts. In autumn 2012, after the interviews, conversations on the subject were managed through detailed questions and supplementary materials delivered via e-mail. The interviews were transcribed and analysed in the autumn of 2012.
As part of the methodological triangulation, documentary evidence in each target city was used, along with interviews and observations. The researchers also endeavoured to pay attention to what was not included in the documentation and other written materials, or what people did not want to include in it (Laitinen, 2009). This was used as complementary material.
The documentation gathered in the target cities included plans, reports, reviews, assessments and studies of services and their integration. A need for developing models of operation was identified as the common premise of the cities chosen for the comparison, where the aim had been to reduce bureaucracy, increase effectiveness and make the production of value in collaboration with the customer more efficient than previously.
The empirical material was used in searching for answers explicating the background motives and factors in the integration processes, the benefits and results aspired to by means of the integration, how the integration of social and health services is related to the revolution in service production, and the level of success of change management. This revolution in services is connected to the service generations presented above. The material has been used in analysis of how the integration discussion is situated in relation to the various generations of services; how integration is justified; and the differences and tensions, if any, between the grounds and goals, on the one hand, and the implementation, on the other. In the Finnish discussion, the benefits of integration have been deemed to extend to productivity, the availability of labour in the near future and the growing need for services that is being created by an ageing population.
Indeed, the development of productivity has been a key driver for the integration of social and health services. One challenge to the robustness of the public economy is posed by the trend in long-term health expenditure for an ageing population at a time when growth in service productivity remains weak. Another challenge posed to health services is that if there is no change to the methods and models of operation, both maintaining financial robustness and the shortage of labour will become a significant problem for Finnish society in the next few years. Pressure, from various quarters, that could affect the flexibility and availability of service production is related directly to growing customer demands and dwindling resources, which cannot be fully addressed by expansion of electronic services and striving to postpone employees’ retirement on their own initiative. In key respects, the development of productivity of health services is related to the aim to transform the service-production thinking of the first and second generations of thought.
As part of a general European trend, the number of hospitals and beds per capita has decreased, as has the number of beds in acute-care services. At the same time, the average duration of treatment has decreased. The above notwithstanding, the general trend in Europe involves hospitals remaining the primary source of treatment costs, accounting for more than half of all treatment expenses in the system in European Union (EU) member states (Pollitt, 2012).
Enhancing the production of public services has been judged to be one of the key questions with a bearing on the sustainability of the public economy on the whole. The discussion in the Nordic countries, for example, has been marked by a concern that, unless we want to be forced into cutbacks of public services, we will have to find a balance between defining our services and tax levels realistically and taking on public debt (Korkman, 2011; Kostiainen, 2009). Reforming and enhancing the service sector and the productivity of services can be regarded as a key method in this context.
The evidence indicates that the discussion of integrating and reforming social and health services has been associated with such enhancement efforts, because the services in question, in combination, account for a significant percentage of all public expenditure. This discussion of integration could be characterised as taking place on three fronts: being centred on health services; in a structure-centric fashion; and, most recently, focusing on the third-generation service models, especially in international discussion.
Discussion of the integration of social and health services
The choices of target cities are associated with good or best practice and learning from them, on the one hand, and, at the same time, with three points of emphasis in the integration-related discussion of social and health services – the perspectives of structures, customer participation and the development of the dynamics of the surrounding region.
According to the European material referred to above, the UK was the only country to develop and work further on a model covering the entire system. These efforts to reform proceeded from the goals of increasing user-centricity by emphasising the customer’s right of choice and through increasing the extent of partnership and collaboration. The ‘trust’ model of Britain’s national health services is known as one specific integration methods that has been tested in actual use. The British concepts of integration also encompass ‘managed care’, which also has historical links with the models of operation of social services.
In the Netherlands, personal budgeting and transmural care have been highlighted in integration models. This Dutch model differs from the versions of integration that focus on organisation; at the same time as being customer-centric, it emphasises the customers’ power and control of their own lives. For the most part, this transmural care, which has been based on cross-sectoral collaboration and converging co-operation since 1994, combines primary health care and specialised health care; it also brings together other operators in the treatment and care sectors, stressing bottom-up customer-centricity.
Through organisation-centric models, the City of Barcelona has engaged in varied experiments in horizontal and vertical integration. The Barcelona Interxarxes project, for instance, has become famous as a successful and effective method that integrates various services. Interxarxes is a customer-centric network of co-operation for the surrounding areas in the Horta-Guinardó district. Aimed at children and young people under 18 years of age, it brings together operators in the fields of health services, social welfare and education. The model involves operations in accordance with a matrix, which are carried out in a customer-centred and client-specific manner that integrates services into functions specified and designed in collaboration with the customer. One part of this new thinking is an effort, related to the model’s meta-level goals, to develop operation and service dynamics by drawing on diverse cases, through learning from the needs for change they highlight and from advances in service production and management. This model is also associated with active development of the surrounding region (Abril & Ubieto, 2008; Ubieto, 2012).
Integration experiments in Australian social and health services have had a history of two parts. In terms of structural, organisation-centric integration, on the one hand, history tells of integration experiments and the dissolution of structural integration. On the other hand, more recent integration thinking includes multi-profession, individualised care plans (IPSs) and also multidisciplinary services that have been integrated by function. In such cases, the premises are customer-centricity; services provided from a single address; and integration of services, partnerships, early intervention and evaluative case management. Important roles in this more recent discussion have been played by customer participation and models for developing and strengthening local communities (Carlyon, 2012; Community Health Services, 2008; Hugman, 2009; Wong, 2012).
Case management of individual services in its various forms has been applied in Australian, Canadian, and British services. The Canadian models entail good practices in, for instance, youth services and services for families with children and for the elderly. Canada has developed several models for around-the-clock operations at community centres for health and social services. These models emphasise multi-profession activities by employing the ‘one-stop shop’ principle. Under this model, Canadian integration experiments and models have used, among other tools, pooling of budgets, multidisciplinary teams, investments in prevention, care/case management, joint assessment practices, integrated information services and single-entry services (MacAdam, 2009).
The Canadian integration discussion also emphasises thinking centred on seamless co-operation (seamless care). Its starting point also is patient- or customer-centricity. Models whose developers originally strove for vertical integration (known as integrated services and integrated delivery systems (IDSs) but also as organised services, organised delivery systems or integrated delivery networks/integrated service networks) have begun to stress the comprehensive, general well-being of the customer. This has meant, for instance, expanding the seamless care chain for the elderly to address social factors such as income level, life management and linguistic capacity and the significance of social services is essential at the ‘seam point’ of a senior patient returning home (MacAdam, 2009; Putting Patients First, 2007).
The ‘Blueprint’ model, used in the state of Vermont in the US, is a specific service model with one source of financing. This model integrates operators and focuses on prevention and the activities of multi-profession teams. Its kinship and association with Kaiser Permanente is obvious, but it also features other elements that are associated with placing value on collaboration and learning together (Aejmelaeus, 2012).
Typology for the structure-centric integration.
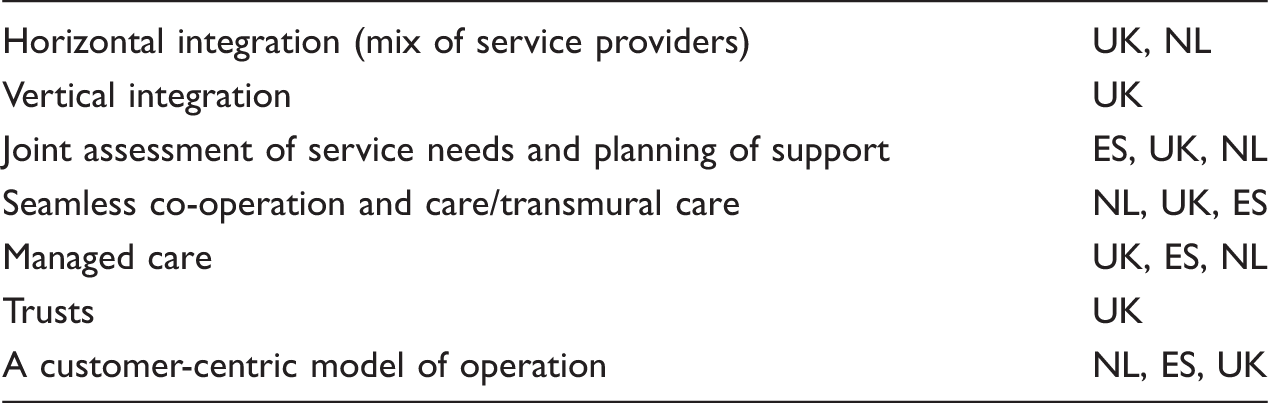
In the Table 1, Vertical Integration, refers to a model of operation wherein all services, such as those related to compensation and financing, are provided by one converging health management organisation (HMO), for instance. Transmural care denotes such care solutions as are aimed at convergence of primary health care with specialised health care through a departure from earlier sector-based divisions. Transmural care in, for example, the Dutch context involves such bottom-up solutions as are intended to eliminate boundaries along lines of the funding, organisation, co-operation and co-ordination related to both primary and specialised health care.
The term Managed Care refers to care wherein the aim is to create well-functioning care chains and control the growth of costs. In this case, the key position is held by a general practitioner who evaluates the need for care and then for further care, also assessing the value a specialist would provide in each case. Trusts refers to the British model under which foundations are charged not only with local duties in primary health care but also with duties in social services, mental health services, etc. These trusts have been established, through joint agreements between the National Health Service (NHS) and local authorities, in regions in which a need has been seen for close co-operation in the provision of social and health services.
One could say that the models of operation and policies described above are situated, most centrally, in the second-generation discussion of service production. The customer-centric model is more multidimensional in that the concept can be interpreted as belonging to both the second and the third generation, depending on its content. In our interview material, we distinguished between producing value for a customer and having the customer participate in the entire value-production process, from design all the way to assessment.
Development trends in integration discussions and models.
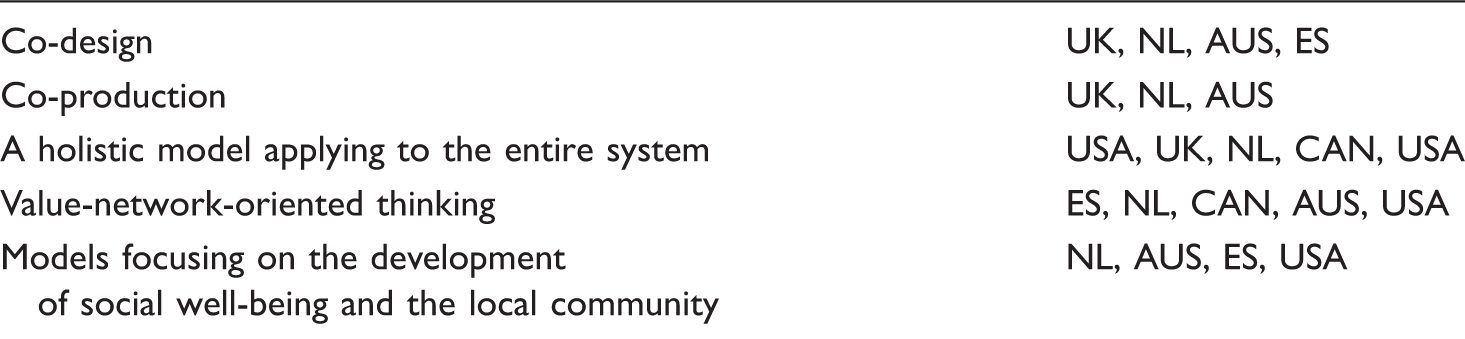
This classification shows focus on the customer and the operating environment as a way of thinking that applies to the whole system. The holistic system approach means systemic flexibility. We described this flexibility in relation to the customer and operating environment as a transition from a closed system to an open one. Within the confines of a closed system, services could be predetermined and be of standard type, even when the customer is engaged in the process. Engagement in closed systems has been seen mostly as involving consideration for how a standard service produces value for the customer.
The text above can be summed up with the conclusion that, according to our study, the trend of increase in services points to foci on three main areas. Integration models in social and health services express a transition from closed systems to open ones. This development has taken place in the areas of management, customer engagement and local co-operation models.
Management in the third-generation integrated service models
Structurally managed, integrated models of operation in social and health services can be divided into three main categories: 1. separate social and health services that co-operate, 2. a combined health service model under which the core function comprises separate units collected under it and the managers belong to a combined system of health services and 3. a decentralised model wherein employees in different professions and with different areas of competence and expertise have been decentralised across separate units. Of the above, the third category, in particular, has been regarded as a difficult model that should be strongly opposed in terms of professional identity and special competence in the profession. This model is not very commonly used. Alternatives versions and evolution of these models have begun to develop in the late 20th and early 21st century. In an integrated, decentralised model, profession-specific units, focusing on special competence, report to the management of combined health services, as in the second model described above, but operations in the units are grounded in team-based solutions and service agreements for combined services, which specify joint responsibility in service production.
A common trait of the models discussed above is that professional ‘tribes’ are preserved in all of them. The term ‘tribes’ in the context of professionals in health care and nursing was applied by Battie (1995), in a borrowing from social anthropology. In analysis extending the analogy, relations between individual trades and professions can be characterised as tribal conflicts. An illustration of Battie’s views can be found in the situation of integrated social and health services and, to some degree, be discerned among the areas of specialisation in various trades, though in a much more moderate form than that in the above-mentioned division between social and health services. The processes of classification and diversification can be linked to the mechanisms of tribalisation. In other words, the development of tribal professions is a type of struggle wherein classification and diversification are amongst the methods applied. Amongst the ways of drawing lines between professions via classification and diversification are education, professional skills, information and knowledge, competence, values, and their expression in relation to the clientele. In processes such as these, which create and categorise tribes, multidisciplinary work and a cross-profession approach are typically perceived as a threat (Hugman, 2009).
Management of integrated services has been given specific attention; it means not expanding that which existed before but, rather, a new method of management (McKimm & Held, 2009; McKimm & Phillips, 2009). Merely the premise that it involves perspectives of different schools of thought and guilds is a special challenge in the efficient management of integrated services when one is attempting to balance the independence and integration of separate professions (Engel & Gursky, 2009). A management implication is that the managers must be able to learn rapidly from those being managed; this does not and cannot mean applying only traditional principles of management and classic management models. Fundamentally, it must also incorporate emotional intelligence, competence in various aspects of change management, and continuous readiness for change (Engel & Gursky, 2009).
Our research material shows that change rooted in aspirations for integration is not implemented from one state to the next; instead, the process is always dynamic and creates value in its own right. In other words, it constantly – i.e. before change, during the change and after it – produces interpretations, understanding and perceptions of what is, why it is and what should be. That process of creating understanding is dynamic and interactive; it affects those taking part in the change while simultaneously being formulated by them. In our examples, tribes and their associated competitive situations, with the tensions between individual trades, can be described as associated with dynamism of this nature. It is significant from the standpoint of change and the integration process that the customer – a human – is chosen as a key element and motive, instead of a predetermined structure. As this selection is made, we make a transition from an internal, closed world of systems to an open world.
The integration structure is typically conceptualised such that third-generation management thinking entails multi-profession, customer-centric, integrated teams. In third-generation service models, the focus in the management is on customer-centricity and a holistic approach applied to the entire system. In such cases, enabling flexibility and promoting local solutions tailored to local circumstances are specified as relevant management duties. With openness of the system, this means a model of operation wherein customers, partners and associates have the opportunity to be part of the design, development and assessment of services.
Operation environments of this type share traits in common with networking, clear-cut operator and other roles being widened into multidimensional space, and increasing variation in conjunction with this development. Roles based on the position of public operators become blurred in both vertically and horizontally arranged networks. Management in such environments is developing from a starting point of positioning in relation to such relationships to create networks and interaction, along with an understanding of the customer’s needs. Networking brings a challenge to management efforts to synthesise divergence and variation, and to create a coherent entity from building blocks that feature such divergence. They are constructed together, linked fairly loosely to some other building blocks and relying on others for support.
Core questions of management in the third-generation models for integration of social and health services involve perspectives on how to produce services with the customer, how other service providers can be supported, and how services can be co-produced. The answers imply a change in the role of the management and a shift of the focal point from the manager’s position to management that emphasises the relationship. In other words, management in third-generation services is depicted in the relevant models not in terms of a position but as involving a relationship interaction.
Especially trust and learning processes are important in the context of third generation services. The organisation in which the interaction is the key thing can be characterised as a place where people may trust each other, members are trustworthy and may maintain self-respect – e.g. rights to their own perceptions and beliefs, and the possibility to integrate them with the reports, approaches, views, opinions and discussions. It pays attention to three meta-values, which are community, pleasure and meaning. Pleasure comes from learning and being creative. That kind of an organisation learns also from failures. When failures are accepted as a part of learning process, an organisation’s members are less motivated to cover up mistakes and their learning needs.
As far as management of a learning organisation is concerned, what is described above requires enhancing and strengthening the culture of learning, maintaining and rewarding a spirit of positiveness, and developing the work community such that independent thinking is permissible. Managing a learning organisation includes allowing people to take risks and rewarding them. Management in this context forces people to create structures and strategies whereby individuals and profit centres are each other’s resources and provide support instead of only partial optimisation.
The open system theory emphasises knowledge as a complex ongoing and mutual interpretation process, which is complex by its nature (Stenvall & Virtanen, 2015). That approach importantly rejects the idea of design processes as a black box or inside the minds of managers (Walsh, 1995) and instead insists upon active learning of groups and engagement by individuals. Especially, the open system in which customers are seen as co-designers and co-producers, shifts the role of learning. Co-design then becomes learning: iterative, creative and with a referencing context.
Innovative service models and customer-centricity
The roots of the ‘co-production’ concept can be traced to research projects in the analysis of political theory and programmes conducted by Elinor Ostrom at the University of Indiana in the 1970s. In her study, Ostrom used the concept to describe how the engagement of citizens in day-to-day life is limited and enabled in the production of public services. Ostrom struggled with the prevailing interpretations, ‘dominant urban governance theories’, which repeatedly proposed centralising administration and public services. Ostrom’s study group found no proof that centralisation and larger structures would provide any real benefits. They noticed that, instead, the quality of service perceived was linked to the engagement of the customer using the service (Pestoff, 2011).
In this context, co-production refers to micro-level activities in which residents or citizens at minimum take part in the production of their own public service. Over the past decade, this thinking has been refined from referring to the production of a service and been turned toward joint design and assessment. Conceptually, the writings produced by this school of thought have been bundled together under the terms ‘co-design’ and ‘co-production’, though the latter has begun to be taken to encompass service design in broader terms (Realpe & Wallace, 2010).
According to our research material, co-production is one of the most central new principles in the production of integrated social and health services. When we interviewed representatives of integrated social and health services, they commonly recognised co-production and cited it as the prevailing policy. It was seen as an important principle guiding and otherwise contributing to the development of operations in all of the target cities. Several participants were also able to associate it with a more extensive strategic change in the development of services.
Co-production was defined as, for example service design (co-design), an umbrella term for customer participation and co-production, a top-down–bottom-up approach and a functionalised model of local democracy.
Our interviewees generally saw genuine improvement of the customer or patient’s state and interactive development of services as grounds for integration. In other words, co-production is one of the key justifying goals and motives for integration of public institutions. Engaging a customer requires more: seamless co-operation and flexibility from the organisations mentioned above. In most of the target cities and their organisations, the levels of co-design and co-production were measured and assessed.
Co-production was the general principle in our target cities, but more typical areas of application in social and health services at the level of actual operations and activities included house-building and social housing, services for intoxicant abusers and mental-health patients, services for the handicapped, support for families, services for the elderly, and district associations and regional forums.
According to our interview material, co-production is an important, but still rather new way of thinking, one whose content and various options people are still learning, and where we are still at the beginning of the path, even though that path is the prevailing method of operation, as one interviewee described it. Co-production was seen as an approach that changes and brings development to operations but also as a risk, in the view of some interviewees. They stated that it poses a risk to the previous, profession-centric way of thinking and to operations in line with it. According to the interviewee mentioned above, at the same time, it involves being aware of a great risk from the organisation’s perspective – and not just awareness of it but also allowing that risk to exist.
Models related to co-production thinking have been developed, they are in use, and they are being assessed. It is interesting to note that resource thinking, whilst among the co-production premises described above, was not linked to co-production in many interviews. In fact, in much of the best practice presented by the target cities, use of additional resources was obvious. This was true of both social capital and financial resources.
In such cases, the models proceed from the principle of transition from illness-centricity towards comprehensive promotion and maintenance of both health and treatment, along with multi-profession treatment teams. Customer participation in service design and production means multi-sector co-operation with the customer. For instance, services are planned in customer forums, bottom-up, so that diverse metrics and methods of service design are applied. These methods include customer forums where traditional providers of social and health services work in collaboration with customers, together outlining a path for the patient. This service path is specified from the customer’s perspective, in stages, in line with the relevant needs. These methods make use of ethnographic approaches, narratives and idea workshops, among other techniques. The goal of customer-centricity and client-orientation serves as a starting point for service development (Laitinen et al., 2013).
Particular attention is paid to two target groups simultaneously: at-risk groups and customers needing special support in engagement. From the perspective of engagement, customers in need of special support require finding context-appropriate answers to the questions of who gives a voice to the silent and of how one is to listen to customers who cannot act independently as participants. Identifying risk groups is also, in part, related to how one moves the emphasis from the treatment of an illness to supporting and maintaining health. This means promoting a change in a customer’s risky behaviour by utilising peer support and new technology.
Ecosystems as co-operation models in services
So in a sense the changes in the organisational structure need to also be somehow reflected in changes on the ground in communities, how those services connect with all of their relevant stakeholders. Certainly in our case this is not something that we’ve done well. And I hope that this organisational restructure will lend itself to that improvement on the ground. (Interviewee.)
On the basis of our data, three converging factors can be linked to these views that emphasise local responsibility and local democracy as a part of third generation services. Firstly, the divergence of services follows local lines and communal spirit rather than fractures along functional boundaries; secondly, the factors act primarily horizontally and are related to eschewing hierarchical (and centralised) decision-making; and, thirdly, they emphasise, as a legitimating factor, participation rather than general efficiency stemming from standardisation efforts. At the level of ideals, the goal is to engage all those people belonging to the local community who are affected by the decisions made. When standardised procedures are supplemented by engagement, one finds that engaging governance – i.e. the open model – is a particularly efficient tool in implementation and in the pursuit of effectiveness (Pestoff, 2011).
We have outlined local co-operation models as ecosystems. In the context of third generation services by ‘ecosystems’, we mean up-and-coming models under which local, multi-form co-operation develops new activities through joint learning and innovation and via varied uses of resources. In our target cities in the current form of ecosystem thinking, the emphasis on concepts is being redefined and increasingly stresses elements such as ideas produced jointly, multi-sector approaches and collaboration with customers, (local, co-operative) culture and communal values, local co-operation between organisations, co-ordination, people’s creativity, problem-centric learning and co-operation with research institutes and universities, multi-channel communication and sharing of information and application of technology.
In such discussions, ecosystems have been seen as bounded by the local communities where the organisations and inhabitants operate, acting for the good of the local community to which they belong. In such cases, this ecosystem thinking refers to seeking the joint benefit of everyone. The question, then, is no longer one of co-ordinated co-operation between service providers so much as of customers taking part in the design and production of services; the ecosystem strives to enhance ‘bottom-up’ activation in the definition, design and production of services (Hwang & Horowitt, 2012; Laitinen, 2011; Voima et al., 2011; see also Mercan & Göktaş, 2011; Komninos, 2009; cf. Gómez et al., 2010).
In other words, efficiency involves how one can act outside the boundaries of one’s own organisation and create value in collaboration, rather than how one’s internal functions are managed. Those organisations acted in a pragmatic rather than an ideologically motivated fashion. We have named this direction of change ‘development of a local ecosystem in social and health services’.
The best and most efficient service models are local, flexible and holistic, and they engage local operators in service production in the local community. This is a ‘bottom-up’ approach; it emphasises holistic understanding of local characteristics just as much as joint discussion, design and production of services. The process discussed above contributes to the political programmes of third generation services no longer being able to be interpreted top-down rather than as ongoing local and multipartite negotiations among various groups of interested parties. Therefore, it is difficult to see even the production of public services merely as involving processes that generate true effectiveness of public groups of experts or professionals. In particular, it should be considered as a multilevel process with many participants and groups of participants.
We are stepping into a world of open systems from one of closed systems. This is a significant change. Its motivating factors and drivers have been divergence in customer needs, the need to engage customers, technological advances, constant development and the complexity of the issues. When standard solutions do not produce the desired results, the focus moves from ‘top-down’ definition of the standard toward ‘bottom-up’ flexibility and service production. In a process of this nature, particular attention is paid to creative interaction wherein better equivalence is attained through combining of tangible and intangible resources of various types. In other words, equivalence and effectiveness are more local and these are preferred over standard outputs. These micro-systems are the stuff of the new, ecosystem-oriented logic of open systems. That process utilises new technologies and a local approach.
Conclusions
According to our research material, discussion has undergone transition to third-generation service models and thinking. What service thinking and models of the third generation share is a position within the logic of an open system.
Our work shows that the co-production system is rising to a position in the nucleus of the discussion. This indicates that the role of local regions and a local approach will be enhanced, along with the role of the family and the user/customer, in the production of public services. We can name the following as starting points of this way of thinking: 1. identification of local communities and users of services as subjects and resources, 2. a change in the ways of working in public service production, 3. promotion of reciprocity and 4. enhancement of local networks.
Institutionalisation versus ego-centricity.
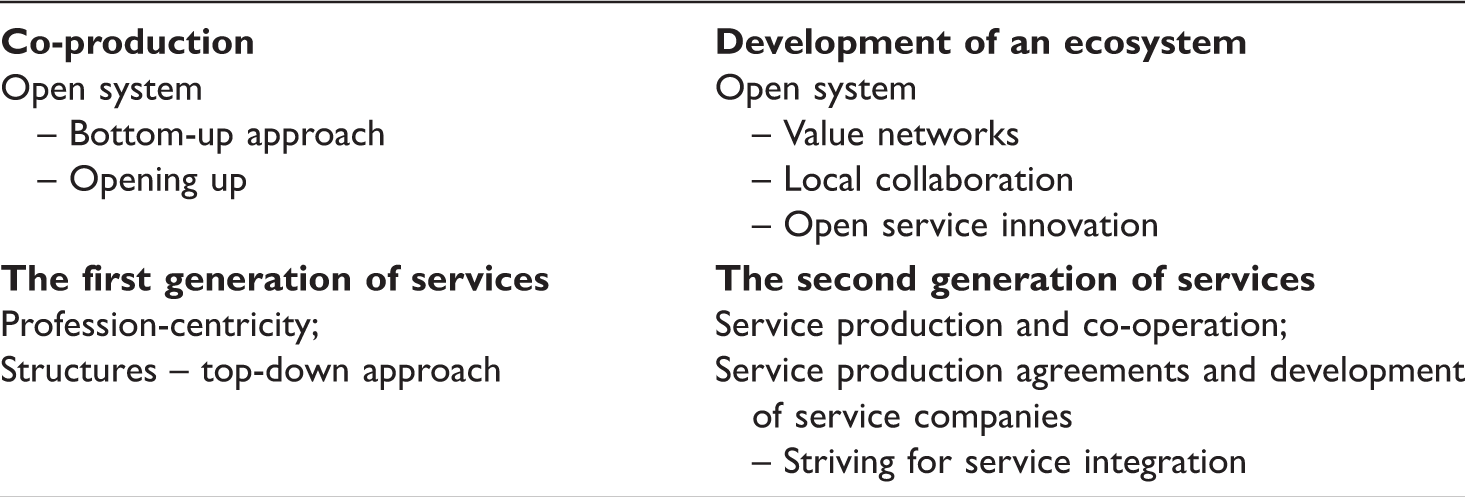
The top level in the table represents a lower level of institutionalisation, an open way of working and customer participation in service production. The top level can be compared to third-generation service production. The bottom level in the table is associated with greater institutionalisation. It reflects a more closed-type structure and administration- and expert-centricity. At the left in the table is the organisation’s ego-centricity, a micro level, and the right side represents a relationship between organisations, a meso level. The bottom left-hand corner can be compared to structure- and profession-centricity, discussed previously as representing the first generation of services. At the bottom right-hand corner, in contrast, is structures and service integration acting in concert. This is referred to above as the second service generation. The top left-hand corner is defined as co-production as defined in this chapter. The top right-hand corner represents development of a service ecosystem in an open environment.
Our research material suggests that a change is underway, with the discourse valuing the third generation although many practices still represent models of the first or second generation. Therefore, as one might expect in a transitional stage, the rhetoric and practical applications do not yet correspond to each other.
The theoretical foundation of the third generation of services comprises thinking associated with open systems and complexity sciences. In this context, local solutions are seen as based on flexibility, which is a fundamental element in bringing about equivalence and effectiveness. The local aspect also means development of the ecosystem that is based on an agile, ever-changing and open system. The primary characteristic of the system is that it is fine-tuned according to need, not on the terms of a push from the standards written on services. Flexibility makes it possible to respond to needs and make the services individualised and personal in collaboration with the customer – i.e. the service-user.
We are in the midst of a significant transition from the service models employed in agricultural and industrial societies. Today, our services are not extended or steered ‘top-down’; instead, the process proceeds, at its core, ‘bottom-up’. New technology has opened completely new opportunities for customer participation and self-direction in social and health services. According to our material, the trend should be expected to continue in the direction of becoming ever more personalised, incorporating big data and individualised service solutions.
As we move to an open system, it is worthy of note how a ‘both and’ logic is being realised in the third-generation services of multiple players. In others’ implementations, the third-generation models emphasise an ever more individualised, customer-oriented and somewhat more independent side and, at the same time, local co-operation and a communal spirit. Thus, supported by new technology, it simultaneously represents individuality as well as activation of the community, along with the choices and values of the local community.
According to the interviews, responding to the diversity of the operation environment requires a considerable change in organisational and management thinking, extending both to employees’ adaptability and to their capacity for collaborating with others. The case is one of co-evolution, the actors’ mutual development as forces bound to one another. The interview material in this study highlights the fact that, for the development of an entity such as a well-being ecosystem – preparing mutual goals and playing rules, increasing the customer’s decision-making power, and creating structures that support this are key factors in both innovativeness and the productivity of service production. Such a model of operation calls for openness and, equally, for readiness to learn with others and from others. However, managers in the social-welfare and health care organisations stated that they had not yet achieved that state of co-operation.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.